
Relationship between Lean Tissue Mass and Muscle Function in Women with Obesity

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject
Participant Consent
2.2. Methods
2.2.1. Determination of LTM and FM
2.2.2. Cut-Offs Used for the Definition of Low LTM
2.2.3. Assessment of Muscle Performance
2.2.4. Sarcopenic Obesity Definition
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients
3.2. Body Composition
3.3. Sarcopenic Index
3.4. Muscle Function
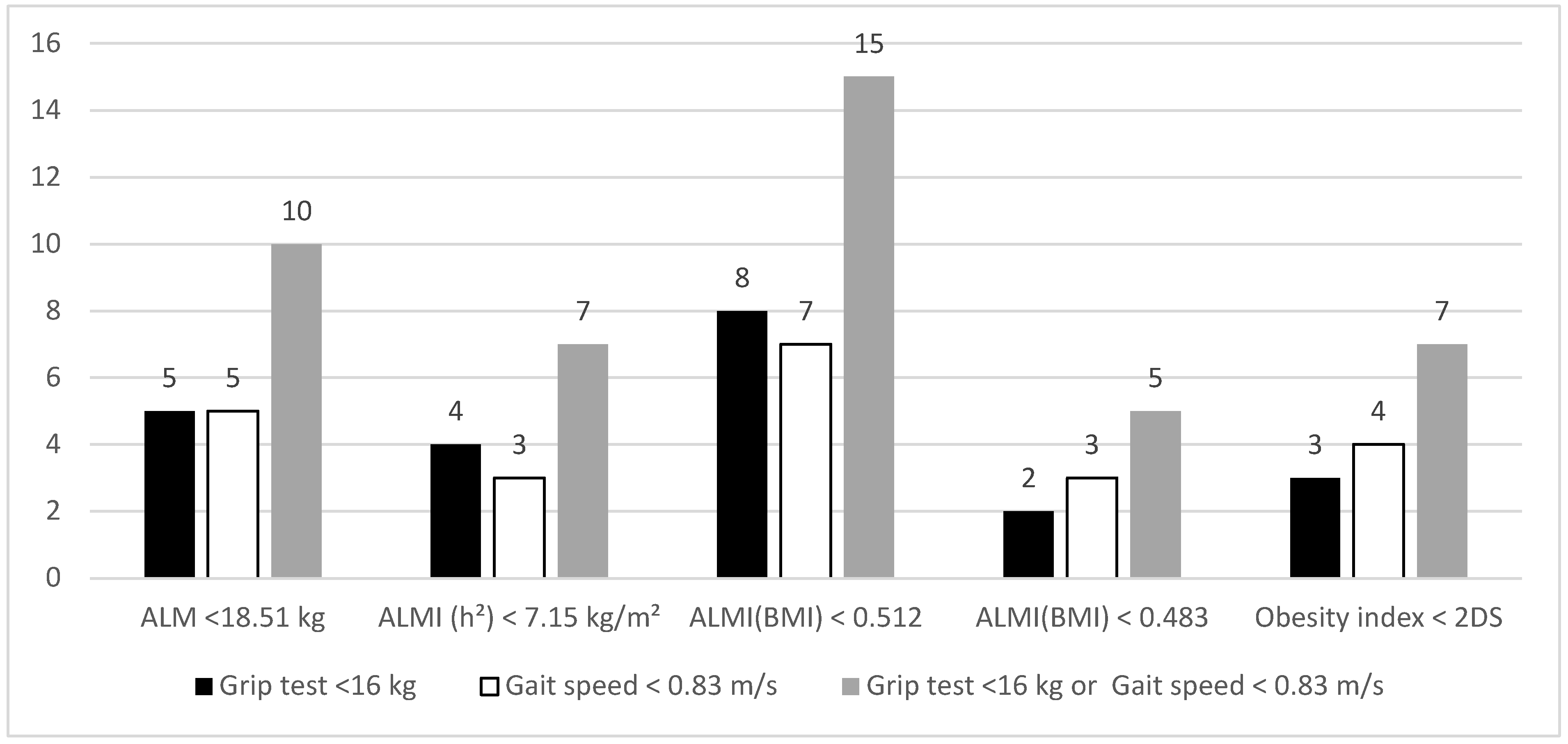
3.5. Prevalence of Sarcopenic Obesity
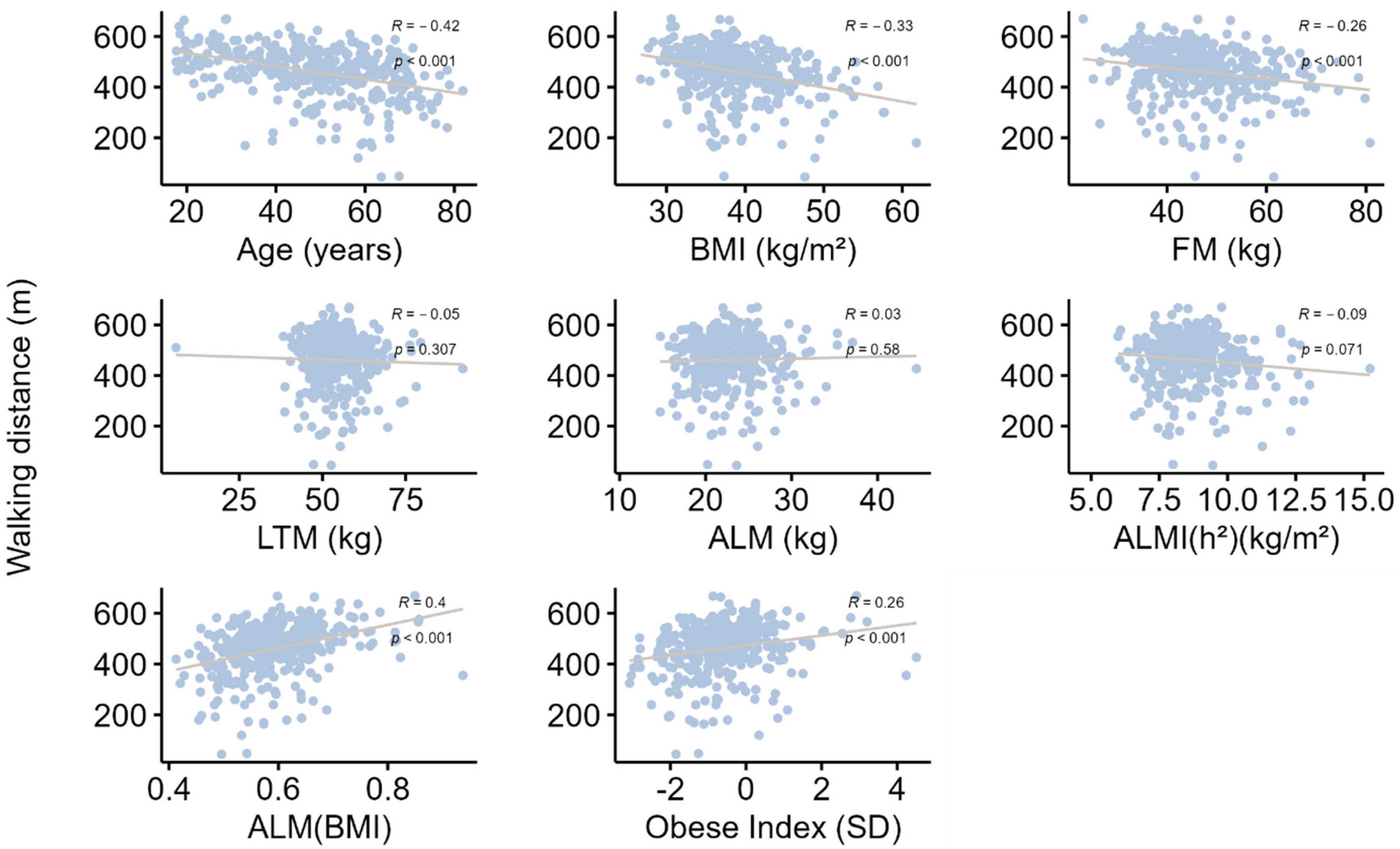
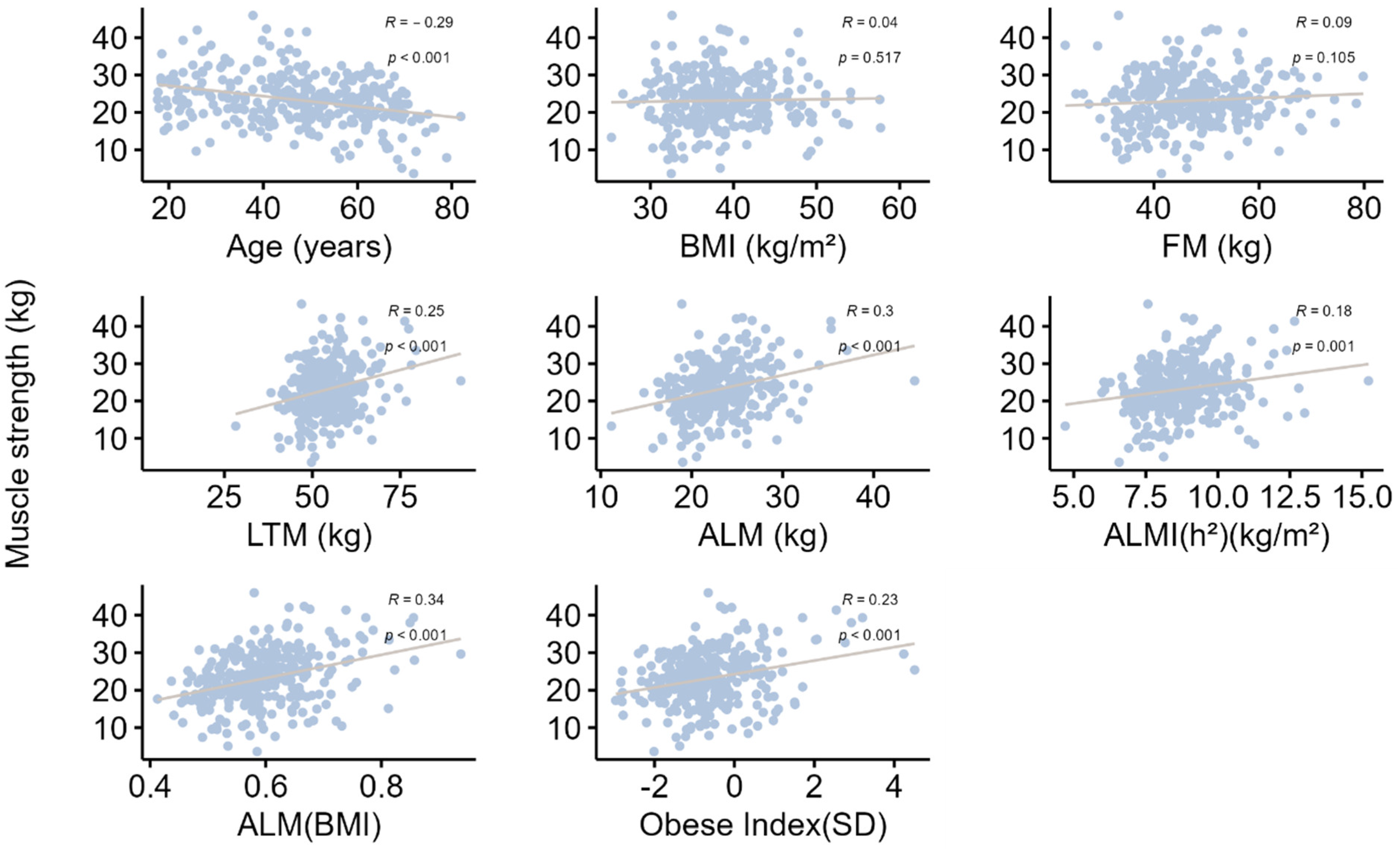
3.6. Impact of Age and BMI on Muscle Mass and Muscle Performance
4. Discussion
4.1. Body Composition Change with Age
4.2. Variation in Muscle Function with Age
4.3. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baumgartner, R.N.; Stauber, P.M.; McHugh, D.; Koehler, K.M.; Garry, P.J. Cross-sectional age differences in body composition in persons 60+ years of age. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, M307–M316. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.M.; Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J. Appl. Physiol. (1985) 2000, 89, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Genton, L.; Hans, D.; Karsegard, L.; Slosman, D.O.; Pichard, C. Age-related differences in fat-free mass, skeletal muscle, body cell mass and fat mass between 18 and 94 years. Eur. J. Clin. Nutr. 2001, 55, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Coin, A.; Sergi, G.; Minicuci, N.; Giannini, S.; Barbiero, E.; Manzato, E.; Pedrazzoni, M.; Minisola, S.; Rossini, M.; Del Puente, A.; et al. Fat-free mass and fat mass reference values by dual-energy X-ray absorptiometry (DEXA) in a 20–80 year-old Italian population. Clin. Nutr. 2008, 27, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. 2018, 14, 513–537. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Wayne, S.J.; Waters, D.L.; Janssen, I.; Gallagher, D.; Morley, J.E. Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes. Res. 2004, 12, 1995–2004. [Google Scholar] [CrossRef]
- Roh, E.; Choi, K.M. Health Consequences of Sarcopenic Obesity: A Narrative Review. Front. Endocrinol. 2020, 11, 332. [Google Scholar] [CrossRef]
