

Nutrition Status of Female Winter Sports Athletes


 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
4. Discussion
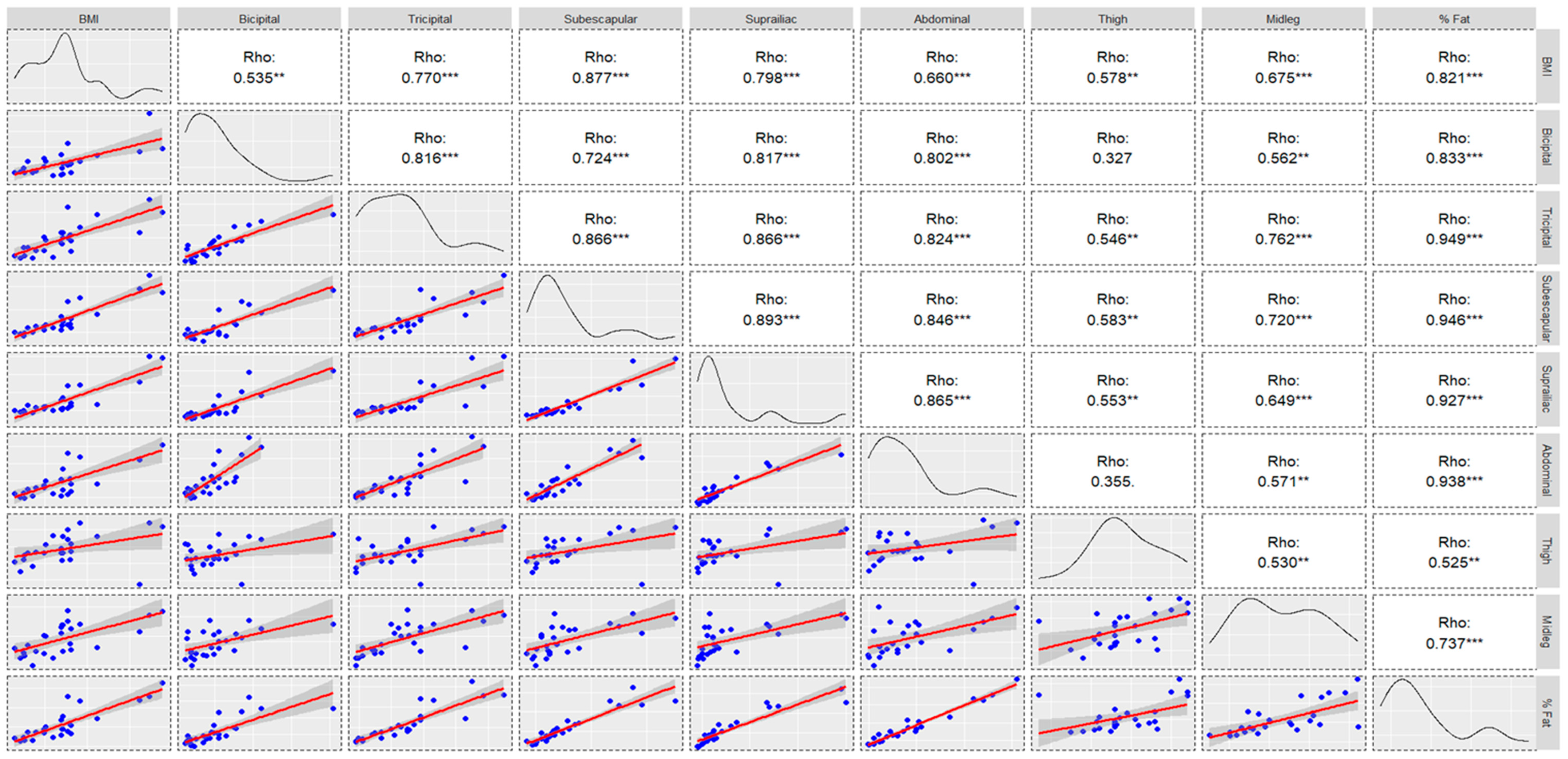
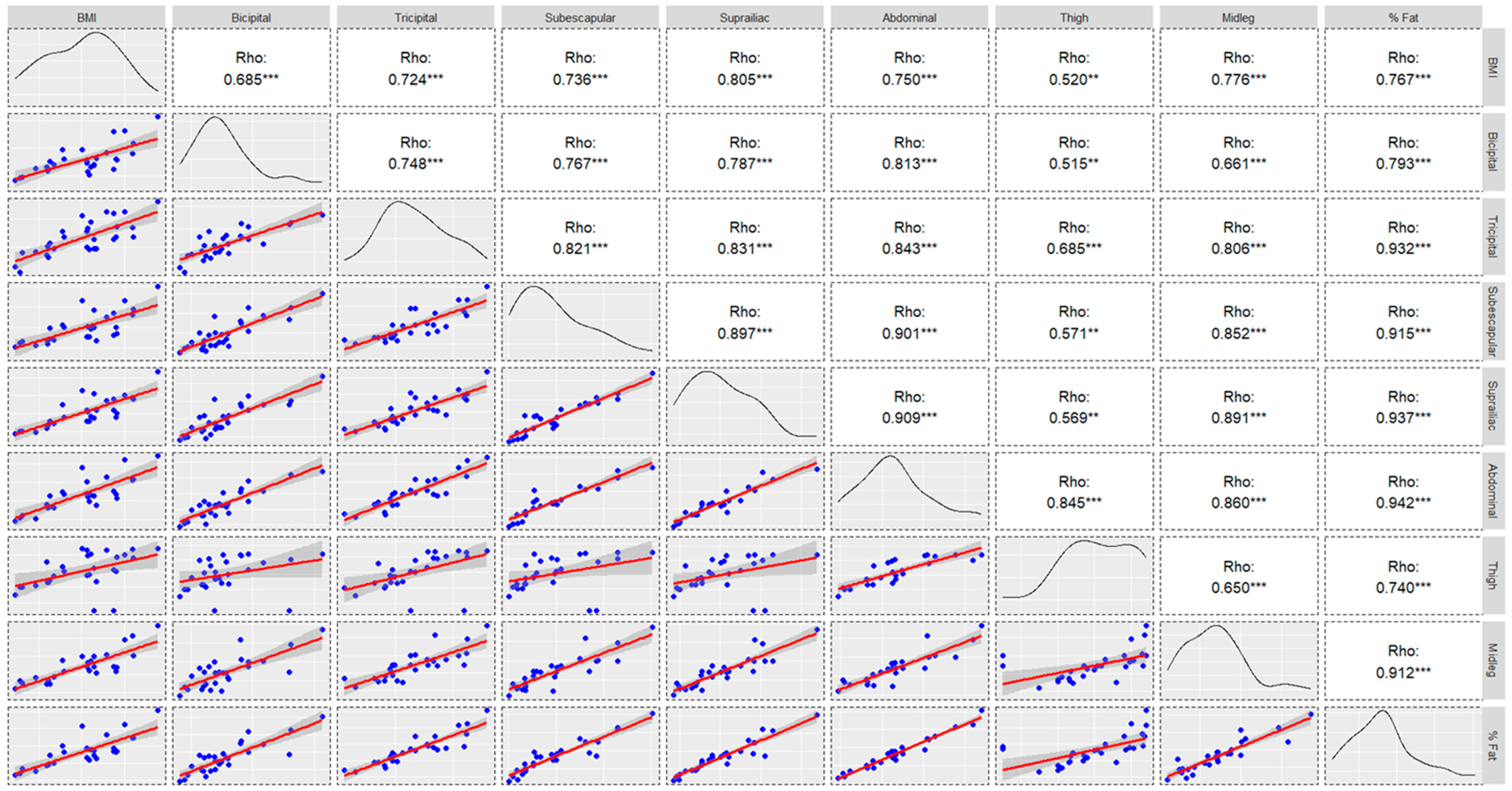
4.1. Anthropometry
4.2. Macronutrients
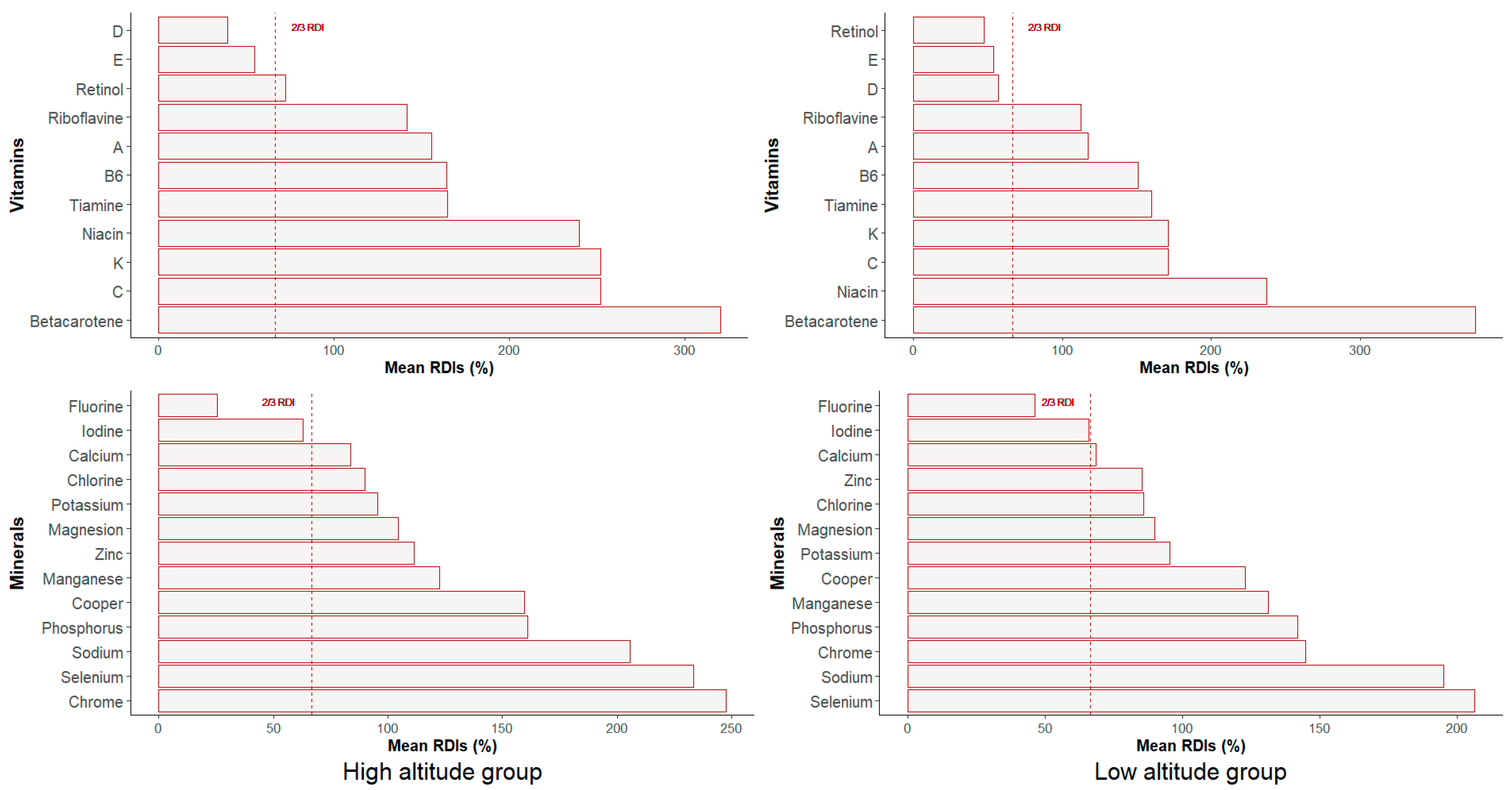
4.3. Micronutrients: Vitamins
4.4. Micronutrients: Minerals
4.5. Menstrual Cycle
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ravi, S.; Ihalainen, J.K.; Taipale-Mikkonen, R.S.; Kujala, U.M.; Waller, B.; Mierlahti, L.; Lehto, J.; Valtonen, M. Self-reported restrictive eating, eating disorders, menstrual dysfunction, and injuries in athletes competing at different levels and sports. Nutrients 2021, 13, 3275. [Google Scholar] [CrossRef]
- Vermeulen, T.F.; Boyd, L.A.; Spriet, L.L. Dietary macronutrient and micronutrient intake over a 7-day period in female varsity ice hockey players. Nutrients 2021, 13, 2262. [Google Scholar] [CrossRef]
- Meyer, N.L.; Manore, M.M.; Helle, C. Nutrition for winter sports. J. Sports Sci. 2011, 29 (Suppl. S1), S127–S136. [Google Scholar] [CrossRef]
- Butterfield, G.E. Nutrient Requirements at High Altitude. Clin. Sports Med. 1999, 18, 607–621. [Google Scholar] [CrossRef] [PubMed]
- Vigh-Larsen, J.F.; Ermidis, G.; Rago, V.; Randers, M.B.; Fransson, D.; Nielsen, J.L.; Gliemann, L.; Pill, J.F.; Morris, N.B.; De Paoli, F.V. Muscle Metabolism and Fatigue during Simulated Ice Hockey Match-Play in Elite Players. Med. Sci. Sports Exerc. 2020, 52, 2162–2171. [Google Scholar] [CrossRef] [PubMed]
- Vigh-Larsen, J.F.; Beck, J.H.; Daasbjerg, A.; Knudsen, C.B.; Kvorning, T.; Overgaard, K.; Andersen, T.B.; Mohr, M. Fitness Characteristics of Elite and Subelite Male Ice Hockey Players: A Cross-Sectional Study. J. Strength Cond. Res. 2019, 33, 2352–2360. [Google Scholar] [CrossRef]
- Petré, H.; Psilander, N.; Rosdahl, H. Between-Session Reliability of Strength- and Power-Related Variables Obtained during Isometric Leg Press and Countermovement Jump in Elite Female Ice Hockey Players. Sports 2023, 11, 96. [Google Scholar] [CrossRef]
