

Determining Dietary Patterns to Recommend for Type 2 Diabetes: An Umbrella Review


Abstract
:1. Introduction
2. Materials and Methods
3. Results
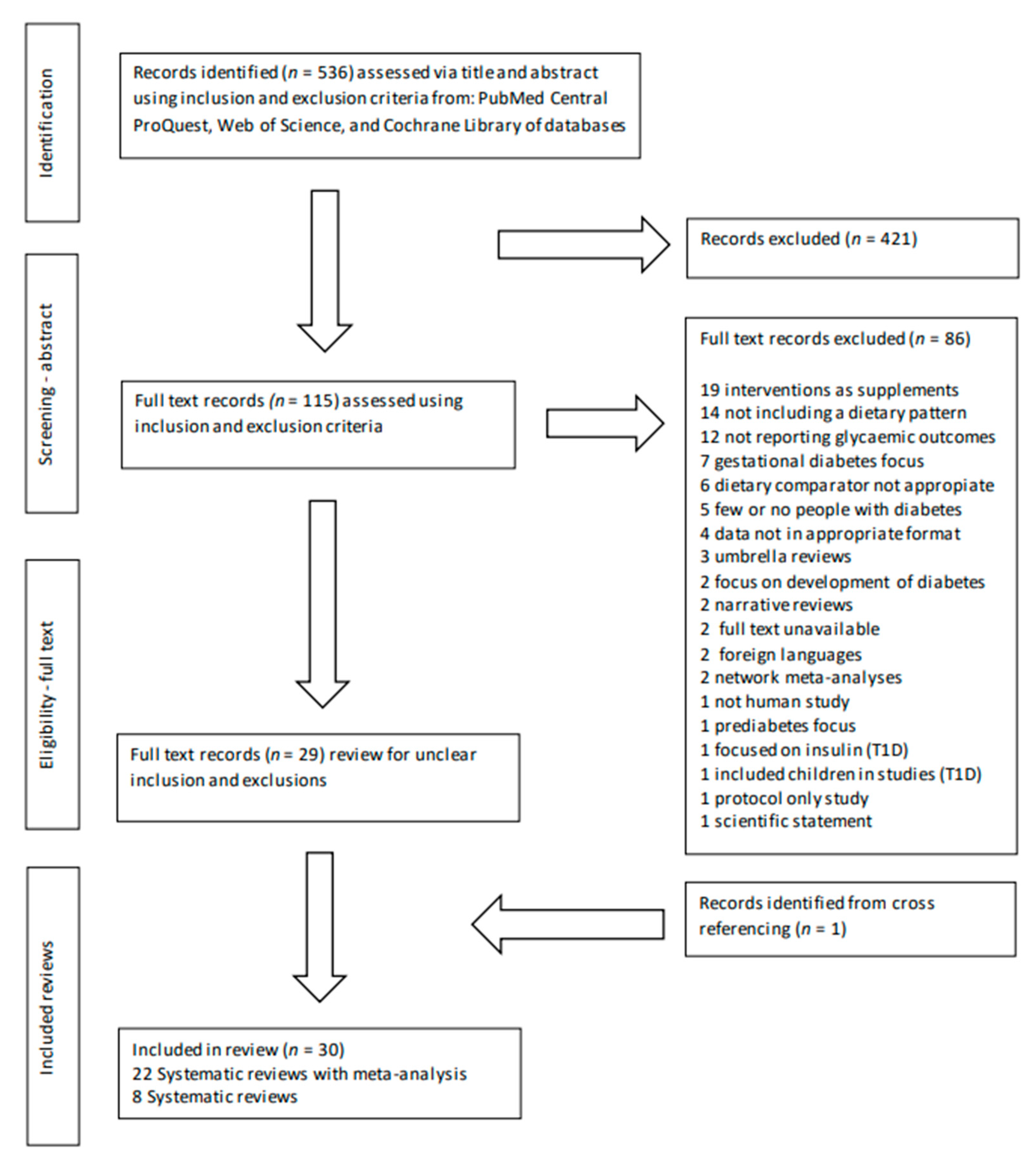
3.1. Identification of Records Included in This Umbrella Review
3.2. Characteristics of the Systematic Reviews Included in This Umbrella Review
3.3. Primary Outcomes
3.4. Secondary Outcomes
3.5. Quality and Risk of Bias of Appraisals
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Global Report on Diabetes; WHO Press: Geneva, Switzerland, 2016. [Google Scholar]
- Australian Institute of Health and Welfare A. Diabetes; AIHW: Canberra, Australia, 2020.
- Diabetes Australia. About-Diabetes. 2022. Available online: https://www.diabetesaustralia.com.au/about-diabetes/diabetes-in-australia/ (accessed on 5 July 2022).