- Prado, C.M.; Wells, J.C.; Smith, S.R.; Stephan, B.C.; Siervo, M. Sarcopenic obesity: A Critical appraisal of the current evidence. Clin. Nutr. 2012, 31, 583–601. [Google Scholar] [CrossRef]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Clin. Nutr. 2022, 41, 990–1000. [Google Scholar] [CrossRef]
- Batsis, J.A.; Barre, L.K.; Mackenzie, T.A.; Pratt, S.I.; Lopez-Jimenez, F.; Bartels, S.J. Variation in the prevalence of sarcopenia and sarcopenic obesity in older adults associated with differente research definitions: Dual-energy X-ray absorptiometry data from the National Health and Nutrition Examination Survery: 1999–2004. J. Am. Geriatr. Soc. 2013, 61, 974–980. [Google Scholar] [CrossRef]
- Purcell, S.A.; Mackenzie, M.; Barbosa-Silva, T.G.; Dionne, I.J.; Ghosh, S.; Siervo, M.; Ye, M.; Prado, C.M. Prevalence of Sarcopenic Obesity Using Different Definitions and the Relationship with Strength and Physical Performance in the Canadian Longitudinal Study of Aging. Front. Physiol. 2020, 11, 583825. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, M.; Mazzali, G.; Fantin, F.; Rossi, A.; Di Francesco, V. Sarcopenic obesity: A new category of obesity in the elderly. Nutrition, metabolism, and cardiovascular diseases. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Maimoun, L.; Mura, T.; Avignon, A.; Mariano-Goulart, D.; Sultan, A. Body Composition in Individuals with Obesity according to Age and Sex: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 1188. [Google Scholar] [CrossRef]
- Maimoun, L.; Serrand, C.; Mura, T.; Renard, E.; Nocca, D.; Lefebvre, P.; Boudousq, V.; Avignon, A.; Mariano-Goulart, D.; Sultan, A. Definition of an adapted cut-off for determining low lean tissue mass in older women with obesity: A comparison to current cut-offs. Sci. Rep. 2022, 12, 16905. [Google Scholar] [CrossRef]
- WHO. Obesity and Overweight—Fact Sheet. Nº311. [Updated January 2015; May 2016]. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 13 July 2023).
- Ray, K.K.; Colhoun, H.M.; Szarek, M.; Baccara-Dinet, M.; Bhatt, D.L.; Bittner, V.A.; Budaj, A.J.; Diaz, R.; Goodman, S.G.; Hanotin, C.; et al. Effects of alirocumab on cardiovascular and metabolic outcomes after acute coronary syndrome in patients with or without diabetes: A prespecified analysis of the ODYSSEY OUTCOMES randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 618–628. [Google Scholar] [CrossRef]
