
PRO-DEMET Randomized Controlled Trial on Probiotics in Depression—Pilot Study Results



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Outcome Measures
2.3. Questionnaires and Scales
2.4. Biological Material
2.5. Intervention
2.6. Data Management
2.7. Ethics
2.8. Data Analysis
3. Results
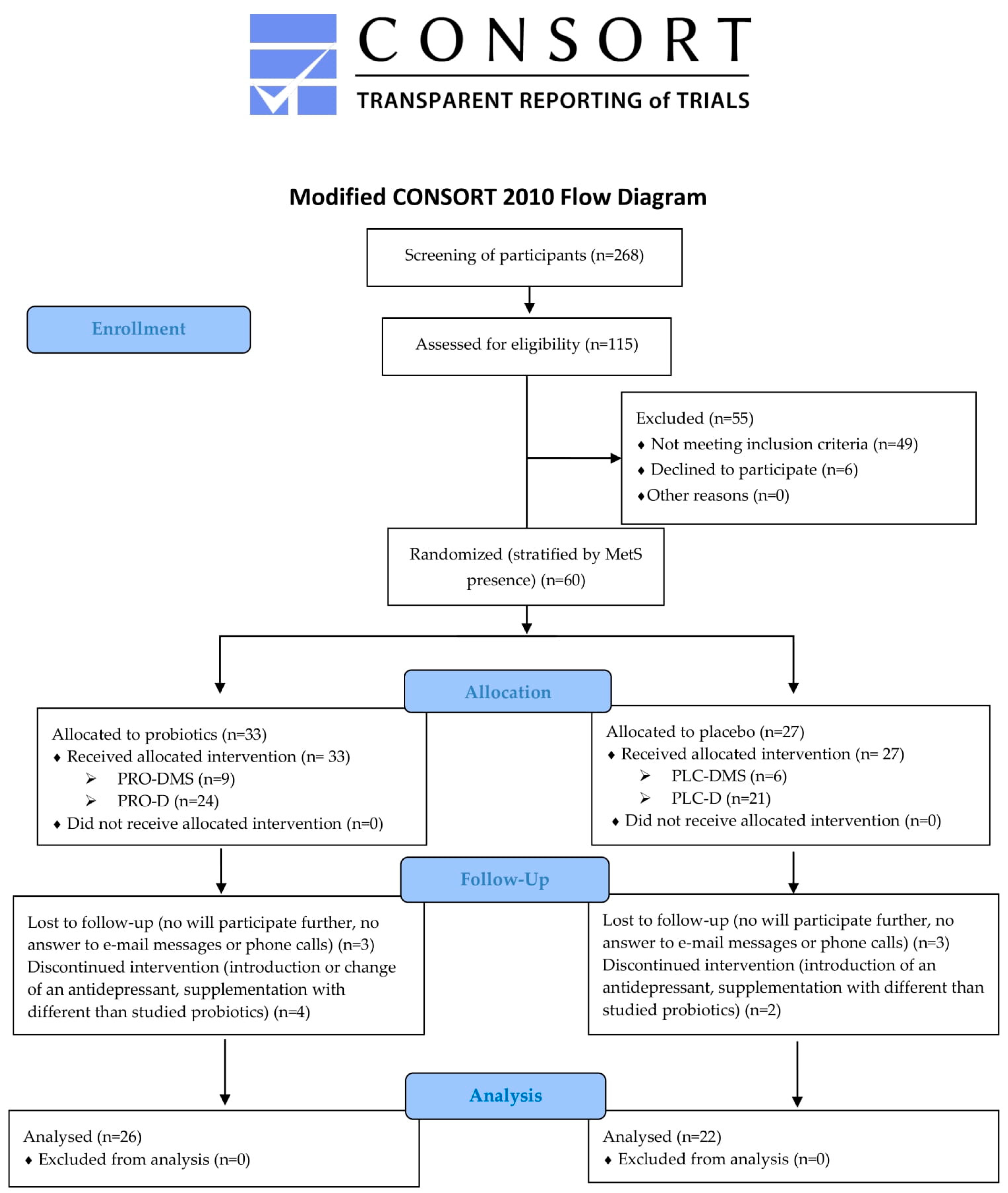
3.1. Participant Flow
3.2. Feasibility
3.2.1. Rate of Recruitment, Eligibility, Enrolment, and Retention
3.2.2. Retention Ratio, Intervention Adherence and Tolerability
3.2.3. Procedures
3.3. Population Characteristics
3.4. Clinical and Laboratory Outcome Measures
3.4.1. Psychometric Measures
3.4.2. Metabolic Syndrome Components and Related Parameters
3.4.3. Inflammation-Related Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marazziti, D.; Rutigliano, G.; Baroni, S.; Landi, P.; Dell’Osso, L. Metabolic syndrome and major depression. CNS Spectr. 2014, 19, 293–304. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Lange, S.M.M. Metabolic syndrome in psychiatric patients: Overview, mechanisms, and implications. Dialogues Clin. Neurosci. 2018, 20, 63–73. [Google Scholar] [CrossRef]
- Lamers, F.; Milaneschi, Y.; De Jonge, P.; Giltay, E.J.; Penninx, B.W.J.H. Metabolic and inflammatory markers: Associations with individual depressive symptoms. Psychol. Med. 2018, 48, 1102–1110. [Google Scholar] [CrossRef]
- Moazzami, K.; Lima, B.B.; Sullivan, S.; Shah, A.; Bremner, J.D.; Vaccarino, V. Independent and Joint Association of Obesity and Metabolic Syndrome with Depression and Inflammation. Health Psychol. 2019, 38, 586–595. [Google Scholar] [CrossRef]
- Soto-Angona, Ó.; Anmella, G.; Valdés-Florido, M.J.; De Uribe-Viloria, N.; Carvalho, A.F.; Penninx, B.W.J.H.; Berk, M. Non-alcoholic fatty liver disease (NAFLD) as a neglected metabolic companion of psychiatric disorders: Common pathways and future approaches. BMC Med. 2020, 18, 261. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Gerhard, T.; Stroup, T.S.; Correll, C.U.; Setoguchi, S.; Strom, B.L.; Huang, C.; Tan, Z.; Crystal, S.; Olfson, M. Mortality risk of antipsychotic augmentation for adult depression. PLoS ONE 2020, 15, e0239206. [Google Scholar] [CrossRef]
- Matta, J.; Hoertel, N.; Kesse-Guyot, E.; Plesz, M.; Wiernik, E.; Carette, C.; Czernichow, S.; Limosin, F.; Goldberg, M.; Zins, M.; et al. Diet and physical activity in the association between depression and metabolic syndrome: Constances study. J. Affect. Disord. 2019, 244, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Salvucci, E. The disappearing microbiota: Diseases of the Western civilization. In How Fermented Foods Feed a Healthy Gut Microbiota: A Nutrition Continuum; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 325–347. ISBN 9783030287375. [Google Scholar]
- Skonieczna-Żydecka, K.; Marlicz, W.; Misera, A.; Koulaouzidis, A.; Łoniewski, I. Microbiome—The Missing Link in the Gut-Brain Axis: Focus on Its Role in Gastrointestinal and Mental Health. J. Clin. Med. 2018, 7, 521. [Google Scholar] [CrossRef] [Green Version]
- Dinan, T.G.; Cryan, J.F. The Microbiome-Gut-Brain Axis in Health and Disease. Gastroenterol. Clin. N. Am. 2017, 46, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Carlessi, A.S.; Borba, L.A.; Zugno, A.I.; Quevedo, J.; Réus, G.Z. Gut microbiota–brain axis in depression: The role of neuroinflammation. Eur. J. Neurosci. 2019, 53, 222–235. [Google Scholar] [CrossRef] [PubMed]
- Liśkiewicz, P.; Kaczmarczyk, M.; Misiak, B.; Wroński, M.; Bąba-Kubiś, A.; Skonieczna-Żydecka, K.; Marlicz, W.; Bieńkowski, P.; Misera, A.; Pełka-Wysiecka, J.; et al. Analysis of gut microbiota and intestinal integrity markers of inpatients with major depressive disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 106, 110076. [Google Scholar] [CrossRef] [PubMed]
- Sanada, K.; Nakajima, S.; Kurokawa, S.; Barceló-Soler, A.; Ikuse, D.; Hirata, A.; Yoshizawa, A.; Tomizawa, Y.; Salas-Valero, M.; Noda, Y.; et al. Gut microbiota and majore depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2020, 266, 1–13. [Google Scholar] [CrossRef]
- Mason, B.L.; Li, Q.; Minhajuddin, A.; Czysz, A.H.; Coughlin, L.A.; Hussain, S.K.; Koh, A.Y.; Trivedi, M.H. Reduced anti-inflammatory gut microbiota are associated with depression and anhedonia. J. Affect. Disord. 2020, 266, 394–401. [Google Scholar] [CrossRef]
