
How the Presence of a Doctor Known to Patients Impacts a Web-Based Intervention to Promote Physical Activity and Healthy Eating Behaviour in Individuals with an Overweight/Obesity–Hypertension Phenotype: A Randomised Clinical Trial
 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
Eligibility Criteria
2.2. Procedure
2.3. Intervention
2.4. Outcome Measures
2.5. Primary Outcome
2.6. Secondary Outcomes
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration. Rising rural body-mass index is the main driver of the global obesity epidemic in adults. Nature 2019, 569, 260–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [PubMed]
- Lotta, L.A.; Wittemans, L.B.L.; Zuber, V.; Stewart, I.D.; Sharp, S.J.; Luan, J.; Day, F.R.; Li, C.; Bowker, N.; Cai, L.; et al. Association of genetic variants related to gluteofemoral vs abdominal fat distribution with type 2 diabetes, coronary disease, and cardiovascular risk factors. JAMA 2018, 320, 2553–2563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical P. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). J. Hypertens. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Diffusion of eHealth: Making Universal Health Coverage 356 Achievable; World Health Organization: Geneva, Switzerland, 2016; 160p. [Google Scholar]
- Oh, H.; Rizo, C.; Enkin, M.; Jadad, A. What is eHealth (3): A systematic review of published definitions. J. Med. Internet Res. 2005, 7, 1–12. [Google Scholar] [CrossRef]
- Lewis, B.A.; Williams, D.M.; Neighbors, C.J.; Jakicic, J.M.; Marcus, B.H. Cost analysis of Internet vs. print interventions for physical activity promotion. Psychol. Sport Exerc. 2010, 11, 246–249. [Google Scholar] [CrossRef] [Green Version]
- Joseph, R.P.; Durant, N.H.; Benitez, T.J.; Pekmezi, D.W. Internet-Based Physical Activity Interventions. Am. J. Lifestyle Med. 2014, 8, 42–67. [Google Scholar] [CrossRef] [Green Version]
- Kodama, S.; Saito, K.; Tanaka, S.; Horikawa, C.; Fujiwara, K.; Hirasawa, R.; Yachi, Y.; Iida, K.T.; Shimano, H.; Ohashi, Y.; et al. Effect of web-based lifestyle modification on weight control: A meta-analysis. Int. J. Obes. 2012, 36, 675–685. [Google Scholar] [CrossRef] [Green Version]
- Wieland, L.; Falzon, L.; Sciamanna, C.N.; Trudeau, K.J.; Folse, S.B.; Schwartz, J.E.; Davidson, K.W. Interactive computer-based interventions for weight loss or weight maintenance in overweight or obese people (Review). Cochrane Database Syst. Rev. 2012, 8, CD007675. [Google Scholar]
- Vegting, I.L.; Schrijver, E.J.M.; Otten, R.H.J.; Nanayakkara, P.W.B. Internet programs targeting multiple lifestyle interventions in primary and secondary care are not superior to usual care alone in improving cardiovascular risk profile: A systematic review. Eur. J. Intern. Med. 2014, 25, 73–81. [Google Scholar] [CrossRef]
- Liu, S.; Dunford, S.D.; Leung, Y.W.; Brooks, D.; Thomas, S.G.; Eysenbach, G.; Nolan, R.P. Reducing blood pressure with internet-based interventions: A meta-analysis. Can. J. Cardiol. 2013, 29, 613–621. [Google Scholar] [CrossRef]