- Akermark, C.; Jacobs, I.; Rasmusson, M.; Karlsson, J. Diet and muscle glycogen concentration in relation to physical performance in swedish elite ice hockey players. Int. J. Sport Nutr. 1996, 6, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Zaborova, V.; Kurshev, V.; Kryuchkova, K.; Anokhina, V.; Malakhovskiy, V.; Morozova, V.; Sysoeva, V.; Zimatore, G.; Bonavolontà, V.; Guidetti, L.; et al. Metabolic and Body Composition Changes in Ice Hockey Players Using an Ergogenic Drug (Cytoflavin). Biology 2023, 12, 214. [Google Scholar] [CrossRef]
- Mostaert, M.; Deconinck, F.; Pion, J.; Lenoir, M. Anthropometry, Physical Fitness and Coordination of Young Figure Skaters of Different Levels. Int. J. Sports Med. 2016, 37, 531–538. [Google Scholar] [CrossRef]
- Ziegler, P.J.; Jonnalagadda, S.S.; Lawrence, C. Dietary intake of elite figure skating dancers. Nutr. Res. 2001, 21, 983–992. [Google Scholar] [CrossRef]
- Conde-Pipó, J.; Valenzuela-Barranco, I.; López-Moro, A.; Román-Alconchel, B.; Mariscal-Arcas, M.; Zurita-Ortega, F. Influence of Alpine Skiing on Health-Related Quality of Life and Physical Self-Concept in Physically Active Adults over 55 Years of Age. Sports 2022, 10, 10. [Google Scholar] [CrossRef]
- Pellicer-Caller, R.; Vaquero-Cristóbal, R.; González-Gálvez, N.; Abenza-Cano, L.; Horcajo, J.; de la Vega-Marcos, R. Influence of Exogenous Factors Related to Nutritional and Hydration Strategies and Environmental Conditions on Fatigue in Endurance Sports: A Systematic Review with Meta-Analysis. Nutrients 2023, 15, 2700. [Google Scholar] [CrossRef]
- Seifert, J.G.; Burke, E.R.; White, A.; Luetkemeier, M.J. The effects of ad libitum fluid ingestion on fluid balance during alpine skiing in recreational skiers. J. Sports Sci. 2006, 24, 137–142. [Google Scholar] [CrossRef]
- Seifert, J.G.; Kipp, R.W.; Amann, M.; Gazal, O. Muscle Damage, Fluid Ingestion, and Energy Supplementation During Recreational Alpine Skiing. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Bigg, J.L.; Gamble, A.S.D.; Vermeulen, T.F.; Bigg, L.M.; Spriet, L.L. Sweat Loss and Fluid Intake of Female Varsity Ice Hockey Players During On-Ice Practices and Games. J. Strength Cond. Res. 2019, 34, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Palmer, M.S.; Heigenhauser, G.; Duong, M.; Spriet, L.L. Ingesting A Sports Drink Enhances Simulated Ice Hockey Performance while Reducing Perceived Effort. Int. J. Sports Med. 2017, 38, 1061–1069. [Google Scholar] [CrossRef]