- Madan, A.; Thompson, D.; Fowler, J.C.; Ajami, N.J.; Salas, R.; Frueh, B.C.; Bradshaw, M.R.; Weinstein, B.L.; Oldham, J.M.; Petrosino, J.F. The gut microbiota is associated with psychiatric symptom severity and treatment outcome among individuals with serious mental illness. J. Affect. Disord. 2020, 264, 98–106. [Google Scholar] [CrossRef]
- Ortega, M.A.; Alvarez-Mon, M.A.; García-Montero, C.; Fraile-Martinez, O.; Guijarro, L.G.; Lahera, G.; Monserrat, J.; Valls, P.; Mora, F.; Rodríguez-Jiménez, R.; et al. Gut Microbiota Metabolites in Major Depressive Disorder—Deep Insights into Their Pathophysiological Role and Potential Translational Applications. Metabolites 2022, 12, 50. [Google Scholar] [CrossRef]
- Belkaid, Y.; Hand, T.W. Role of the microbiota in immunity and inflammation. Cell 2014, 157, 121–141. [Google Scholar] [CrossRef] [Green Version]
- Dai, X.; Hou, H.; Zhang, W.; Liu, T.; Li, Y.; Wang, S.; Wang, B.; Cao, H. Microbial Metabolites: Critical Regulators in NAFLD. Front. Microbiol. 2020, 11, 567654. [Google Scholar] [CrossRef]
- Yu, H.-R.; Sheen, J.-M.; Hou, C.-Y.; Lin, I.-C.; Huang, L.-T.; Tain, Y.-L.; Cheng, H.-H.; Lai, Y.-J.; Lin, Y.-J.; Tiao, M.-M.; et al. Effects of Maternal Gut Microbiota-Targeted Therapy on the Programming of Nonalcoholic Fatty Liver Disease in Dams and Fetuses, Related to a Prenatal High-Fat Diet. Nutrients 2022, 14, 4004. [Google Scholar] [CrossRef]
- Miao, Z.H.; Wang, J.N.; Shen, X.; Zhou, Q.Q.; Luo, Y.T.; Liang, H.J.; Wang, S.; Qi, S.H.; Cheng, R.Y.; He, F. Long-term use of Lacticaseibacillus paracasei N1115 from early life alleviates high-fat-diet-induced obesity and dysmetabolism in mice. Benef. Microbes 2022, 13, 407–416. [Google Scholar] [CrossRef]
- Dabke, K.; Hendrick, G.; Devkota, S. The gut microbiome and metabolic syndrome. J. Clin. Investig. 2019, 129, 4050–4057. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.; Stratigou, T.; Christodoulatos, G.S.; Dalamaga, M. Understanding the Role of the Gut Microbiome and Microbial Metabolites in Obesity and Obesity-Associated Metabolic Disorders: Current Evidence and Perspectives. Curr. Obes. Rep. 2019, 8, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Dash, S.; Clarke, G.; Berk, M.; Jacka, F.N. The gut microbiome and diet in psychiatry: Focus on depression. Curr. Opin. Psychiatry 2015, 28, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, E.; Egea-Zorrilla, A.; Plaza-Díaz, J.; Aragón-Vela, J.; Muñoz-Quezada, S.; Tercedor-Sánchez, L.; Abadia-Molina, F. The Gut Microbiota and Its Implication in the Development of Atherosclerosis and Related Cardiovascular Diseases. Nutrients 2020, 12, 605. [Google Scholar] [CrossRef] [Green Version]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document: The international scientific association for probiotics and prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [Green Version]
- Huang, R.; Wang, K.; Hu, J. Effect of probiotics on depression: A systematic review and meta-analysis of randomized controlled trials. Nutrients 2016, 8, 483. [Google Scholar] [CrossRef] [Green Version]
- Goh, K.K.; Liu, Y.W.; Kuo, P.H.; Chung, Y.C.E.; Lu, M.L.; Chen, C.H. Effect of probiotics on depressive symptoms: A meta-analysis of human studies. Psychiatry Res. 2019, 282, 112568. [Google Scholar] [CrossRef]
- Liu, R.T.; Walsh, R.F.L.; Sheehan, A.E. Prebiotics and probiotics for depression and anxiety: A systematic review and meta-analysis of controlled clinical trials. Neurosci. Biobehav. Rev. 2019, 102, 13–23. [Google Scholar] [CrossRef]
- Ng, Q.X.; Peters, C.; Ho, C.Y.X.; Lim, D.Y.; Yeo, W.S. A meta-analysis of the use of probiotics to alleviate depressive symptoms. J. Affect. Disord. 2018, 228, 13–19. [Google Scholar] [CrossRef]
- Nikolova, V.L.; Cleare, A.J.; Young, A.H.; Stone, J.M. Updated Review and Meta-Analysis of Probiotics for the Treatment of Clinical Depression: Adjunctive vs. Stand-Alone Treatment. J. Clin. Med. 2021, 10, 647. [Google Scholar] [CrossRef]
- Alli, S.R.; Gorbovskaya, I.; Liu, J.C.W.; Kolla, N.J.; Brown, L.; Müller, D.J. The Gut Microbiome in Depression and Potential Benefit of Prebiotics, Probiotics and Synbiotics: A Systematic Review of Clinical Trials and Observational Studies. Int. J. Mol. Sci. 2022, 23, 4494. [Google Scholar] [CrossRef] [PubMed]