- Deed, G.; Barlow, J.; Kawol, D.; Kilov, G.; Sharma, A.; Yu Hwa, L. Diet and diabetes. Aust. Fam. Physician 2015, 44, 288–292. [Google Scholar]
- Diabetes Australia. About-Diabetes Myths-Facts. 2022. Available online: https://www.diabetesaustralia.com.au/about-diabetes/myths-facts/ (accessed on 5 July 2022).
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, nutrients, and dietary patterns: Interconnections and implications for dietary guidelines. Adv. Nutr. 2016, 7, 445–454. [Google Scholar] [PubMed]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and nutritional approaches for prevention and management of type 2 diabetes. BMJ 2018, 361, k2234. [Google Scholar] [PubMed]
- Hendrie, G.A.; Lyle, G.; Mauch, C.E.; Haddad, J.; Golley, R.K. Understanding the Variation within a Dietary Guideline Index Score to Identify the Priority Food Group Targets for Improving Diet Quality across Population Subgroups. Int. J. Environ. Res. Public Health 2021, 18, 378. [Google Scholar] [PubMed]
- Australian Bureau of Statistics (ABS). 4364.0.55.012—Australian Health Survey: Consumption of Food Groups from the Australian Dietary Guidelines, 2011–2012. Published 2016. Available online: https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/77E3E65E4D967249CA2581F40016ABD6/$File/4364.0.55.012%20-%20consumption%20of%20food%20groups%20from%20australian%20dietary%20guidelines.pdf (accessed on 13 September 2021).
- National Health and Medical Research Council N. Australian Dietary Guidelines; Australian Government: Canberra, Australia, 2013.
- Mozaffarian, D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: A comprehensive review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Himmelstein, M.; Puhl, R. At multiple fronts: Diabetes stigma and weight stigma in adults with type 2 diabetes. Diabet. Med. 2021, 38, e14387. [Google Scholar] [CrossRef]
- Pillen, H.; Ward, P.R. How might diabetes organisations address diabetes-related stigma? Findings from a deliberative democratic case study. Health Expect. 2021, 25, 2213–2222. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; Boucher, J.L.; Evert, A.B. Evidence-based diabetes nutrition therapy recommendations are effective: The key is individualization. Diabetes Metab. Syndr. Obes. 2014, 7, 65–72. [Google Scholar]
- Franz, M.J.; MacLeod, J.; Evert, A.; Brown, C.; Gradwell, E.; Handu, D.; Reppert, A.; Robinson, M. Academy of Nutrition and Dietetics nutrition practice guideline for type 1 and type 2 diabetes in adults: Systematic review of evidence for medical nutrition therapy effectiveness and recommendations for integration into the nutrition care process. J. Acad. Nutr. Diet. 2017, 117, 1659–1679. [Google Scholar]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults with Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731. [Google Scholar] [CrossRef] [PubMed]
- Vijan, S.; Stuart, N.S.; Fitzgerald, J.T.; Ronis, D.L.; Hayward, R.A.; Slater, S.; Hofer, T.P. Barriers to following dietary recommendations in type 2 diabetes. Diabet. Med. 2005, 22, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Bruce, D.G.; Davis, W.A.; Cull, C.A.; Davis, T.M. Diabetes education and knowledge in patients with type 2 diabetes from the community: The Fremantle Diabetes Study. J. Diabetes Complicat. 2003, 17, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Rosenberg, I.; Uauy, R. History of modern nutrition science—Implications for current research, dietary guidelines, and food policy. BMJ 2018, 361, k2392. [Google Scholar]
- Cena, H.; Calder, P.C. Defining a healthy diet: Evidence for the role of contemporary dietary patterns in health and disease. Nutrients 2020, 12, 334. [Google Scholar]
- Sievenpiper, J.L.; Dworatzek, P.D. Food and dietary pattern-based recommendations: An emerging approach to clinical practice guidelines for nutrition therapy in diabetes. Can. J. Diabetes 2013, 37, 51–57. [Google Scholar] [CrossRef]
- Maghsoudi, Z.; Azadbakht, L. How dietary patterns could have a role in prevention, progression, or management of diabetes mellitus? Review on the current evidence. J. Res. Med. Sci. 2012, 17, 694–709. [Google Scholar]