- McCarthy, D.G.; Wickham, K.A.; Vermeulen, T.F.; Nyman, D.L.; Ferth, S.; Pereira, J.M.; Larson, D.J.; Burr, J.F.; Spriet, L.L. Impairment of Thermoregulation and Performance via Mild Dehydration in Ice Hockey Goaltenders. Int. J. Sports Physiol. Perform. 2020, 15, 833–840. [Google Scholar] [CrossRef]
- Hannon, M.P.; Flueck, J.L.; Gremeaux, V.; Place, N.; Kayser, B.; Donnelly, C. Key Nutritional Considerations for Youth Winter Sports Athletes to Optimize Growth, Maturation and Sporting Development. Front. Sports Act. Living. 2021, 27, 3. [Google Scholar] [CrossRef]
- Orysiak, J.; Mazur-Rozycka, J.; Fitzgerald, J.; Starczewski, M.; Malczewska-Lenczowska, J.; Busko, K. Vitamin D status and its relation to exercise performance and iron status in young ice hockey players. PLoS ONE 2018, 13, e0195284. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, M.; Giménez-Blasi, N.; Latorre-Rodríguez, J.; Martínez-Bebiá, M.; Bach-Faig, A.; Olea, F.; Mariscal-Arcas, M. Actualización sobre deficiencias nutricionales en la mujer deportista a partir de la literatura científica. Arch. Latinoam. Nutr. 2020, 70, 191–204. [Google Scholar] [CrossRef]
- Giménez-Blasi, N.; Latorre, J.A.; Martínez-Bebia, M.; Sáenz, M.; Cantero, L.; López-Moro, A.; Jiménez-Casquet, M.J.; Conde-Pipó, J.; Mariscal-Arcas, M. Menstrual Cycle and Sport: Effects on the performance and metabolism of the athlete woman. Retos 2022, 28, 565–572. [Google Scholar] [CrossRef]
- Conde-Pipó, J.; Bouzas, C.; Mariscal-Arcas, M.; Tur, J.A. Association between Functional Fitness and Health-Related Quality of Life in the Balearic Islands’ Old Adults with Metabolic Syndrome. Nutrients 2022, 14, 1798. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Rodríguez, A.; Sánchez-Sánchez, J.; Vicente-Martínez, M.; Martínez-Olcina, M.; Miralles-Amorós, L.; Sánchez-Sáez, J.A. Anthropometric dimensions and bone quality in international male beach handball players: Junior vs. senior comparison. Nutrients 2021, 13, 1817. [Google Scholar] [CrossRef]
- Kerksick, C.M.; Kulovitz, M. Requirements of Energy, Carbohydrates, Proteins and Fats for Athletes. In Nutrition and Enhanced Sports Performance; Elsevier: Amsterdam, The Netherlands, 2013; pp. 355–366. [Google Scholar]