- Le Morvan de Sequeira, C.; Hengstberger, C.; Enck, P.; Mack, I. Effect of Probiotics on Psychiatric Symptoms and Central Nervous System Functions in Human Health and Disease: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 621. [Google Scholar] [CrossRef] [PubMed]
- Skowron, K.; Budzyńska, A.; Wiktorczyk-Kapischke, N.; Chomacka, K.; Grudlewska-Buda, K.; Wilk, M.; Wałecka-Zacharska, E.; Andrzejewska, M.; Gospodarek-Komkowska, E. The Role of Psychobiotics in Supporting the Treatment of Disturbances in the Functioning of the Nervous System—A Systematic Review. Int. J. Mol. Sci. 2022, 23, 7820. [Google Scholar] [CrossRef]
- Koutnikova, H.; Genser, B.; Monteiro-Sepulveda, M.; Faurie, J.M.; Rizkalla, S.; Schrezenmeir, J.; Clement, K. Impact of bacterial probiotics on obesity, diabetes and non-alcoholic fatty liver disease related variables: A systematic review and meta-analysis of randomised controlled trials. BMJ Open 2019, 9, e017995. [Google Scholar] [CrossRef] [PubMed]
- Tenorio-Jiménez, C.; Martínez-Ramírez, M.J.; Gil, Á.; Gómez-Llorente, C. Effects of probiotics on metabolic syndrome: A systematic review of randomized clinical trials. Nutrients 2020, 12, 124. [Google Scholar] [CrossRef] [Green Version]
- Paul, P.; Kaul, R.; Harfouche, M.; Arabi, M.; Al-Najjar, Y.; Sarkar, A.; Saliba, R.; Chaari, A. The effect of microbiome-modulating probiotics, prebiotics and synbiotics on glucose homeostasis in type 2 diabetes: A systematic review, meta-analysis, and meta-regression of clinical trials. Pharmacol. Res. 2022, 185, 106520. [Google Scholar] [CrossRef]
- Tan, J.; Zhou, H.; Deng, J.; Sun, J.; Zhou, X.; Tang, Y.; Qin, W. Effectiveness of Microecological Preparations for Improving Renal Function and Metabolic Profiles in Patients with Chronic Kidney Disease. Front. Nutr. 2022, 9, 850014. [Google Scholar] [CrossRef]
- Zeighamy Alamdary, S.; Afifirad, R.; Asgharzadeh, S.; Asadollahi, P.; Mahdizade Ari, M.; Dashtibin, S.; Sabaghan, M.; Shokouhamiri, M.R.; Ghanavati, R.; Darbandi, A. The Influence of Probiotics Consumption on Management of Prediabetic State: A Systematic Review of Clinical Trials. Int. J. Clin. Pract. 2022, 2022, 5963679. [Google Scholar] [CrossRef]
- Naseri, K.; Saadati, S.; Ashtary-Larky, D.; Asbaghi, O.; Ghaemi, F.; Pashayee-Khamene, F.; Yari, Z.; de Courten, B. Probiotics and synbiotics supplementation improve glycemic control parameters in subjects with prediabetes and type 2 diabetes mellitus: A GRADE-assessed systematic review, meta-analysis, and meta-regression of randomized clinical trials. Pharmacol. Res. 2022, 184, 106399. [Google Scholar] [CrossRef]
- Naseri, K.; Saadati, S.; Ghaemi, F.; Ashtary-Larky, D.; Asbaghi, O.; Sadeghi, A.; Afrisham, R.; de Courten, B. The effects of probiotic and synbiotic supplementation on inflammation, oxidative stress, and circulating adiponectin and leptin concentration in subjects with prediabetes and type 2 diabetes mellitus: A GRADE-assessed systematic review, meta-analysis, and meta-regression of randomized clinical trials. Eur. J. Nutr. 2022, 62, 543–561. [Google Scholar] [CrossRef]
- Dong, Y.; Xu, M.; Chen, L.; Bhochhibhoya, A. Probiotic Foods and Supplements Interventions for Metabolic Syndromes: A Systematic Review and Meta-Analysis of Recent Clinical Trials. Ann. Nutr. Metab. 2019, 74, 224–241. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Deng, Y.; He, Q.; Yang, K.; Li, J.; Xiang, W.; Liu, H.; Zhu, X.; Chen, H. Safety and efficacy of probiotic supplementation in 8 types of inflammatory arthritis: A systematic review and meta-analysis of 34 randomized controlled trials. Front. Immunol. 2022, 13, 961325. [Google Scholar] [CrossRef]
- Desai, V.; Kozyrskyj, A.L.; Lau, S.; Sanni, O.; Dennett, L.; Walter, J.; Ospina, M.B. Effectiveness of Probiotic, Prebiotic, and Synbiotic Supplementation to Improve Perinatal Mental Health in Mothers: A Systematic Review and Meta-Analysis. Front. Psychiatry 2021, 12, 622181. [Google Scholar] [CrossRef] [PubMed]
- Trifkovič, K.Č.; Mičetić-Turk, D.; Kmetec, S.; Strauss, M.; Dahlen, H.G.; Foster, J.P.; Fijan, S. Efficacy of Direct or Indirect Use of Probiotics for the Improvement of Maternal Depression during Pregnancy and in the Postnatal Period: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 970. [Google Scholar] [CrossRef] [PubMed]
- Lof, J.; Smits, K.; Melotte, V.; Kuil, L.E. The health effect of probiotics on high-fat diet-induced cognitive impairment, depression and anxiety: A cross-species systematic review. Neurosci. Biobehav. Rev. 2022, 136, 104634. [Google Scholar] [CrossRef]
