
Determinants of Diet Quality in Adolescents: Results from the Prospective Population-Based EVA-Tyrol and EVA4YOU Cohorts

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
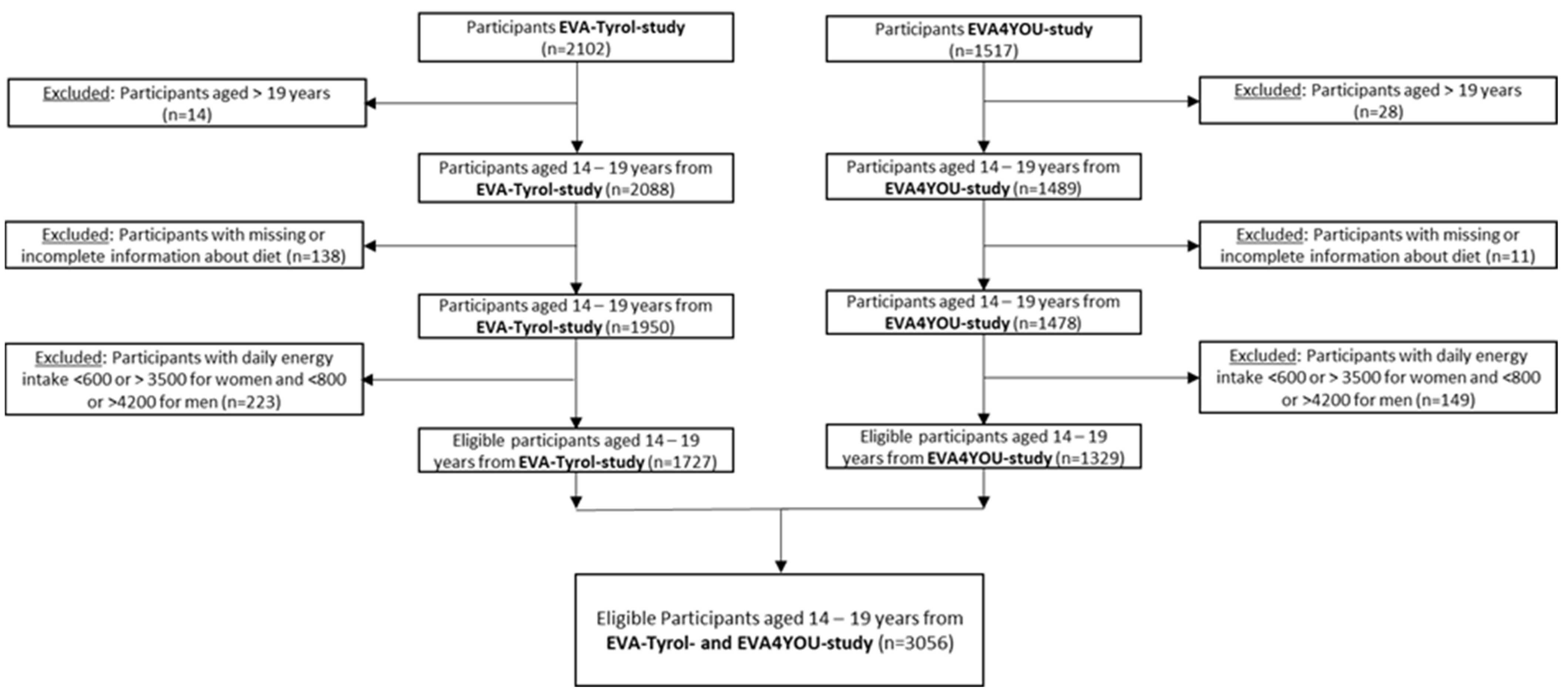
2.1. Study Population
2.2. Procedures and Assessments
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Distribution of Characteristics across Quartiles of the AHEI-2010 Score
3.3. Distribution of Characteristics across Quartiles of the DASH Score
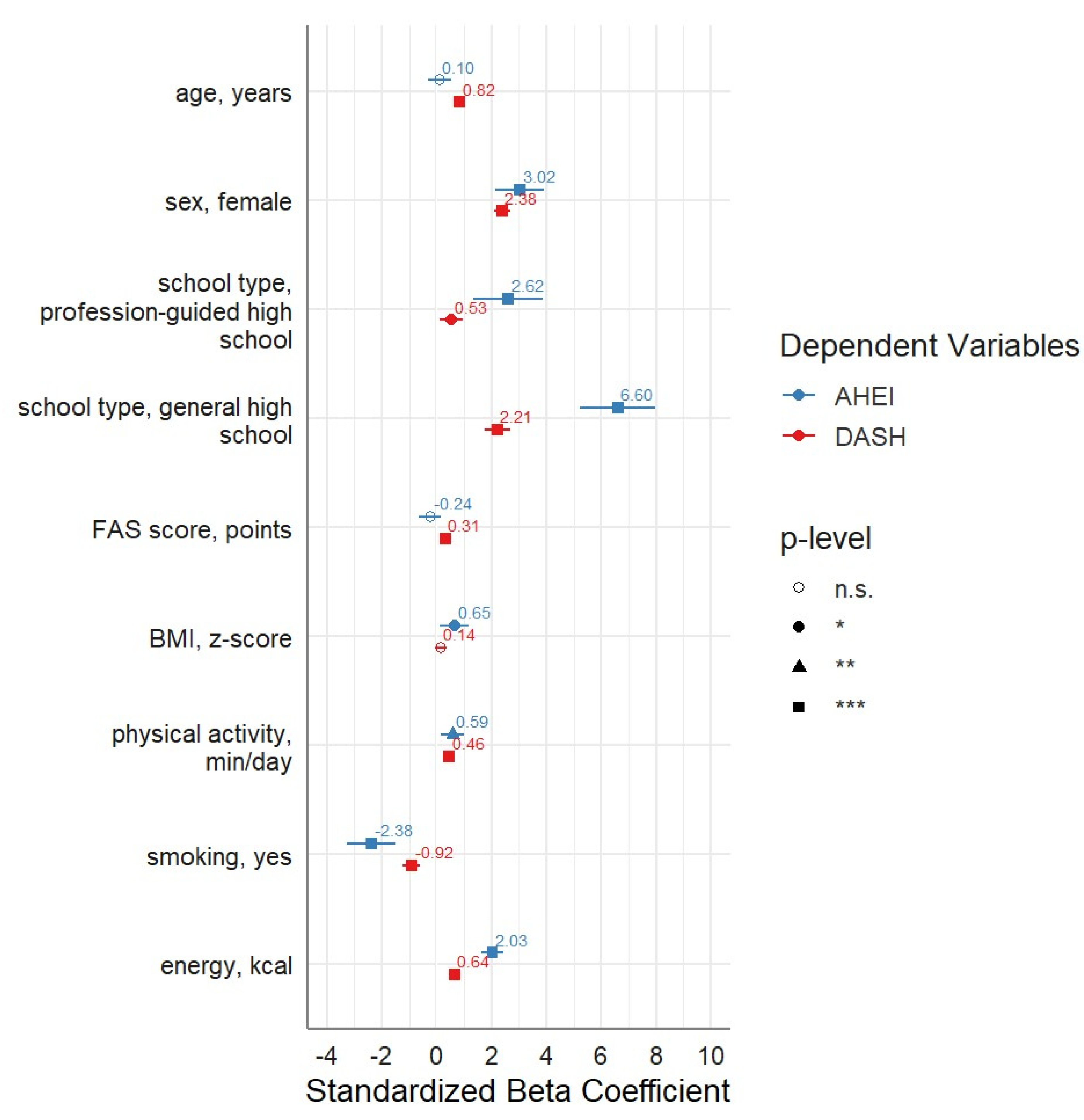
3.4. Association of Adolescent Factors and the Dietary Scores AHEI-2010 and DASH Score
3.5. Nutrition Knowledge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.; Malik, V.S.; Hu, F.B. Cardiovascular Disease Prevention by Diet Modification: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 914–926. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Peñalvo, J.L.; Cudhea, F.; Imamura, F.; Rehm, C.D.; Mozaffarian, D. Association Between Dietary Factors and Mortality From Heart Disease, Stroke, and Type 2 Diabetes in the United States. JAMA 2017, 317, 912–924. [Google Scholar] [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed]
- Montaño, Z.; Smith, J.D.; Dishion, T.J.; Shaw, D.S.; Wilson, M.N. Longitudinal relations between observed parenting behaviors and dietary quality of meals from ages 2 to 5. Appetite 2015, 87, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: A comprehensive review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- Zheng, Y.; Li, Y.; Satija, A.; Pan, A.; Sotos-Prieto, M.; Rimm, E.; Willett, W.C.; Hu, F.B. Association of changes in red meat consumption with total and cause specific mortality among US women and men: Two prospective cohort studies. BMJ 2019, 365, l2110. [Google Scholar] [CrossRef]
- Dehghan, M.; Mente, A.; Zhang, X.; Swaminathan, S.; Li, W.; Mohan, V.; Iqbal, R.; Kumar, R.; Wentzel-Viljoen, E.; Rosengren, A.; et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. Lancet 2017, 390, 2050–2062. [Google Scholar] [CrossRef]
- Fung, T.T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Akseer, N.; Mehta, S.; Wigle, J.; Chera, R.; Brickman, Z.J.; Al-Gashm, S.; Sorichetti, B.; Vandermorris, A.; Hipgrave, D.B.; Schwalbe, N.; et al. Non-communicable diseases among adolescents: Current status, determinants, interventions and policies. BMC Public Health 2020, 20, 1908. [Google Scholar] [CrossRef] [PubMed]
- Chatelan, A.; Lebacq, T.; Rouche, M.; Kelly, C.; Fismen, A.S.; Kalman, M.; Dzielska, A.; Castetbon, K. Long-term trends in the consumption of sugary and diet soft drinks among adolescents: A cross-national survey in 21 European countries. Eur. J. Nutr. 2022, 61, 2799–2813. [Google Scholar] [CrossRef] [PubMed]
- Makri, R.; Katsoulis, M.; Fotiou, A.; Kanavou, E.; Stavrou, M.; Richardson, C.; Kanellopoulou, A.; Orfanos, P.; Benetou, V.; Kokkevi, A. Prevalence of Overweight and Obesity and Associated Diet-Related Behaviours and Habits in a Representative Sample of Adolescents in Greece. Children 2022, 9, 119. [Google Scholar] [CrossRef] [PubMed]