- World Health Organization. Energy and Protein Requirements. Report of a Joint FAO/WHO/UNU Expert Consultation; World Health Organization Technical Report Series; World Health Organization: Geneva, Switzerland, 1985; Volume 724, pp. 1–206. [Google Scholar]
- WHO. Human Energy Requirements: Report of a Joint Fao/Who/Unu Expert Consultation, Rome 17–24 October 2001; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Calleja, C.A.; Hurtado, M.M.C.; Daschner, A.; Fernández Escámez, P.; Franco Abuín, C.M.; Giner Pons, R.M.; González Fandos, E.; González Muñoz, M.J.; Lopez Garcia, E.; Mañes Vinuesa, J.; et al. Informe del Comité Científico de la Agencia Española de Seguridad Alimentaria y Nutrición (AESAN) sobre Ingestas Nutricionales de Referencia para la población española. Rev. Com. Científico AESAM 2019, 29, 43–68. [Google Scholar]
- Cuervo, M.; Abete, I.; Baladia, E.; Corbalán, M.; Manera, M.; Basulto, J.; Martínez, J.A. Ingestas dietéticas de referencia para la población española, 2010. Act. Diet. 2010, 14, 196–197. [Google Scholar]
- Rivas, A.; Romero, A.; Mariscal, M.; Monteagudo, C.; Hernández, J.; Olea-Serrano, F. Validation of questionnaires for the study of food habits and bone mass. Nutr. Hosp. 2009, 24, 521–528. [Google Scholar]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under- recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar] [PubMed]
- Goldberg, G.R.; Black, A.E. Assessment of the validity of reported energy intakes-review and recent developments. Scand. J. Nutr. 1998, 42, 6–9. [Google Scholar] [CrossRef]
- Black, A.E.; Goldberg, G.R.; Jebb, S.A.; Livingstone, M.B.; Cole, T.J.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 2. Evaluating the results of published surveys. Eur. J. Clin. Nutr. 1991, 45, 583–599. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef]
- Black, A.E. The sensitivity and specificity of the Goldberg cut-off for EI:BMR for identifying diet reports of poor validity. Eur. J. Clin. Nutr. 2000, 54, 395–404. [Google Scholar] [CrossRef]
- Ortega, R.M.; López-Sobaler, A.M.; Andrés, P.; Requejo, A.M.; Aparicio, A.; Molinero, L.M. DIAL Software for Assessing Diets and Food Calculations. Department of Nutrition (UCM) & Alce Ingeniería. S.L. Madrid, Spain. 2016. Available online: http://www.alceingenieria.net/nutricion/descarga.htm (accessed on 12 November 2018).