- Baxter, M.; Hudson, R.; Mahon, J.; Bartlett, C.; Samyshkin, Y.; Alexiou, D.; Hex, N. Estimating the impact of better management of glycaemic control in adults with type 1 and type 2 diabetes on the number of clinical complications and the associated financial benefit. Diabet. Med. 2016, 33, 1575–1581. [Google Scholar] [CrossRef]
- Dal Canto, E.; Ceriello, A.; Rydén, L.; Ferrini, M.; Hansen, T.B.; Schnell, O.; Standl, E.; Beulens, J.W. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Eur. J. Prev. Cardiol. 2019, 26 (Suppl. 2), 25–32. [Google Scholar] [CrossRef]
- Kirkpatrick, C.F.; Bolick, J.P.; Kris-Etherton, P.M.; Sikand, G.; Aspry, K.E.; Soffer, D.E.; Willard, K.E.; Maki, K.C. Review of current evidence and clinical recommendations on the effects of low-carbohydrate and very-low-carbohydrate (including ketogenic) diets for the management of body weight and other cardiometabolic risk factors: A scientific statement from the National Lipid Association Nutrition and Lifestyle Task Force. J. Clin. Lipidol. 2019, 13, 689–711.e1. [Google Scholar]
- Jamka, M.; Kulczyński, B.; Juruć, A.; Gramza-Michałowska, A.; Stokes, C.S.; Walkowiak, J. The Effect of the Paleolithic Diet vs. Healthy Diets on Glucose and Insulin Homeostasis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 2, 296. [Google Scholar]
- Malaeb, S.; Bakker, C.; Chow, L.S.; Bantle, A.E. High-Protein Diets for Treatment of Type 2 Diabetes Mellitus: A Systematic Review. Adv. Nutr. 2019, 10, 621–633. [Google Scholar] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [PubMed]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef]
- Papamichou, D.; Panagiotakos, D.B.; Itsiopoulos, C. Dietary patterns and management of type 2 diabetes: A systematic review of randomised clinical trials. Nutr. Metab. Carbiovasc. Dis. 2019, 29, 531–543. [Google Scholar]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Qian, F.; Korat, A.A.; Malik, V.; Hu, F.B. Metabolic Effects of Monounsaturated Fatty Acid-Enriched Diets Compared with Carbohydrate or Polyunsaturated Fatty Acid-Enriched Diets in Patients with Type 2 Diabetes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Diabetes Care 2016, 39, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Ajala, O.; English, P.; Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Alcorta, A.; Porta, A.; Tárrega, A.; Alvarez, M.D.; Vaquero, M.P. Foods for plant-based diets: Challenges and innovations. Foods 2021, 10, 293. [Google Scholar] [CrossRef]
- Craig, W.J. Health effects of vegan diets. Am. J. Clin. Nutr. 2009, 89, 1627S–1633S. [Google Scholar] [PubMed]
- Fung, T.T.; Schulze, M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Dietary patterns, meat intake, and the risk of type 2 diabetes in women. Arch. Intern. Med. 2004, 164, 2235–2240. [Google Scholar] [CrossRef] [PubMed]
- Medawar, E.; Huhn, S.; Villringer, A.; Veronica Witte, A. The effects of plant-based diets on the body and the brain: A systematic review. Transl. Psychiatry 2019, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Ojo, O.; Ojo, O.O.; Adebowale, F.; Wang, X.H. The Effect of Dietary Glycaemic Index on Glycaemia in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Kendall, C.W.; McKeown-Eyssen, G.; Josse, R.G.; Silverberg, J.; Booth, G.L.; Vidgen, E.; Josse, A.R.; Nguyen, T.H.; Corrigan, S.; et al. Effect of a low–glycemic index or a high–cereal fiber diet on type 2 diabetes: A randomized trial. JAMA 2008, 300, 2742–2753. [Google Scholar] [PubMed]
- Chiavaroli, L.; Viguiliouk, E.; Nishi, S.K.; Blanco Mejia, S.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Kendall, C.W.; Sievenpiper, J.L. DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutrients 2019, 11, 338. [Google Scholar] [CrossRef]
- Vitale, R.; Kim, Y. The Effects of Intermittent Fasting on Glycemic Control and Body Composition in Adults with Obesity and Type 2 Diabetes: A Systematic Review. Metab. Syndr. Relat. Disord. 2020, 10, 450–461. [Google Scholar] [CrossRef]
- Welton, S.; Minty, R.; O’Driscoll, T.; Willms, H.; Poirier, D.; Madden, S.; Kelly, L. Intermittent fasting and weight loss: Systematic review. Can. Fam. Physician 2020, 66, 117–125. [Google Scholar]
- van Zuuren, E.J.; Fedorowicz, Z.; Kuijpers, T.; Pijl, H. Effects of low-carbohydrate- compared with low-fat-diet interventions on metabolic control in people with type 2 diabetes: A systematic review including GRADE assessments. Am. J. Clin. Nutr. 2018, 108, 300–331. [Google Scholar] [CrossRef]