- Rouche, M.; Lebacq, T.; Pedroni, C.; Holmberg, E.; Bellanger, A.; Desbouys, L.; Castetbon, K. Dietary disparities among adolescents according to individual and school socioeconomic status: A multilevel analysis. Int. J. Food Sci. Nutr. 2022, 73, 669–682. [Google Scholar] [CrossRef]
- Dong, Y.; Pollock, N.; Stallmann-Jorgensen, I.S.; Gutin, B.; Lan, L.; Chen, T.C.; Keeton, D.; Petty, K.; Holick, M.F.; Zhu, H. Low 25-hydroxyvitamin D levels in adolescents: Race, season, adiposity, physical activity, and fitness. Pediatrics 2010, 125, 1104–1111. [Google Scholar] [CrossRef]
- Zhang, Z.; Jackson, S.L.; Steele, E.M.; Gillespie, C.; Yang, Q. Relationship Between Ultraprocessed Food Intake and Cardiovascular Health Among U.S. Adolescents: Results From the National Health and Nutrition Examination Survey 2007–2018. J. Adolesc. Health 2022, 70, 249–257. [Google Scholar] [CrossRef]
- Uauy, R.; Solomons, N. Diet, nutrition, and the life-course approach to cancer prevention. J. Nutr. 2005, 135, 2934S–2945S. [Google Scholar] [CrossRef]
- Whincup, P.H.; Gilg, J.A.; Donald, A.E.; Katterhorn, M.; Oliver, C.; Cook, D.G.; Deanfield, J.E. Arterial distensibility in adolescents: The influence of adiposity, the metabolic syndrome, and classic risk factors. Circulation 2005, 112, 1789–1797. [Google Scholar] [CrossRef]
- Acar Tek, N.; Yildiran, H.; Akbulut, G.; Bilici, S.; Koksal, E.; Gezmen Karadag, M.; Sanlıer, N. Evaluation of dietary quality of adolescents using Healthy Eating Index. Nutr. Res. Pract. 2011, 5, 322–328. [Google Scholar] [CrossRef]
- Mayne, S.L.; Virudachalam, S.; Fiks, A.G. Clustering of unhealthy behaviors in a nationally representative sample of U.S. children and adolescents. Prev. Med. 2020, 130, 105892. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, S.; Jalaludin, M.Y.; Su, T.T.; Dahlui, M.; Azmi Mohamed, M.N.; Abdul Majid, H. Determinants of Diet and Physical Activity in Malaysian Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 603. [Google Scholar] [CrossRef] [PubMed]
- Gautam, N.; Dessie, G.; Rahman, M.M.; Khanam, R. Socioeconomic status and health behavior in children and adolescents: A systematic literature review. Front. Public Health 2023, 11, 1228632. [Google Scholar] [CrossRef] [PubMed]
- Rippin, H.L.; Hutchinson, J.; Jewell, J.; Breda, J.J.; Cade, J.E. Child and adolescent nutrient intakes from current national dietary surveys of European populations. Nutr. Res. Rev. 2019, 32, 38–69. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; Bel-Serrat, S.; Santaliestra-Pasías, A.; Bueno, G. Dairy products, yogurt consumption, and cardiometabolic risk in children and adolescents. Nutr. Rev. 2015, 73, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Arenaza, L.; Huybrechts, I.; Ortega, F.B.; Ruiz, J.R.; De Henauw, S.; Manios, Y.; Marcos, A.; Julián, C.; Widhalm, K.; Bueno, G.; et al. Adherence to the Mediterranean diet in metabolically healthy and unhealthy overweight and obese European adolescents: The HELENA study. Eur. J. Nutr. 2019, 58, 2615–2623. [Google Scholar] [CrossRef] [PubMed]
