
Adherence to the Mediterranean Diet and Ultra-Processed Foods Consumption in a Group of Italian Patients with Celiac Disease

 ,
,  , , , ,
, , , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. NOVA Food Frequency Questionnaire (NFFQ)
2.3. The Medi-Lite Adherence Score
2.4. Statistical Analysis
3. Results
3.1. Ultra-Processed Foods’ Consumption
3.2. Adherence to the Mediterranean Diet
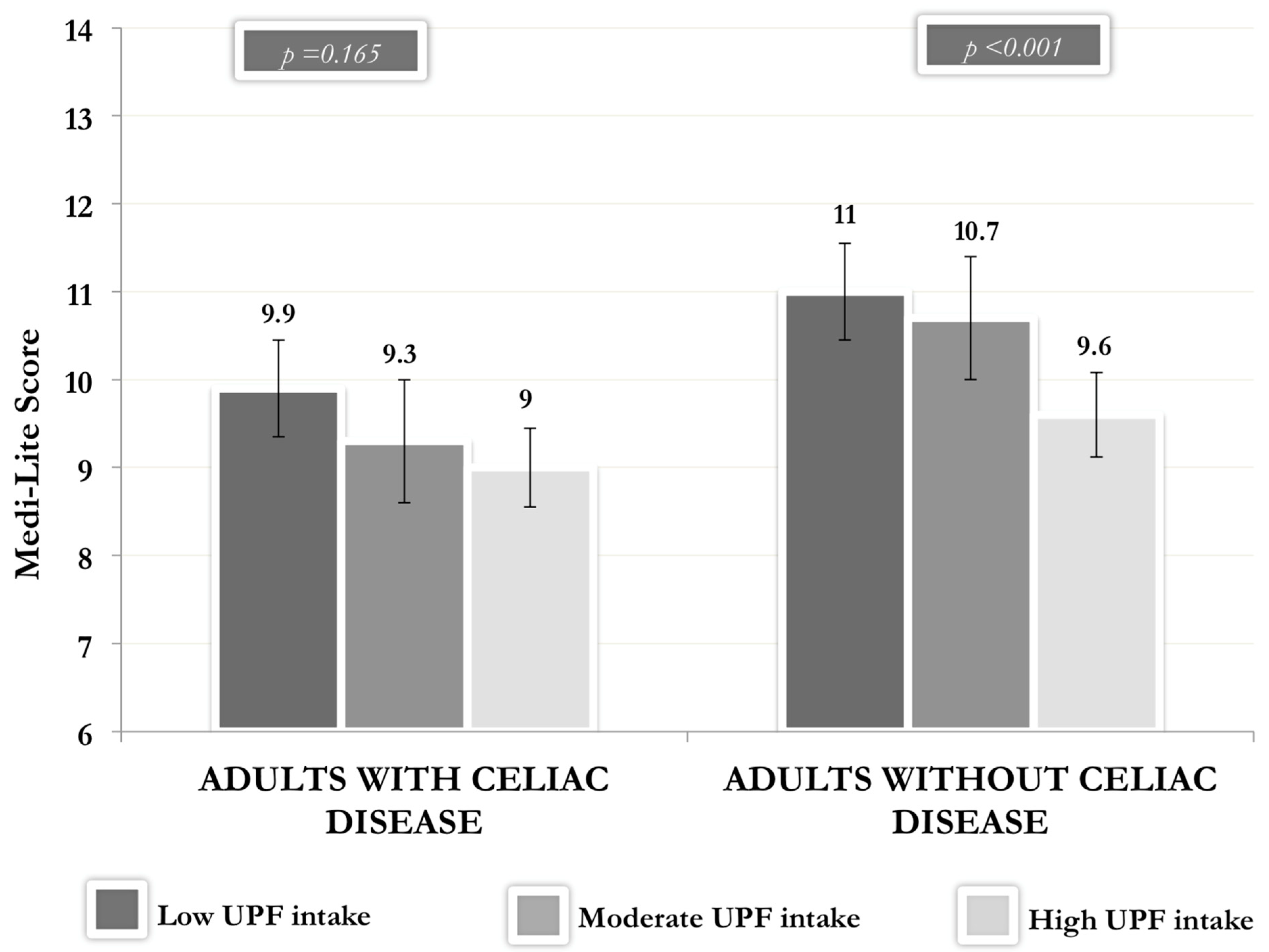
3.3. Ultra-Processed Foods’ Consumption and Adherence to the Mediterranean Diet
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.; Hadjivassiliou, M.; Holdoway, A.; van Heel, D.A.; et al. Diagnosis and management of adult coeliac disease: Guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef] [PubMed]
- Cardo, A.; Churruca, I.; Lasa, A.; Navarro, V.; Vázquez-Polo, M.; Perez-Junkera, G.; Larretxi, I. Nutritional Imbalances in Adult Celiac Patients Following a Gluten-Free Diet. Nutrients 2021, 13, 2877. [Google Scholar] [CrossRef]
- Fry, L.; Madden, A.M.; Fallaize, R. An investigation into the nutritional composition and cost of gluten-free versus regular food products in the UK. J. Hum. Nutr. Diet. 2018, 31, 108–120. [Google Scholar] [CrossRef]
- Larretxi, I.; Simon, E.; Benjumea, L.; Miranda, J.; Bustamante, M.A.; Lasa, A.; Eizaguirre, F.J.; Churruca, I. Gluten-free-rendered products contribute to imbalanced diets in children and adolescents with celiac disease. Eur. J. Nutr. 2019, 58, 775–783. [Google Scholar] [CrossRef]
- Babio, N.; Lladó Bellette, N.; Besora-Moreno, M.; Castillejo, G.; Guillén, N.; Martínez-Cerezo, F.; Vilchez, E.; Roger, E.; Hernández-Alonso, P.; Salas Salvadó, J. A comparison of the nutritional profile and price of gluten-free products and their gluten-containing counterparts available in the Spanish market. Nutr. Hosp. 2020, 37, 814–822. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez- Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Martínez Steele, E.; Baraldi, L.G.; da Costa Louzada, M.; Moubarac, J.C.; Mozaffarian, D.; Monteiro, C.A. Ultra-processed foods and added sugars in the US diet: Evidence from a nationally representative cross-sectional study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef]