- Gawlik-Kotelnicka, O.; Strzelecki, D. Probiotics as a Treatment for “Metabolic Depression”? A Rationale for Future Studies. Pharmaceuticals 2021, 14, 384. [Google Scholar] [CrossRef]
- Kazemi, A.; Noorbala, A.A.; Azam, K.; Djafarian, K. Effect of prebiotic and probiotic supplementation on circulating pro-inflammatory cytokines and urinary cortisol levels in patients with major depressive disorder: A double-blind, placebo-controlled randomized clinical trial. J. Funct. Foods 2019, 52, 596–602. [Google Scholar] [CrossRef]
- Romijn, A.R.; Rucklidge, J.J.; Kuijer, R.G.; Frampton, C. A double-blind, randomized, placebo-controlled trial of Lactobacillus helveticus and Bifidobacterium longum for the symptoms of depression. Aust. N. Z. J. Psychiatry 2017, 51, 810–821. [Google Scholar] [CrossRef] [Green Version]
- Diop, L.; Guillou, S.; Durand, H. Probiotic food supplement reduces stress-induced gastrointestinal symptoms in volunteers: A double-blind, placebo-controlled, randomized trial. Nutr. Res. 2008, 28, 1–5. [Google Scholar] [CrossRef]
- Pinto-Sanchez, M.I.; Hall, G.B.; Ghajar, K.; Nardelli, A.; Bolino, C.; Lau, J.T.; Martin, F.P.; Cominetti, O.; Welsh, C.; Rieder, A.; et al. Probiotic Bifidobacterium longum NCC3001 Reduces Depression Scores and Alters Brain Activity: A Pilot Study in Patients with Irritable Bowel Syndrome. Gastroenterology 2017, 153, 448–459.e8. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; Tompkins, T.A.; Matera, M.G. Immunomodulatory impact of a synbiotic in T(h)1 and T(h)2 models of infection. Ther. Adv. Respir. Dis. 2010, 4, 259–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messaoudi, M.; Lalonde, R.; Violle, N.; Javelot, H.; Desor, D.; Nejdi, A.; Bisson, J.-F.; Rougeot, C.; Pichelin, M.; Cazaubiel, M.; et al. Assessment of psychotropic-like properties of a probiotic formulation (Lactobacillus helveticus R0052 and Bifidobacterium longum R0175) in rats and human subjects. Br. J. Nutr. 2011, 105, 755–764. [Google Scholar] [CrossRef] [Green Version]
- Arseneault-Bréard, J.; Rondeau, I.; Gilbert, K.; Girard, S.A.; Tompkins, T.A.; Godbout, R.; Rousseau, G. Combination of Lactobacillus helveticus R0052 and Bifidobacterium longum R0175 reduces post-myocardial infarction depression symptoms and restores intestinal permeability in a rat model. Br. J. Nutr. 2012, 107, 1793–1799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, K.; Arseneault-Bréard, J.; Monaco, F.F.; Beaudoin, A.; Bah, T.M.; Tompkins, T.A.; Godbout, R.; Rousseau, G. Attenuation of post-myocardial infarction depression in rats by n-3 fatty acids or probiotics starting after the onset of reperfusion. Br. J. Nutr. 2013, 109, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.J.; Wang, R.; Li, X.F.; Wang, R.L. Bifidobacterium longum supplementation improved high-fat-fed-induced metabolic syndrome and promoted intestinal reg I gene expression. Exp. Biol. Med. 2011, 236, 823–831. [Google Scholar] [CrossRef]
- Ghorbani, Z.; Nazari, S.; Etesam, F.; Nourimajd, S.; Ahmadpanah, M.; Razeghi Jahromi, S. The Effect of Synbiotic as an Adjuvant Therapy to Fluoxetine in Moderate Depression: A Randomized Multicenter Trial. Arch. Neurosci. 2018, 5, e60507. [Google Scholar] [CrossRef] [Green Version]
- Chahwan, B.; Kwan, S.; Isik, A.; van Hemert, S.; Burke, C.; Roberts, L. Gut feelings: A randomised, triple-blind, placebo-controlled trial of probiotics for depressive symptoms. J. Affect. Disord. 2019, 253, 317–326. [Google Scholar] [CrossRef]
- Gawlik-Kotelnicka, O.; Skowrońska, A.; Margulska, A.; Czarnecka-Chrebelska, K.H.; Łoniewski, I.; Skonieczna-Żydecka, K.; Strzelecki, D. The Influence of Probiotic Supplementation on Depressive Symptoms, Inflammation, and Oxidative Stress Parameters and Fecal Microbiota in Patients with Depression Depending on Metabolic Syndrome Comorbidity—PRO-DEMET Randomized Study Protocol. J. Clin. Med. 2021, 10, 1342. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef] [Green Version]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A.; O’Cathain, A.; Altman, D.; Bretz, F.; et al. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ Br. Med. J. 2016, 2, 64. [Google Scholar] [CrossRef] [Green Version]
- ICD-11. Available online: https://icd.who.int/en (accessed on 2 January 2020).
