
Sex Differences in Effects of Mood, Eating-Related Behaviors, and BMI on Food Appeal and Desire to Eat: A Cross-Sectional Survey Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Study Design
2.3. Questionnaires
2.4. Food Pictures Task
2.5. Statistical Analyses
3. Results
3.1. Sex-Based Group Differences
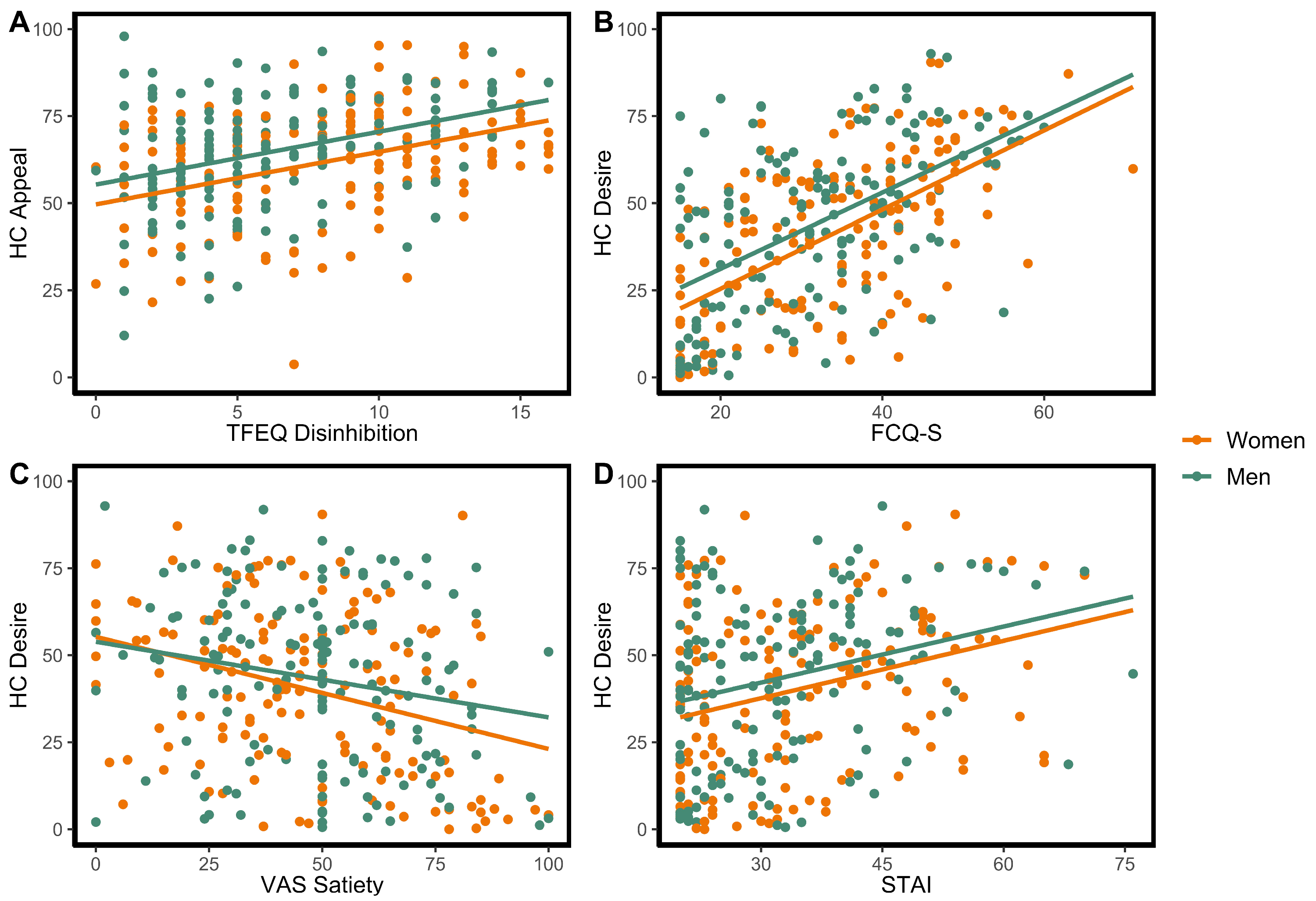
3.2. High-Calorie Food Ratings
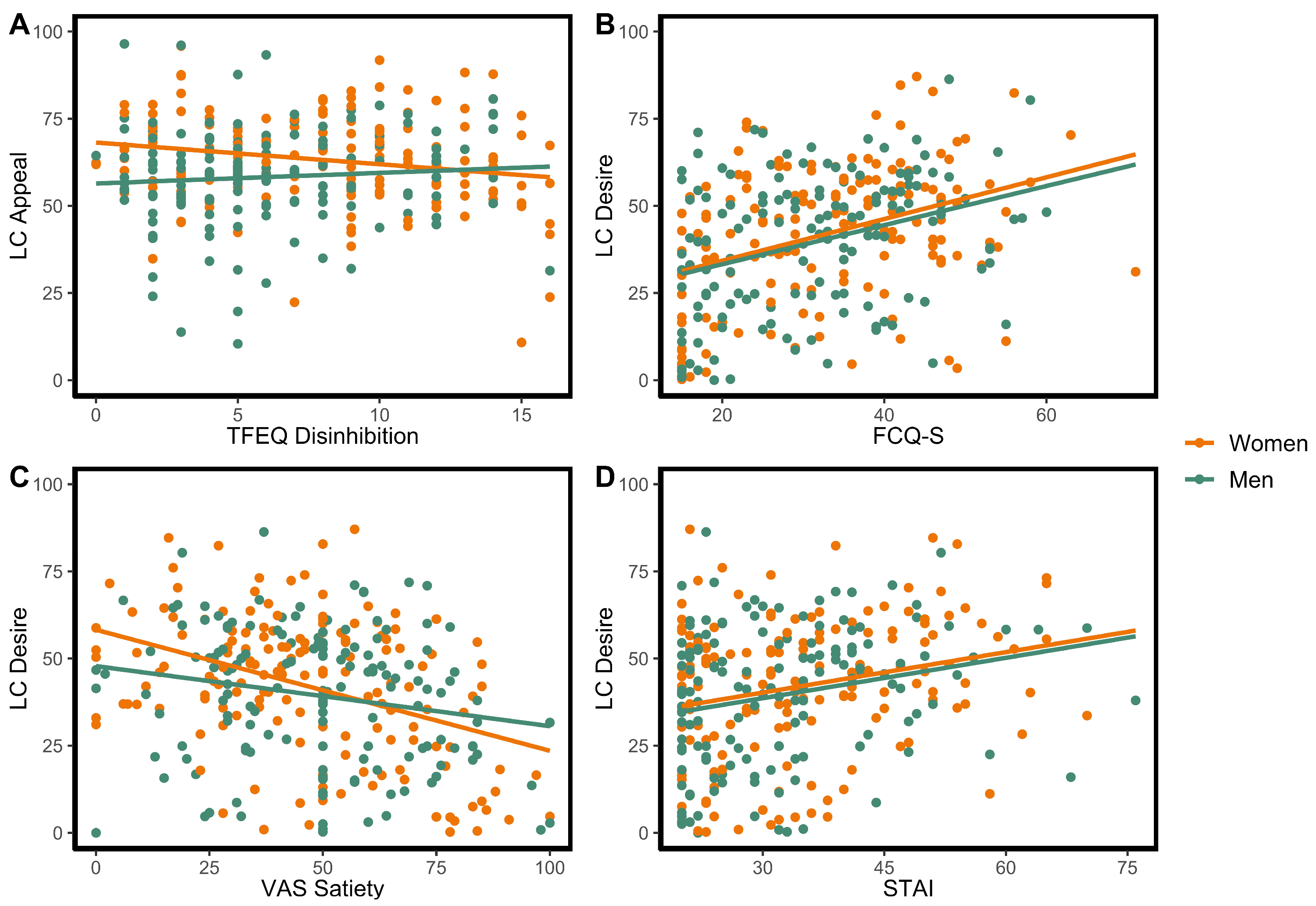
3.3. Low-Calorie Food Ratings
3.4. High-Calorie vs. Low-Calorie Food Rating Differences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Sturm, R.; Ringel, J.S.; Andreyeva, T. Increasing obesity rates and disability trends. Health Aff. 2004, 23, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Sturm, R.; Hattori, A. Morbid obesity rates continue to rise rapidly in the United States. Int. J. Obes. 2013, 37, 889–891. [Google Scholar] [CrossRef]
- Dixon, J.B. The effect of obesity on health outcomes. Mol. Cell Endocrinol. 2010, 316, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Olshansky, S.J.; Passaro, D.J.; Hershow, R.C.; Layden, J.; Carnes, B.A.; Brody, J.; Hayflick, L.; Butler, R.N.; Allison, D.B.; Ludwig, D.S. A potential decline in life expectancy in the United States in the 21st century. N. Engl. J. Med. 2005, 352, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Kadouh, H.C.; Acosta, A. Current paradigms in the etiology of obesity. Tech. Gastrointest. Endosc. 2017, 19, 2–11. [Google Scholar] [CrossRef]
- Weinsier, R.L.; Hunter, G.R.; Heini, A.F.; Goran, M.I.; Sell, S.M. The etiology of obesity: Relative contribution of metabolic factors, diet, and physical activity. Am. J. Med. 1998, 105, 145–150. [Google Scholar] [CrossRef]
- Anversa, R.G.; Muthmainah, M.; Sketriene, D.; Gogos, A.; Sumithran, P.; Brown, R.M. A review of sex differences in the mechanisms and drivers of overeating. Front. Neuroendocrinol. 2021, 63, 100941. [Google Scholar] [CrossRef]
- Courtenay, W.H.; McCreary, D.R.; Merighi, J.R. Gender and ethnic differences in health beliefs and behaviors. J. Health Psychol. 2002, 7, 219–231. [Google Scholar] [CrossRef]
- Culbert, K.M.; Sisk, C.L.; Klump, K.L. A narrative review of sex differences in eating disorders: Is there a biological basis? Clin. Ther. 2021, 43, 95–111. [Google Scholar] [CrossRef]
- Stea, T.H.; Nordheim, O.; Bere, E.; Stornes, P.; Eikemo, T.A. Fruit and vegetable consumption in Europe according to gender, educational attainment and regional affiliation: A cross-sectional study in 21 European countries. PLoS ONE 2020, 15, e0232521. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Bale, T.L.; Epperson, C.N. Sex differences and stress across the lifespan. Nat. Neurosci. 2015, 18, 1413–1420. [Google Scholar] [CrossRef]