- Steele, E.M.; Marrón Ponce, J.A.; Cediel, G.; Louzada, M.L.C.; Khandpur, N.; Machado, P.; Moubarac, J.C.; Rauber, F.; Corvalán, C.; Levy, R.B.; et al. Potential reductions in ultra-processed food consumption substantially improve population cardiometabolic-related dietary nutrient profiles in eight countries. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2739–2750. [Google Scholar] [CrossRef]
- Batal, M.; Johnson-Down, L.; Moubarac, J.C.; Ing, A.; Fediuk, K.; Sadik, T.; Tikhonov, C.; Chan, L.; Willows, N. Quantifying associations of the dietary share of ultra-processed foods with overall diet quality in First Nations peoples in the Canadian provinces of British Columbia, Alberta, Manitoba and Ontario. Public Health Nutr. 2018, 21, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Morreale, F.; Agnoli, C.; Roncoroni, L.; Sieri, S.; Lombardo, V.; Mazzeo, T.; Elli, L.; Bardella, M.T.; Agostoni, C.; Doneda, L.; et al. Are the dietary habits of treated individuals with celiac disease adherent to a Mediterranean diet? Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1148–1154. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Nestares, T.; Martín-Masot, R.; Flor-Alemany, M.; Bonavita, A.; Maldonado, J.; Aparicio, V.A. Influence of Ultra-Processed Foods Consumption on Redox Status and Inflammatory Signaling in Young Celiac Patients. Nutrients 2021, 13, 156. [Google Scholar] [CrossRef]
- Suárez-González, M.; Bousoño García, C.; Jiménez Treviño, S.; Iglesias Cabo, T.; Díaz Martín, J.J. Influence of nutrition education in paediatric coeliac disease: Impact of the role of the registered dietitian: A prospective, single-arm intervention study. J. Hum. Nutr. Diet. 2020, 33, 775–785. [Google Scholar] [CrossRef]
- Lionetti, E.; Antonucci, N.; Marinelli, M.; Bartolomei, B.; Franceschini, E.; Gatti, S.; Catassi, G.N.; Verma, A.K.; Monachesi, C.; Catassi, C. Nutritional Status, Dietary Intake, and Adherence to the Mediterranean Diet of Children with Celiac Disease on a Gluten-Free Diet: A Case-Control Prospective Study. Nutrients 2020, 12, 143. [Google Scholar] [CrossRef]
- SurveyMonkey. Available online: https://www.surveymonkey.com/ (accessed on 31 September 2022).