- Kozioł-Kozakowska, A.; Kozłowska, M.; Jagielski, P. Assessment of diet quality, nutrient intake, and dietary behaviours in obese children compared to healthy children. Pediatr. Endocrinol. Diabetes Metab. 2020, 26, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Bernar, B.; Gande, N.; Stock, K.A.; Staudt, A.; Pechlaner, R.; Geiger, R.; Griesmacher, A.; Kiechl, S.; Knoflach, M.; Kiechl-Kohlendorfer, U. for Early Vascular Aging (EVA) Study Group. The Tyrolean early vascular ageing-study (EVA-Tyrol): Study protocol for a non-randomized controlled trial: Effect of a cardiovascular health promotion program in youth, a prospective cohort study. BMC Cardiovasc. Disord. 2020, 20, 59. [Google Scholar] [CrossRef]
- Shan, Z.; Li, Y.; Baden, M.Y.; Bhupathiraju, S.N.; Wang, D.D.; Sun, Q.; Rexrode, K.M.; Rimm, E.B.; Qi, L.; Willett, W.C.; et al. Association Between Healthy Eating Patterns and Risk of Cardiovascular Disease. JAMA Intern. Med. 2020, 180, 1090–1100. [Google Scholar] [CrossRef]
- Shan, Z.; Wang, F.; Li, Y.; Baden, M.Y.; Bhupathiraju, S.N.; Wang, D.D.; Sun, Q.; Rexrode, K.M.; Rimm, E.B.; Qi, L.; et al. Healthy Eating Patterns and Risk of Total and Cause-Specific Mortality. JAMA Intern. Med. 2023, 183, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den body-mass-index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Monatsschr. Kinderheilk. 2001, 149, 807–818. [Google Scholar] [CrossRef]
- Hampl, S.E.; Hassink, S.G.; Skinner, A.C.; Armstrong, S.C.; Barlow, S.E.; Bolling, C.F.; Avila Edwards, K.C.; Eneli, I.; Hamre, R.; Joseph, M.M.; et al. Clinical practice guideline for the evaluation and treatment of children and adolescents with obesity. Pediatrics 2023, 151, e2022060640. [Google Scholar] [CrossRef] [PubMed]
- Daniels, S.R.; Pratt, C.A.; Hayman, L.L. Reduction of risk for cardiovascular disease in children and adolescents. Circulation 2011, 124, 1673–1686. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity Guidelines for Americans. Office of Disease Prevention & Health Promotion, US Department of Health and Human Services, October 2008. Available online: www.health.gov/paguidelines (accessed on 4 December 2023).
- Inchley, J.; Currie, D.; Budisavljevic, S.; Stevens, G.W.; Samdal, O. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. Int. Rep. 2020, 14–15. [Google Scholar]
- Boyce, W.; Torsheim, T.; Currie, C.; Zambon, A. The family affluence scale as a measure of National Wealth: Validation of an adolescent self-report measure. Soc. Indic. Res. 2006, 78, 473–487. [Google Scholar] [CrossRef]
- Kiechl, S.; Pechlaner, R.; Willeit, P.; Notdurfter, M.; Paulweber, B.; Willeit, K.; Werner, P.; Ruckenstuhl, C.; Iglseder, B.; Weger, S.; et al. Higher spermidine intake is linked to lower mortality: A prospective population-based study. Am. J. Clin. Nutr. 2018, 108, 371–380. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitive food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 24; 2011. Available online: https://fdc.nal.usda.gov/ (accessed on 11 September 2023).