- Legget, K.T.; Cornier, M.A.; Bessesen, D.H.; Mohl, B.; Thomas, E.A.; Tregellas, J.R. Greater reward-related neuronal response to hedonic foods in women compared with men. Obesity 2018, 26, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Lovejoy, J.C.; Sainsbury, A. Sex differences in obesity and the regulation of energy homeostasis. Obes. Rev. 2009, 10, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Sicilia, A.; Fuller-Tyszkiewicz, M.; Rodgers, R.F.; Granero-Gallegos, A.; Lo Coco, G.; Dion, J.; McCabe, M.; Strodl, E.; Markey, C.H.; Aime, A.; et al. Cross-country measurement invariance and effects of sociodemographic factors on body weight and shape concern: Related constructs in eight countries. Body Image 2020, 35, 288–299. [Google Scholar] [CrossRef]
- Ekebas-Turedi, C.; Cilingir Uk, Z.; Basfirinci, C.; Pinar, M. A cross-cultural analysis of gender-based food stereotypes and consumption intentions among millenial consumers. J. Int. Consum. Mark 2020, 33, 209–225. [Google Scholar] [CrossRef]
- Bhargava, A.; Arnold, A.P.; Bangasser, D.A.; Denton, K.M.; Gupta, A.; Hilliard Krause, L.M.; Mayer, E.A.; McCarthy, M.; Miller, W.L.; Raznahan, A.; et al. Considering Sex as a biological variable in basic and clinical studies: An Endocrine Society scientific statement. Endocr. Rev. 2021, 42, 219–258. [Google Scholar] [CrossRef]
- Cornier, M.A.; Von Kaenel, S.S.; Bessesen, D.H.; Tregellas, J.R. Effects of overfeeding on the neuronal response to visual food cues. Am. J. Clin. Nutr. 2007, 86, 965–971. [Google Scholar] [CrossRef]
- Cornier, M.A.; McFadden, K.L.; Thomas, E.A.; Bechtell, J.L.; Eichman, L.S.; Bessesen, D.H.; Tregellas, J.R. Differences in the neuronal response to food in obesity-resistant as compared to obesity-prone individuals. Physiol. Behav. 2013, 110, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Neseliler, S.; Han, J.E.; Dagher, A. The use of functional magnetic resonance imaging in the study of appetite and obesity. In Appetite and Food Intake: Central Control; RBS, H., Ed.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2017. [Google Scholar]
- Tang, D.W.; Fellows, L.K.; Small, D.M.; Dagher, A. Food and drug cues activate similar brain regions: A meta-analysis of functional MRI studies. Physiol. Behav. 2012, 106, 317–324. [Google Scholar] [CrossRef]
- Brignell, C.; Griffiths, T.; Bradley, B.P.; Mogg, K. Attentional and approach biases for pictorial food cues: Influence of external eating. Appetite 2009, 52, 299–306. [Google Scholar] [CrossRef]
