
Effect of Lactoferrin on Clinical Outcomes of Hospitalized Patients with COVID-19: The LAC Randomized Clinical Trial
 , , ,
, , ,  , ,
, ,  , , , , ,
, , , , ,  ,
,  ,
,  , ,
, ,  , , , and add
Show full author list
, , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Study Design
2.2. Population
2.3. Randomization
2.4. Intervention
2.5. Safety
2.6. Clinical and Laboratory Monitoring
2.7. Data Management
2.8. Definition of Endpoints
2.9. Sample Size
2.10. Statistical Analysis
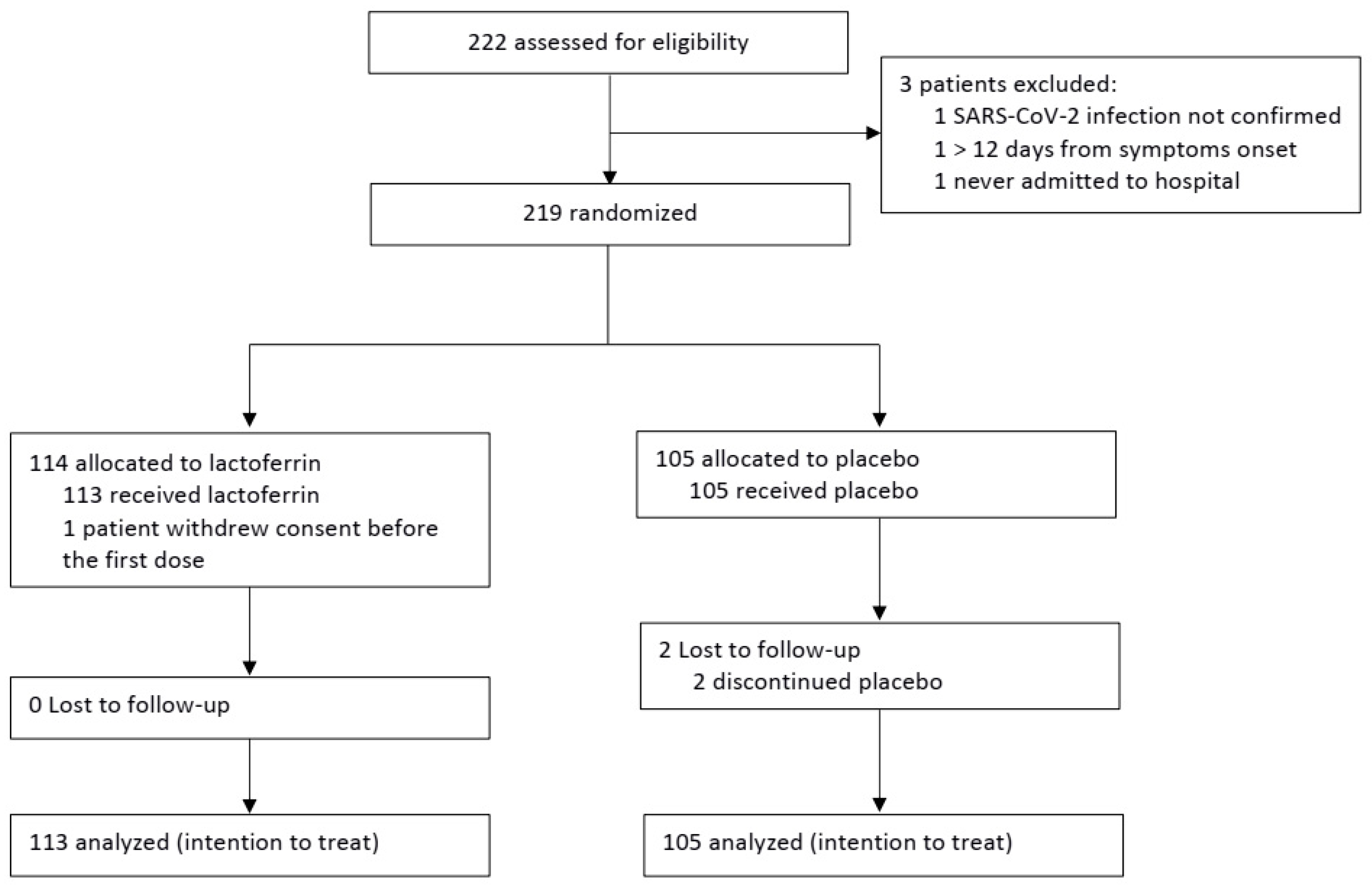
3. Results
3.1. Primary Outcomes
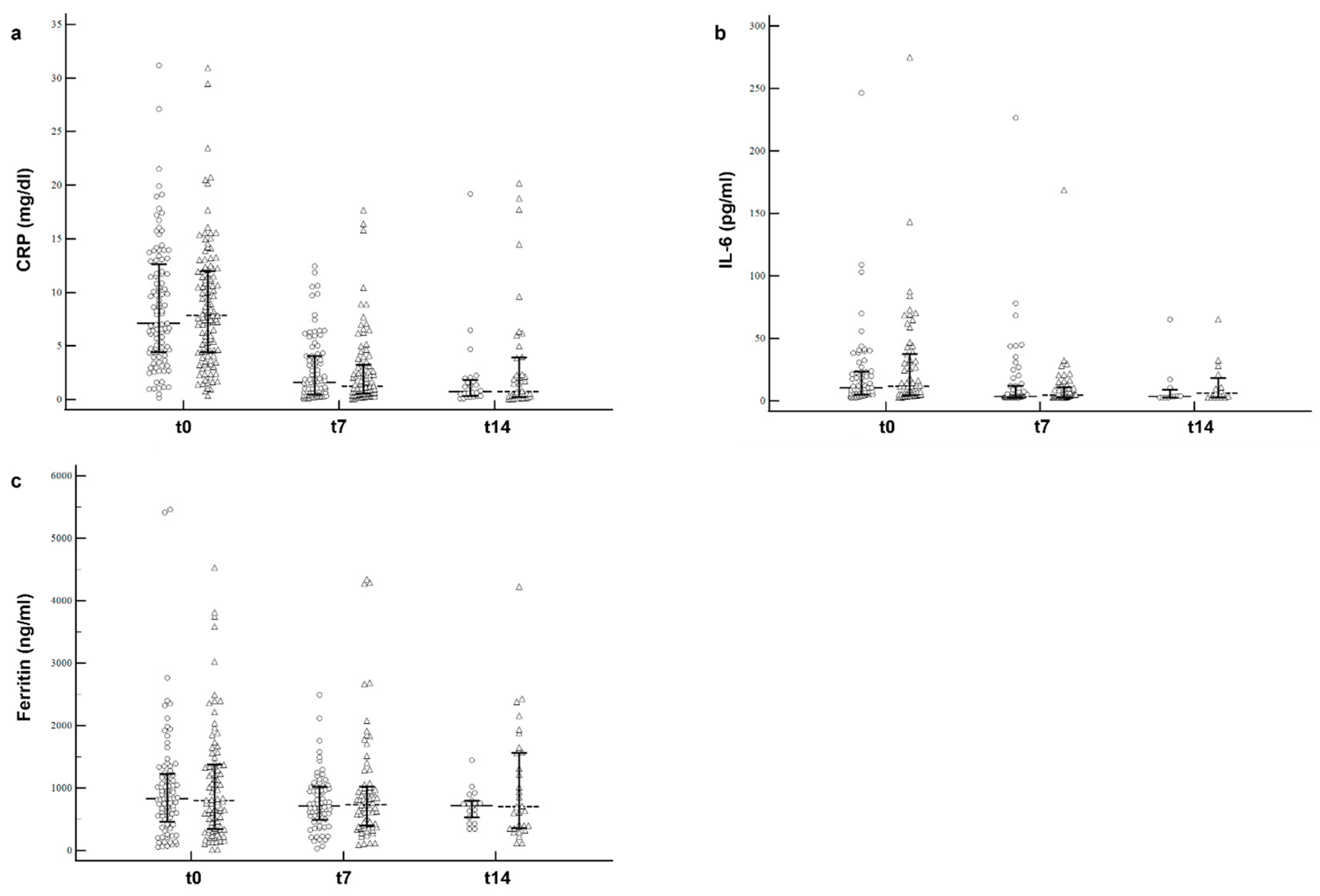
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Shafqat, A.; Shafqat, S.; Al Salameh, S.; Kashir, J.; Alkattan, K.; Yaqinuddin, A. Mechanistic Insights into the Immune Pathophysiology of COVID-19; An In-Depth Review. Front. Immunol. 2022, 13, 835104. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Osuchowski, M.F.; Winkler, M.S.; Skirecki, T.; Cajander, S.; Shankar-Hari, M.; Lachmann, G.; Monneret, G.; Venet, F.; Bauer, M.; Brunkhorst, F.M.; et al. The COVID-19 puzzle: Deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir. Med. 2021, 9, 622–642. [Google Scholar] [CrossRef]