- Park, M.J.; Kim, H.S.; Kim, K.S. Cellular phone and Internet-based individual intervention on blood pressure and obesity in obese patients with hypertension. Int. J. Med. Inform. 2009, 78, 704–710. [Google Scholar] [CrossRef]
- Bennett, G.G.; Herring, S.J.; Puleo, E.; Stein, E.K.; Emmons, K.M.; Gillman, M.W. Web-based weight loss in primary care: A randomized controlled trial. Obesity 2010, 18, 308–313. [Google Scholar] [CrossRef]
- Mensorio, M.S.; Cebolla-Martí, A.; Rodilla, E.; Palomar, G.; Lisón, J.F.; Botella, C.; Fernández-Aranda, F.; Jimenez-Murcia, S.; Baños, R.M. Analysis of the efficacy of an internet-based self-administered intervention (“Living Better”) to promote healthy habits in a population with obesity and hypertension: An exploratory randomized controlled trial. Int. J. Med. Inform. 2019, 124, 13–23. [Google Scholar] [CrossRef]
- Lisón, J.F.; Palomar, G.; Mensorio, M.S.; Baños, R.M.; Cebolla-Martí, A.; Botella, C.; Benavent-Caballer, V.; Rodilla, E. Impact of a web-based exercise and nutritional education intervention in patients who are obese with hypertension: Randomized wait-list controlled trial. J. Med. Internet Res. 2020, 22, e14196. [Google Scholar] [CrossRef]
- Múzquiz-Barberá, P.; Ruiz-Cortés, M.; Herrero, R.; Vara, M.D.; Escrivá-Martínez, T.; Carcelén, R.; Baños, R.M.; Rodilla, E.; Lisón, J.F. The Impact of a Web-Based Lifestyle Educational Program (‘Living Better’) Reintervention on Hypertensive Overweight or Obese Patients. Nutrients 2022, 14, 2235. [Google Scholar] [CrossRef]
- Tuong, W.; Larsen, E.R.; Armstrong, A.W. Videos to influence: A systematic review of 384 effectiveness of video-based education in modifying health behaviors. J. Behav. Med. 2014, 37, 218–233. [Google Scholar] [CrossRef]
- Oberg, E.B.; Frank, E. Physicians’ health practices strongly influence patient health practices. J. R. Coll. Physicians Edinb. 2009, 39, 290–291. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.A.; Hearld, L.R.; Mittler, J.N.; Harvey, J. Patient-physician role relationships and patient activation among individuals with chronic illness. Health Serv. Res. 2012, 47, 1201–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordgren, L.B.; Carlbring, P.; Linna, E.; Andersson, G. Role of the working alliance on treatment outcome in tailored internet-based cognitive behavioural therapy for anxiety disorders: Randomized controlled pilot trial. JMIR Res. Protoc. 2013, 2, e2292. [Google Scholar]
- Moher, D.; Schulz, K.; Altman, D. The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomized trials. J. Am. Pediatr. Med. Assoc. 2001, 91, 437–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baños, R.M.; Mensorio, M.S.; Cebolla, A.; Rodilla, E.; Palomar, G.; Lisón, J.; Botella, C. An internet-based self-administered intervention for promoting healthy habits and weight loss in hypertensive people who are overweight or obese: A randomized controlled trial. BMC Cardiovasc. Disord. 2015, 15, 83. [Google Scholar] [CrossRef] [Green Version]