- AUSNUT 2011-13 Food Nutrient Database. Available online: http://www.foodstandards.gov.au/science/monitoringnutrients/ausnut/ausnutdatafiles/Pages/foodnutrient.aspx (accessed on 12 November 2018).
- Ransdell, L.B.; Murray, T. A physical profile of elite female ice hockey players from the USA. J. Strength Cond. Res. 2011, 25, 2358–2363. [Google Scholar] [CrossRef] [PubMed]
- Ferland, P.M.; Comtois, A.S. Athletic Profile of Alpine Ski Racers: A Systematic Review. J. Strength Cond. Res. 2018, 32, 3574–3583. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.E.; Montgomery, D.L. Physiology of Alpine Skiing. Sports Med. 1988, 6, 210–221. [Google Scholar] [CrossRef]
- Seifert, J.; Kroll, J.; Muller, E. The relationship of heart rate and lactate to cumulative muscle fatigue during recreational alpine skiing. J. Strength Cond. Res. 2009, 23, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Conde-Pipó, J.; Bouzas, C.; Zurita-Ortega, F.; Olea-Serrano, F.; Tur, J.A.; Mariscal-Arcas, M. Adherence to a Mediterranean Diet Pattern, Physical Activity, and Physical Self-Concept in Spanish Older Adults. Nutrients 2022, 14, 12. [Google Scholar] [CrossRef]
- Dela, F.; Niederseer, D.; Patsch, W.; Pirich, C.; Müller, E.; Niebauer, J. Glucose homeostasis and cardiovascular disease biomarkers in older alpine skiers. Scand. J. Med. Sci. Sports. 2011, 21 (Suppl. S1), 56–61. [Google Scholar] [CrossRef]
- Niederseer, D.; Ledl-Kurkowski, E.; Kvita, K.; Patsch, W.; Dela, F.; Mueller, E.; Niebauer, J. Salzburg Skiing for the Elderly Study: Changes in cardiovascular risk factors through skiing in the elderly. Scand. J. Med. Sci. Sports 2011, 21 (Suppl. S1), 47–55. [Google Scholar] [CrossRef]
- Dervish, R.A.; Wilson, L.J.; Curtis, C. Investigating the prevalence of low energy availability, disordered eating and eating disorders in competitive and recreational female endurance runners. Eur. J. Sport Sci. 2023, 23, 869–876. [Google Scholar] [CrossRef]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P. Direct and indirect impact of low energy availability on sports performance. Scand. J. Med. Sci. Sports 2023. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe. Food-Based Dietary Guidelines in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2003. [Google Scholar]
- Valtueña, J.; Aparicio-Ugarriza, R.; Medina, D.; Lizarraga, A.; Rodas, G.; González-Gross, M.; Franchek, D. Vitamin D status in spanish elite team sport players. Nutrients 2021, 13, 1311. [Google Scholar] [CrossRef]
- Vitale, J.A.; Lombardi, G.; Cavaleri, L.; Graziani, R.; Schoenhuber, H.; La Torre, A.; Banfi, G. Rates of insufficiency and deficiency of vitamin D levels in elite professional male and female skiers: A chronobiologic approach. Chronobiol. Int. 2018, 35, 441–449. [Google Scholar] [CrossRef]
- Most, A.; Dörr, O.; Nef, H.; Hamm, C.; Bauer, T.; Bauer, P. Influence of 25-Hydroxy-Vitamin D Insufficiency on Maximal Aerobic Power in Elite Indoor Athletes: A Cross-Sectional Study. Sports Med. Open 2021, 7, 74. [Google Scholar] [CrossRef]
- Subudhi, A.W.; Davis, S.L.; Kipp, R.W.; Askew, E.W. Antioxidant Status and Oxidative Stress in Elite Alpine Ski Racers. Int. J. Sport Nutr. Exerc. Metab. 2001, 11, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Schippinger, G.; Fankhauser, F.; Abuja, P.M.; Winklhofer-Roob, B.M.; Nadlinger, K.; Halwachs-Baumann, G.; Wonish, W. Competitive and seasonal oxidative stress in elite alpine ski racers. Scand. J. Med. Sci. Sports 2009, 19, 206–212. [Google Scholar] [CrossRef]