- Geldsetzer, P.; Manne-Goehler, J.; Marcus, M.E.; Ebert, C.; Zhumadilov, Z.; Wesseh, C.S.; Tsabedze, L.; Supiyev, A.; Sturua, L.; Bahendeka, S.K.; et al. The state of hypertension care in 44 low-income and middle-income countries: A cross-sectional study of nationally representative individual-level data from 1.1 million adults. Lancet 2019, 394, 652–662. [Google Scholar] [CrossRef]
- Maimoun, L.; Lefebvre, P.; Jaussent, A.; Fouillade, C.; Mariano-Goulart, D.; Nocca, D. Body composition changes in the first month after sleeve gastrectomy based on gender and anatomic site. Surg. Obes. Relat. Dis. 2017, 13, 780–787. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Smith, R.; Aulet, M.; Bensen, B.; Lichtman, S.; Wang, J.; Pierson, R.N., Jr. Appendicular skeletal muscle mass: Measurement by dual-photon absorptiometry. Am. J. Clin. Nutr. 1990, 52, 214–218. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- McLean, R.R.; Shardell, M.D.; Alley, D.E.; Cawthon, P.M.; Fragala, M.S.; Harris, T.B.; Kenny, A.M.; Peters, K.W.; Ferrucci, L.; Guralnik, J.M.; et al. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: The foundation for the National Institutes of Health (FNIH) sarcopenia project. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 576–583. [Google Scholar] [CrossRef]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip strength across the life course: Normative data from twelve British studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [PubMed]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Yung, Y.; Lamm, M.; Zhang, W. Causal Mediation Analysis with the CASUALMED Procedure. In SAS Global Forum 2018; SAS Institute Inc.: Cary, NC, USA, 2018. [Google Scholar]
- Valeri, L.; Vanderweele, T.J. Mediation analysis allowing for exposure-mediator interactions and causal interpretation: Theoretical assumptions and implementation with SAS and SPSS macros. Psychol. Methods 2013, 18, 137–150. [Google Scholar] [CrossRef]
- Bahat, G.; Kilic, C.; Ozkok, S.; Ozturk, S.; Karan, M.A. Associations of sarcopenic obesity versus sarcopenia alone with functionality. Clin. Nutr. 2021, 40, 2851–2859. [Google Scholar] [CrossRef]
- Otten, L.; Bosy-Westphal, A.; Ordemann, J.; Rothkegel, E.; Stobaus, N.; Elbelt, U.; Norman, K. Abdominal fat distribution differently affects muscle strength of the upper and lower extremities in women. Eur. J. Clin. Nutr. 2017, 71, 372–376. [Google Scholar] [CrossRef]