- Cabaro, S.; D’Esposito, V.; Di Matola, T.; Sale, S.; Cennamo, M.; Terracciano, D.; Parisi, V.; Oriente, F.; Portella, G.; Beguinot, F.; et al. Cytokine signature and COVID-19 prediction models in the two waves of pandemics. Sci. Rep. 2021, 11, 20793. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Zhang, W.; Zhang, F.; Huang, C.; Yang, M.; Tang, Z.; Li, Y.; Mi, J.; Zhong, W. Prognostic Role and Diagnostic Power of Seven Indicators in COVID-19 Patients. Front. Med. 2021, 8, 733274. [Google Scholar] [CrossRef]
- Wen, W.; Chen, C.; Tang, J.; Wang, C.; Zhou, M.; Cheng, Y.; Zhou, X.; Wu, Q.; Zhang, X.; Feng, Z.; et al. Efficacy and safety of three new oral antiviral treatment (molnupiravir, fluvoxamine and Paxlovid) for COVID-19: A meta-analysis. Ann. Med. 2022, 54, 516–523. [Google Scholar] [CrossRef]
- Dyer, O. Covid-19: Unvaccinated face 11 times risk of death from delta variant, CDC data show. BMJ 2021, 374, n2282. [Google Scholar] [CrossRef] [PubMed]
- Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Korompoki, E.; Fotiou, D.; Migkou, M.; Tzanninis, I.-G.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Emerging treatment strategies for COVID-19 infection. Clin. Exp. Med. 2021, 21, 167–179. [Google Scholar] [CrossRef]
- Izda, V.; Jeffries, M.A.; Sawalha, A.H. COVID-19: A review of therapeutic strategies and vaccine candidates. Clin. Immunol. 2021, 222, 108634. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov (accessed on 25 May 2022).