- Huntriss, R.; Campbell, M.; Bedwell, C. The interpretation and effect of a low-carbohydrate diet in the management of type 2 diabetes: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2018, 72, 15. [Google Scholar]
- Howard, B.V.; Van Horn, L.; Hsia, J.; Manson, J.E.; Stefanick, M.I.; Wassertheil-Smoller, S.; Kuller, L.H.; LaCroix, A.Z.; Langer, R.D.; Lasser, N.I.; et al. Low-fat dietary pattern and risk of cardiovascular disease: The Women’s Health Initiative Randomized Controlled Dietary Modification Trial. JAMA 2006, 295, 655–666. [Google Scholar]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley Blackwell: Oxford, UK, 2008. [Google Scholar]
- Schwingshackl, L.; Chaimani, A.; Hoffmann, G.; Schwedhelm, C.; Boeing, H. A network meta-analysis on the comparative efficacy of different dietary approaches on glycaemic control in patients with type 2 diabetes mellitus. Eur. J. Epidemiol. 2018, 33, 157–170. [Google Scholar] [PubMed]
- de Carvalho, G.B.; Dias-Vasconcelos, N.L.; Santos, R.K.F.; Brandao-Lima, P.N.; da Silva, D.G.; Pires, L.V. Effect of different dietary patterns on glycemic control in individuals with type 2 diabetes mellitus: A systematic review. Crit. Rev. Food Sci. Nutr. 2020, 60, 1999–2010. [Google Scholar] [PubMed]
- Emadian, A.; Andrews, R.C.; England, C.Y.; Wallace, V.; Thompson, J.L. The effect of macronutrients on glycaemic control: A systematic review of dietary randomised controlled trials in overweight and obese adults with type 2 diabetes in which there was no difference in weight loss between treatment groups. Br. J. Nutr. 2015, 114, 1656–1666. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.F.; Di, H.J.; Chen, G.F.; Mao, X.D.; Liu, C. Effects of low carbohydrate diets in individuals with type 2 diabetes: Systematic review and meta-analysis. Int. J. Clin. Exp. Med. 2016, 9, 11166–11174. [Google Scholar]
- Korsmo-Haugen, H.K.; Brurberg, K.G.; Mann, J.; Aas, A.M. Carbohydrate quantity in the dietary management of type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2019, 21, 15–27. [Google Scholar] [CrossRef]
- McArdle, P.D.; Greenfield, S.M.; Rilstone, S.K.; Narendran, P.; Haque, M.S.; Gill, P.S. Carbohydrate restriction for glycaemic control in Type 2 diabetes: A systematic review and meta-analysis. Diabet. Med. 2019, 36, 335–348. [Google Scholar] [CrossRef]
- Meng, Y.; Bai, H.; Wang, S.J.; Li, Z.P.; Wang, Q.; Chen, L.Y. Efficacy of low carbohydrate diet for type 2 diabetes mellitus management: A systematic review and meta-analysis of randomized controlled trials. Diabetes Res. Clin. Pract. 2017, 131, 124–131. [Google Scholar]
- Naude, C.E.; Schoonees, A.; Senekal, M.; Young, T.; Garner, P.; Volmink, J. Low Carbohydrate versus Isoenergetic Balanced Diets for Reducing Weight and Cardiovascular Risk: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, 30. [Google Scholar]
- Sainsbury, E.; Kizirian, N.V.; Partridge, S.R.; Gill, T.; Colagiuri, S.; Gibson, A.A. Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2018, 139, 239–252. [Google Scholar]
- Snorgaard, O.; Poulsen, G.M.; Andersen, H.K.; Astrup, A. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2017, 5, 10. [Google Scholar] [CrossRef]
- Yu, Z.P.; Nan, F.W.; Wang, L.Y.; Jiang, H.; Chen, W.; Jiang, Y. Effects of high-protein diet on glycemic control, insulin resistance and blood pressure in type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2020, 39, 1724–1734. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Kabeya, Y.; Noto, H. Dietary Approaches for Japanese Patients with Diabetes: A Systematic Review. Nutrients 2018, 10, 9. [Google Scholar]
- Castaneda-Gonzalez, L.M.; Gascon, M.B.; Cruz, A.J. Effects of low carbohydrate diets on weight and glycemic control among type 2 diabetes individuals: A systemic review of RCT greater than 12 weeks. Nutr. Hosp. 2011, 26, 1270–1276. [Google Scholar]
- Goldenberg, J.Z.; Day, A.; Brinkworth, G.D.; Sato, J.; Yamada, S.; Jönsson, T.; Beardsley, J.; A Johnson, J.; Thabane, L.; Johnston, B.C. Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: Systematic review and meta-analysis of published and unpublished randomized trial data. BMJ 2021, 372, m4743. [Google Scholar] [CrossRef]