- Beriault, K.; Carpentier, A.C.; Gagnon, C.; Menard, J.; Baillargeon, J.P.; Ardilouze, J.L.; Langlois, M.F. Reproducibility of the 6-minute walk test in obese adults. Int. J. Sport. Med. 2009, 30, 725–727. [Google Scholar] [CrossRef]
- Donini, L.M.; Poggiogalle, E.; Mosca, V.; Pinto, A.; Brunani, A.; Capodaglio, P. Disability affects the 6-minute walking distance in obese subjects (BMI>40 kg/m2). PLoS ONE 2013, 8, e75491. [Google Scholar] [CrossRef]
- Kong, H.H.; Won, C.W.; Kim, W. Effect of sarcopenic obesity on deterioration of physical function in the elderly. Arch. Gerontol. Geriatr. 2020, 89, 104065. [Google Scholar] [CrossRef]
- Kera, T.; Kawai, H.; Hirano, H.; Kojima, M.; Fujiwara, Y.; Ihara, K.; Obuchi, S. Differences in body composition and physical function related to pure sarcopenia and sarcopenic obesity: A study of community-dwelling older adults in Japan. Geriatr. Gerontol. Int. 2017, 17, 2602–2609. [Google Scholar] [CrossRef]
- Keevil, V.L.; Luben, R.; Dalzell, N.; Hayat, S.; Sayer, A.A.; Wareham, N.J.; Khaw, K.T. Cross-sectional associations between different measures of obesity and muscle strength in men and women in a British cohort study. J. Nutr. Health Aging 2015, 19, 3–11. [Google Scholar] [CrossRef]
- Barrea, L.; de Alteriis, G.; Muscogiuri, G.; Vetrani, C.; Verde, L.; Camajani, E.; Aprano, S.; Colao, A.; Savastano, S. Impact of a Very Low-Calorie Ketogenic Diet (VLCKD) on Changes in Handgrip Strength in Women with Obesity. Nutrients 2022, 14, 4213. [Google Scholar] [CrossRef]
- Bouchard, D.R.; Dionne, I.J.; Brochu, M. Sarcopenic/obesity and physical capacity in older men and women: Data from the Nutrition as a Determinant of Successful Aging (NuAge)-the Quebec longitudinal Study. Obesity 2009, 17, 2082–2088. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.B.; Haggerty, C.L.; Goodpaster, B.; Harris, T.; Kritchevsky, S.; Nevitt, M.; Miles, T.P.; Visser, M.; Health, A.; Body Composition Research, G. Strength and muscle quality in a well-functioning cohort of older adults: The Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2003, 51, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Stobaus, N.; Kulka, K.; Schulzke, J. Effect of inflammation