- Onvani, S.; Haghighatdoost, F.; Surkan, P.J.; Larijani, B.; Azadbakht, L. Adherence to the Healthy Eating Index and Alternative Healthy Eating Index dietary patterns and mortality from all causes, cardiovascular disease and cancer: A meta-analysis of observational studies. J. Hum. Nutr. Diet 2017, 30, 216–226. [Google Scholar] [CrossRef]
- Kerley, C.P. Dietary patterns and components to prevent and treat heart failure: A comprehensive review of human studies. Nutr. Res. Rev. 2018, 32, 1–27. [Google Scholar] [CrossRef]
- Turconi, G.; Celsa, M.; Rezzani, C.; Biino, G.; Sartirana, M.A.; Roggi, C. Reliability of a dietary questionnaire on food habits, eating behaviour and nutritional knowledge of adolescents. Eur. J. Clin. Nutr. 2003, 57, 753–763. [Google Scholar] [CrossRef]
- Zheng, X.; Wang, H.; Wu, H. Association between diet quality scores and risk of overweight and obesity in children and adolescents. BMC Pediatr. 2023, 23, 169. [Google Scholar] [CrossRef] [PubMed]
- Ducharme-Smith, K.; Chambers, R.; Garcia-Larsen, V.; Larzelere, F.; Kenney, A.; Reid, R.; Nelson, L.; Richards, J.; Begay, M.; Barlow, A.; et al. Native Youth Participating in the Together on Diabetes 12-Month Home-Visiting Program Reported Improvements in Alternative Healthy Eating Index-2010 Diet Quality Domains Likely to Be Associated With Blood Pressure and Glycemic Control. J. Acad. Nutr. Diet 2021, 121, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Li, Y.; Afshin, A.; Springmann, M.; Mozaffarian, D.; Stampfer, M.J.; Hu, F.B.; Murray, C.J.L.; Willett, W.C. Global Improvement in Dietary Quality Could Lead to Substantial Reduction in Premature Death. J. Nutr. 2019, 149, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Bricarello, L.P.; de Almeida Alves, M.; Retondario, A.; de Moura Souza, A.; de Vasconcelos, F.A.G. DASH diet (Dietary Approaches to Stop Hypertension) and overweight/obesity in adolescents: The ERICA study. Clin. Nutr. ESPEN 2021, 42, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Mahdavi, A.; Mohammadi, H.; Bagherniya, M.; Foshati, S.; Clark, C.C.T.; Moafi, A.; Elyasi, M.; Rouhani, M.H. The effect of the Dietary Approaches to Stop Hypertension (DASH) diet on body composition, complete blood count, prothrombin time, inflammation and liver function in haemophilic adolescents. Br. J. Nutr. 2022, 128, 1771–1779. [Google Scholar] [CrossRef] [PubMed]
- Bricarello, L.P.; de Moura Souza, A.; de Almeida Alves, M.; Retondario, A.; Fernandes, R.; Santos de Moraes Trindade, E.B.; Zanette Ramos Zeni, L.A.; de Assis Guedes de Vasconcelos, F. Association between DASH diet (Dietary Approaches to Stop Hypertension) and hypertension in adolescents: A cross-sectional school-based study. Clin. Nutr. ESPEN 2020, 36, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Aljahdali, A.A.; Peterson, K.E.; Cantoral, A.; Ruiz-Narvaez, E.; Tellez-Rojo, M.M.; Kim, H.M.; Hébert, J.R.; Wirth, M.D.; Torres-Olascoaga, L.A.; Shivappa, N.; et al. Diet Quality Scores and Cardiometabolic Risk Factors in Mexican Children and Adolescents: A Longitudinal Analysis. Nutrients 2022, 14, 896. [Google Scholar] [CrossRef]
- Grosso, G.; Mistretta, A.; Turconi, G.; Cena, H.; Roggi, C.; Galvano, F. Nutrition knowledge and other determinants of food intake and lifestyle habits in children and young adolescents living in a rural area of Sicily, South Italy. Public Health Nutr. 2013, 16, 1827–1836. [Google Scholar] [CrossRef]
- Turconi, G.; Guarcello, M.; Maccarini, L.; Cignoli, F.; Setti, S.; Bazzano, R.; Roggi, C. Eating habits and behaviors, physical activity, nutritional and food safety knowledge and beliefs in an adolescent Italian population. J. Am. Coll. Nutr. 2008, 27, 31–43. [Google Scholar] [CrossRef]
- Yang, Q.; Zhang, Z.; Kuklina, E.V.; Fang, J.; Ayala, C.; Hong, Y.; Loustalot, F.; Dai, S.; Gunn, J.P.; Tian, N.; et al. Sodium intake and blood pressure among US children and adolescents. Pediatrics 2012, 130, 611–619. [Google Scholar] [CrossRef]
- Hasenegger, V.; Rust, P.; König, J.; Purtscher, A.E.; Erler, J.; Ekmekcioglu, C. Main Sources, Socio-Demographic and Anthropometric Correlates of Salt Intake in Austria. Nutrients 2018, 10, 311. [Google Scholar] [CrossRef] [PubMed]