- Román Viñas, B.; Ribas Barba, L.; Ngo, J.; Serra Majem, L. Validity of the international physical activity questionnaire in the Catalan population (Spain). Gac. Sanit. 2013, 27, 254–257. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Muñoz, S.; Corella, C.; Abarca-Sos, A.; Zaragoza, J. Validation of three short physical activity questionnaires with accelerometers among university students in Spain. J. Sports Med. Phys. Fit. 2017, 57, 1660–1668. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Markland, D.; Tobin, V. A modification to behavioural regulation in exercise questionnaire to include an assessment of amotivation. J. Sport Exerc. Psychol. 2004, 26, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Moreno, J.; Cervelló, E.; Martínez, A. Measuring self-determination motivation in a physical fitness setting; Validation of the behavioural regulation in exercise questionnaire-2 (BREQ-2) in a Spanish sample. J. Sports Med. Phys. Fit. 2006, 47, 366–378. [Google Scholar]
- Duncan, L.R.; Hall, C.R.; Wilson, P.M.; Jenny, O. Exercise motivation: A cross-sectional analysis examining its relationships with frequency, intensity, and duration of exercise. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and selfdetermination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [Green Version]
- Vanroy, J.; Seghers, J.; Van Uffelen, J.; Boen, F. Can a framed intervention motivate older adults in assisted living facilities to exercise? BMC Geriatr. 2019, 19, 46. [Google Scholar] [CrossRef]
- Carcelén, R.; Navarro, J.; Juesas, A.; Baños, R.M.; Colado, J.C.; Lisón, J.F. Effects of different strength training intensities on health-related parameters towards engaging in physical activity in elderly. Cult. Cienc. Deporte 2022, 17, 21–30. [Google Scholar]
- Van Strien, T.; Frijters, J.; Bergers, G.; Defares, P. The Dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Cebolla, A.; Barrada, J.; van Strien, T.; Oliver, E.; Baños, R. Validation of the Dutch eating behavior questionnaire (DEBQ) in a sample of Spanish women. Appetite 2014, 73, 58–64. [Google Scholar] [CrossRef]
- Van Strien, T.; Cebolla, A.; Etchemendy, E.; Gutiérrez-Maldonado, J.; Ferrer-García, M.; Botella, C.; Baños, R. Emotional eating and food intake after sadness and joy. Appetite 2013, 66, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Bongers, P.; de Graaff, A.; Jansen, A. “Emotional” does not even start to cover it: Generalization of overeating in emotional eaters. Appetite 2016, 96, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Koenders, P.G.; Van Strien, T. Emotional eating, rather than lifestyle behavior, drives weight gain in a prospective study in 1562 employees. J. Occup. Environ. Med. 2011, 53, 1287–1293. [Google Scholar] [CrossRef]
- Snoek, H.M.; Van Strien, T.; Janssens, J.M.A.M.; Engels, R.C.M.E. Emotional, external, restrained eating and overweight in Dutch adolescents. Scand. J. Psychol. 2007, 48, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Baños, R.; Cebolla, A.; Moragrega, I.; Van Strien, T.; Fernández-Aranda, F.; Agüera, Z.; Botella, C. Relationship between eating styles and temperament in an anorexia nervosa, healthy control, and morbid obesity female sample. Appetite 2014, 76, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. E ects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Ghosh, A.; Arora, B.; Gupta, R.; Anoop, S.; Misra, A. Effects of nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes Metab. Syndr. 2020, 14, 917–920. [Google Scholar] [CrossRef]