on handgrip strength in the non-critically ill is independent from age, gender and body composition. Eur. J. Clin. Nutr. 2014, 68, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Mei, F.; Shang, Y.; Hu, K.; Chen, F.; Zhao, L.; Ma, B. Global prevalence of sarcopenic obesity in older adults: A systematic review and meta-analysis. Clin. Nutr. 2021, 40, 4633–4641. [Google Scholar] [CrossRef]
- Scott, D.; Sanders, K.M.; Aitken, D.; Hayes, A.; Ebeling, P.R.; Jones, G. Sarcopenic obesity and dynapenic obesity: A 5 year associations woth fall risk in middle-aged and older adults. Obesity 2014, 22, 1568–1574. [Google Scholar] [CrossRef]
- Chang, C.I.; Huang, K.C.; Chan, D.C.; Wu, C.H.; Lin, C.C.; Hsiung, C.A.; Hsu, C.C.; Chen, C.Y. The impacts of sarcopenia and obesity on physical performance in the elderly. Obes. Res. Clin. Pract. 2015, 9, 256–265. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Lubrano, C.; Sergi, G.; Coin, A.; Gnessi, L.; Mariani, S.; Lenzi, A.; Donini, L.M. Sarcopenic Obesity and Metabolic Syndrome in Adult Caucasian Subjects. J. Nutr. Health Aging 2016, 20, 958–963. [Google Scholar] [CrossRef]
- Bogdanis, G.C. Effects of physical activity and inactivity on muscle fatigue. Front. Physiol. 2012, 3, 142. [Google Scholar] [CrossRef] [PubMed]
- El Ghoch, M.; Rossi, A.P.; Calugi, S.; Rubele, S.; Soave, F.; Zamboni, M.; Chignola, E.; Mazzali, G.; Bazzani, P.V.; Dalle Grave, R. Physical performance measures in screening for reduced lean body mass in adult females with obesity. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Bredella, M.A.; Ghomi, R.H.; Thomas, B.J.; Torriani, M.; Brick, D.J.; Gerweck, A.V.; Misra, M.; Klibanski, A.; Miller, K.K. Comparison of DXA and CT in the assessment of body composition in premenopausal women with obesity and anorexia nervosa. Obesity 2010, 18, 2227–2233. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Women with Obesity (Class of Age) | ||||
|---|---|---|---|---|
| ≤35 Yrs (n = 80) | 35–60 Yrs (n = 201) | >60 Yrs (n = 102) | p-Value | |
| Age, years | 26.4 ± 5.2 a | 48.5 ± 6.8 b | 66.6 ± 5.0 c | <0.01 |
| Clinical characteristics | ||||
| Weight, kg | 104.8 ± 16.6 a | 104.0± 15.8 a | 96.2 ± 13.5 b | <0.01 |
| Height, m | 163.4 ± 6.3 a | 162.7 ± 6.3 a | 160.1 ± 5.6 b | <0.01 |
| BMI, kg/m2 | 39.2 ± 5.8 a | 39.4 ± 6.0 b | 37.5 ± 4.5 a | 0.02 |