- Cocks, K.; Torgerson, D.J. Sample size calculations for pilot randomized trials: A confidence interval approach. J. Clin. Epidemiol. 2013, 66, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Reed, G.M.; First, M.B.; Kogan, C.S.; Hyman, S.E.; Gureje, O.; Gaebel, W.; Maj, M.; Stein, D.J.; Maercker, A.; Tyrer, P.; et al. Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders. World Psychiatry 2019, 18, 3–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziebold, C.; Goldberg, D.P.; Reed, G.M.; Minhas, F.; Razzaque, B.; Fortes, S.; Robles, R.; Lam, T.P.; Bobes, J.; Iglesias, C.; et al. Dimensional analysis of depressive, anxious and somatic symptoms presented by primary care patients and their relationship with ICD-11 PHC proposed diagnoses. Psychol. Med. 2019, 49, 764–771. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Liang, Q.; Balakrishnan, B.; Belobrajdic, D.P.; Feng, Q.J.; Zhang, W. Role of dietary nutrients in the modulation of gut microbiota: A narrative review. Nutrients 2020, 12, 381. [Google Scholar] [CrossRef] [Green Version]
- Vich Vila, A.; Collij, V.; Sanna, S.; Sinha, T.; Imhann, F.; Bourgonje, A.R.; Mujagic, Z.; Jonkers, D.M.A.E.; Masclee, A.A.M.; Fu, J.; et al. Impact of commonly used drugs on the composition and metabolic function of the gut microbiota. Nat. Commun. 2020, 11, 362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Yun, Y.; Kim, S.J.; Lee, E.-J.; Chang, Y.; Ryu, S.; Shin, H.; Kim, H.-L.; Kim, H.-N.; Lee, J.H. Association between Cigarette Smoking Status and Composition of Gut Microbiota: Population-Based Cross-Sectional Study. J. Clin. Med. 2018, 7, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd-Price, J.; Abu-Ali, G.; Huttenhower, C. The healthy human microbiome. Genome Med. 2016, 8, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, J.H. The Distinction between Randomized Clinical Trials (RCTs) and Preliminary Feasibility and Pilot Studies: What They Are and Are Not. J. Orthop. Sport. Phys. Ther. 2014, 44, 555–558. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A consensus statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Wądołowska, L. Validation of Food Frequency Questionnaire (FFQ). Reproducibility Assessment. Bromat. Chem. Toksykol. 2005, 38, 27–33. Available online: http://www.sciepub.com/reference/219880 (accessed on 20 November 2020).
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.A.; Chorpita, B.F.; Korotitsch, W.; Barlow, D.H. Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behav. Res. Ther. 1997, 35, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial a Report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef]
- Chodkiewicz, J.; Miniszewska, J.; Krajewska, E.; Biliński, P. Mental Health during the Second Wave of the COVID-19 Pandemic—Polish Studies. Int. J. Environ. Res. Public Health 2021, 18, 3423. [Google Scholar] [CrossRef] [PubMed]
- Lamers, F.; Milaneschi, Y.; Vinkers, C.H.; Schoevers, R.A.; Giltay, E.J.; Penninx, B.W.J.H. Depression profilers and immuno-metabolic dysregulation: Longitudinal results from the NESDA study. Brain. Behav. Immun. 2020, 88, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.A.; Möller, H.J. Is the significant superiority of escitalopram compared with other antidepressants clinically relevant? Int. Clin. Psychopharmacol. 2009, 24, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Thase, M.E.; Mahableshwarkar, A.R.; Dragheim, M.; Loft, H.; Vieta, E. A meta-analysis of randomized, placebo-controlled trials of vortioxetine for the treatment of major depressive disorder in adults. Eur. Neuropsychopharmacol. 2016, 26, 979–993. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | PRO Group (n = 26) | PLC Group (n = 22) | p |
|---|---|---|---|
| Sex (F:M) | 21:5 | 20:2 | 0.56 |
| Age (years) | 34.30 | 35.70 | 0.37 |
| Diagnosis according to ICD-11 (6A70:6A71:6A72:6A73) | 5:9:0:12 | 4:2:0:16 | 0.13 |
| Psychotropic medications (%) | 61.5 | 81.8 | 0.13 |
| Antidepressants (%) | 61.5 | 81.8 | 0.13 |