- Li, S.; Ding, L.; Xiao, X. Comparing the Efficacy and Safety of Low-Carbohydrate Diets with Low-Fat Diets for Type 2 Diabetes Mellitus Patients: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Endocrinol. 2021, 2021, 8521756. [Google Scholar]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.; Giugliano, D. A journey into a Mediterranean diet and type 2 diabetes: A systematic review with meta-analyses. BMJ Open 2015, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Maiorino, M.I.; Ceriello, A.; Giugliano, D. Prevention and control of type 2 diabetes by Mediterranean diet: A systematic review. Diabetes Res. Clin. Pract. 2010, 89, 97–102. [Google Scholar] [CrossRef]
- Sleiman, D.; Al-Badri, M.R.; Azar, S.T. Effect of Mediterranean diet in diabetes control and cardiovascular risk modification: A systematic review. Front. Public Health 2015, 3, 8. [Google Scholar]
- Viguiliouk, E.; Stewart, S.E.; Jayalath, V.H.; Ng, A.P.; Mirrahimi, A.; De Souza, R.J.; Hanley, A.J.; Bazinet, R.P.; Mejia, S.B.; Leiter, L.A.; et al. Effect of Replacing Animal Protein with Plant Protein on Glycemic Control in Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2015, 7, 9804–9824. [Google Scholar]
- Viguiliouk, E.; Kendall, C.W.; Kahleová, H.; Rahelić, D.; Salas-Salvadó, J.; Choo, V.L.; Mejia, S.B.; Stewart, S.E.; Leiter, L.A.; Jenkins, D.J.; et al. Effect of vegetarian dietary patterns on cardiometabolic risk factors in diabetes: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2019, 38, 1133–1145. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Barnard, N.D.; Levin, S.M.; Watanabe, M. Vegetarian diets and glycemic control in diabetes: A systematic review and meta-analysis. Cardiovasc. Diagn. Ther. 2014, 4, 373–382. [Google Scholar] [PubMed]
- Toumpanakis, A.; Turnbull, T.; Alba-Barba, I. Effectiveness of plant-based diets in promoting well-being in the management of type 2 diabetes: A systematic review. BMJ Open Diabetes Res. Care 2018, 6, e000534. [Google Scholar] [CrossRef] [PubMed]
- Johannesen, C.O.; Dale, H.F.; Jensen, C.; Lied, G.A. Effects of Plant-Based Diets on Outcomes Related to Glucose Metabolism: A Systematic Review. Diabetes Metab. Syndr. Obes. 2020, 13, 2811–2822. [Google Scholar] [PubMed]
- Zafar, M.; Mills, K.; Zheng, J.; Peng, M.; Ye, X.; Chen, L. Low glycaemic index diets as an intervention for obesity: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 290–315. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Becerra-Tomás, N.; Papandreou, C.; Bulló, M. Dietary Patterns Emphasizing the Consumption of Plant Foods in the Management of Type 2 Diabetes: A Narrative Review. Adv. Nutr. 2019, 10 (Suppl. 4), S320–S331. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Petrizzo, M.; Bellastella, G.; Giugliano, D. The effects of a Mediterranean diet on the need for diabetes drugs and remission of newly diagnosed type 2 diabetes: Follow-up of a randomized trial. Diabetes Care 2014, 37, 1824–1830. [Google Scholar]
- Stratton, I.M.; Adler, A.I.; Neil, H.A.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 2000, 321, 405–412. [Google Scholar]
- Pan, B.; Wu, Y.; Yang, Q.; Ge, L.; Gao, C.; Xun, Y.; Tian, J.; Ding, G. The impact of major dietary patterns on glycemic control, cardiovascular risk factors, and weight loss in patients with type 2 diabetes: A network meta-analysis. J. Evid.-Based Med. 2019, 12, 29–39. [Google Scholar]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar]
- Morris, E.; Jebb, S.; Oke, J.; Nickless, A.; Ahern, A.; Boyland, E.; Caterson, I.; Halford, J.; Hauner, H.; Aveyard, P. How effective is weight loss in reducing cardiometabolic risk? An observational analysis of two randomised controlled trials of community weight loss programmes. Br. J. Gen. Pract. 2020, 71. [Google Scholar] [CrossRef]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight Loss with a Low-Carbohydrate, Mediterranean, or Low-Fat Diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [PubMed] [Green Version]


{kind=link}
| Dietary Pattern | Description | Foods Included |
|---|---|---|