- Kwong, E.J.L.; Whiting, S.; Bunge, A.C.; Leven, Y.; Breda, J.; Rakovac, I.; Cappuccio, F.P.; Wickramasinghe, K. Population-level salt intake in the WHO European Region in 2022: A systematic review. Public Health Nutr. 2022, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.M.; Karim, M.N.; Hébert, J.R.; Shivappa, N.; de Courten, B. Association between Diet Quality Indices and Incidence of Type 2 Diabetes in the Melbourne Collaborative Cohort Study. Nutrients 2021, 13, 4162. [Google Scholar] [CrossRef] [PubMed]
- Patel, Y.R.; Robbins, J.M.; Gaziano, J.M.; Djoussé, L. Mediterranean, DASH, and Alternate Healthy Eating Index Dietary Patterns and Risk of Death in the Physicians’ Health Study. Nutrients 2021, 13, 1893. [Google Scholar] [CrossRef] [PubMed]
- Pinto, V.; Landaeta-Díaz, L.; Castillo, O.; Villarroel, L.; Rigotti, A.; Echeverría, G.; Study Group, E. Assessment of Diet Quality in Chilean Urban Population through the Alternate Healthy Eating Index 2010: A Cross-Sectional Study. Nutrients 2019, 11, 891. [Google Scholar] [CrossRef] [PubMed]
- Fallaize, R.; Livingstone, K.M.; Celis-Morales, C.; Macready, A.L.; San-Cristobal, R.; Navas-Carretero, S.; Marsaux, C.F.M.; O’Donovan, C.B.; Kolossa, S.; Moschonis, G.; et al. Association between Diet-Quality Scores, Adiposity, Total Cholesterol and Markers of Nutritional Status in European Adults: Findings from the Food4Me Study. Nutrients 2018, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Krølner, R.; Rasmussen, M.; Brug, J.; Klepp, K.I.; Wind, M.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part II: Qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 112. [Google Scholar] [CrossRef]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef]
- Ottevaere, C.; Huybrechts, I.; Benser, J.; De Bourdeaudhuij, I.; Cuenca-Garcia, M.; Dallongeville, J.; Zaccaria, M.; Gottrand, F.; Kersting, M.; Rey-López, J.P.; et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: The HELENA study. BMC Public Health 2011, 11, 328. [Google Scholar] [CrossRef]
- Bibiloni, M.D.M.; Gallardo-Alfaro, L.; Gómez, S.F.; Wärnberg, J.; Osés-Recalde, M.; González-Gross, M.; Gusi, N.; Aznar, S.; Marín-Cascales, E.; González-Valeiro, M.A.; et al. Determinants of Adherence to the Mediterranean Diet in Spanish Children and Adolescents: The PASOS Study. Nutrients 2022, 14, 738. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Jewell, J.; Breda, J.; Barnekow, V. Adolescent obesity and related behaviours: Trends and inequalities in the WHO European Region, 2002–2014. In Observations from the Health Behaviour in School-Aged Children (HBSC) WHO Collaborative Cross-National Study; WHO Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- Winpenny, E.M.; Greenslade, S.; Corder, K.; van Sluijs, E.M.F. Diet Quality through Adolescence and Early Adulthood: Cross-Sectional Associations of the Dietary Approaches to Stop Hypertension Diet Index and Component Food Groups with Age. Nutrients 2018, 10, 1585. [Google Scholar] [CrossRef] [PubMed]
- Winpenny, E.M.; van Sluijs, E.M.F.; White, M.; Klepp, K.I.; Wold, B.; Lien, N. Changes in diet through adolescence and early adulthood: Longitudinal trajectories and association with key life transitions. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 86. [Google Scholar] [CrossRef] [PubMed]
- French, S.A.; Tangney, C.C.; Crane, M.M.; Wang, Y.; Appelhans, B.M. Nutrition quality of food purchases varies by household income: The SHoPPER study. BMC Public Health 2019, 19, 231. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.A.; Keil, J.E. Socioeconomic factors and cardiovascular disease: A review of the literature. Circulation 1993, 88, 1973–1998. [Google Scholar] [CrossRef] [PubMed]
- Salam, R.A.; Hooda, M.; Das, J.K.; Arshad, A.; Lassi, Z.S.; Middleton, P.; Bhutta, Z.A. Interventions to Improve Adolescent Nutrition: A Systematic Review and Meta-Analysis. J. Adolesc. Health 2016, 59, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Kesten, J.M.; Griffiths, P.L.; Cameron, N. A systematic review to determine the effectiveness of interventions designed to prevent overweight and obesity in pre-adolescent girls. Obes. Rev. 2011, 12, 997–1021. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Moin, A.; Das, J.K.; Salam, R.A.; Bhutta, Z.A. Systematic review on evidence-based adolescent nutrition interventions. Ann. N. Y. Acad. Sci. 2017, 1393, 34–50. [Google Scholar] [CrossRef] [PubMed]
- Lister, N.B.; Baur, L.A.; Felix, J.F.; Hill, A.J.; Marcus, C.; Reinehr, T.; Summerbell, C.; Wabitsch, M. Child and adolescent obesity. Nat. Rev. Dis. Prim. 2023, 9, 24. [Google Scholar] [CrossRef]