- Dinu, M.; Bonaccio, M.; Martini, D.; Madarena, M.P.; Vitale, M.; Pagliai, G.; Esposito, S.; Ferraris, C.; Guglielmetti, M.; Rosi, A.; et al. Reproducibility and validity of a food-frequency questionnaire (NFFQ) to assess food consumption based on the NOVA classification in adults. Int. J. Food. Sci. Nutr. 2021, 72, 861–869. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef]
- Sofi, F.; Dinu, M.; Pagliai, G.; Marcucci, R.; Casini, A. Validation of a literature-based adherence score to Mediterranean diet: The MEDI-LITE score. Int. J. Food. Sci. Nutr. 2017, 68, 757–762. [Google Scholar] [CrossRef]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef]
- Ferrara, P.; Cicala, M.; Tiberi, E.; Spadaccio, C.; Marcella, L.; Gatto, A.; Calzolari, P.; Castellucci, G. High fat consumption in children with celiac disease. Acta Gastro-Enterol. Belg. 2009, 72, 296–300. [Google Scholar]
- Zuccotti, G.; Fabiano, V.; Dilillo, D.; Picca, M.; Cravidi, C.; Brambilla, P. Intakes of nutrients in Italian children with celiac disease and the role of commercially available gluten-free products. J. Hum. Nutr. Diet. 2013, 26, 436–444. [Google Scholar] [CrossRef]
- Spychaj, A.; Pospiech, E.; Iwanska, E.; Montowska, M. Detection of allergenic additives in processed meat products. J. Sci. Food. Agric. 2018, 98, 4807–4815. [Google Scholar] [CrossRef]
- Ruggiero, E.; Esposito, S.; Costanzo, S.; Di Castelnuovo, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Bonaccio, M.; INHES Study Investigators. Ultra-processed food consumption and its correlates among Italian children, adolescents and adults from the Italian Nutrition & Health Survey (INHES) cohort study. Public Health Nutr. 2021, 24, 6258–6271. [Google Scholar] [CrossRef]
- Perez-Junkera, G.; Vázquez-Polo, M.; Eizagirre, F.J.; Benjumea, L.; Tutau, C.; Esteban, B.; Miranda, J.; Larretxi, I.; Navarro, V.; Churruca, I.; et al. Application of a Platform for Gluten-Free Diet Evaluation and Dietary Advice: From Theory to Practice. Sensors 2022, 22, 732. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Notarnicola, M.; Cisternino, A.M.; Inguaggiato, R.; Guerra, V.; Reddavide, R.; Donghia, R.; Rotolo, O.; Zinzi, I.; Leandro, G.; et al. Trends in adherence to the Mediterranean diet in South Italy: A cross sectional study. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 410–417. [Google Scholar] [CrossRef]
- Da Silva, R.; Bach-Faig, A.; Quintana, B.R.; Buckland, G.; de Almeida, M.D.V.; Serra-Majem, L. Worldwide variation of adherence to the Mediterranean diet, in 1961-1965 and 2000-2003. Public Health Nutr. 2009, 12, 1676–1684. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72, 83–91. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef]
- Dinu, M.; Asensi, M.T.; Pagliai, G.; Lotti, S.; Martini, D.; Colombini, B.; Sofi, F. Consumption of Ultra-Processed Foods Is Inversely Associated with Adherence to the Mediterranean Diet: A Cross-Sectional Study. Nutrients 2022, 14, 2073. [Google Scholar] [CrossRef]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Suárez-González, M.; Bousoño-García, C.; Jiménez-Treviño, S.; Díaz-Martín, J.J. Gluten-Free Diet: Nutritional Strategies to Improve Eating Habits in Children with Celiac Disease: A Prospective, Single-arm Intervention Study. Nutrients 2021, 13, 1108. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Adults with Celiac Disease (n = 103) | Adults without Celiac Disease (n = 312) | p-Value | |
|---|---|---|---|
| Age (years) | 40.4 ± 12.6 | 39.3 ± 13.3 | 0.471 |
| Gender, n (% women) | 89 (86.4) | 261 (83.7) | 0.505 |
| Body weight (kg) | 63.4 ± 12.1 | 64.8 ± 14 | 0.823 |
| BMI (kg/m2) | 23.2 ± 4.2 | 23.1 ± 4.1 | 0.740 |
| BMI ≥ 25, n (%) | 25 (24) | 78 (25.0) | 0.882 |
| Education level | |||
| Secondary school, n (%) | 10 (9.7) | 14 (4.5) | 0.049 |
| High school, n (%) | 36 (35) | 133 (42.6) | 0.169 |
| University degree, n (%) | 57 (55.3) | 165 (52.9) | 0.206 |