| Antipsychotics (%) | 11.5 | 4.5 | 0.73 |
| Comorbidities (%) | 38.5 | 54.5 | 0.27 |
| COVID-19 in the past (%) | 15.4 | 18.2 | 0.95 |
| Other than psychotropics pharmacological treatment (%) | 34.6 | 45.5 | 0.45 |
| Smoking cigarettes (%) | 19.2 | 22.7 | 0.77 |
| Dietary supplements (%) | 57.7 | 36.4 | 0.14 |
| Overweight (according to BMI) (%) | 38.5 | 31.8 | 0.58 |
| Obesity (according to BMI) (%) | 11.5 | 22.7 | |
| MetS (%) | 26.9 | 27.3 | 0.97 |
| Abdominal obesity (%) | 53.8 | 63.6 | 0.49 |
| Raised TG (%) | 11.5 | 18.2 | 0.81 |
| Reduced HDL-c (%) | 19.2 | 13.6 | 0.89 |
| Raised BP (%) | 46.2 | 40.9 | 0.72 |
| Raised fGlc (%) | 15.4 | 13.6 | 0.81 |
| Characteristics | PRO Group | PLC Group | p |
|---|---|---|---|
| Sweets and snacks | 2.42 ± 0.52 | 2.85 ± 0.85 | 0.09 |
| Dairy and eggs | 2.81 ± 0.61 | 3.21 ± 0.86 | 0.01 |
| Highly-processed | 1.58 ± 0.57 | 2.12 ± 1.09 | 0.16 |
| Cereal products | 3.04 ± 0.54 | 3.20 ± 0.52 | 0.20 |
| Oils | 2.48 ± 0.71 | 2.55 ± 0.67 | 0.48 |
| Fruits | 2.65 ± 0.48 | 2.63 ± 0.51 | 0.66 |
| Vegetables and seeds | 3.27 ± 0.45 | 3.42 ± 0.70 | 0.41 |
| Meat (including fish) | 2.40 ± 0.64 | 2.29 ± 0.52 | 0.44 |
| Drinks (excluding water) | 2.14 ± 0.55 | 1.95 ± 0.52 | 0.22 |
| Highly-processed food products | 2.29 ± 0.42 | 2.44 ± 0.34 | 0.17 |
| Characteristics | PRO Group | PLC Group | p |
|---|---|---|---|
| MADRS score | 20.12 ± 5.38 | 17.7 ± 4.08 | 0.17 |
| DASS score | 61.24 ± 21.66 | 57.93 ± 19.71 | 0.58 |
| Depression | 20.41 ± 11.43 | 20.53 ± 8.84 | 0.88 |
| Anxiety | 16.59 ± 7.98 | 14.83 ± 6.85 | 0.55 |
| Stress | 24.24 ± 8.82 | 22.67 ± 10.36 | 0.60 |
| QoL score | 71.69 ± 12.88 | 73.07 ± 12.97 | 0.76 |
| Physical | 17.88 ± 4.69 | 19.23 ± 4.12 | 0.34 |
| Psychological | 13.75 ± 3.02 | 15.29 ± 4.14 | 0.29 |
| Social | 9.35 ± 2.26 | 8.00 ± 1.97 | 0.12 |
| Environment | 25.71 ± 4.96 | 25.71 ± 4.96 | 0.25 |
| Characteristics | PRO Group | PLC Group | p |
|---|---|---|---|
| Weight (kg) | 71.95 ± 17.26 | 70.92 ± 17.26 | 0.99 |
| BMI (kg/m2) | 24.29 ± 3.41 | 25.77 ± 5.98 | 0.49 |
| WC * (cm) | 86.46 ± 11.76 | 86.60 ± 15.85 | 0.90 |
| sBP * (mmHg) | 122.48 ± 16.77 | 120.19 ± 18.22 | 0.53 |
| dBP * (mmHg) | 83.28 ± 10.22 | 81.52 ± 9.38 | 0.66 |
| fGlc * (mmol/l) | 5.22 ± 0.54 | 5.09 ± 0.44 | 0.53 |
| HDL-c * (mmol/l) | 1.67 ± 0.46 | 1.56 ± 0.30 | 0.43 |
| TG * (mmol/l) | 1.19 ± 0.68 | 1.35 ± 0.52 | 0.10 |
| TG/HDL-c | 0.80 ± 0.56 | 0.95 ± 0.48 | 0.11 |
| AST (U/l) | 24.69 ± 6.17 | 24.27 ± 10.01 | 0.44 |
| ALT (U/l) | 22.52 ± 15.79 | 21.28 ± 16.28 | 0.83 |
| AST/ALT | 1.36 ± 0.49 | 1.32 ± 0.41 | 0.95 |
| APRI | 0.27 ± 0.10 | 0.25 ± 0.10 | 0.29 |
| FIB-4 | 0.73 ± 0.38 | 0.72 ± 0.36 | 0.93 |
| Characteristics | PRO Group | PLC Group | p |
|---|---|---|---|
| CRP (mg/L) | 2.37 ± 1.84 | 2.54 ± 2.55 | 0.65 |
| WBC (×103/µL) | 5.79 ± 1.31 | 6.25 ± 1.45 | 0.30 |
| NEU (×103/µL) | 3.13 ± 1.05 | 3.37 ± 1.03 | 0.39 |
| LYM (×103/µL) | 1.88 ± 0.55 | 2.12 ± 0.49 | 0.09 |
| PLT (×103/µL) | 278.12 ± 64.99 | 282.00 ± 48.51 | 0.34 |
| NEU/LYM | 1.87 ± 1.26 | 1.64 ± 0.51 | 0.89 |
| PLT/LYM | 158.10 ± 47.19 | 137.42 ± 34.34 | 0.06 |
| SII | 507.23 ± 305.66 | 455.90 ± 148.14 | 0.89 |
| Characteristics [mean ± SD] | V1 PRO-D | V2 PRO-D | Δ [95% CI] | V1 PLC-D | V2 PLC-D | Δ [95% CI] | V1 PRO-DMS | V2 PRO-DMS | Δ [95% CI] | V1 PLC-DMS | V2 PLC-DMS | Δ [95% CI] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MADRS score | 20.11 ± 5.21 | 14.63 ± 5.19 | −5.47 [−8.12, –2.81] | 17.15 ± 4.06 | 14.62 ± 6.19 | −2.54 [−5.57, 0.49] | 20.17 ± 6.40 | 19.67 ± 5.61 | −0.50 [−5.50, 4.50] | 19.00 ± 4.20 | 14.83 ± 6.55 | −4.17 [−8.83, 0.50] |
| DASS score | 62.25 ± 17.43 | 45.75 ± 20.12 | −16.50 [−31.10, −1.90] | 55.50 ± 17.14 | 41.00 ± 23.23 | −14.50 [−25.67′ −3.33] | 58.80 ± 32.10 | 54.00 ± 17.68 | −4.80 [−32.07, 22.47] | 62.80 ± 25.58 | 50.20 ± 24.63 | −12.6 [−32.52, 7.32] |