- Larson-Meyer, D.E.; Gostas, D.E. Thyroid Function and Nutrient Status in the Athlete. Curr. Sports Med. Rep. 2020, 19, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-San Emeterio, C.; Antuñano, N.P.G.; López-Sobaler, A.M.; González-Badillo, J.J. Effect of strength training and the practice of alpine skiing on bone mass density, growth, body composition, and the strength and power of the legs of adolescent skiers. J. Strength Cond. Res. 2011, 25, 2879–2890. [Google Scholar] [CrossRef]
- Wohlgemuth, K.J.; Arieta, L.R.; Brewer, G.J.; Hoselton, A.L.; Gould, L.M.; Smith-Ryan, A.E. Sex differences and considerations for female specific nutritional strategies: A narrative review. J. Int. Soc. Sports Nutr. 2021, 18, 27. [Google Scholar] [CrossRef] [PubMed]
- Gorczyca, A.M.; Sjaarda, L.A.; Mitchell, E.M.; Perkins, N.J.; Schliep, K.C.; Wactawski-Wende, J.; Mumford, S.L. Changes in macronutrient, micronutrient, and food group intakes throughout the menstrual cycle in healthy, premenopausal women. Eur. J. Nutr. 2016, 55, 1181–1188. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable (Mean, SD) | Sample (N = 58) | Group | Sig. | Effect Size | ||
|---|---|---|---|---|---|---|
| High Altitude HA (n = 29) | Low Altitude LA (n = 29) | p | d | IC | ||
| Age (years) | 19.81(12.61) | 21.55(15.47) | 18.07(8.84) | 0.522 | 0.21 | (−0.31, 0.72) |
| Height (cm) | 153.16(17.51) | 149.17(21.23) | 157.14(11.85) | 0.230 | −0.46 | (−0.98, 0.06) |
| Weight (kg) | 51.70(17.82) | 46.21(16.70) | 57.19(17.46) | 0.031 | 0.64 | (0.11, −1.17) |
| BMI (kg/m2) | 21.28(4.50) | 19.98(4.38) | 22.59(4.31) | 0.028 | 0.60 | (0.07, 1.12) |
| Tricipital skinfold (mm) | 16.46(6.37) | 14.58(6.25) | 18.15(6.08) | 0.021 | 0.58 | (0.04, 1.12) |
| Bicipital skinfold (mm) | 9.23(5.01) | 7.64(4.12) | 10.65(5.36) | 0.010 | 0.62 | (0.08, 1.16) |
| Subscapular skinfold (mm) | 12.77(7.47) | 10.61(6.80) | 14.71(7.63) | 0.012 | 0.57 | (0.02, 1.10) |
| Supra-iliac skinfold (mm) | 13.01(8.68) | 10.42(8.42) | 15.33(8.37) | 0.008 | 0.59 | (0.04, 1.12) |
| Abdominal skinfold (mm) | 16.16(9.04) | 13.84(8.66) | 18.31(9.01) | 0.033 | −0.51 | (−1.06, 0.05) |
| Thigh skinfold (mm) | 24.24(10.01) | 23.45(9.00) | 24.94(10.95) | 0.473 | −0.15 | (−0.68, 0.38) |
| Midleg skinfold (mm) | 16.89(7.42) | 14.15(5.31) | 19.34(8.23) | 0.009 | 0.74 | (0.19, 1.29) |
| Faulkner body fat (%) | 14.59(4.38) | 13.27(4.05) | 15.77(4.39) | 0.013 | 0.59 | (0.05, 1.13) |
| Variable | Sample | Group | Sig. | Effect Size | ||
|---|---|---|---|---|---|---|
| High Altitude HA | Low Altitude LA | p | d | IC | ||
| BMR, kcal * | 1272.63(238.86) | 1197.33(261.85) | 1347.93(189.30) | 0.102 | 0.66 | (0.13, 1.19) |
| TEE, kcal * | 2068.52(613.89) | 2115.16(825.86) | 2021.89(283.94) | 0.699 | 0.15 | (−0.37, 0.67) |
| Energy intake, kcal * | 1755.76(453.28) | 1652.86(409.72) | 1858.66(477.98) | 0.125 | −0.46 | (−0.98, 0.60) |
| Water, g * | 2471.48(910.90) | 2242.00(861.03) | 2700.97(915.78) | 0.035 | −0.52 | (−1.04, 0.01) |
| Protein, g * | 80.81(28.30) | 76.11(19.88) | 85.51(34.48) | 0.262 | −0.33 | (−0.85, 0.19) |
| Carbohydrate, g * | 165.06(47.59) | 150.51(46.54) | 179.62(44.78) | 0.018 | 0.64 | (0.11, 1.16) |
| Lipid, g * | 80.21(30.33) | 77.65(28.82) | 82.76(32.07) | 0.797 | −0.17 | (−0.68, 0.35) |
| Simple carbohydrate | ||||||
| Glucose, g * | 7.78(4.59) | 6.25(3.93) | 9.32(4.75) | 0.004 | 0.70 | (0.17, 1.23) |
| Fructose, g * | 9.73(6.01) | 8.11(5.90) | 11.35(5.77) | 0.013 | 0.56 | (0.03, 1.08) |
| Lactose, g * | 9.12(6.48) | 7.69(5.12) | 10.56(7.41) | 0.135 | −0.45 | (−0.97, 0.07) |
| Soluble fiber, g * | 3.61(2.89) | 2.85(1.43) | 4.37(3.70) | 0.009 | 0.54 | (0.02, 1.06) |
| Indissoluble fiber, g * | 6.34(4.50) | 4.97(2.65) | 7.71(5.51) | 0.008 | 0.63 | (0.10, 1.16) |