- Hargreaves, D.; Mates, E.; Menon, P.; Alderman, H.; Devakumar, D.; Fawzi, W.; Greenfield, G.; Hammoudeh, W.; He, S.; Lahiri, A.; et al. Strategies and interventions for healthy adolescent growth, nutrition, and development. Lancet 2022, 399, 198–210. [Google Scholar] [CrossRef]
- Hoelscher, D.M.; Evans, A.; Parcel, G.S.; Kelder, S.H. Designing effective nutrition interventions for adolescents. J. Am. Diet Assoc. 2002, 102, 52–63. [Google Scholar] [CrossRef]
- Dimitratos, S.M.; Swartz, J.R.; Laugero, K.D. Pathways of parental influence on adolescent diet and obesity: A psychological stress-focused perspective. Nutr. Rev. 2022, 80, 1800–1810. [Google Scholar] [CrossRef] [PubMed]
- Pirouznia, M. The association between nutrition knowledge and eating behaviour in male and female adolescents in the US. Int. J. Food Sci. Nutr. 2001, 52, 127–132. [Google Scholar] [CrossRef]
- Pirouznia, M. The correlation between nutrition knowledge and eating behaviour in an American school: The role of ethnicity. Nutr. Health 2000, 14, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Sichert-Hellert, W.; Beghin, L.; De Henauw, S.; Grammatikaki, E.; Hallström, L.; Manios, Y.; Mesana, M.I.; Molnár, D.; Dietrich, S.; Piccinelli, R.; et al. Nutritional knowledge in European adolescents: Results from the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Public Health Nutr. 2011, 14, 2083–2091. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Pan, H.; Cao, H.; Zhao, S.; Yao, P. Reliability and validity of a semi-quantitative food frequency questionnaire: Dietary intake assessment among multi-ethnic populations in Northwest China. J. Health Popul. Nutr. 2023, 2, 111. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.K.; Bilek, L.D.; Waltman, N.L.; Ma, J.; Hébert, J.R.; Price, S.; Graeff-Armas, L.; Poole, J.A.; Mack, L.R.; Hans, D.; et al. Dietary Inflammatory Potential and Bone Outcomes in Midwestern Post-Menopausal Women. Nutrients 2023, 15, 4277. [Google Scholar] [CrossRef]
- Bernstein, A.M.; Pan, A.; Rexrode, K.M.; Stampfer, M.; Hu, F.B.; Mozaffarian, D.; Willett, W.C. Dietary protein sources and the risk of stroke in men and women. Stroke 2012, 43, 637–644. [Google Scholar] [CrossRef]
- Ahmadijoo, P.; Eftekhari, M.H.; Masoumi, S.J.; Zahedani, M.R.; Mohammadi, F. The possible relationship between the healthy eating index-2015 and the 10-year risk of cardiovascular diseases. BMC Nutr. 2023, 9, 76. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Total Sample (n = 3056) | EVA4YOU (n = 1329) | EVA-Tyrol (n = 1727) | p |
|---|---|---|---|---|
| Age, years, mean ± SD | 16.8 ± 1.3 | 17.2 ± 1.3 | 16.5 ± 1.2 | <0.001 * |
| Sex, n (%) | <0.001 *** | |||
| male | 1205 (39.4) | 468 (35.2) | 737 (42.7) | |
| female | 1851 (60.6) | 861 (64.8) | 990 (57.3) | |
| Schooltype, n (%) | <0.001 *** | |||
| Vocational school | 437 (14.3) | 264 (19.9) | 173 (10.0) | |
| Profession-guided high school | 1667 (54.5) | 678 (51.0) | 989 (57.3) | |
| General high school | 952 (31.2) | 387 (29.1) | 565 (32.7) | |
| FAS(II) Scale, n (%) a | <0.001 *** | |||
| Low | 18 (0.6) | 4 (0.3) | 14 (0.8) | |
| Medium | 821 (26.9) | 262 (19.7) | 559 (32.4) | |
| High | 2192 (71.7) | 1063 (80.0) | 1129 (66.3) | |
| BMI, kg/m2, mean ± SD | 22.06 ± 3.63 | 22.29 ± 3.77 | 21.89 ± 3.51 | 0.003 * |
| BMI Z-score, mean ± SD | 0.11 ± 1.04 | −0.05 ± 1.04 | 0.22 ± 1.02 | <0.001 * |
| Weight Group, n (%) b | <0.001 *** | |||
| Underweight | 133 (4.4) | 84 (6.3) | 49 (2.8) | |
| Normal | 2347 (76.8) | 1039 (78.2) | 1308 (75.7) | |
| Overweight | 347 (11.4) | 148 (11.1) | 199 (11.5) | |
| Obesity | 229 (7.5) | 58 (4.4) | 171 (9.9) | |
| Physical activity, min/d, M (Q1, Q3) | 45 (30, 75) | 55 (30, 80) | 45 (25, 60) | <0.001 ** |
| Total Energy, kcal/d, M (Q1, Q3) | 1975 (1483, 2542) | 2014 (1548, 2586) | 1941 (1439, 2517) | 0.004 ** |
| Never-smoker, n (%) | 2059 (67.4) | 843 (63.4) | 1216 (70.4) | <0.001 *** |
| AHEI-2010 score, M (Q1, Q3) | 42 (34, 50) | 39 (32, 47) | 44 (36, 52) | <0.001 ** |
| DASH score, M (Q1, Q3) | 18 (15, 21) | 19 (17, 22) | 17 (14, 20) | <0.001 ** |
| Quartiles of AHEI-2010 Score | |||||
|---|---|---|---|---|---|
| Characteristics | Q1 (n = 805) | Q2 (n = 777) | Q3 (n = 745) | Q4 (n = 729) | p |
| AHEI-2010 score, M (Q1, Q3) Possible Range of 0–100 | 29 (25, 32) | 39 (36, 40) | 46 (44, 48) | 57 (53, 61) | <0.001 * |
| Age, years, mean ± SD | 16.9 ± 1.3 | 16.8 ± 1.3 | 16.7 ± 1.3 | 16.8 ± 1.3 | 0.200 * |
| Female, n (%) | 461 (57.3) | 445 (57.3) | 449 (60.3) | 496 (68.0) | <0.001 ** |
| Schoolt ype, n (%) | <0.001 ** | ||||