| Waist circumference, cm | 105.4 ± 12.3 a | 109.8 ± 12.2 b | 110.1 ± 11.6 b | 0.04 |
| Hip circumference, cm | 124.8 ± 11.9 b,c | 125.9 ± 12.8 a,c | 121.1 ± 11.5 b | 0.02 |
| Comorbidities | ||||
| HTA, n; % | 4 (5) a | 72 (35.8) b | 63 (61.8) c | <0.01 |
| Diabetes, n; % | 5 (6.3) a | 45 (22.4) b | 41 (40.2) c | <0.01 |
| Metabolism parameter | ||||
| REE, cal/24 h | 1802.3 ± 249.9 a | 1739.1 ± 288.3 a | 1622.5 ± 243.9 b | <0.01 |
| Women with Obesity (Class of Age) | ||||
|---|---|---|---|---|
| ≤35 Yrs (n = 80) | 35–60 Yrs (n = 201) | >60 Yrs (n = 102) | p-Value | |
| Body composition | ||||
| Fat mass | ||||
| Whole body, kg | 47.2 ± 6.9 | 46.8 ± 4.3 | 47.0 ± 6.2 | 0.725 |
| Whole body, % | 45.4 ± 5.6 | 45.1 ± 3.5 | 45.1 ± 5.1 | 0.800 |
| Trunk, kg | 21.9 ± 4.9 a | 23.1 ± 3.1 b | 23.9 ± 4.4 c | <0.001 |
| Upper limbs, kg | 5.8 ± 3.3 | 5.9 ± 2.1 | 6.4 ± 3.0 | 0.090 |
| Lower limbs, kg | 18.5 ± 5.2 a | 16.9 ± 3.3 b | 15.8 ± 4.7 c | <0.001 |
| Lean tissue mass | ||||
| Whole body, kg | 53.8 ± 7.2 | 53.9 ± 4.5 | 54.4 ± 6.5 | 0.630 |
| Trunk, kg | 27.0 ± 4.9 a | 28.1 ± 3.1 b | 28.9 ± 4.4 c | 0.0002 |
| Upper limbs, kg | 5.2 ± 1.2 | 5.3 ± 0.8 | 5.2 ± 1.2 | 0.720 |
| Lower limbs, kg | 18.4 ± 2.6 a | 17.6 ± 1.6 b | 17.3 ± 2.4 b | <0.0001 |
| Women with Obesity (Age Class) | ||||
|---|---|---|---|---|
| ≤35 Yrs (n = 80) | 35–60 Yrs (n = 201) | >60 Yrs (n = 102) | p-Value | |
| Low lean tissue mass | ||||
| ALM. kg | 24.24 ± 3.43 a | 23.27 ± 4.01 a | 21.24 ± 3.20 b | <0.01 |
| ALM < 15 kg (n, %) | 0 (0) | 1 (0.5) | 2 (2.0) | 0.49 |
| ALM < 18.51 kg (n, %) | 2 (2.5) a | 19 (9.5) a,b | 19 (18.6) b | <0.01 |
| ALMI(h2), kg/m2 | 9.07 ± 1.15 a | 8.78 ± 1.40 a | 8.27 ± 1.03 b | <0.01 |
| ALMI(h2) < 5.5 kg/m2 (n.%) | 0 (0) | 1 (0.5) | 0 (0) | 1 |
| ALMI(h2) < 5.67 kg/m2 (n.%) | 0 (0) | 1 (0.5) | 0 (0) | 1 |
| ALMI (h2) < 7.15 kg/m2 | 0 (0) a | 16 (8) b | 13 (12.8) b | <0.01 |
| ALMI(BMI) | 0.622 ± 0.083 a | 0.603 ± 0.076 b | 0.570 ± 0.074 c | <0.01 |
| ALMI(BMI) < 0.512 | 5 (6.3) a | 25 (12.4) a,b | 21 (20.6) b | 0.02 |
| ALMI(BMI) < 0.483 | 3 (3.8) | 8 (4.0) | 8(7.9) | 0.32 |
| Obesity index * | −0.26 ± 1.06 a | −0.68 ± 1.05 b | −0.93 ± 1.00 b | <0.01 |
| Obesity index * (<2DS) | 3 (3.8) | 17 (8.5) | 13 (12.8) | 0.1 |
| Physical performance | ||||