| Civil status | |||
| Single, n (%) | 37 (35.9) | 131 (42) | 0.276 |
| Married/partner, n (%) | 61 (59.2) | 150 (48.1) | 0.050 |
| Divorced/Widowed, n (%) | 5 (4.9) | 31(10) | 0.112 |
| Years of disease | 11.4 ± 8.6 | - | - |
| Adults with Celiac Disease (n = 103) | Adults without Celiac Disease (n = 312) | p-Value | |
|---|---|---|---|
| Vegetables and legumes UPF | 15.9 (5.4–26.4) | 30.1 (24.1–36.2) | 0.021 |
| Ready-to-heat vegetables and legumes (with added ingredients) | 15.9 (5.4–26.4) | 30.1 (24.1–36.2) | 0.021 |
| Cereals and tubers UPF | 66.5 (57.0–75.9) | 56.2 (50.8–61.6) | 0.066 |
| Ready-to-heat pasta/gnocchi dishes | 9.7 (7.2–12.1) | 6.6 (5.1–8.0) | 0.033 |
| Pre-packaged breads and bread alternatives | 26.3 (21.7–30.9) | 19.6 (17.0–22.2) | 0.012 |
| Pre-packaged pizza, focaccia, sandwich, and savory pies | 15.9 (11.6–20.2) | 13.0 (10.5–15.5) | 0.254 |
| Breakfast cereals and energy bars (with added sugar) | 5.1 (3.0–7.1) | 5.6 (4.4–6.8) | 0.667 |
| Pre-packaged potatoes, croquets, and instant soups | 9.2 (6.0–12.3) | 11.1 (9.3–13.0) | 0.292 |
| Meat and fish UPF | 8.7 (6.1–11.2) | 12.2 (10.8–13.8) | 0.016 |
| Nuggets, sticks, sausages, burgers, and other reconstituted meat products | 7.5 (5.3–9.8) | 10.2 (8.9–11.5) | 0.043 |
| Fish nuggets, fish sticks, and other reconstituted fish products | 1.1 (0.3–1.9) | 2.1 (1.6–2.5) | 0.043 |
| Milk and dairy products UPF | 28.6 (19.9–37.3) | 33.4 (28.4–38.4) | 0.346 |
| Milk beverages (e.g., probiotic milk with added sugar) | 6.4 (1.7–11.1) | 7.9 (5.2–10.6) | 0.579 |
| Fruit or flavored yogurts (e.g., vanilla flavored) | 20.6 (13.4–27.8) | 23.9 (19.8–28.1) | 0.431 |
| Melted cheese (also used as a sandwich filling) | 1.6 (1.0–2.2) | 1.6 (1.2–1.9) | 0.949 |
| Fats and seasoning UPF | 4.9 (3.5–6.2) | 5.2 (4.5–6.0) | 0.654 |
| Margarines and other spreads, or instant sauces (e.g., mayonnaise, ketchup) | 4.9 (3.5–6.2) | 5.2 (4.5–6.0) | 0.654 |
| Sweets and Sweeteners UPF | 51.4 (44.4–58.4) | 45.8 (41.7–49.8) | 0.173 |
| Pre-packaged biscuits, cakes, snacks, and ice-cream | 38.4 (32.1–44.7) | 33.3 (29.7–36.9) | 0.169 |
| Chocolate, spreads (e.g., nut spread), and candies | 13.0 (10.2–15.8) | 12.4 (10.8–14.0) | 0.740 |
| Beverages UPF | 36.9 (24.9–49.0) | 46.3 (39.4–53.2) | 0.186 |
| Alcoholic beverages, soft and energy drinks (e.g., iced tea, coke) | 36.9 (24.9–49.0) | 46.3 (39.4–53.2) | 0.186 |
| Other UPF | 26.6 (17.3–35.8) | 19.9 (14.6–25.1) | 0.216 |
| Plant-based dairy substitutes (e.g., soy drinks) | 25.0 (16.3–33.7) | 16.9 (11.9–21.9) | 0.112 |
| Plant-based meat substitutes (e.g., veggie burger) | 1.6 (0.2–3.0) | 3.0 (2.2–3.8) | 0.078 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tristan Asensi, M.; Pagliai, G.; Lotti, S.; Corrao, A.; Colombini, B.; Giangrandi, I.; Sofi, F.; Dinu, M. Adherence to the Mediterranean Diet and Ultra-Processed Foods Consumption in a Group of Italian Patients with Celiac Disease. Nutrients 2023, 15, 938. https://doi.org/10.3390/nu15040938
Tristan Asensi M, Pagliai G, Lotti S, Corrao A, Colombini B, Giangrandi I, Sofi F, Dinu M. Adherence to the Mediterranean Diet and Ultra-Processed Foods Consumption in a Group of Italian Patients with Celiac Disease. Nutrients. 2023; 15(4):938. https://doi.org/10.3390/nu15040938
Chicago/Turabian StyleTristan Asensi, Marta, Giuditta Pagliai, Sofia Lotti, Abigail Corrao, Barbara Colombini, Ilaria Giangrandi, Francesco Sofi, and Monica Dinu. 2023. "Adherence to the Mediterranean Diet and Ultra-Processed Foods Consumption in a Group of Italian Patients with Celiac Disease" Nutrients 15, no. 4: 938. https://doi.org/10.3390/nu15040938
APA StyleTristan Asensi, M., Pagliai, G., Lotti, S., Corrao, A., Colombini, B., Giangrandi, I., Sofi, F., & Dinu, M. (2023). Adherence to the Mediterranean Diet and Ultra-Processed Foods Consumption in a Group of Italian Patients with Celiac Disease. Nutrients, 15(4), 938. https://doi.org/10.3390/nu15040938