| Cholesterol, mg * | 352.57(21.99) | 343.07(218.70) | 363.20(208.17) | 0.662 | −0.09 | (−0.63, 0.45) |
| Caloric profile | ||||||
| Proteins, % | 18.47(4.46) | 18.80(4.32) | 18.15(4.65) | 0.888 | 0.15 | (−0.37, 0.66) |
| Carbohydrates, % | 38.07(7.91) | 36.71(8.19) | 39.43(7.52) | 0.269 | −0.35 | (−0.86, 0.17) |
| Lipids, % | 40.49(7.20) | 41.62(7.28) | 39.36(7.06) | 0.297 | 031 | (−0.21, 0.83) |
| Lipids profile | ||||||
| SFA, % | 11.41(4.23) | 13.62(2.99) | 9.20(4.17) | 0.001 | 1.22 | (0.65, 1.78) |
| MUFA, % | 15.84(5.93) | 16.63(6.35) | 15.04(5.49) | 0.291 | 0.27 | (−0.25, 0.78) |
| PUFA, % | 5.08(2.57) | 4.99(2.49) | 5.16(2.70) | 0.779 | −0.06 | (−0.58, 0.45) |
| Mineral | Sample | Group | Sig. | Effect Size | |||
|---|---|---|---|---|---|---|---|
| High Altitude HA | Low Altitude LA | p | d | IC | |||
| Calcium | Intake, mg | 815(463.13) | 855.88(349.29) | 778.50(549.28) | 0.123 | 0.17 | (−0.38, 0.71) |
| % RDI | 75.70(40.81) | 83.75(36.39) | 68.52(43.77) | 0.059 | 0.38 | −0.17, 0.92) | |
| Iron | Intake, mg | 14.55(6.38) | 15.09(7.77) | 14.07(4.94) | 0.694 | 0.16 | (−0.38, 0.70) |
| % RDI | 110.48(59.42) | 117.26(59.32) | 104.43(59.94) | 0.322 | 0.22 | (−0.33, 0.75) | |
| Iodine | Intake, µg | 82.72(35.10) | 81.58(34.19) | 83.74(36.48) | 0.992 | −0.06 | (−0.60, 0.48) |
| % RDI | 64.50(30.31) | 62.82(29.09) | 65.99(31.81) | 0.823 | −0.10 | (−0.64, 0.44) | |
| Zinc | Intake, mg | 9.73(2.99) | 9.78(3.00) | 9.69(3.049 | 0.936 | 0.03 | (−0.51, 0.57) |
| % RDI | 97.68(49.56) | 111.37(56.34) | 85.45(39.76) | 0.085 | 0.54 | (−0.01, 1.08) | |
| Magnesium | Intake, mg | 285.32(109.85) | 292.20(125.18) | 279.18(96.06) | 0.796 | 0.12 | (−0.42, 0.66) |
| % RDI | 96.69(43.64) | 104.39(49.37) | 89.81(37.88) | 0.314 | 0.34 | (−0.21, 0.88) | |
| Potassium | Intake, mg | 2944.21(987.14) | 3004.68(1204.81) | 2890.21(761.59) | 0.852 | 0.12 | (−0.43, 0.65) |
| % RDI | 95.39(37.59) | 101.28(43.96) | 90.13(30.69) | 0.518 | 0.30 | (−0.25, 0.84) | |
| Sodium | Intake, mg | 2917.57) | 2962.88(1524.79) | 2877.11(1589.22) | 0.839 | 0.06 | (−0.48, 0.59) |
| % RDI | 200.03(109.41) | 205.63(110.84) | 195.03(109.90) | 0.730 | 0.10 | (−0.44, 0.64) | |
| Selenium | Intake, µg | 96.18(46.75) | 93.20(47.86) | 98.83(46.45) | 0.796 | −0.12 | (−0.66, 0.42) |
| % RDI | 219.15(128.30) | 233.32(154.83) | 206.49(100.21) | 0.734 | 0.21 | (−0.33, 0.75) | |
| Manganese | Intake, mg | 2.88(1.47) | 2.58(1.31) | 3.15(1.57) | 0.151 | −0.39 | (−0.93, 0.16) |
| % RDI | 127.22(58.34) | 122.62(49.48) | 131.33(65.89) | 0.755 | −0.15 | (−0.69, 0.39) | |
| Cooper | Intake, mg | 1.52(0.78) | 1.63(1.05) | 1.41(0.43) | 0.844 | 0.28 | (−0.26, 0.82) |
| % RDI | 140.18(79.08) | 159.43(103.30) | 122.99(43.70) | 0.322 | 0.47 | (−0.08, 1.01) | |
| Chrome | Intake, µg | 48.58(47.68) | 59.60(44.88) | 38.75(20.58) | 0.127 | 0.44 | (−0.10, 0.99) |
| % RDI | 193.36(206.89) | 247.56(274.49) | 144.96(101.55) | 0.128 | 0.47 | (−0.08, 1.01) | |
| Chlorine | Intake, mg | 1981.66(792.22) | 2019.80(919.47) | 1947.61(674.31) | 0.907 | 0.09 | (−0.45, 0.63) |
| % RDI | 87.94(36.21) | 90.07(41.67) | 86.03(31.20) | 0.852 | 0.11 | (−0.43, 0.65) | |
| Fluorine | Intake, mg | 2.34(1.06) | 2.22(1.12) | 2.44(1.01) | 0.446 | −0.20 | (−0.74, 0.33) |
| % RDI | 36.59(37.45) | 25.64(29.58) | 46.36(41.39) | 0.123 | 0.57 | (0.02, 1.12) | |
| Phosphorus | Intake, mg | 1324.98(396.61) | 1347.28(410.20) | 1305.07(390.53) | 0.957 | 0.11 | (−0.43, 0.64) |
| % RDI | 150.92(65.08) | 161.07(61.87) | 141.85(67.63) | 0.210 | 0.30 | (−0.25, 0.84) | |
| Vitamin | Sample | Group | Sig. | Effect Size | |||
|---|---|---|---|---|---|---|---|
| High Altitude HA | Low Altitude LA | p | d | IC | |||