| 6-min walking test, m | 511.9 ± 76.9 a | 464.5 ± 93.1 b | 410.4 ± 105.0 c | <0.01 |
| Walking speed m/s | 1.42 ± 0.21 a | 1.29 ± 0.26 b | 1.14 ± 0.29 c | <0.01 |
| Walking speed < 0.83 m/s (n, %) | 1.0 (1.3) a | 11 (5.6) a,b | 13 (13.4) b | <0.01 |
| Grip test, kg | 24.9 ± 6.8 a | 23.7 ± 6.7 a | 20.3 ± 6.3 b | <0.01 |
| Grip test < 16 kg (n, %) | 6 (8) a | 15 (9.4) a | 18 (22.8) b | <0.01 |
| Grip Test | Gait Speed | |||
|---|---|---|---|---|
| Parameters | <16 kg (n = 39) | ≥16 kg (n = 275) | <0.83 m/s | ≥0.83 m/s |
| Age, years | 57.2 ± 14.8 | 46.6 ± 14.8 ** | 58.1 ± 11.4 | 48.0 ± 15.0 ** |
| BMI, kg/m2 | 37.1 ± 6.3 | 39.0 ± 5.4 * | 41.0 ± 7.1 | 39.0 ± 5.6 |
| WB FM, kg | 43.2 ± 9.7 | 47.5 ± 9.7 ** | 47.58 ± 10.9 | 47.1 ± 9.8 |
| Trunk FM, kg | 43.3 ± 4.1 | 44.2 ± 4.9 * | 23.7 ± 5.8 | 23.1 ± 5.4 |
| Arms FM, kg | 5.6 ± 1.8 | 6.0 ± 1.5 | 6.2 ± 1.7 | 6.0 ± 2.4 |
| Legs FM, kg | 16.3 ± 5.1 | 17.2 ± 4.7 | 16.7 ± 5.1 | 17.0 ± 4.8 |
| WB LTM, kg | 51.2 ± 7.2 | 54.9 ± 7.4 ** | 54.2 ± 8.4 | 54.2 ± 7.6 |
| Trunk LTM, kg | 26.6 ± 3.5 | 28.0 ± 3.9 * | 29.5 ± 9.2 | 28.1 ± 3.8 |
| Arms LTM, kg | 5.0 ± 0.9 | 5.3 ± 0.9 * | 5.3 ± 1.15.3 ± 3.3 | 5.3 ± 0.9 |
| Legs LTM, kg | 16.5 ± 3.2 | 18.0 ± 3.2 ** | 17.8 ± 3.4 | 17.8 ± 3.2 |
| ALM, kg | 21.5 ± 4.0 | 23.3 ± 3.8 ** | 22.6 ± 4.1 | 23.1 ± 3.8 |
| ALMI(h2), kg/m2 | 8.37 ± 1.41 | 8.76 ± 1.26 * | 8.9 ± 1.6 | 8.7 ± 1.3 |
| ALMI(BMI), | 0.580 ± 0.080 | 0.600 ± 0.080 | 0.560 ± 0.070 | 0.600 ± 0.080 * |
| 6-min walking test, m | 417.5 ± 108.4 | 474.5 ± 93.4 ** | 209.4 ± 67.3 | 478.6 ± 73.3 ** |
| Gait speed. m/s | 1.16 ± 0.30 | 1.32 ± 0.26 ** | 0.58 ± 0.19 | 1.33 ± 0.2 ** |
| Grip test, kg | 11.9 ± 3.05 | 24.7 ± 5.7 ** | 18.2 ± 5.3 | 23.5 ± 6.9 ** |
| REE, cal/24 h | 1582.3 ± 270.0 | 1743.8 ± 271.3 ** | 1745.5 ± 303.4 | 1724.8 ± 273.7 |
| Parameters | Age | BMI | Grip Strength | Gait Speed | ALM | ALMI(h2) | ALMI(BMI) | Obesity Index |
|---|---|---|---|---|---|---|---|---|
| Age | - | −0.113 * | −0.292 *** | −0.417 *** | −0.354 *** | −0.283 *** | −0.317 *** | −0.284 *** |
| BMI | - | 0.036 | −0.330 *** | 0.636 *** | 0.785 *** | −0.266 *** | −0.040 | |
| Grip strength | −0.292 *** | 0.036 | - | 0.369 *** | 0.297 *** | 0.183 ** | 0.339 *** | 0.234 *** |
| Walking distance | −0.417 *** | −0.330 *** | 0.369 *** | - | 0.029 | −0.094 | 0.398 *** | 0.259 *** |