- Yokum, S.; Ng, J.; Stice, E. Attentional bias to food images associated with elevated weight and future weight gain: An fMRI study. Obesity 2011, 19, 1775–1783. [Google Scholar] [CrossRef]
- Chao, A.M.; Loughead, J.; Bakizada, Z.M.; Hopkins, C.M.; Geliebter, A.; Gur, R.C.; Wadden, T.A. Sex/gender differences in neural correlates of food stimuli: A systematic review of functional neuroimaging studies. Obes. Rev. 2017, 18, 687–699. [Google Scholar] [CrossRef] [PubMed]
- Cornier, M.A.; Salzberg, A.K.; Endly, D.C.; Bessesen, D.H.; Tregellas, J.R. Sex-based differences in the behavioral and neuronal responses to food. Physiol. Behav. 2010, 99, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.; Laharnar, N.; Kullmann, S.; Veit, R.; Canova, C.; Hegner, Y.L.; Fritsche, A.; Preissl, H. Processing of food pictures: Influence of hunger, gender and calorie content. Brain Res. 2010, 1350, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Geliebter, A.; Pantazatos, S.P.; McOuatt, H.; Puma, L.; Gibson, C.D.; Atalayer, D. Sex-based fMRI differences in obese humans in response to high vs. low energy food cues. Behav. Brain Res. 2013, 243, 91–96. [Google Scholar] [CrossRef]
- Uher, R.; Treasure, J.; Heining, M.; Brammer, M.J.; Campbell, I.C. Cerebral processing of food-related stimuli: Effects of fasting and gender. Behav. Brain Res. 2006, 169, 111–119. [Google Scholar] [CrossRef]
- Burger, K.S.; Cornier, M.A.; Ingebrigtsen, J.; Johnson, S.L. Assessing food appeal and desire to eat: The effects of portion size & energy density. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 101. [Google Scholar] [CrossRef]
- Udo, T.; Grilo, C.M. Prevalence and correlates of DSM-5-defined Eating disorders in a nationally representative sample of U.S. adults. Biol. Psychiatry 2018, 84, 345–354. [Google Scholar] [CrossRef]
- Bourdier, L.; Orri, M.; Carre, A.; Gearhardt, A.N.; Romo, L.; Dantzer, C.; Berthoz, S. Are emotionally driven and addictive-like eating behaviors the missing links between psychological distress and greater body weight? Appetite 2018, 120, 536–546. [Google Scholar] [CrossRef]
- Gibson, E.L. The psychobiology of comfort eating: Implications for neuropharmacological interventions. Behav. Pharmacol. 2012, 23, 442–460. [Google Scholar] [CrossRef]