- Mieziene, B.; Burkaite, G.; Emeljanovas, A.; Tilindiene, I.; Novak, D.; Kawachi, I. Adherence to Mediterranean diet among Lithuanian and Croatian students during COVID-19 pandemic and its health behavior correlates. Front. Public Health 2022, 10, 1000161. [Google Scholar] [CrossRef]
- Neville, L.; O’Hara, B.; Milat, A. Computer-tailored physical activity behavior change interventions targeting adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 30. [Google Scholar] [CrossRef] [Green Version]
- Biviá-Roig, G.; Boldó-Roda, A.; Blasco-Sanz, R.; Serrano-Raya, L.; DelaFuente-Díez, E.; Múzquiz-Barberá, P.; Lisón, J.F. Impact of the COVID-19 Pandemic on the Lifestyles and Quality of Life of Women With Fertility Problems: A Cross-Sectional Study. Front. Public Health 2021, 9, 686115. [Google Scholar] [CrossRef]
- Biviá-Roig, G.; Soldevila-Matías, P.; Haro, G.; González-Ayuso, V.; Arnau, F.; Peyró-Gregori, L.; García-Garcés, L.; Sánchez-López, M.I.; Lisón, J.F. The Impact of the COVID-19 Pandemic on the Lifestyles and Levels of Anxiety and Depression of Patients with Schizophrenia: A Retrospective Observational Study. Healthcare 2022, 10, 128. [Google Scholar] [CrossRef]
- Wunsch, K.; Kienberger, K.; Niessner, C. Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 2250. [Google Scholar] [CrossRef]
- Pérez-Gisbert, L.; Torres-Sánchez, I.; Ortiz-Rubio, A.; Calvache-Mateo, A.; López-López, L.; Cabrera-Martos, I.; Valenza, M.C. Effects of the COVID-19 Pandemic on Physical Activity in Chronic Diseases: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12278. [Google Scholar] [CrossRef]
- Richardson, C.R.; Buis, L.R.; Janney, A.W.; Goodrich, D.E.; Sen, A.; Hess, M.L.; Mehari, K.S.; Fortlage, L.A.; Resnick, P.J.; Zikmund-Fisher, B.J.; et al. An online community improves adherence in an internet-mediated walking program. Part 1: Results of a randomized controlled trial. J. Med. Internet Res. 2010, 12, e71. [Google Scholar] [CrossRef]
- Pietrzak, E.; Cotea, C.; Pullman, S. Primary and secondary prevention of cardiovascular disease: Is there a place for Internet-based interventions? J. Cardiopulm. Rehabil. Prev. 2014, 34, 303–317. [Google Scholar] [CrossRef]
- Richard, E.; Jongstra, S.; Soininen, H.; Brayne, C.; Moll van Charante, E.P.; Meiller, Y.; van der Groep, B.; Beishuizen, C.R.; Mangialasche, F.; Barbera, M.; et al. Healthy ageing through internet counselling in the elderly: The HATICE randomised controlled trial for the prevention of cardiovascular disease and cognitive impairment. BMJ Open 2016, 6, e010806. [Google Scholar] [CrossRef] [Green Version]