- Cairns, D.M.; Dulko, D.; Griffiths, J.K.; Golan, Y.; Cohen, T.; Trinquart, L.; Price, L.L.; Beaulac, K.R.; Selker, H.P. Efficacy of niclosamide vs placebo in SARS-CoV-2 respiratory viral clearance, viral shedding, and duration of symptoms among patients with mild to moderate COVID-19. A phase 2 randomized clinical trial. JAMA Netw. Open 2022, 5, e2144942. [Google Scholar] [CrossRef] [PubMed]
- Mirabelli, C.; Wotring, J.W.; Zhang, C.J.; McCarty, S.M.; Fursmidt, R.; Pretto, C.D.; Qiao, Y.; Zhang, Y.; Frum, T.; Kadambi, N.S.; et al. Morphological cell profiling of SARS-CoV-2 infection identifies drug repurposing candidates for COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2105815118. [Google Scholar] [CrossRef] [PubMed]
- Ricordi, C.; Pacifici, F.; Lanzoni, G.; Palamara, A.; Garaci, E.; Della-Morte, D. Dietary and Protective Factors to Halt or Mitigate Progression of Autoimmunity, COVID-19 and Its Associated Metabolic Diseases. Int. J. Mol. Sci. 2021, 22, 3134. [Google Scholar] [CrossRef]
- Habib, H.M.; Ibrahim, S.; Zaim, A.; Ibrahim, W.H. The role of iron in the pathogenesis of COVID-19 and possible treatment with lactoferrin and other iron chelators. Biomed. Pharmacother. 2021, 136, 111228. [Google Scholar] [CrossRef]
- Presti, S.; Manti, S.; Parisi, G.F.; Papale, M.; Barbagallo, I.A.; Li Volti, G.; Leonardi, S. Lactoferrin: Cytokine modulation and application in clinical partice. J. Clin. Med. 2021, 10, 5482. [Google Scholar] [CrossRef]
- Chang, R.; Ng, T.B.; Sun, W.-Z. Lactoferrin as potential preventative and adjunct treatment for COVID-19. Int. J. Antimicrob. Agents 2020, 56, 106118. [Google Scholar] [CrossRef]
- Lang, J.; Yang, N.; Deng, J.; Liu, K.; Yang, P.; Zhang, G.; Jiang, C. Inhibition of SARS Pseudovirus Cell Entry by Lactoferrin Binding to Heparan Sulfate Proteoglycans. PLoS ONE 2011, 6, e23710. [Google Scholar] [CrossRef] [PubMed]
- Rosa, L.; Cutone, A.; Conte, M.P.; Campione, E.; Bianchi, L.; Valenti, P. An overview on in vitro and in vivo antiviral activity of lactoferrin: Its efficacy against SARS-CoV-2 infection. BioMetals 2022, 1–20. [Google Scholar] [CrossRef]
- Wotring, J.W.; Fursmidt, R.; Ward, L.; Sexton, J.Z. Evaluating the in vitro efficacy of bovine lactoferrin products against SARS-CoV-2 variants of concern. J. Diary Sci. 2022, 105, 2791–2802. [Google Scholar] [CrossRef]
- Campione, E.; Lanna, C.; Cosio, T.; Rosa, L.; Conte, M.P.; Iacovelli, F.; Romeo, R.; Falconi, M.; Del Vecchio, C.; Franchin, E.; et al. Lactoferrin against SARS-COV-2: In Vitro and in silico evidences. Front. Pharmacol. 2021, 12, 666600. [Google Scholar] [CrossRef]
- Hu, Y.; Meng, X.; Zhang, F.; Xiang, Y.; Wang, J. The in vitro antiviral activity of lactoferrin against common human coronaviruses and SARS-CoV-2 is mediated by targeting the heparan sulfate co-receptor. Emerg. Microbes Infect. 2021, 10, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Salaris, C.; Scarpa, M.; Elli, M.; Bertolini, A.; Guglielmetti, S.; Pregliasco, F.; Blandizzi, C.; Brun, P.; Castagliuolo, I. Protective effects of lactoferrin against SARS-CoV-2 infection in vitro. Nutrients 2021, 13, 328. [Google Scholar] [CrossRef] [PubMed]
- Miotto, M.; Di Rienzo, L.; Bò, L.; Boffi, A.; Ruocco, G.; Milanetti, E. Molecular mechanisms behind anti SARS-CoV-2 action of lactoferrin. Front. Mol. Biosci. 2021, 8, 607443. [Google Scholar] [CrossRef]
- Rosa, L.; Tripepi, G.; Naldi, E.; Aimati, M.; Santangeli, S.; Venditto, F.; Caldarelli, M.; Valenti, P. Ambulatory COVID-19 Patients Treated with Lactoferrin as a Supplementary Antiviral Agent: A Preliminary Study. J. Clin. Med. 2021, 10, 4276. [Google Scholar] [CrossRef]
- Al-Alaiyan, S.; Abdulaziz, N.; Alkohlani, A.; Almairi, S.O.; Al Hazzani, F.; Binmanee, A.; Alfattani, A. Effects of Probiotics and Lactoferrin on Necrotizing Enterocolitis in Preterm Infants. Cureus 2021, 13, e18256. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, T.J.; Loli, S.; Mendoza, K.; Carcamo, C.; Bellomo, S.; Cam, L.; Castaneda, A.; Campos, M.; Jacobs, J.; Cossey, V.; et al. Effect of bovine lactoferrin on prevention of late-onset sepsis in infants < 1500 g: A pooled analysis of individual patient data from two randomized controlled trials. Biochem. Cell Biol. 2021, 99, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, T.J.; Zegarra, J.; Bellomo, S.; Carcamo, C.P.; Cam, L.; Castañeda, A.; Villavicencio, A.; Gonzales, J.; Rueda, M.S.; Turin, C.G.; et al. Randomized controlled trial of bovine lactoferrin for prevention of sepsis and neuro-development impairment in infants weighing less than 2000 grams. J. Pediatr. 2020, 219, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Tarnow-Mordi, W.O.; Abdel-Latif, M.E.; Martin, A.; Pammi, M.; Robledo, K.; Manzoni, P.; Osborn, D.; Lui, K.; Keech, A.; Hague, W.; et al. The effect of lactoferrin supplementation on death or major morbidity in very low birthweight infants (LIFT): A multicentre, double-blind, randomised controlled trial. Lancet Child Adolesc. Health 2020, 4, 444–454. [Google Scholar] [CrossRef]