- Burger, K.S.; Berner, L.A. A functional neuroimaging review of obesity, appetitive hormones and ingestive behavior. Physiol. Behav. 2014, 136, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Devoto, F.; Zapparoli, L.; Bonandrini, R.; Berlingeri, M.; Ferrulli, A.; Luzi, L.; Banfi, G.; Paulesu, E. Hungry brains: A meta-analytical review of brain activation imaging studies on food perception and appetite in obese individuals. Neurosci. Biobehav. Rev. 2018, 94, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D.; Yurgelun-Todd, D.A. Body mass predicts orbitofrontal activity during visual presentations of high-calorie foods. Neuroreport 2005, 16, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Stoeckel, L.E.; Weller, R.E.; Cook, E.W., 3rd; Twieg, D.B.; Knowlton, R.C.; Cox, J.E. Widespread reward-system activation in obese women in response to pictures of high-calorie foods. Neuroimage 2008, 41, 636–647. [Google Scholar] [CrossRef] [PubMed]
- Murdaugh, D.L.; Cox, J.E.; Cook, E.W., 3rd; Weller, R.E. fMRI reactivity to high-calorie food pictures predicts short- and long-term outcome in a weight-loss program. Neuroimage 2012, 59, 2709–2721. [Google Scholar] [CrossRef] [PubMed]
- Yokum, S.; Gearhardt, A.N.; Harris, J.L.; Brownell, K.D.; Stice, E. Individual differences in striatum activity to food commercials predict weight gain in adolescents. Obesity 2014, 22, 2544–2551. [Google Scholar] [CrossRef] [PubMed]
- Boswell, R.G.; Kober, H. Food cue reactivity and craving predict eating and weight gain: A meta-analytic review. Obes. Rev. 2016, 17, 159–177. [Google Scholar] [CrossRef]
- Deglaire, A.; Mejean, C.; Castetbon, K.; Kesse-Guyot, E.; Hercberg, S.; Schlich, P. Associations between weight status and liking scores for sweet, salt and fat according to the gender in adults (The Nutrinet-Sante study). Eur. J. Clin. Nutr. 2015, 69, 40–46. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap): A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Messick, S. The Three-Factor Eating Questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Eaton, W.W.; Smith, C.; Ybarra, M.; Muntaner, C.; Tien, A. Center for Epidemiologic Studies Depression Scale: Review and revision (CESD and CESD-R). In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment, 3rd ed.; Maurish, M.E., Ed.; Lawrence Erlbaum: Mahwah, NJ, USA, 2004; pp. 363–377. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Cepeda-Benito, A.; Gleaves, D.H.; Williams, T.L.; Erath, S.A. The development and validation of the state and trait food-cravings questionnaries. Behav. Ther. 2000, 31, 151–173. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Lang, P.; Bradley, M.M.; Cuthbert, B.N. International Affective Picture System (IAPS): Instruction Manual and Affective Ratings; The Center for Research in Psychophysiology, University of Florida: Gainesville, FL, USA, 2001. [Google Scholar]
- Rosner, B. Percentage points for a generalized ESD many-outlier procedure. Technometrics 1983, 25, 165–172. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 15 August 2022).