- Castelnuovo, G.; Manzoni, G.M.; Cuzziol, P.; Cesa, G.L.; Tuzzi, C.; Villa, V.; Liuzzi, A.; Petroni, M.L.; Molinari, E. TECNOB: Study design of a randomized controlled trial of a multidisciplinary telecare intervention for obese patients with type-2 diabetes. BMC Public Health 2010, 10, 204. [Google Scholar] [CrossRef] [Green Version]
- Staffileno, B.A.; Tangney, C.C.; Fogg, L. Favorable outcomes using an eHealth approach to promote physical activity and nutrition among young African American women. J. Cardiovasc. Nurs. 2018, 33, 62–71. [Google Scholar] [CrossRef]
- Seo, D.; Niu, J. Evaluation of internet-based interventions on waist circumference reduction: A meta-analysis. J. Med. Internet Res. 2015, 17, e181. [Google Scholar] [CrossRef] [Green Version]
- Hesse, B.W.; Nelson, D.E.; Kreps, G.L.; Croyle, R.T.; Arora, N.K.; Rimer, B.K.; Viswanath, K. Trust and sources of health information: The impact of the Internet and its implications for health care providers: Findings from the first Health Information National Trends Survey. Arch. Intern. Med. 2005, 165, 2618–2624. [Google Scholar] [CrossRef] [Green Version]
- DiMatteo, M.R. Variations in patients’ adherence to medical recommendations: A quantitative review of 50 years of research. Med. Care 2004, 42, 200–209. [Google Scholar] [CrossRef]
- Falagas, M.E.; Zarkadoulia, E.A.; Pliatsika, P.A.; Panos, G. Socioeconomic status (SES) as a determinant of adherence to treatment in HIV infected patients: A systematic review of the literature. Retrovirology 2008, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Adams, S.A.; Matthews, C.E.; Ebbeling, C.B.; Moore, C.G.; Cunningham, J.E.; Fulton, J. The effect of social desirability and social approval on self-reports of physical activity. Am. J. Epidemiol. 2005, 161, 389–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McConnon, Á.; Kirk, S.; Cockroft, J.; Harvey, E.; Greenwood, D.; Thomas, J.; Bojke, L. The internet for weight control in an obese sample: Results of a randomised controlled trial. BMC Health Serv. Res. 2007, 7, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wantland, D.; Portillo, C.; Holzemer, W.; Slaughter, R.; McGhee, E. The effectiveness of web-based vs. non-web-based interventions: A meta-analysis of behavioral change outcomes. J. Med. Internet Res. 2004, 6, e40. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | |||
|---|---|---|---|
| Control (n = 62) | Experimental (n = 70) | p | |
| Age (years) | 57.7 (10.7) | 56.2 (9.5) | 0.397 |
| Men/women (n) | 34/28 | 38/32 | 0.949 |
| Specialist visits (n) | 9.8 (8.3) | 9.4 (7.9) | 0.819 |
| BMI | 29.7 (3.2) | 29.5 (3.6) | 0.787 |
| Physical activity (IPAQ) METs | 2692 (3299) | 3046 (3220) | 0.542 |
| Adherence to the Mediterranean diet (MEDAS) | 8.1 (2.0) | 8.4 (2.0) | 0.388 |
| Motivation to change eating habits | |||
| Intrinsic | 9.5 (3.9) | 9.7 (4.4) | 0.857 |
| Identified | 9.8 (2.4) | 10.1 (2.1) | 0.463 |
| Introjected | 5.6 (3.0) | 6.5 (3.4) | 0.145 |
| External | 3.5 (3.8) | 4.0 (3.9) | 0.476 |
| Amotivation | 1.6 (2.9) | 1.8 (3.1) | 0.706 |
| Motivation towards PA | |||
| Intrinsic | 10.3 (4.2) | 10.8 (4.6) | 0.477 |
| Identified | 10.5 (2.7) | 11.2 (3.2) | 0.245 |