| Low-carbohydrate (LC) diet [26], Very-low carbohydrate diet (VLCD) [26], Paleolithic (paleo) [27], High protein diets (HPD) [28] | LC diet focus on restricting foods high in CHO. There are various levels of CHO restriction–i.e., LC is defined as <26% of total energy (TE) from CHO per day (equates to <130 g/day for an 8360 kJ/day). VLCD is defined as <10% of TE from CHO per day (equates to <50 g/day for an 8360 kJ/day. Paleolithic diets and high protein diets tend to resemble LC because some CHO is replaced by protein. | LC diets promote low-carbohydrate (CHO) vegetables, some low starch fruits and restrict starchy foods, grains, added sugars, lean protein foods, and foods rich in healthy fats and oils. Paleo diets are based on lean meat, fish, fruit, vegetables, eggs, nuts and exclude dairy products, cereal grains, legumes, fats, refined sweets, and sugar. HPD usually replace CHO dense foods with protein and may be low or high in saturated fat. |
| Mediterranean-style diet (M) [29,30,31,32], including Traditional Mediterranean (TM) and diets high in monounsaturated fatty acids (MUFA) [33] | The M diet reflects diets from the Mediterranean, rich in plant-based foods, olive oil, and fish. TM diets closely follow traditional foods and are used in LC studies as low CHO (LCTM). Energy ranges of 10–55% (TE) from CHO per day, 30–45% (TE) from fat per day (10–50% MUFA) [32,33,34]. High MUFA diets are based on Mediterranean-style eating, including a moderate intake of olive oil (and nuts) and are compared to high CHO control diets. | All emphasise a high intake of unrefined cereals, vegetables, legumes, fruits, nuts, and olive oil, low amounts of saturated fats, a moderately high intake of fish, a low-to-moderate intake of dairy products (cheese or yogurt), eggs and poultry, and a low intake of red meat. M and TM diets include regular but moderate wine consumption with meals. |
| Plant-based (PB) diet, vegetarian, or vegan diets [34,35,36,37,38] | Plant-based diets focus predominately on eating whole foods from plants, and most exclude meat, poultry, and seafood (or products containing these foods). Energy ranges of 50–78% (TE) from CHO per day, 10–35% fat per day. There are different classifications of Plant-based diets with various inclusions and exclusions and varying daily quantities of foods. | Diets include vegan diets without animal products or bi-products, Lacto includes dairy foods, ovo-lacto contains dairy foods and eggs. Vegetarian diets contain fruits, vegetables (legumes), bread, cereals, dairy products or alternatives, and healthy fats. Semi-vegetarians or flexitarians eat selected animal products sometimes. |
| Low-glycaemic Index (LGI) [39,40] diet | LGI promotes CHO foods that are less likely to produce significant increases in blood glucose levels. Energy ranges of 37–50% (TE) from CHO per day (GI < 55, 25–42% fat per day. LGI foods are assigned a value as ‘low’ when GI is 55 or less (some studies LGI is assigned 40) compared to high GI foods with a value of 70 or over. | Features include swapping high GI foods for whole, less processed CHO foods with a low–glycaemic index, such as oats, legumes, green vegetables, and other LGI food options from different food groups (i.e., whole grain cereals). |
| Dietary Approaches to Stop Hypertension (DASH) [41] | The DASH diet is a balanced eating plan limiting sodium, saturated fat, and added sugars. Initially created to lower blood pressure, the approach is used to amend eating habits and reduce cardiovascular disease. | Focuses on intake of fruits, vegetables, low-fat dairy; includes whole grains, poultry, fish, nuts; and supports the reduction in red meat, sweets, sugary beverages, total fat, saturated fat, and cholesterol. Sodium is reduced to 1500–2300 mg/day. |
| Intermittent fasting diet (IFD) [42,43] | Consists of periods of no and limited calorie intake. Diets generally consist of fasting for 16 h a day, a 24 h period on alternate days, or two days a week. | Comprises of eating less food (restricting); based on omitting food or types of food eaten for certain periods of time. |
| Low-fat diet (LFD) [44,45,46] | A diet with an overall reduction in fat, reducing total energy to promote health and weight loss. Recently, it has been used as a control or usual diet to compare specific food-based dietary patterns. | Reducing total daily fat intake to approximately 20% of energy (kilocalories) by increasing the daily intake of vegetables, fruits, and grains. Higher daily intake of CHO and protein foods. |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Dietary or dietary patterns for diabetes; human studies; adults ≥18 years; systematic reviews that included randomised control trials (RCTs) reporting on health outcomes with an appropriate comparator. | Children; adolescent; youth; aged <18 yrs; pregnancy; gestational diabetes; nutritional supplements; isolated foods or nutrients; acute trials; drug trials; animal studies. |