| Thiamine | Intake, mg | 1.59(0.69) | 1.54(0.72) | 1.78(0.73) | 0.865 | 0.07 | (−0.47, 0.61) |
| % RDI | 162.31(73.20) | 164.98(73.44) | 159.92(74.26) | 0.809 | 0.07 | (−0.47, 0.61) | |
| Riboflavin | Intake, mg | 1.69(0.60) | 1.84(0.66) | 1.55(0.51) | 0.107 | 0.50 | (−0.05, 1.05) |
| % RDI | 126.37(49.54) | 141.88(58.52) | 112.52(35.52) | 0.054 | 0.62 | (0.06, 1.05) | |
| Niacin | Intake, mg | 35.03(10.85) | 34.92(11.56) | 35.15(10.24) | 0.809 | −0.02 | (−0.56, 0.52) |
| % RDI | 238.53(77.73) | 242.30(86.95) | 234.31(67.44) | 0.914 | 0.10 | (−0.44, 0.64) | |
| B6 | Intake, mg | 2.19(0.80) | 2.12(0.68) | 2.25(0.90) | 0.661 | −0.15 | (−0.69, 0.39) |
| % RDI | 157.34(62.08) | 164.35(58.52) | 151.07(65.52) | 0.309 | 0.21 | (−0.33, 0.75) | |
| Folic acid | Intake, µg | 275.75(132.40) | 278.60(146.28) | 273.21(121.35) | 0.950 | 0.04 | (−0.50, 0.58) |
| % RDI | 88.74(46.67) | 96.19(50.27) | 82.10(43.03) | 0.170 | 0.30 | (−0.24, 0.84) | |
| B12 | Intake, µg | 4.77(4.109 | 4.42(2.17) | 5.08(5.28) | 0.590 | −0.16 | (−0.70, 0.38) |
| % RDI | 174.39(199.31) | 141.07(77.88) | 204.15(263.00) | 0.475 | −0.32 | (−0.86, 0.23) | |
| Vitamin C | Intake, mg | 118.32(94.48) | 121.60(116.33) | 115.39(71.73) | 0.816 | 0.07 | (−0.47, 0.60) |
| % RDI | 210.00(185.74) | 252.30(245.17) | 170.84(94.22) | 0.489 | 0.45 | (−0.11, 0.99) | |
| Vitamin A | Intake, µg | 901.00(503.10) | 988.84(608.11) | 822.57(381.11) | 0.636 | 0.33 | (−0.21, 0.87) |
| % RDI | 135.62(93.56) | 155.48(105.29) | 117.23(78.78) | 0.785 | −0.04 | (−0.58, 0.51) | |
| Vitamin D | Intake, µg | 2.57(2.40) | 1.98(1.55) | 3.09(2.89) | 0.172 | −0.47 | (−1.02, 0.08) |
| % RDI | 48.72(40.61) | 39.59(30.92) | 57.18(46.89) | 0.226 | −0.44 | (−0.99, 0.11) | |
| Vitamin E | Intake, mg | 8.15(3.75) | 8.19(4.59) | 8.10(2.89) | 0.655 | 0.02 | (−0.52, 0.56) |
| % RDI | 54.30(25.00) | 54.61(30.58) | 54.02(19.29) | 0.655 | 0.02 | (−0.52, 0.56) | |
| Vitamin K | Intake, µg | 168.43(144.84) | 179.08(172.28) | 158.92(117.56) | 0.907 | 0.14 | (−0.40, 0.68) |
| % RDI | 179.01(169.36) | 210.36(197.86) | 151.02(136.81) | 0.462 | 0.35 | (−0.19, 0.89) | |
| Retinol | Intake, µg | 384.58(343.87) | 469.68(388.07) | 308.63(284.94) | 0.025 | 0.48 | (−0.07, 1.02) |
| % RDI | 59.17(52.90) | 72.25(59.70) | 47.48(43.84) | 0.462 | 0.35 | (−0.19, 0.89) | |
| Betacarotene | Intake, µg | 2452.37(896.53) | 2239.59(1658.70) | 2690.70(2141.49) | 0.538 | −0.24 | (−0.78, 0.31) |
| % RDI | 350.34(270.93) | 319.94(236.96) | 384.39(305.93) | 0.538 | −0.24 | (−0.78, 0.31) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Casquet, M.J.; Conde-Pipó, J.; Valenzuela-Barranco, I.; Rienda-Contreras, R.; Olea-Serrano, F.; Bouzas, C.; Tur, J.A.; Mariscal-Arcas, M. Nutrition Status of Female Winter Sports Athletes. Nutrients 2023, 15, 4472. https://doi.org/10.3390/nu15204472
Jiménez-Casquet MJ, Conde-Pipó J, Valenzuela-Barranco I, Rienda-Contreras R, Olea-Serrano F, Bouzas C, Tur JA, Mariscal-Arcas M. Nutrition Status of Female Winter Sports Athletes. Nutrients. 2023; 15(20):4472. https://doi.org/10.3390/nu15204472
Chicago/Turabian StyleJiménez-Casquet, María José, Javier Conde-Pipó, Ignacio Valenzuela-Barranco, Raquel Rienda-Contreras, Fátima Olea-Serrano, Cristina Bouzas, Josep A. Tur, and Miguel Mariscal-Arcas. 2023. "Nutrition Status of Female Winter Sports Athletes" Nutrients 15, no. 20: 4472. https://doi.org/10.3390/nu15204472
APA StyleJiménez-Casquet, M. J., Conde-Pipó, J., Valenzuela-Barranco, I., Rienda-Contreras, R., Olea-Serrano, F., Bouzas, C., Tur, J. A., & Mariscal-Arcas, M. (2023). Nutrition Status of Female Winter Sports Athletes. Nutrients, 15(20), 4472. https://doi.org/10.3390/nu15204472