- ELFIN Trial Investigators Group. Enteral lactoferrin supplementation for very preterm infants: A randomized place-bo-controlled trial. Lancet 2019, 393, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, J.; Jenkins, P.; Vargova, M.; Bowler, U.; Juszczak, E.; King, A.; Linsell, L.; Murray, D.; Partlett, C.; Patel, M.; et al. Enteral lactoferrin to prevent infection for very preterm infants: The ELFIN RCT. Health Technol. Assess. 2018, 22, 1–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, T.; Cai, K.; Yu, J. Prophylactic lactoferrin for preventing late-onset sepsis and necrotizing enterocolitis in preterm infants. A PRISMA-complaint systematic review and meta-analysis. Medicine 2018, 97, e11976. [Google Scholar] [CrossRef]
- Barrington, K.J.; Assaad, M.-A.; Janvier, A. The Lacuna Trial: A double-blind randomized controlled pilot trial of lactoferrin supplementation in the very preterm infant. J. Perinatol. 2016, 36, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Gatwala, G. Efficacy of bovine lactoferrin supplementation in preventing late-onset sepsis in low birth weight neo-nates: A randomized placebo-controlled clinical trial. J. Trop. Pediatr. 2015, 61, 370–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochoa, T.J.; Zegarra, J.; Cam, L.; Llanos, R.; Pezo, A.; Cruz, K.; Zea-Vera, A.; Cárcamo, C.; Campos, M.; Bellomo, S. Randomized Controlled Trial of Lactoferrin for Prevention of Sepsis in Peruvian Neonates Less than 2500 g. Pediatr. Infect. Dis. J. 2015, 34, 571–576. [Google Scholar] [CrossRef] [Green Version]
- Manzoni, P.; Meyer, M.; Stolfi, I.; Rinaldi, M.; Cattani, S.; Pugni, L.; Romeo, M.G.; Messner, H.; Decembrino, L.; Laforgia, N.; et al. Bovine lactoferrin supplementation for prevention of necrotizing enterocolitis in very-low-birth-weight neonates: A randomized clinical trial. Early Hum. Dev. 2014, 90, S60–S65. [Google Scholar] [CrossRef]
- Manzoni, P.; Rinaldi, M.; Cattani, S.; Pugni, L.; Romeo, M.G.; Messner, H.; Stolfi, I.; Decembrino, L.; Laforgia, N.; Vagnarelli, F.; et al. Bovine lactoferrin supplementation for prevention of late-onset sepsis in very low-birth-weight neonates: A randomized trial. JAMA 2009, 302, 1421–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campione, E.; Lanna, C.; Cosio, T.; Rosa, L.; Conte, M.P.; Iacovelli, F.; Romeo, A.; Falconi, M.; Del Vecchio, C.; Franchin, E.; et al. Lactoferrin as Antiviral Treatment in COVID-19 Management: Preliminary Evidence. Int. J. Environ. Res. Public Health 2021, 18, 10985. [Google Scholar] [CrossRef] [PubMed]
- Serrano, G.; Kochergina, I.; Albors, A.; Diaz, E.; Oroval, M.; Hueso, G.; Serrano, J.M. Liposomal Lactoferrin as Potential Preventative and Cure for COVID-19. Int. J. Res. Health Sci. 2020, 8, 08–15. [Google Scholar] [CrossRef]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Broglio, K. Randomization in clinical trials. Permuted blocks and stratification. JAMA 2018, 319, 223–224. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing; R Core Team: Wien, Austria, 2015. [Google Scholar]
- Champely, S.; Ekstrom, C.; Dalgaard, P.; Gill, J.; Weibelzahl, S.; Anandkumar, A.; Ford, C.; Volcic, R.; De Rosario, H. Package “Pwr”, R Package Version. Available online: https://CRAN.R-project.org/package=pwr (accessed on 15 December 2020).
- Algahtani, F.D.; ELabbasy, M.T.; Sanak, M.A.; Adeboye, A.A.; Yusuf, R.A.; Ghoniem, M.E. The prospect of lactoferrin use ad adjunctive agent in management of SARS-CoV-2 patients: A randomized pilot study. Medicina 2021, 57, 842. [Google Scholar] [CrossRef]
- Fischer, R.; Debbabi, H.; Blais, A.; Dubarry, M.; Rautureau, M.; Boyaka, P.N.; Tome, D. Uptake of ingested bovine lactoferrin and its accumulation in adult mouse tissues. Int. Immunopharmacol. 2007, 7, 1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, H.; Yoshizawa, Y.; Yokoyama, T.; Takeuchi, T.; Talukder, M.J.R.; Shimizu, H.; Ando, K.; Harada, E. Persorption of bovine lactoferrin from the intestinal lumen into the systemic circulation via the portal vein and the mesenteric lymphatics in growing pigs. J. Vet.-Med. Sci. 2003, 65, 567–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashida, K.; Sasaki, H.; Suzuki, Y.A.; Lönnerdal, B. Cellular internalization of lactoferrin in intestinal epithelial cells. Biometals 2004, 17, 311–315. [Google Scholar] [CrossRef]
- Kawakami, H.; Lonnerdal, B. Isolation and function of a receptor for human lactoferrin in human fetal intestinal brush-border membranes. Am. J. Physiol. 1991, 261, G841–G846. [Google Scholar] [CrossRef]
- Jiang, R.; Lopez, V.; Kelleher, S.L.; Lönnerdal, B. Apo- and holo-lactoferrin are both internalized by lactoferrin receptor via clathrin-mediated endocytosis but differentially affect ERK-signaling and cell proliferation in caco-2 cells. J. Cell. Physiol. 2011, 226, 3022–3031. [Google Scholar] [CrossRef] [Green Version]
- Lopez, V.; Kelleher, S.L.; Lönnerdal, B. Lactoferrin receptor mediates apo- but not hol-lactoferrin internalization via clath-rin-mediated endocytosis in trophoblasts. Biochem. J. 2008, 411, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, Y.A.; Lopez, V.; Lönnerdal, B. Mammalian lactoferrin receptors: Structure and function. Cell. Mol. Life Sci. 2005, 62, 2560–2575. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Ansems, K.; Grundeis, F.; Dahms, K.; Mikolajewska, A.; Thieme, V.; Piechotta, V.; Metzendorf, M.I.; Stegemann, M.; Benstoem, C.; Fichtner, F. Remdesivir for the Treatment of COIVD-19. Cochrane Database of Systematic Reviews. Art. N:CD014962. 2021. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD014962/full (accessed on 8 August 2022).