| Vocational school | 171 (21.2) | 102 (13.1) | 96 (12.9) | 68 (9.3) | |
| Profession-guided high school | 468 (58.2) | 438 (56.4) | 423 (56.8) | 338 (46.4) | |
| General high school | 166 (20.6) | 237 (30.5) | 226 (30.3) | 323 (44.3) | |
| FAS(II) Score, Points, M (Q1, Q3) | 6 (5, 7) | 6 (6, 8) | 6 (5, 8) | 6 (5, 8) | 0.357 * |
| BMI Z-score, M (Q1, Q3) | 0.03 (−0.64, 0.74) | 0.14 (−0.60, 0,77) | 0.11 (−0.60, 0.84) | 0.12 (−0.54, 0.80) | 0.192 * |
| Physical activity, min/d, M (Q1, Q3) | 45 (25, 70) | 45 (30, 75) | 45 (30, 70) | 60 (30, 80) | 0.435 * |
| Never-smoker, n (%) | 491 (61.0) | 532 (68.5) | 513 (68.9) | 523 (71.7) | <0.001 ** |
| Total energy, kcal/d, M (Q1, Q3) | 1857 (1401, 2330) | 1909 (1466, 2423) | 2070 (1526, 2653) | 2141 (1613, 2762) | <0.001 * |
| Components of AHEI-2010, M (Q1, Q3) | |||||
| Fruits a, servings/d | 1.22 (0.70, 1.91) | 1.65 (1.05, 2.56) | 2.49 (1.56, 3.71) | 3.52 (2.21, 5.11) | <0.001 * |
| Vegetables b, servings/d | 1.29 (0.71, 1.94) | 1.91 (1.27, 2.64) | 2.47 (1.76, 3.43) | 3.56 (2.41, 4.99) | <0.001 * |
| Whole grain, g/d | 23.65 (3.63, 55.00) | 27.5 (7.70, 55.00) | 43.45 (15.12, 55.00) | 43.45 (23.65, 55.00) | <0.001 * |
| Red and processed meat intake c, servings/d | 3.05 (1.81, 5.19) | 2.62 (1.39, 4.84) | 1.90 (0.69, 3.61) | 0.89 (0.26, 2.40) | <0.001 * |
| Nuts and legumes d, servings/d | 0.14 (0.07, 0.35) | 0.35 (0.14, 0.71) | 0.64 (0.29, 1.12) | 1.20 (0.72, 1.97) | <0.001 * |
| Long-chain (ω-3) fats (EPA + DHA), mg/d | 0 (0, 40) | 90 (0, 790) | 130 (2, 830) | 640 (90, 920) | <0.001 * |
| Polyunsaturated fatty acids, % of energy | 2.35 (1.70, 4.44) | 3.01 (1.82, 4.85) | 3.72 (2.01, 5.13) | 4.27 (2.33, 5.48) | <0.001 * |
| Trans fat, % of energy | 0.67 (0.58, 0.78) | 0.64 (0.54, 0.74) | 0.60 (0.50, 0.69) | 0.51 (0.42, 0.63) | <0.001 * |
| SSBs and fruit juice e, servings/d | 1.20 (0.62, 2.11) | 0.88 (0.42, 1.82) | 0.84 (0.42, 1.64) | 0.42 (0.14, 0.91) | <0.001 * |
| Sodium intake, mg/d | 5920 (4420, 7835) | 5540 (3980, 7820) | 5480 (3585, 7705) | 4800 (3220, 6740) | <0.001 * |
| Quartiles of DASH Score | |||||
|---|---|---|---|---|---|
| Characteristics | Q1 (n = 819) | Q2 (n = 851) | Q3 (n = 722) | Q4 (n = 664) | p |
| DASH score, M (Q1, Q3) Possible Range of 8–40 | 14 (12, 15) | 17 (16, 18) | 20 (19, 21) | 24 (22, 26) | <0.001 * |
| Age, years, mean ± SD | 16.5 ± 1.3 | 16.8 ± 1.3 | 16.9 ± 1.3 | 17.0 ± 1.3 | <0.001 * |
| Female, n (%) | 374 (45.3) | 503 (59.1) | 476 (66.2) | 498 (75.3) | <0.001 ** |
| School type, n (%) | <0.001 ** | ||||
| Vocational school | 154 (18.8) | 131 (15.4) | 83 (11.5) | 69 (10.4) | |
| Profession-guided high school | 510 (62.3) | 483 (56.8) | 386 (53.5) | 288 (43.4) | |
| General high school | 155 (18.9) | 237 (27.8) | 253 (35.0) | 307 (46.2) | |
| FAS(II) Score, Points, M (Q1, Q3) | 6 (5, 7) | 6 (5, 8) | 7 (5, 8) | 7 (6, 8) | <0.001 * |
| BMI Z-score, M (Q1, Q3) | 0.10 (−0.59, 0.78) | 0.12 (−0.58, 0.81) | 0.08 (−0.63, 0.82) | 0.09 (−0.57, 0.78) | 0.174 * |
| Physical activity, min/d, M (Q1, Q3) | 45 (25, 75) | 45 (30, 70) | 50 (30, 75) | 60 (30, 80) | <0.001 * |
| Never-smoker, n (%) | 522 (63.7) | 566 (66.5) | 499 (69.1) | 472 (71.1) | 0.016 |
| Total energy, kcal/d, M (Q1, Q3) | 1921 (1421, 2488) | 1898 (1464, 2407) | 1986 (1463, 2571) | 2163 (1631, 2682) | <0.001 * |
| Components of DASH score, M (Q1, Q3) | |||||
| Fruit and fruit juice a, servings/d | 1.35 (0.77, 2.00) | 1.91 (1.19, 3.07) | 2.70 (1.63, 4.09) | 3.70 (2.43, 5.59) | <0.001 * |
| Vegetables and vegetable juice b, servings/d | 1.35 (0.78, 2.00) | 1.91 (1.26, 2.64) | 2.51 (1.64, 3.48) | 3.73 (2.56, 5.00) | <0.001 * |
| Nuts and legumes c, servings/d | 0.25 (0.12, 0.58) | 0.35 (0.14, 0.72) | 0.45 (0.21, 0.95) | 0.85 (0.43, 1.57) | <0.001 * |
| Whole grain d, servings/d | 0.43 (0.14, 0.79) | 0.43 (0.14, 1.00) | 0.79 (0.43, 1.00) | 1.00 (0.43, 1.75) | <0.001 * |
| Low-fat dairy products e, servings/d | 0 (0, 0) | 0 (0, 0) | 0 (0, 0.07) | 0 (0, 0.10) | <0.001 * |
| Sodium intake, mg/d | 6170 (4455, 8480) | 5510 (4050, 7630) | 5230 (3510, 7330) | 4770 (3300, 6550) | <0.001 * |
| Red and processed meat intake f, servings/d | 1.93 (1.2, 2.87) | 1.18 (0.68, 2.14) | 0.85 (0.42, 1.57) | 0.46 (0.14, 0.97) | <0.001 * |
| SSBs g, servings/d | 1.44 (0.56, 2.94) | 0.69 (0.26, 1.72) | 0.33 (0.04, 1.12) | 0.14 (0, 0.56) | <0.001 * |
| AHEI-2010 Score | DASH Score | |||||
|---|---|---|---|---|---|---|
| Regression Coefficient (95% CI) | R2 | p | Regression Coefficient (95% CI) | R2 | p | |