| Depression | 19.25 ± 10.12 | 15.00 ± 9.76 | −4.25 [−9.84, 1.34] | 19.60 ± 8.95 | 15.10 ± 8.74 | −4.50 [−9.52, 0.52] | 23.20 ± 15.07 | 21.60 ± 11.99 | −1.60 [−10.62, 7.42] | 22.40 ± 9.32 | 20.40 ± 10.67 | −2.00 [−9.24, 5.24] |
| Anxiety | 16.33 ± 7.24 | 10.08 ± 6.58 | −4.25 [−9.84, 1.34] | 14.30 ± 7.07 | 9.50 ± 7.79 | −4.50 [−9.52, 0.52] | 17.20 ± 10.47 | 13.20 ± 3.77 | −1.60 [−10.62, 7.42] | 15.60 ± 7.09 | 11.60 ± 5.55 | −2.00 [−9.24, 5.24] |
| Stress | 26.67 ± 6.91 | 20.67 ± 10.29 | −6.00 [−13.58, 1.58] | 21.60 ± 10.29 | 16.40 ± 10.75 | −5.20 [−10.18, −0.22] | 18.40 ± 10.95 | 19.20 ± 9.04 | 0.80 [−8.95, 10.55] | 24.80 ± 11.34 | 18.20 ± 9.28 | −6.60 [−16.86, 3.66] |
| QoL score | 71.73 ± 13.44 | 83.45 ± 9.41 | 11.73 [0.35, 23.11] | 76.70 ± 13.05 | 82.70 ± 15.23 | 6.00 [−0.23, 12.23] | 71.60 ± 13.05 | 69.80 ± 12.54 | −1.80 [−13.69, 10.09] | 64.00 ± 8.04 | 66.25 ± 9.43 | 2.25 [−1.93, 6.43] |
| Physical | 17.18 ± 5.17 | 20.73 ± 2.53 | 3.55 −0.22, 7.31] | 20.00 ± 4.28 | 23.00 ± 4.08 | 3.00 [0.57, 5.43] | 19.17 ± 3.71 | 20.00 ± 6.78 | 0.83 [−4.20, 5.86] | 16.75 ± 2.50 | 16.25 ± 2.36 | −0.50 [−4.71, 3.71] |
| Psychological | 13.73 ± 3.26 | 16.82 ± 3.25 | 3.09 [−0.01, 6.19] | 16.50 ± 3.92 | 17.40 ± 4.17 | 0.90 [−0.87, 2.67] | 13.80 ± 2.77 | 13.80 ± 2.86 | 0.00 [−1.76, 1.76] | 12.25 ± 3.30 | 13.00 ± 3.46 | 0.75 [−0.77, 2.27] |
| Social | 9.55 ± 2.25 | 10.18 ± 1.83 | 0.64 [−0.65, 1.92] | 8.38 ± 2.02 | 9.69 ± 1.97 | 1.31 [0.44, 2.18] | 9.00 ± 2.45 | 9.83 ± 2.48 | 0.83 [−0.97, 2.64] | 6.75 ± 1.26 | 7.00 ± 1.41 | 0.25 [0.55, 1.05] |
| Environment | 26.00 ± 4.43 | 29.27 ± 3.50 | 3.27 [−0.46, 7.00] | 23.62 ± 5.84 | 26.85 ± 6.38 | 3.23 0.48, 5.98] | 25.27 ± 6.24 | 25.67 ± 6.56 | 0.50 [−4.88, 5.88] | 24.35 ± 2.63 | 25.50 ± 4.36 | 1.25 [−2.03, 4,53] |
| Parameter [mean ±SD] | V1 PRO-D | V2 PRO-D | Δ [95% CI] | V1 PLC-D | V2 PLC-D | Δ [95% CI] | V1 PRO-DMS | V2 PRO-DMS | Δ [95% CI] | V1 PLC-DMS | V2 PLC-DMS | Δ [95% CI] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weight (kg) | 67.24 ± 10.55 | 67.71 ± 11.25 | 0.46 [−0.14, 1.06] | 63.04 ± 12.95 | 63.28 ± 12.82 | 0.24 [−0.53, 1.01] | 86.85 ± 21.66 | 85.83 ± 19.56 | −1.02 [−4.08, 2.05] | 89.32 ± 10.79 | 89.08 ± 11.23 | −0.23 [−2.57, 2.11] |
| BMI (kg/m2) | 23.29 ± 2.65 | 23.54 ± 2.86 | 0.13 [−0.08, 0.34] | 23.05 ± 4.46 | 23.13 ± 4.35 | 0.08 [−0.20, 0.36] | 28.07 ± 3.54 | 27.73 ± 2.95 | −0.34 [−1.53, 0.85] | 32.12 ± 3.86 | 31.37 ± 3.96 | −0.03 [−1.18, 1.11] |
| WC (cm) | 82.63 ± 9.90 | 82.03 ± 10.31 | −0.60 [−2.32, 1.11] | 79.79 ± 13.04 | 79.93 ± 12.85 | 0.14 [−1.59, 1.88] | 98.58 ± 8.90 | 99.00 ± 9.84 | 0.42 [−2.20, 3.04] | 102.50 ± 8.87 | 101..92 ± 7.53 | −0.58 [−7.29, 6.12] |
| sBP (mmHg) | 121.00 ± 16.69 | 121.37 ± 17.22 | 0.37 [−2.62, 3.36] | 116.07 ± 14.41 | 117.87 ± 11.58 | 1.80 [−3.59, 7.19] | 127.17 ± 17.66 | 124.50 ± 20.86 | −2.67 [−7.44, 2.10] | 130.50 ± 23.82 | 133.67 ± 14.00 | 3.17 [−10.11, 16.45] |
| dBP (mmHg) | 82.47 ± 9.91 | 81.00 ± 7.98 | −1.47 [−4.91, 1.97] | 79.60 ± 8.36 | 79.60 ± 7.59 | 0.00 [−3.50, 3.50] | 85.83 ± 11.72 | 85.17 ± 13.00 | −0.67 [−4.85, 3.51] | 86.33 ± 10.86 | 86.67 ± 10.93 | 0.33 [−5.36, 6.03] |
| fGlc (mmol/L) | 5.18 ± 0.59 | 5.10 ± 0.48 | −0.10 [−0.36, 0.15] | 4.92 ± 0.31 | 4.91 ± 0.46 | −0.02 [−0.21, 0.17] | 5.36 ± 0.32 | 5.27 ± 0.39 | −0.09 [−0.25, 0.07] | 5.51 ± 0.46 | 5.55 ± 0.59 | 0.04 [−0.63, 0.71] |
| HDL-c (mmol/L) | 1.75 ± 0.45 | 1.71 ± 0.37 | 0.07 [0.08, 0.22] | 1.61 ± 0.28 | 1.68 ± 0.28 | −0.14 [−0.32, 0.04] | 1.42 ± 0.44 | 1.47 ± 0.45 | −0.45 [−1.09, 0.19] | 1.44 ± 0.34 | 1.38 ± 0.29 | 0.53 [−0.50, 1.56] |
| TG (mmol/L) | 0.96 ± 0.29 | 1.03 ± 0.38 | −0.04 [−0.20, 0.11] | 1.24 ± 0.44 | 1.09 ± 0.42 | 0.06 [−0.03, 0.16] | 1.92 ± 1.05 | 1.47 ± 0.56 | 0.05 [−0.07, 0.16] | 1.65 ± 0.62 | 2.18 ± 1.15 | −0.06 [−0.21, 0.09] |
| TG/ HDL-c | 0.60 ± 0.29 | 0.63 ± 0.27 | 0.04 [−0.09, 0.17] | 0.81 ± 0.35 | 0.69 ± 0.33 | −0.12 [−0.25, 0.01] | 1.41 ± 0.76 | 1.05 ± 0.45 | −0.36 [−0.81, 0.09] | 1.40 ± 0.60 | 1.65 ± 0.84 | 0.46 [−0.40, 1.33] |