- Ernst, B.; Wilms, B.; Thurnheer, M.; Schultes, B. Eating behaviour in treatment-seeking obese subjects: Influence of sex and BMI classes. Appetite 2015, 95, 96–100. [Google Scholar] [CrossRef]
- Bottera, A.R.; Kambanis, P.E.; De Young, K.P. Persistence: A key factor in understanding the circumstances under which dietary restraint predicts restriction of caloric intake. Eat. Behav. 2021, 43, 101563. [Google Scholar] [CrossRef]
- Burton, P.; Smit, H.J.; Lightowler, H.J. The influence of restrained and external eating patterns on overeating. Appetite 2007, 49, 191–197. [Google Scholar] [CrossRef]
- Hill, A.J.; Weaver, C.F.; Blundell, J.E. Food craving, dietary restraint and mood. Appetite 1991, 17, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef]
- Tryon, M.S.; Carter, C.S.; Decant, R.; Laugero, K.D. Chronic stress exposure may affect the brain’s response to high calorie food cues and predispose to obesogenic eating habits. Physiol. Behav. 2013, 120, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.L.; Boles, R.E.; Burger, K.S. Using participant hedonic ratings of food images to construct data driven food groupings. Appetite 2014, 79, 189–196. [Google Scholar] [CrossRef]
- Jensen, C.D.; Duraccio, K.M.; Barnett, K.A.; Stevens, K.S. Appropriateness of the food-pics image database for experimental eating and appetite research with adolescents. Eat. Behav. 2016, 23, 195–199. [Google Scholar] [CrossRef]
- Spinelli, S.; Monteleone, E. Food preferences and obesity. Endocrinol. Metab. 2021, 36, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Ahima, R.S.; Lazar, M.A. Physiology. The health risk of obesity: Better Metrics Imperative. Science 2013, 341, 856–858. [Google Scholar] [CrossRef]
- Shah, N.R.; Braverman, E.R. Measuring adiposity in patients: The utility of body mass index (BMI), percent body fat, and leptin. PLoS ONE 2012, 7, e33308. [Google Scholar] [CrossRef]
- Ristori, J.; Cocchetti, C.; Romani, A.; Mazzoli, F.; Vignozzi, L.; Maggi, M.; Fisher, A.D. Brain Sex differences related to gender identity development: Genes or hormones? Int. J. Mol. Sci. 2020, 21, 2123. [Google Scholar] [CrossRef]
- Munt, A.E.; Partridge, S.R.; Allman-Farinelli, M. The barriers and enablers of healthy eating among young adults: A missing piece of the obesity puzzle: A scoping review. Obes. Rev. 2017, 18, 1–17. [Google Scholar] [CrossRef]