- Arribas, J.R.; Bhagani, S.; Lobo, S.M.; Khaertynova, I.; Mateu, L.; Fishchuk, R.; Park, W.Y.; Hussein, K.; Kim, S.W.; Ghosn, J.; et al. Randomized Trial of Molnupiravir or Placebo in Patients Hospitalized with COVID-19. NEJM Évid. 2022, 1, EVIDoa2100044. [Google Scholar] [CrossRef]
- Legrand, D.; Mazurier, J. A critical review of the roles of host lactoferrin in immunity. Biometals 2010, 23, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.M. Clinical Pharmacology of Corticosteroids. Respir. Care 2018, 63, 655–670. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.J. How corticosteroids control inflammation: Quintiles Prize Lecture 2005. Br. J. Pharmacol. 2006, 148, 245–254. [Google Scholar] [CrossRef]
- Redwan, E.M.; Uversky, V.N.; El-Fakharany, E.M.; Al-Mehdar, H. Potential lactoferrin activity against pathogenic viruses. Comptes Rendus Biol. 2014, 337, 581–595. [Google Scholar] [CrossRef]
- Hoxa, B.; Hodaj, A. Potential role of lactoferrin and heparin in COIVD-19: A review. Eur. Sci. J. ESJ 2021, 17, 14–23. [Google Scholar]
- Andersen, J.H.; Jenssen, H.; Sandvik, K.; Gutteberg, T.J. Anti-HSV activity of lactoferrin and lactoferricin is dependent on the presence of heparan sulphate at the cell surface. J. Med. Virol. 2004, 74, 262–271. [Google Scholar] [CrossRef]
- Avula, A.; Nalleballe, K.; Narula, N.; Sapozhnikov, S.; Dandu, V.; Toom, S.; Glaser, A.; Elsayegh, D. COVID-19 presenting as stroke. Brain Behav. Immun. 2020, 87, 115–119. [Google Scholar] [CrossRef]
- Belting, M. Heparan sulfate proteoglycan as a plasma membrane carrier. Trends Biochem. Sci. 2003, 28, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Berlutti, F.; Pantanella, F.; Natalizi, T.; Frioni, A.; Paesano, R.; Polimeni, A.; Valenti, P. Antiviral properties of lactoferrin—A natural immunity molecule. Molecules 2011, 16, 6992–7018. [Google Scholar] [CrossRef] [Green Version]
- Campione, E.; Cosio, T.; Rosa, L.; Lanna, C.; Di Girolamo, S.; Gaziano, R.; Valenti, P.; Bianchi, L. Lactoferrin as protective natural barrier of respiratory and intestinal mucosa against coronavirus infection and inflammation. Int. J. Mol. Sci. 2020, 21, 4903. [Google Scholar] [CrossRef]
- Campione, E.; Lanna, C.; Cosio, T.; Rosa, L.; Conte, M.P.; Iacovelli, F.; Romeo, A.; Falconi, M.; Del Vecchio, C.; Franchin, E.; et al. Pleiotropic effect of lactoferrin in the prevention and treatment of COIVD-19 infection: In Vivo, in silico and in vitro preliminary evidences. BioRxiv 2020. Available online: https://www.biorxiv.org/content/10.1101/2020.08.11.244996v2.full.pdf (accessed on 25 May 2022).