| AST (U/L) | 24.76 ± 5.69 | 23.51 ± 4.96 | −1.25 [−3.37, 0.86] | 21.98 ± 8.26 | 21.31 ± 6.31 | −0.67 [−2.54, 1.19] | 24.47 ± 8.14 | 24.58 ± 8.16 | 0.12 [−10.33, 10.56] | 29.98 ± 12.39 | 26.80 ± 12.22 | −3.18 [−6.65, 0.28] |
| ALT (U/L) | 20.71 ± 10.71 | 19.33 ± 8.52 | −1.38 [−4.24, 1.47] | 15.71 ± 6.38 | 17.12 ± 7.16 | 1.41 [−1.15, 3.98] | 28.25 ± 27.06 | 26.93 ± 26.37 | −1.32 [−12.77, 10.14] | 35.20 ± 24.91 | 34.02 ± 27.66 | −1.18 [−9.64, 7.27] |
| AST/ ALT | 1.38 ± 0.47 | 1.40 ± 0.60 | 0.03 [−0.13, 0.19] | 1.47 ± 0.38 | 1.31 ± 0.30 | −0.16 [−0.30, −0.02] | 1.31 ± 0.61 | 1.35 ± 0.70 | 0.04 [−0.54, 0.61] | 0.97 ± 0.28 | 0.98 ± 0.39 | 0.01 [−0.14, 0.16] |
| APRI | 0.27 ± 0.08 | 0.26 ± 0.08 | −0.01 [−0.04, 0.02] | 0.23 ± 0.08 | 0.23 ±0.07 | 0.005 [−0.02, 0.03] | 0.28 ± 0.16 | 0.27 ± 0.14 | −0.01 [−0.15, 0.13] | 0.31 ± 0.14 | 0.26 ± 0.12 | −0.05 [−0.14, 0.03] |
| FIB-4 | 0.72 ± 0.39 | 0.75 ± 0.41 | 0.02 [−0.03, 0.08] | 0.69 ± 0.34 | 0.66 ± 0.32 | −0.03 [−0.09, 0.03] | 0.74 ± 0.39 | 0.82 ± 0.65 | 0.075 [−0.23, 0.38] | 0.78 ± 0.44 | 0.65 ± 0.25 | −0.13 [−0.38, 0.11] |
| Parameter [mean ±SD] | V1 PRO-D | V2 PRO-D | Δ [95% CI] | V1 PLC-D | V2 PLC-D | Δ [95% CI] | V1 PRO-DMS | V2 PRO-DMS | Δ [95% CI] | V1 PLC-DMS | V2 PLC-DMS | Δ [95% CI] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CRP (mg/L) | 2.17 ± 1.88 | 1.53 ± 1.24 | −0.64 [−1.66, 0.38] | 1.91 ± 2.34 | 2.18 ± 2.03 | 0.27 [−0.59, 1.13] | 2.97 ± 1.72 | 2.53 ± 1.98 | −0.43 [−1.51, 0.65] | 4.32 ± 2.48 | 3.88 ± 2.04 | −0.44 [−5.18, 4.30] |
| WBC (×103/µL) | 5.88 ± 1.41 | 5.99 ± 1.51 | 0.11 [−0.44, 0.66] | 5.87 ± 1.07 | 6.13 ± 1.19 | 0.26 [−0.25, 0.77] | 5.52 ± 1.02 | 5.63 ± 1.53 | 0.11 [−0.57, 0.79] | 7.29 ± 1.97 | 7.41 ± 1.72 | 0.12 [−1.49, 1.72] |
| NEU (×103/µL) | 3.23 ± 1.16 | 3.29 ± 1.15 | 0.05 [−0.42, 0.52] | 3.06 ± 0.65 | 3.29 ± 0.73 | 0.23 [−0.19, 0.66] | 2.80 ± 0.58 | 2.94 ± 0.85 | 0.14 [−0.19, 0.465] | 4.22 ± 1.48 | 4.13 ± 0.99 | −0.09 [−1.19, 1.01] |
| LYM (×103/µL) | 1.83 ± 0.57 | 1.93 ± 0.55 | 0.09 [−0.07, 0.26] | 2.09 ± 0.51 | 2.13 ± 0.54 | 0.04 [−0.20, 0.28] | 2.04 ± 0.48 | 1.97 ± 0.54 | −0.06 [−0.35, 0.23] | 2.23 ± 0.47 | 2.37 ± 0.64 | 0.15 [−0.45, 0.75] |
| NEU /LYM | 2.02 ± 1.42 | 1.81 ± 0.74 | −0.20 [−0.78, 0.38] | 1.55 ± 0.49 | 1.63 ± 0.43 | 0.08 [−0.20, 0.36] | 1.43 ± 0.34 | 1.51 ± 0.26 | 0.09 [−0.06, 0.23] | 1.91 ± 0.50 | 1.80 ± 0.38 | −0.11 [−0.68, 0.46] |
| PLT | 271.47 ± 43.75 | 259.11 ± 47.68 | −12.37 [−22.42, −2.32] | 279.27 ± 45.05 | 275.53 ± 56.05 | −3.73 [−18.42, 10.95] | 299.17 ± 112.62 | 303.33 ± 105.85 | 4.17 [−15.34, 23.67] | 288.83 ± 60.42 | 305.33 ± 39.62 | 16.50 [−23.35, 56.35] |
| PLT /LYM | 161.27 ± 48.84 | 145.99 ± 48.43 | −15.29 [−36.77, 6.20] | 142.14 ± 38.89 | 136.14 ± 30.37 | −6.00 [−23.41, 11.41] | 148.57 ± 44.56 | 158.29 ± 43.53 | 9.72 [−18.29, 37.72] | 124.22 ± 9.79 | 130.14 ± 34.21 | 5.92 [−38.95, 50.79] |
| SII | 541.55 ± 344.05 | 482.12 ± 235.55 | −59.42 [−199.08, 80.23] | 432.21 ± 136.94 | 448.70 ± 133.64 | 16.49 [−70.82, 103.79] | 404.27 ± 101.82 | 439.22 ± 82.38 | 34.95 [−0.55, 70.45] | 522.24 ± 174.18 | 521.77 ± 104.44 | −0.47 [−227.57, 226.62] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gawlik-Kotelnicka, O.; Margulska, A.; Skowrońska, A.; Strzelecki, D. PRO-DEMET Randomized Controlled Trial on Probiotics in Depression—Pilot Study Results. Nutrients 2023, 15, 1400. https://doi.org/10.3390/nu15061400
Gawlik-Kotelnicka O, Margulska A, Skowrońska A, Strzelecki D. PRO-DEMET Randomized Controlled Trial on Probiotics in Depression—Pilot Study Results. Nutrients. 2023; 15(6):1400. https://doi.org/10.3390/nu15061400
Chicago/Turabian StyleGawlik-Kotelnicka, Oliwia, Aleksandra Margulska, Anna Skowrońska, and Dominik Strzelecki. 2023. "PRO-DEMET Randomized Controlled Trial on Probiotics in Depression—Pilot Study Results" Nutrients 15, no. 6: 1400. https://doi.org/10.3390/nu15061400
APA StyleGawlik-Kotelnicka, O., Margulska, A., Skowrońska, A., & Strzelecki, D. (2023). PRO-DEMET Randomized Controlled Trial on Probiotics in Depression—Pilot Study Results. Nutrients, 15(6), 1400. https://doi.org/10.3390/nu15061400