- Sharkey, T.; Whatnall, M.C.; Hutchesson, M.J.; Haslam, R.L.; Bezzina, A.; Collins, C.E.; Ashton, L.M. Effectiveness of gender-targeted versus gender-neutral interventions aimed at improving dietary intake, physical activity and/or overweight/obesity in young adults (aged 17–35 years): A systematic review and meta-analysis. Nutr. J. 2020, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Dog, T.L.; Smith-Ryan, A.E.; Das, S.K.; Baker, F.C.; Madak-Erdogan, Z.; Hammond, B.R.; Sesso, H.D.; Eapen, A.; Mitmesser, S.H.; et al. Sex differences across the life course: A focus on unique nutritional and health considerations among women. J. Nutr. 2022, 152, 1597–1610. [Google Scholar] [CrossRef] [PubMed]
- Keleher, H. Why build a health promotion evidence base about gender? Health Promot. Int. 2004, 19, 277–279. [Google Scholar] [CrossRef]
- Ostlin, P.; Eckermann, E.; Mishra, U.S.; Nkowane, M.; Wallstam, E. Gender and health promotion: A multisectoral policy approach. Health Promot. Int. 2006, 21, 25–35. [Google Scholar] [CrossRef]
- White, J.; Tannenbaum, C.; Klinge, I.; Schiebinger, L.; Clayton, J. The Integration of sex and gender considerations into biomedical research: Lessons from international funding agencies. J. Clin. Endocrinol. Metab. 2021, 106, 3034–3048. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Difference | ||
|---|---|---|---|
| Measure | Women (n = 155) | Men (n = 151) | p1 |
| Age (years) 2,3 | 44.9 ± 15.6 | 49.5 ± 14.0 | 0.007 |
| BMI (kg/m2) 2,3 | 28.6 ± 7.8 | 29.3 ± 5.7 | 0.358 |
| Race, n (%) 4 | 0.541 | ||
| White | 140 (90.3) | 143 (94.7) | |
| Asian | 7 (4.5) | 2 (1.3) | |
| Black or African American | 4 (2.6) | 3 (2.0) | |
| American Indian or Alaska | 1 (0.7) | 1 (0.7) | |
| Native | |||
| Other | 3 (1.9) | 2 (1.3) | |
| Ethnicity, n (%) 4 | 0.071 | ||
| Hispanic or Latino | 5 (3) | 12 (8) | |
| Not Hispanic of Latino | 150 (97) | 139 (92) | |
| Time Since Last Ate (hours) 2,3 | 2.9 ± 2.0 | 3.0 ± 1.8 | 0.811 |
| VAS: Hunger 2,3 | 38.0 ± 25.2 | 32.6 ± 24.7 | 0.061 |
| VAS: Satiety 2,3 | 46.6 ± 23.1 | 48.2 ± 21.9 | 0.520 |
| TFEQ: Restraint 2,3 | 10.0 ± 4.8 | 8.5 ± 4.5 | 0.004 |
| TFEQ: Hunger 2,3 | 5.4 ± 3.6 | 4.6 ± 3.5 | 0.044 |
| TFEQ: Disinhibition 2,3 | 8.0 ± 4.2 | 6.1 ± 3.6 | <0.001 |
| FCQ-S 2,3 | 33.1 ± 12.3 | 31.2 ± 11.7 | 0.170 |
| EAT-26 2,3 | 12.3 ± 10.5 | 8.1 ± 7.4 | <0.001 |
| CESD-R 2,3 | 17.7 ± 11.2 | 14.3 ± 10.4 | 0.006 |
| STAI 2,3 | 34.8 ± 12.7 | 32.3 ± 11.8 | 0.082 |
| PSS 2,3 | 31.1 ± 4.3 | 28.6 ± 5.0 | <0.001 |
| HC Familiarity 2,3 | 3.4 ± 0.3 | 3.4 ± 0.3 | 0.340 |
| LC Familiarity 2,3 | 3.6 ± 0.3 | 3.4 ± 0.3 | <0.001 |
| HC Desire to Eat 2,3 | 40.3 ± 23.2 | 43.4 ± 24.0 | 0.250 |
| LC Desire to Eat 2,3 | 42.1 ± 20.0 | 39.5 ± 19.4 | 0.255 |
| HC–LC Desire to Eat 2,3 | −1.8 ± 18.8 | 3.9 ± 18.7 | 0.009 |