| Age, years * | −0.250 (−0.570–0.071) | 0.001 | 0.126 | 0.524 (0.410–0.638) | 0.026 | <0.001 |
| Sex, female * | 2.292 (1.44–3.139) | 0.009 | <0.001 | 1.982 (1.683–2.281) | 0.052 | <0.001 |
| School type ** | ||||||
| Profession-guided high school | −2.124 (−2.954–−1.293) | 0.018 | <0.001 | −1.098 (−1.385–−0.810) | 0.096 | <0.001 |
| General high school | 4.575 (3.689–5.460) | 0.042 | <0.001 | 1.896 (1.590–2.202) | 0.122 | <0.001 |
| FAS(II) Score, Points | 0.226 (−0.044–0.496) | 0.011 | 0.101 | 0.326 (0.233–0.419) | 0.094 | <0.001 |
| BMI Z-score | 0.331 (−0.069–0.731) | 0.011 | 0.105 | −0.067 (−0.207–0.072) | 0.080 | 0.343 |
| Physical activity, min/d | 0.010 (0.002–0.018) | 0.012 | 0.012 | 0.008 (0.006–0.011) | 0.092 | <0.001 |
| Smoking, never | 2.582 (1.680–3.484) | 0.020 | <0.001 | 1.013 (0.699–1.326) | 0.091 | <0.001 |
| Total energy, kcal/d | 0.003 (0.002–0.003) | 0.038 | <0.001 | 0.001 (0.001–0.001) | 0.107 | <0.001 |
| Nutrition Knowledge Score | ||||
|---|---|---|---|---|
| Variable | Section E Possible Range: 5–20 | p * | Section H Possible Range: 0–11 | p * |
| Sex | 0.034 | 0.483 | ||
| Male | 12 ± 2 | 6 ± 2 | ||
| Female | 12 ± 1 | 6 ± 2 | ||
| Schooltype | <0.001 | <0.001 | ||
| Vocational school | 11 ± 2 | 5 ± 2 | ||
| Profession-guided high school | 12 ± 1 | 6 ± 2 | ||
| General high school | 12 ± 1 | 7 ± 2 | ||
| FAS(II) Scale a, | 0.276 | 0.628 | ||
| Low | 11 ± 2 | 6 ± 2 | ||
| Medium | 12 ± 2 | 6 ± 2 | ||
| High | 12 ± 1 | 6 ± 2 | ||
| Weight Group b | 0.34 | 0.615 | ||
| Underweight | 12 ± 2 | 6 ± 2 | ||
| Normal | 12 ± 2 | 6 ± 2 | ||
| Overweight | 12 ± 2 | 7 ± 2 | ||
| Obesity | 12 ± 2 | 7 ± 2 | ||
| AHEI-2010 score Quartiles | 0.225 | 0.003 | ||
| Quartile 1 | 12 ± 1 | 6 ± 2 | ||
| Quartile 2 | 12 ± 2 | 6 ± 2 | ||
| Quartile 3 | 12 ± 1 | 6 ± 2 | ||
| Quartile 4 | 12 ± 2 | 7 ± 2 | ||
| DASH score Quartiles | 0.412 | <0.001 | ||
| Quartile 1 | 12 ± 2 | 6 ± 2 | ||
| Quartile 2 | 12 ± 1 | 6 ± 2 | ||
| Quartile 3 | 12 ± 1 | 7 ± 2 | ||
| Quartile 4 | 12 ± 2 | 7 ± 2 | ||
| Section E | Section H | |||||
|---|---|---|---|---|---|---|
| Standardized Beta Coefficient | R2 | p | Standardized Beta Coefficient | R2 | p | |
| Age, years * | 0.041 | 0.002 | 0.107 | 0.255 | 0.065 | <0.001 |
| Sex, female * | 0.021 | 0.000 | 0.423 | −0.011 | 0.000 | 0.664 |
| School type ** | ||||||
| Profession-guided high school | 0.001 | 0.002 | 0.966 | −0.095 | 0.074 | <0.001 |
| General high school | 0.071 | 0.007 | 0.006 | 0.187 | 0.099 | <0.001 |
| FAS(II) Scale | 0.049 | 0.005 | 0.061 | 0.085 | 0.074 | <0.001 |
| BMI Z-score | −0.064 | 0.006 | 0.014 | 0.016 | 0.064 | 0.540 |
| Physical activity, min/d | −0.018 | 0.003 | 0.493 | −0.012 | 0.066 | 0.638 |
| Smoking, never | 0.075 | 0.008 | 0.005 | 0.101 | 0.075 | <0.001 |
| AHEI-2010 score | 0.000 | 0.002 | 0.990 | 0.166 | 0.092 | <0.001 |
| DASH score | 0.003 | 0.002 | 0.908 | 0.181 | 0.095 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mueller, K.; Messner, A.; Nairz, J.; Winder, B.; Staudt, A.; Stock, K.; Gande, N.; Hochmayr, C.; Bernar, B.; Pechlaner, R.; et al. Determinants of Diet Quality in Adolescents: Results from the Prospective Population-Based EVA-Tyrol and EVA4YOU Cohorts. Nutrients 2023, 15, 5140. https://doi.org/10.3390/nu15245140
Mueller K, Messner A, Nairz J, Winder B, Staudt A, Stock K, Gande N, Hochmayr C, Bernar B, Pechlaner R, et al. Determinants of Diet Quality in Adolescents: Results from the Prospective Population-Based EVA-Tyrol and EVA4YOU Cohorts. Nutrients. 2023; 15(24):5140. https://doi.org/10.3390/nu15245140
Chicago/Turabian StyleMueller, Katharina, Alex Messner, Johannes Nairz, Bernhard Winder, Anna Staudt, Katharina Stock, Nina Gande, Christoph Hochmayr, Benoît Bernar, Raimund Pechlaner, and et al. 2023. "Determinants of Diet Quality in Adolescents: Results from the Prospective Population-Based EVA-Tyrol and EVA4YOU Cohorts" Nutrients 15, no. 24: 5140. https://doi.org/10.3390/nu15245140
APA StyleMueller, K., Messner, A., Nairz, J., Winder, B., Staudt, A., Stock, K., Gande, N., Hochmayr, C., Bernar, B., Pechlaner, R., Griesmacher, A., Egger, A. E., Geiger, R., Kiechl-Kohlendorfer, U., Knoflach, M., Kiechl, S. J., & on behalf of the EVA-Tyrol and EVA4YOU Study Groups. (2023). Determinants of Diet Quality in Adolescents: Results from the Prospective Population-Based EVA-Tyrol and EVA4YOU Cohorts. Nutrients, 15(24), 5140. https://doi.org/10.3390/nu15245140