| Primary outcome of Haemoglobin A1c (HbA1c) with or without other indices of glycaemic control (i.e., fasting blood glucose (FBG), fasting or non-fasting insulin (FBI)). | Nutritional supplements; isolated foods or nutrients; acute trials; drug trials; animal studies; renal or kidney disease; cancer; palliative care. |
| Secondary findings of weight loss, blood pressure, and blood lipids (total-cholesterol (TC), low density lipoproteins (LDL), high density lipoproteins (HDL) and triglycerides (TG)). | Weight loss surgery or weight loss as single aim. Letters; editorials; commentaries; foreign language studies. |
| Search terms | |
| [MeSH terms] Dietary = #1 [Publication date 10 years] | |
| Advanced–Builder–History: Add #2 Dietary [MeSH terms] | |
| [All fields] #2 AND [All Fields] “Dietary Approaches to Stop Hypertension” OR [All Fields] DASH OR [All Fields] “Intermittent fasting” OR [All Fields] “Time-restricted feeding” OR [All Fields] “Low-carbohydrate” OR [All Fields] Ketogenic OR [All Fields] “High protein” OR [All Fields] Paleo OR [All Fields] “Low-fat” OR [All Fields] “High carbohydrate” OR [All Fields] “Low-glycaemic” OR [All Fields] “High fibre” OR [All Fields] Prudent OR [All Fields] Mediterranean OR [All Fields] MUFA OR [All Fields] Nordic OR [All Fields] Vegetarian OR Portfolio OR Flexitarian OR Vegan = #3 | |
| [All Fields] diabetes OR [MeSH terms] diabetes = #4 | |
| [Title]–“systematic review” OR [Abstract]–“systematic review” = #5 | |
| [Title] glycaemic OR [Title] glycaemic OR [Title] HbA1c OR glycaemic [Abstract] glycaemic OR [Abstract] HbA1c [Abstract] = #6 | |
| Note: Search terms developed for PubMed Central searches were followed for all databases | |
| PICO strategy | |
| Abbreviation-Description | Search components used to review evidence |
| P-Population | Adults living with diabetes |
| I-Intervention | Adoption of specific dietary patterns that improve glycaemia |
| C-Comparator | Control or usual diet for diabetes |
| O-Outcomes | The primary effects of dietary patterns on glycaemic control and inclusion of secondary findings |
| (T)-Type of study | Systematic reviews (with or without meta-analysis) |
| Type of Dietary Pattern | |||
|---|---|---|---|
| Low-Carbohydrate | Mediterranean | Plant-Based | Low-Glycaemic Index |
| Systematic reviews with meta-analysis | |||
| Fan, 2016 [51] Goldenberg, 2021 [61] Huntriss, 2018 [45] Jamka, 2020 a [27] Korsmo-Haugen, 2019 [52] Li, 2021 [62] McArdle, 2019 [53] Meng, 2017 [54] Naude, 2014 [55] Sainsbury, 2018 [56] Snorgaard, 2017 [57] van Zuuren, 2018 [44] Yu, 2020 b [58] Ajala, 2013 e [34] | Esposito, 2015 [63] Huo, 2015 [32] Qian, 2016 c [33] Ajala, 2013 e [34] | Viguiliouk, 2015 d [66] Viguiliouk, 2019 d [67] Yokoyama, 2014 [68] | Ojo, 2019 [39] Zafar, 2019 d [71] Ajala, 2013 e [34] |
| Systematic reviews (without meta-analysis) | |||
| Malaeb, 2019 b [28] Yamada, 2018 [59] Emadian, 2015 e [50] Papamichou, 2019 e [31] | Sleiman, 2015 [65] de Carvalho, 2020 e [49] Emadian, 2015 e [50] Papamichou, 2019 e [31] | Toumpanakis, 2018 [69] Johannesen, 2020 [70] de Carvalho, 2020 e [49] Emadian, 2015 e [50] Papamichou, 2019 e [31] | Emadian, 2015 e [50] Papamichou, 2019 e [31] |
| Type of Dietary Pattern | ||||
|---|---|---|---|---|
| Low-carbohydrate | Mediterranean | Plant-based | Low-glycaemic Index | |
| No. of reviews | n = 14 * | n = 4 * | n = 3 | n = 3 * |
| Glycaemic control | ||||
| HbA1c | 6 Sig favour * MD −0.3% [51], −0.3% [45], −0.4% [54], −0.1% [34], −0.5% [61], −0.4% [62]. 4 Favour, NS MD −0.1% [52], −0.1% [56], −0.04% [57], −0.2% [44]. 4 No difference, NS [27,53,55,58] | 3 Sig favour * MD −0.3% [32], −0.5% [63], −0.5% [34] 1 Favour, NS MD −0.1% [33] | 3 Sig favour MD −0.2% [66], −0.3% [67], −0.4% [68] | 2 Sig favour * MD −0.2% [71], −0.5% [34] 1 Favour, NS MD −0.5% [39] |