| Whole body FM | −0.170 *** | 0.844 *** | 0.091 | −0.256 *** | 0.643 *** | 0.591 *** | −0.127 * | −0.181 *** |
| FM arms | −0.034 | 0.675 *** | 0.042 | −0.283 *** | 0.473 *** | 0.485 *** | −0.149 ** | −0.117 * |
| FM trunk | −0.009 | 0.769 *** | 0.035 | −0.347 *** | 0.505 *** | 0.467 *** | −0.199 *** | −0.277 *** |
| FM legs | −0.334 *** | 0.620 *** | 0.141 * | −0.052 | 0.576 *** | 0.508 *** | 0.013 | −0.029 |
| Whole body LTM | −0.219 *** | 0.643 *** | 0.245 *** | −0.053 | 0.903 *** | 0.754 *** | 0.402 *** | 0.361 *** |
| LTM arms | −0.196 *** | 0.442 *** | 0.244 *** | −0.032 | 0.738 *** | 0.650 *** | 0.441 *** | 0.473 *** |
| LTM trunk | −0.076 | 0.548 *** | 0.173 ** | −0.096 | 0.693 *** | 0.551 *** | 0.269 *** | 0.164 ** |
| LTM legs | −0.372 *** | 0.635 *** | 0.284 *** | 0.038 | 0.976 *** | 0.839 *** | 0.488 *** | 0.504 *** |
| REE | −0.325 *** | 0.544 *** | 0.189 *** | −0.036 | 0.688 *** | 0.579 *** | 0.275 *** | 0.235 *** |
| Muscle Strength | Gait Speed | |||||
|---|---|---|---|---|---|---|
| Effect (%) | SD | p-Value | Effect | SD | p-Value | |
| Proportion of the total effect of age mediated by whole-body LTM | 27.6 | 7.8 | 0.0004 | 20.7 | 5.2 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maïmoun, L.; Bourgeois, E.; Serrand, C.; Mura, T.; Cristol, J.-P.; Myzia, J.; Avignon, A.; Mariano-Goulart, D.; Sultan, A. Relationship between Lean Tissue Mass and Muscle Function in Women with Obesity. Nutrients 2023, 15, 4517. https://doi.org/10.3390/nu15214517
Maïmoun L, Bourgeois E, Serrand C, Mura T, Cristol J-P, Myzia J, Avignon A, Mariano-Goulart D, Sultan A. Relationship between Lean Tissue Mass and Muscle Function in Women with Obesity. Nutrients. 2023; 15(21):4517. https://doi.org/10.3390/nu15214517
Chicago/Turabian StyleMaïmoun, Laurent, Elise Bourgeois, Chris Serrand, Thibault Mura, Jean-Paul Cristol, Justine Myzia, Antoine Avignon, Denis Mariano-Goulart, and Ariane Sultan. 2023. "Relationship between Lean Tissue Mass and Muscle Function in Women with Obesity" Nutrients 15, no. 21: 4517. https://doi.org/10.3390/nu15214517
APA StyleMaïmoun, L., Bourgeois, E., Serrand, C., Mura, T., Cristol, J. -P., Myzia, J., Avignon, A., Mariano-Goulart, D., & Sultan, A. (2023). Relationship between Lean Tissue Mass and Muscle Function in Women with Obesity. Nutrients, 15(21), 4517. https://doi.org/10.3390/nu15214517