| HC Appeal 2,3 | 61.7 ± 16.4 | 64.5 ± 15.7 | 0.132 |
| LC Appeal 2,3 | 63.2 ± 13.1 | 58.3 ± 13.9 | 0.002 |
| HC–LC Appeal 2,3 | −1.4 ± 18.8 | 6.3 ± 19.7 | 0.001 |
| Measure | Rating Type | Effect on Ratings 1,2 | Sex Interaction | ||
|---|---|---|---|---|---|
| F | p 3 | F | p 3 | ||
| Hunger (VAS) | Appeal | 13.50 | <0.001 | 0.11 | 0.742 |
| Desire | 96.21 | <0.001 | 0.04 | 0.849 | |
| Satiety (VAS) | Appeal | 0.69 | 0.408 | 0.15 | 0.699 |
| Desire | 20.32 | <0.001 | 1.21 | 0.272 | |
| TFEQ: Restraint | Appeal | 2.31 | 0.130 | 3.43 | 0.065 |
| Desire | 1.96 | 0.163 | 1.41 | 0.236 | |
| TFEQ: Disinhibition | Appeal | 47.45 | <0.001 | 0.01 | 0.923 |
| Desire | 40.03 | <0.001 | 0.003 | 0.956 | |
| TFEQ: Hunger | Appeal | 46.63 | <0.001 | 0.28 | 0.598 |
| Desire | 78.33 | <0.001 | 0.02 | 0.898 | |
| FCQ-S | Appeal | 28.62 | <0.001 | 0.02 | 0.899 |
| Desire | 137.24 | <0.001 | 0.06 | 0.805 | |
| EAT-26 | Appeal | 1.83 | 0.177 | 0.27 | 0.604 |
| Desire | 0.53 | 0.466 | 0.85 | 0.356 | |
| CESD-R | Appeal | 1.15 | 0.283 | 0.20 | 0.653 |
| Desire | 7.24 | 0.008 | 0.01 | 0.920 | |
| STAI | Appeal | 2.65 | 0.104 | 0.77 | 0.379 |
| Desire | 22.72 | <0.001 | 0.003 | 0.955 | |
| PSS | Appeal | 0.19 | 0.658 | 7.68 | 0.006 |
| Desire | 0.02 | 0.880 | 1.42 | 0.235 | |
| BMI | Appeal | 4.18 | 0.042 | 0.16 | 0.687 |
| Desire | 1.69 | 0.195 | 1.54 | 0.216 | |
| Measure | Rating Type | Effect on Ratings 1,2 | Sex Interaction | ||
|---|---|---|---|---|---|
| F | p3 | F | p 3 | ||
| Hunger (VAS) | Appeal | 6.83 | 0.009 | 0.68 | 0.411 |
| Desire | 61.43 | <0.001 | 3.00 | 0.084 | |
| Satiety (VAS) | Appeal | 3.41 | 0.066 | 0.07 | 0.793 |
| Desire | 29.25 | <0.001 | 3.88 | 0.049 | |
| TFEQ: Restraint | Appeal | 1.23 | 0.268 | 0.03 | 0.859 |
| Desire | 0.08 | 0.784 | 0.40 | 0.527 | |
| TFEQ: Disinhibition | Appeal | 12.15 | <0.001 | 5.18 | 0.024 |
| Desire | 3.53 | 0.061 | 0.86 | 0.355 | |
| TFEQ: Hunger | Appeal | 9.03 | 0.003 | 0.005 | 0.946 |
| Desire | 4.60 | 0.033 | 0.02 | 0.898 | |
| FCQ-S | Appeal | 6.35 | 0.012 | 2.70 | 0.102 |
| Desire | 40.66 | <0.001 | 0.05 | 0.821 | |
| EAT-26 | Appeal | 0.64 | 0.423 | 2.39 | 0.123 |
| Desire | 0.11 | 0.729 | 0.48 | 0.488 | |
| CESD-R | Appeal | 0.001 | 0.979 | 2.78 | 0.097 |
| Desire | 7.10 | 0.008 | 0.99 | 0.321 | |
| STAI | Appeal | 1.41 | 0.235 | 3.66 | 0.057 |
| Desire | 16.45 | <0.001 | 0.006 | 0.940 | |
| PSS | Appeal | 6.92 | 0.009 | 0.80 | 0.372 |
| Desire | 2.19 | 0.140 | 0.01 | 0.929 | |
| BMI | Appeal | 0.08 | 0.773 | 0.08 | 0.779 |
| Desire | 0.58 | 0.445 | 1.55 | 0.214 | |
| Measure | Rating Type | Effect on Ratings 1,2 | Sex Interaction | ||
|---|---|---|---|---|---|