- Carvalho, C.A.; Sousa, I.P.; Silva, J.L.; Oliveira, A.C.; Gonçalves, R.B.; Gomes, A.M. Inhibition of Mayaro virus infection by bovine lactoferrin. Virology 2014, 452-453, 297–302. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Liu, Q.; Guo, D. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J. Med. Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019-COVID-19. Clin. Microbiol. Rev. 2020, 33, e00028-20. [Google Scholar] [CrossRef] [PubMed]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Kochi, A.N.; Tagliari, A.P.; Forleo, G.B.; Fassini, G.M.; Tondo, C. Cardiac and arrhythmic complications in patients with COVID-19. J. Cardiovasc. Electrophysiol. 2020, 31, 1003–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legrand, D.; Elass, E.; Carpentier, M.; Mazurier, J. Interactions of lactoferrin with cells involved in immune function. Biochem. Cell Biol. 2006, 84, 282–290. [Google Scholar] [CrossRef]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L.; et al. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Rosa, L.; Cutone, A.; Lepanto, M.S.; Paesano, R.; Valenti, P. Lactoferrin: A natural glycoprotein involved in iron and inflammatory homeostasis. Int. J. Mol. Sci. 2017, 18, 1985. [Google Scholar] [CrossRef] [PubMed]
- Sapp, M.; Bienkowska-Haba, M. Viral entry mechanisms: Human papillomavirus and a long journey from extracellular matrix to the nucleus. FEBS J. 2009, 276, 7206–7216. [Google Scholar] [CrossRef] [PubMed]
- Spear, P.G. Herpes simplex virus: Receptors and ligands for cell entry. Cell Microbiol. 2004, 6, 401–410. [Google Scholar] [CrossRef]
- Valenti, P.; Antonini, G. Lactoferrin: An important host defence against microbial and viral attack. Cell Mol. Life Sci. 2005, 62, 2576–2587. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Oda, H.; Yamauchi, K.; Abe, F. Lactoferrin for prevention of common viral infections. J. Infect Chemother. 2014, 20, 666–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Zhang, Y.; Wu, L.; Niu, S.; Song, C.; Zhang, Z.; Lu, G.; Qiao, C.; Hu, Y.; Yuen, K.Y.; et al. Structural and functional basis of SARS-CoV-2 entry by using human ACE2. Cell 2020, 181, 894–904.e9. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, P.; Wang, H.; Luo, Y.; Wan, L.; Jiang, M.; Chu, Y. Lactoferrin for the treatment of COVID-19. Exp. Ther. Med. 2020, 20, 272. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for gastrointestinal infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e3. [Google Scholar] [CrossRef]
- Yang, Z.; Jiang, R.; Chen, Q.; Wang, J.; Duan, Y.; Pang, X.; Jiang, S.; Bi, Y.; Zhang, H.; Lönnerdal, B.; et al. Concentration of lactoferrin in human milk and its variation during lactation in different Chinese populations. Nutrients 2018, 10, 1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosemberger, W.F.; Lachin, J.M. Randomization and the Clinical Trial. Wiley Online Library: Hoboken, NJ, USA, 2002; ISBN 0-471-72210-3. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences. Academic Press: Cambridge, MA, USA, 1977; ISBN 978-0-12-179060-8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| At Admission | Daily during Hospitalization | Weekly during Hospitalization | At Discharge |
|---|---|---|---|
|
|
|
|
| Lactoferrin (n = 113) | Placebo (n = 105) | ||
|---|---|---|---|
| Female/Male | 44/69 | 33/72 | χ2 1.3435, p = 0.2464 |
| Age, median (IQR), years | 66 (56–73) | 65 (57–73) | Z = 0.4427, p = 0.6580 |
| Symptoms | |||
| Productive cough | 12/101 | 11/94 | χ2 0.0012, p = 0.9726 |
| Non-productive cough | 41/72 | 43/62 | χ2 0.5010, p = 0.4791 |
| Dyspnea | 79/34 | 71/34 | χ2 0.1333, p = 0.7151 |
| Diarrhea | 18/95 | 22/83 | χ2 0.9166, p = 0.3384 |
| COVID-19 related home treatment | |||
| Hydroxychloroquine | 0/113 | 2/103 | χ2 2.1723, p = 0.1405 |
| Azithromycin | 28/85 | 35/70 | χ2 1.9384, p = 0.1638 |
| Heparin | 34/79 | 25/80 | χ2 1.0871, p = 0.2971 |
| Steroids | 53/60 | 45/60 | χ2 0.3580, p = 0.5494 |
| Number of medications | χ2 12.8569, p = 0.2318 | ||
| None | 30 | 26 | |
| 1 | 20 | 20 | |
| 2–4 | 38 | 32 | |
| ≥4 | 25 | 27 | |
| Comorbidities | |||
| BMI ≥ 30 | 38 | 27 | χ2 1.6212, p = 0.2029 |
| Current or former smokers | 19 | 22 | χ2 0.6290, p = 0.4279 |
| Charlson Comorbidity Index, median (IQR) | 2 (1–4) | 3 (1–4) | Z = −0.0792, p = 0.9368 |