| FBG | 5 No difference, NS [27,44,54,58,61] 9 NR * [34,45,51,52,53,55,56,57,62] | 2 Sig favour MD −0.7 mmol/L [56] −0.6 mmol/L [57] 2 NR * [34,63] | 2 Sig favour MD −0.5 mmol/L [66], MD −0.6 mmol/L [67] 1 No difference [68], NS | 2 Sig favour MD −0.2 mmol/L [71], −0.5 mmol/L [39] 1 NR * [34] |
| FBI | 1 No difference, NS [27] 13 NR * [34,44,45,51,52,53,54,55,56,57,58,61,62] | 1 Favour, NS MD −0.6 mU/L [32] 1 No difference, NS [33] 2 NR * [34,63] | 1 Sig favour WMD −1.5 mU/L [66] 2 NR [67,68] | 1 No difference, NS [71] 2 NR * [34,39] |
| Type of Dietary Pattern | ||||
|---|---|---|---|---|
| Low-carbohydrate (LC) | Mediterranean (M) | Plant-based (PB) | Low-glycaemic Index (LGI) | |
| Body weight | n = 14 * | n = 4 * | n = 3 | n = 3 * |
| 4 Sig favour * MD −0.7 kg [34], −2.3 kg [51], −3.5 kg [61], −3 kg [62] 1 Favour, NS [52] 8 No difference, NS [27,44,45,53,54,55,56,57] 1 NR [58] | 2 Sig favour * MD −1.6 kg [33], −1.8 kg [34] 1 Favour, NS [32] 1 No difference, NS [63] | 1 Sig favour MD −2.2 kg [67] 1 No difference, NS [68] 1 NR [66] | 2 No difference, NS * [34,71] 1 NR [39] | |
| Blood pressure | n = 7 | n = 2 | n = 1 | n = 0 |
| Systolic | 1 Sig favour MD −2.7 mm/Hg [45] 6 No difference, NS [44,52,55,56,58,62] | 1 Sig favour MD −2.3 mmHg [33] 1 Favours, NS [32] | 1 No difference, NS [67] | |
| Diastolic | 7 No difference, NS [44,45,52,55,56,58,62] | 1 Favour, NS [32] 1 No difference, NS [33] | 1 No difference, NS [67] | |
| Blood lipids | n = 12 * | n = 3 * | n = 1 | n = 2 * |
| TC | 1 Sig favour MD 0.2 mmol/L [58] 1 Favour, NS [45] 8 No difference, NS * [34,51,52,54,55,56,61,62] 2 NR [44,57] | 1 Sig favour MD −0.1 mmol/L [32] 2 NR * [33,34] | 1 NR [67] | 1 No difference, NS [71] 1 NR* [34] |
| LDL | 1 Sig favour MD −0.1 mmol/L [58] 11 No difference, NS * [44,45,51,52,54,55,56,57,61,62] | 3 No difference, NS * [32,33,34] | 1 Sig favour MD −0.12 mmol/L [67] | 2 No difference, NS * [34,71] |
| HDL | 5 Sig favour * MD 0.09 mmol/L [51], 0.06 mmol/L [45], 0.07 mmol/L [54], 0.08 mmol/L [34], 0.09 mmol/L [62] 1 Favour, NS [44] 5 No difference, NS [52,55,56,58,61] 1 NR [57] | 2 Sig favour * MD 0.06 mmol/L [33], 0.04 mmol/L [34]. 1 Favour, NS [32] | 1 No difference, NS [67] | 1 Sig favour * MD 0.05 [34] 1 No difference, NS [71] |
| TG | 4 Sig favour MD −0.3 mmol/L [51], −0.2 mmol/L [45], −0.2 mmol/L [58]. −0.2 mmol/L [62] 2 Favour, NS [44,52] 5 No difference, NS * [34,54,55,56,61] 1 NR [57] | 3 Sig favour * MD −0.3 mmol/L [32], −0.3 mmol/L [33] −0.2 mmol/L (35). | 1 No difference, NS [67] | 2 No difference, NS * [34,71] |
| Health Benefits | HbA1c Reduction | FBG Reduction | Weight Loss | Lowered BP | Reduced TC/TG | Improved HDL |
|---|---|---|---|---|---|---|
| Low-carbohydrate | ✓ | * | ✓ | ✓ | ✓ | ✓ |
| Mediterranean | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Plant-based | ✓ | ✓ | ✓ | * | * | * |
| Low-glycaemic Index | ✓ | ✓ | * | * | * | ✓ |
| Low-Carbohydrate | Mediterranean | Plant-Based | Low-Glycaemic Index | |||||
|---|---|---|---|---|---|---|---|---|
| No. of Reviews | n = 14 * | n = 4 * | n = 3 | n = 3 * | ||||
| Quality | Risk of Bias | Quality | Risk of Bias | Quality | Risk of Bias | Quality | Risk of Bias | |
| 0 High | 2 Low | 1 High | 3 Low | 0 High | 0 Low | 0 High | 1 Low | |
| 6 Moderate * | 11 Unclear * | 3 Moderate * | 1 Unclear * | 1 Moderate | 3 Unclear | 2 Moderate * | 2 Unclear * | |
| 8 Low | 1 High | 0 Low | 0 High | 2 low | 0 High | 1 Low | 0 High | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whiteley, C.; Benton, F.; Matwiejczyk, L.; Luscombe-Marsh, N. Determining Dietary Patterns to Recommend for Type 2 Diabetes: An Umbrella Review. Nutrients 2023, 15, 861. https://doi.org/10.3390/nu15040861
Whiteley C, Benton F, Matwiejczyk L, Luscombe-Marsh N. Determining Dietary Patterns to Recommend for Type 2 Diabetes: An Umbrella Review. Nutrients. 2023; 15(4):861. https://doi.org/10.3390/nu15040861
Chicago/Turabian StyleWhiteley, Cathryn, Fiona Benton, Louisa Matwiejczyk, and Natalie Luscombe-Marsh. 2023. "Determining Dietary Patterns to Recommend for Type 2 Diabetes: An Umbrella Review" Nutrients 15, no. 4: 861. https://doi.org/10.3390/nu15040861
APA StyleWhiteley, C., Benton, F., Matwiejczyk, L., & Luscombe-Marsh, N. (2023). Determining Dietary Patterns to Recommend for Type 2 Diabetes: An Umbrella Review. Nutrients, 15(4), 861. https://doi.org/10.3390/nu15040861