| F | p3 | F | p3 | ||
| Hunger (VAS) | Appeal | 25.28 | <0.001 | 0.10 | 0.753 |
| Desire | 10.59 | 0.001 | 2.15 | 0.144 | |
| Satiety (VAS) | Appeal | 4.00 | 0.047 | 0.26 | 0.609 |
| Desire | 0.003 | 0.959 | 0.39 | 0.532 | |
| TFEQ: Restraint | Appeal | 4.25 | 0.040 | 2.83 | 0.094 |
| Desire | 4.79 | 0.029 | 4.69 | 0.031 | |
| TFEQ: Disinhibition | Appeal | 43.23 | <0.001 | 2.63 | 0.106 |
| Desire | 33.23 | <0.001 | 1.17 | 0.280 | |
| TFEQ: Hunger | Appeal | 67.02 | <0.001 | 0.16 | 0.687 |
| Desire | 71.93 | <0.001 | 0.09 | 0.760 | |
| FCQ-S | Appeal | 41.46 | <0.001 | 1.23 | 0.268 |
| Desire | 38.93 | <0.001 | 0.001 | 0.972 | |
| EAT-26 | Appeal | 0.32 | 0.572 | 0.42 | 0.515 |
| Desire | 1.63 | 0.203 | 0.18 | 0.669 | |
| CESD-R | Appeal | 0.78 | 0.378 | 0.63 | 0.427 |
| Desire | 0.32 | 0.571 | 0.82 | 0.367 | |
| STAI | Appeal | 4.88 | 0.028 | 0.37 | 0.543 |
| Desire | 2.62 | 0.106 | <0.001 | 0.993 | |
| PSS | Appeal | 2.15 | 0.144 | 2.83 | 0.093 |
| Desire | 3.02 | 0.083 | 2.53 | 0.113 | |
| BMI | Appeal | 3.67 | 0.057 | 0.02 | 0.890 |
| Desire | 5.95 | 0.015 | 0.06 | 0.806 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Legget, K.T.; Cornier, M.-A.; Sarabia, L.; Delao, E.M.; Mikulich-Gilbertson, S.K.; Natvig, C.; Erpelding, C.; Mitchell, T.; Hild, A.; Kronberg, E.; et al. Sex Differences in Effects of Mood, Eating-Related Behaviors, and BMI on Food Appeal and Desire to Eat: A Cross-Sectional Survey Study. Nutrients 2023, 15, 762. https://doi.org/10.3390/nu15030762
Legget KT, Cornier M-A, Sarabia L, Delao EM, Mikulich-Gilbertson SK, Natvig C, Erpelding C, Mitchell T, Hild A, Kronberg E, et al. Sex Differences in Effects of Mood, Eating-Related Behaviors, and BMI on Food Appeal and Desire to Eat: A Cross-Sectional Survey Study. Nutrients. 2023; 15(3):762. https://doi.org/10.3390/nu15030762
Chicago/Turabian StyleLegget, Kristina T., Marc-Andre Cornier, Lauren Sarabia, Eve M. Delao, Susan K. Mikulich-Gilbertson, Crystal Natvig, Christina Erpelding, Tessa Mitchell, Allison Hild, Eugene Kronberg, and et al. 2023. "Sex Differences in Effects of Mood, Eating-Related Behaviors, and BMI on Food Appeal and Desire to Eat: A Cross-Sectional Survey Study" Nutrients 15, no. 3: 762. https://doi.org/10.3390/nu15030762
APA StyleLegget, K. T., Cornier, M. -A., Sarabia, L., Delao, E. M., Mikulich-Gilbertson, S. K., Natvig, C., Erpelding, C., Mitchell, T., Hild, A., Kronberg, E., & Tregellas, J. R. (2023). Sex Differences in Effects of Mood, Eating-Related Behaviors, and BMI on Food Appeal and Desire to Eat: A Cross-Sectional Survey Study. Nutrients, 15(3), 762. https://doi.org/10.3390/nu15030762