| Days from symptoms onset, median (IQR) | 6 (4–7) | 7 (4–8) | Z = −1.7939, p = 0.0728 |
| Vital parameters | |||
| Temperature, median (IQR), °C | 36.5 (36.1–37.1) | 36.5 (36.1–36.9) | Z = 0.4530, p = 0.6505 |
| Cardiac rate, median (IQR), beats/min | 81 (75–91) | 85 (73–96) | Z = −0.8456, p = 0.3978 |
| Respiratory rate, median (IQR), breaths/min * | 20 (18–24) | 20 (18–25) | Z = 0.9209, p = 0.3571 |
| spO2%, median (IQR) * | 95 (93–97) | 96 (93–97) | Z = −1.7675, p = 0.0771 |
| Systolic pressure, median (IQR), mmHg | 125 (116–140) | 126 (117–142) | Z = −0.2227, p = 0.8238 |
| Diastolic pressure, median (IQR), mmHg | 75 (70–80) | 75 (70–85) | Z = −0.5018, p = 0.6158 |
| NEWS2, median [IQR] | 5 (4–6) | 5 (3–6) | Z = 0.0790, p = 0.9371 |
| Laboratory findings | |||
| Hemoglobin, median (IQR), g/dL | 13.9 (12.7–14.9) | 14.0 (12.3–15.0) | Z = 0.2630, p = 0.7925 |
| Leukocytes, median (IQR), cells×103/µL | 7.4 (5.2–10.1) | 6.6 (4.9–8.9) | Z = 1.1709, p = 0.2417 |
| Neutrophils, median (IQR), cells×103/µL | 6.0 (4.3–8.7) | 5.4 (3.9–7.6) | Z = 1.2130, p = 0.2251 |
| Lymphocytes, median (IQR), cells×103/µL | 0.7 (0.6–1.0) | 0.7 (0.5–1.0) | Z = 0.0807, p = 0.9357 |
| Platelets, median (IQR), cells×103/µL | 200 (156–255) | 210 (167–269) | Z = −0.8852, p = 0.3760 |
| ALT, median (IQR), U/L | 33 (24–54) | 35 (25–52) | Z = −0.3495, p = 0.7267 |
| AST, median (IQR), U/L | 41 (31–57) | 39 (28–54) | Z = 0.9099, p = 0.3629 |
| Creatinine, median (IQR), mg/dL | 0.8 (0.7–1.0) | 0.8 (0.7–1.0) | Z = 0.0303, p = 0.9758 |
| Erythrocyte sedimentation rate, median (IQR), mL/min | 41 (31–55) | 38 (24–49) | Z = 1.5780, p = 0.1146 |
| CRP, median (IQR), mg/dL | 7.8 (4.4–12.0) | 7.1 (4.4–12.9) | Z = 0.1053, p = 0.9161 |
| LDH, median (IQR), U/L | 533 (345–830) | 634 (459–821) | Z = −1.4739, p = 0.1405 |
| Troponin I, median (IQR), ng/mL | 6 (3–17) | 8 (4–14) | Z = −0.4006, p = 0.6887 |
| Ferritin, median (IQR), ng/mL | 797 (343–1373) | 827 (461–1229) | Z = 0.2026, p = 0.8395 |
| D-dimer, median (IQR), µg/L | 658 (438–1148) | 800 (544–1390) | Z = −1.3029, p = 0.1926 |
| IL-6, median (IQR), pg/mL | 11.5 (3.1–28.2) | 9.1 (4.2–22.6) | Z = 0.0970, p = 0.9227 |
| Arterial blood gas analysis * | |||
| pH, median (IQR) | 7.5 (7.4–7.5) | 7.5 (7.4–7.5) | Z = −0.5288, p = 0.5969 |
| pO2, median (IQR), mm Hg | 71 (61–80) | 66 (60–76) | Z = 1.3906, p = 0.1643 |
| pCO2, median (IQR), mm Hg | 37 (34–39) | 36 (33–39) | Z = 0.7675, p = 0.4434 |
| P/F, median (IQR) | 155 (124–209) | 151 (124–243) | Z = −0.2884, p = 0.7884 |
| Demographics, Parameters, and Clinical Scores | Values |
|---|---|
| Female/Male | 77/141 |
| Age, median (IQR), years | 65.5 (56.4–73.4) |
| Symptoms | |
| Productive cough | 23/195 |
| Non-productive cough | 84/134 |
| Dyspnea | 150/68 |
| Diarrhea | 40/178 |
| COVID-19 related home treatment | |
| Hydroxychloroquine | 2/216 |
| Azithromycin | 63/155 |
| Heparin | 59/159 |
| Steroids | 98/120 |
| Number of medications | |
| None | 56 |
| 1 | 40 |
| 2–4 | 70 |
| ≥4 | 52 |
| Comorbidities | |
| BMI ≥ 30 | 65 |
| Current or former smokers | 41 |
| Charlson Comorbidity Index, median (IQR) | 3 (1–4) |
| Days from symptoms onset | 6 (4–8) |
| Vital parameters | |
| Temperature, median (IQR), °C | 36.5 (36.1–37.0) |
| Cardiac rate, median (IQR), beats/min | 82 (74–94) |
| Respiratory rate, median (IQR), breaths/min * | 20 (18–24) |
| spO2%, median (IQR) * | 95 (93–97) |
| Systolic pressure, median (IQR), mmHg | 125 (116–140) |
| Diastolic pressure, median (IQR), mmHg | 75 (70–82) |
| NEWS2, median (IQR) | 5 (4–6) |
| Laboratory findings | |
| Hemoglobin, median (IQR), g/dL | 13.9 (12.5–15) |
| Leukocytes, median (IQR), cells×103/µL | 7.0 (5.1–9.5) |
| Neutrophils, median (IQR), cells×103/µL | 5.7 (4.2–8.3) |
| Lymphocytes, median (IQR), cells×103/µL | 0.7 (0.6–1.0) |
| Platelets, median (IQR), cells×103/µL | 207 (161–260) |
| ALT, median (IQR), U/L | 34 (24–52) |
| AST, median (IQR), U/L | 39 (30–56) |
| Creatinine, median (IQR), mg/dL | 0.8 (0.7–1.0) |
| Erythrocyte sedimentation rate, median (IQR), mL/min | 40 (25–53) |
| CRP, median (IQR), mg/dL | 7.8 (4.4–12.0) |
| LDH, median (IQR), U/L | 585 (379–829) |
| Troponin I, median (IQR), ng/mL | 8 (3–15) |
| Ferritin, median (IQR), ng/mL | 820.5 (394–1341) |
| D-dimer, median (IQR), µg/L | 708 (496–1331) |
| IL-6, median (IQR), pg/mL | 11.3 (5.0–31.6) |
| Arterial blood gas analysis * | |
| pH, median (IQR) | 7.5 (7.4–7.5) |
| pO2, median (IQR), mm Hg | 68.2 (60.0–79.5) |
| pCO2, median (IQR), mm Hg | 36.6 (33.1–39.0) |
| P/F, median (IQR) | 154 (124–222) |
| Lactoferrin (n = 113) | Placebo (n = 105) | ||
|---|---|---|---|
| Variation of NEWS2 from baseline at 7 days, median (IQR) at 14 days, median (IQR) at 21 days, median (IQR) | −2 (−3–0) (n = 85) −2 (−3–0) (n = 41) −1 (−4–1) (n = 19) | −2 (−4–1) (n = 86) −2 (−3–0) (n = 26) −2 (−4–1) (n = 11) | Z = 0.4337, p = 0.6645 Z = 0.5793, p = 0.5624 Z = −0.3055, p = 0.7600 |
| Days of oxygen supplementation, median (IQR) | 11(7–14) | 12 (8–19) | Z = −1.314, p = 0.1888 |
| Patients needing any oxygen supplementation HFNC or NIV mechanical ventilation | 104 88 14 | 99 73 9 | RR = 0.98, 95% CI 0.91–1.05 RR = 1.12, 95% CI 0.95–1.131 RR = 1.45, 95% CI 0.65–3.20 |
| In-hospital mortality at 14 days | 16 | 12 | RR = 1.24, 95% CI 0.62–2.49 |
| In-hospital mortality at 28 days | 18 | 15 | RR = 1.12, 95% CI 0.59–2.10 |
| Age | Outcome | Lactoferrin | Placebo | Difference between Groups 95% CI | p-Value | RR 95% CI |
| <65 years | Adverse outcome | 8/55 | 6/52 | 3% −10.38–16.13 | 0.6467 | 1.26 0.47–3.39 |
| Positive outcome | 43/55 | 42/52 | 2.60% −12.86–17.72 | 0.7405 | 0.97 0.80–1.17 | |
| ≥65 years | Adverse outcome | 16/58 | 15/53 | 0.70% −15.61–17.22 | 0.9349 | 0.97 0.54–1.77 |
| Positive outcome | 24/58 | 31/53 | 17.10% −1.44–34.07 | 0.0732 | 0.71 0.48–1.04 | |
| Sex | Outcome | Lactoferrin | Placebo | Difference between groups 95% CI | p-value | RR 95% CI |
| Females | Adverse outcome | 8/44 | 2/33 | 12.12 −3.96–26.58 | 0.1198 | 3.00 0.68–13.21 |
| Positive outcome | 27/44 | 27/33 | 20.46 −0.26–38.03 | 0.0538 | 2.13 0.94–4.80 | |
| Males | Adverse outcome | 16/69 | 19/72 | 3.20 −11.05–17.18 | 0.6613 | 0.88 0.49–1.57 |
| Positive outcome | 40/69 | 46/72 | 5.92 −9.97–21.44 | 0.4728 | 1.16 0.77–1.76 |
| Lactoferrin | Placebo | Total | χ2 | p-Value | |
|---|---|---|---|---|---|
| Significant bleeding events | 1 | 1 | 2 | 0.0027 | 0.9585 |
| Thoracic pain | 9 | 4 | 13 | 1.6680 | 0.1965 |
| Arrhythmias | 10 | 7 | 17 | 0.3590 | 0.5490 |
| ACS (STEMI/NSTEMI) | 1 | 1 | 2 | 0.0027 | 0.9585 |
| Heart failure | 3 | 3 | 6 | 0.0083 | 0.9275 |
| ALT elevation 3 × ULN | 13 | 13 | 26 | 0.0396 | 0.8422 |
| Pneumomediastinum | 2 | 2 | 4 | 0.0055 | 0.9410 |
| VTE and pulmonary thromboembolism | 3 | 3 | 6 | 0.0083 | 0.9275 |
| AKI | 3 | 5 | 8 | 0.6800 | 0.4094 |
| Bacterial infection including bacteremia | 9 | 6 | 15 | 0.4280 | 0.5129 |
| Diarrhea | 0 | 4 | 4 | 4.3650 | 0.0367 |
| Seizures | 1 | 0 | 1 | 0.9290 | 0.3351 |
| Rhabdomyolysis | 2 | 0 | 2 | 1.8670 | 0.1718 |
| Total | 57 | 49 | 106 | 0.3090 | 0.5782 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matino, E.; Tavella, E.; Rizzi, M.; Avanzi, G.C.; Azzolina, D.; Battaglia, A.; Becco, P.; Bellan, M.; Bertinieri, G.; Bertoletti, M.; et al. Effect of Lactoferrin on Clinical Outcomes of Hospitalized Patients with COVID-19: The LAC Randomized Clinical Trial. Nutrients 2023, 15, 1285. https://doi.org/10.3390/nu15051285
Matino E, Tavella E, Rizzi M, Avanzi GC, Azzolina D, Battaglia A, Becco P, Bellan M, Bertinieri G, Bertoletti M, et al. Effect of Lactoferrin on Clinical Outcomes of Hospitalized Patients with COVID-19: The LAC Randomized Clinical Trial. Nutrients. 2023; 15(5):1285. https://doi.org/10.3390/nu15051285
Chicago/Turabian StyleMatino, Erica, Elena Tavella, Manuela Rizzi, Gian Carlo Avanzi, Danila Azzolina, Antonio Battaglia, Paolo Becco, Mattia Bellan, Giovanni Bertinieri, Massimo Bertoletti, and et al. 2023. "Effect of Lactoferrin on Clinical Outcomes of Hospitalized Patients with COVID-19: The LAC Randomized Clinical Trial" Nutrients 15, no. 5: 1285. https://doi.org/10.3390/nu15051285
APA StyleMatino, E., Tavella, E., Rizzi, M., Avanzi, G. C., Azzolina, D., Battaglia, A., Becco, P., Bellan, M., Bertinieri, G., Bertoletti, M., Casciaro, G. F., Castello, L. M., Colageo, U., Colangelo, D., Comolli, D., Costanzo, M., Croce, A., D’Onghia, D., Della Corte, F., ... Sainaghi, P. P. (2023). Effect of Lactoferrin on Clinical Outcomes of Hospitalized Patients with COVID-19: The LAC Randomized Clinical Trial. Nutrients, 15(5), 1285. https://doi.org/10.3390/nu15051285