| Introjected | 5.6 (3.6) | 5.4 (3.6) | 0.662 |
| External | 4.7 (4.1) | 3.8 (3.9) | 0.194 |
| Amotivation | 2.5 (3.5) | 2.0 (2.9) | 0.461 |
| Eating style (DEBQ) | |||
| Emotional | 29.5 (12.4) | 30.3 (13.9) | 0.745 |
| Restrictive | 26.0 (8.1) | 27.4 (8.3) | 0.332 |
| External | 28.6 (7.6) | 27.7 (8.8) | 0.551 |
| Group | ANOVA Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control (n = 62) | Experimental (n = 70) | Time | Group | Time × Group | |||||||
| Pre | Post | Pre | Post | F | p | F | p | F | p | ηp2 | |
| BMI | 29.7 (3.2) | 29.4 (3.5) | 29.5 (3.6) | 29.1 (3.6) | 26.3 | 0.000 | 0.118 | 0.732 | 0.481 | 0.489 | 0.004 |
| Physical activity (IPAQ) METS | 2692 (3299) | 2931 (3049) | 3046 (3220) | 3429 (3179) | 3.40 | 0.068 | 0.620 | 0.433 | 0.182 | 0.670 | 0.001 |
| Adherence to the Mediterranean diet (MEDAS) | 8.1 (2.0) | 8.5 (2.1) | 8.4 (2.0) | 8.5 (2.1) | 7.44 | 0.007 | 0.236 | 0.628 | 2.04 | 0.156 | 0.017 |
| Motivation to change eating habits | |||||||||||
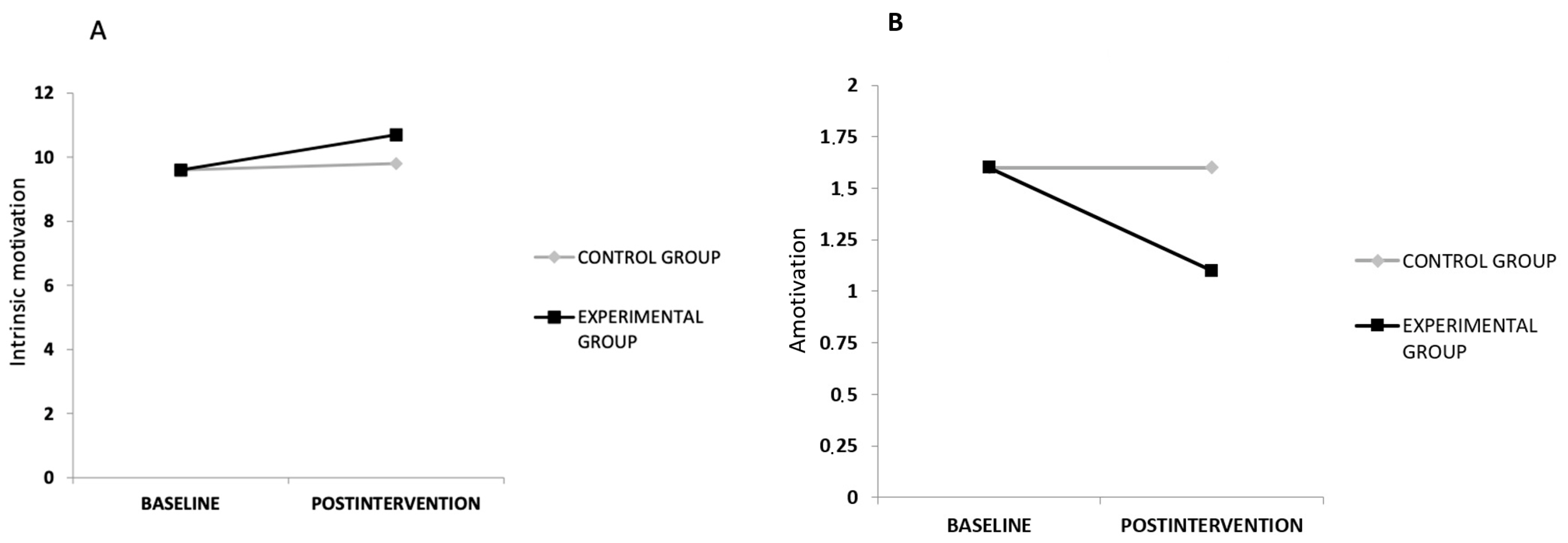
| Intrinsic | 9.5 (3.9) | 9.8 (4.1) | 9.7 (4.4) | 10.8 (3.9) | 11.1 | 0.001 | 0.596 | 0.442 | 3.92 | 0.050 | 0.032 |
| Identified | 9.8 (2.4) | 9.9 (2.5) | 10.1 (2.1) | 10.6 (1.9) | 2.99 | 0.086 | 1.74 | 0.189 | 2.54 | 0.114 | 0.021 |
| Introjected | 5.6 (3.0) | 5.7 (3.2) | 6.5 (3.4) | 6.7 (3.5) | 0.741 | 0.391 | 2.81 | 0.096 | 0.134 | 0.715 | 0.001 |
| External | 3.5 (3.8) | 3.0 (3.6) | 4.0 (3.9) | 3.7 (3.9) | 1.57 | 0.212 | 0.894 | 0.346 | 0.152 | 0.697 | 0.001 |
| Amotivation | 1.6 (2.9) | 1.6 (2.9) | 1.8 (3.1) | 1.1 (2.3) | 4.43 | 0.037 | 0.082 | 0.775 | 4.43 | 0.037 | 0.036 |
| Motivation towards PA | |||||||||||
| Intrinsic | 10.3 (4.2) | 10.4 (4.4) | 10.8 (4.6) | 10.6 (4.5) | 0.016 | 0.899 | 0.228 | 0.634 | 0.981 | 0.324 | 0.008 |
| Identified | 10.5 (2.7) | 10.8 (2.8) | 11.2 (3.2) | 11.4 (2.8) | 2.83 | 0.095 | 1.51 | 0.220 | 0.006 | 0.940 | 0.000 |
| Introjected | 5.6 (3.6) | 5.9 (3.5) | 5.4 (3.6) | 5.3 (3.6) | 0.141 | 0.708 | 0.546 | 0.462 | 0.506 | 0.478 | 0.004 |
| External | 4.7 (4.1) | 4.1 (4.0) | 3.8 (3.9) | 3.3 (3.9) | 4.86 | 0.029 | 1.83 | 0.178 | 0.017 | 0.898 | 0.000 |
| Amotivation | 2.5 (3.5) | 2.0 (3.2) | 2.0 (2.9) | 1.7 (2.7) | 4.19 | 0.043 | 0.424 | 0.516 | 0.203 | 0.653 | 0.002 |
| Eating style (DEBQ) | |||||||||||
| Emotional | 29.5 (12.4) | 28.7 (12.0) | 30.3 (13.9) | 29.9 (14.3) | 1.37 | 0.243 | 0.180 | 0.672 | 0.150 | 0.699 | 0.001 |
| Restrictive | 26.0 (8.1) | 26.0 (8.4) | 27.4 (8.3) | 27.4 (6.9) | 0.000 | 0.985 | 1.11 | 0.293 | 0.000 | 0.985 | 0.000 |
| External | 28.6 (7.6) | 27.2 (8.2) | 27.7 (8.8) | 26.6 (8.5) | 10.7 | 0.001 | 0.265 | 0.608 | 0.155 | 0.695 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Cortés, M.; Múzquiz-Barberá, P.; Herrero, R.; Vara, M.D.; Escrivá-Martínez, T.; Carcelén, R.; Rodilla, E.; Baños, R.M.; Lisón, J.F. How the Presence of a Doctor Known to Patients Impacts a Web-Based Intervention to Promote Physical Activity and Healthy Eating Behaviour in Individuals with an Overweight/Obesity–Hypertension Phenotype: A Randomised Clinical Trial. Nutrients 2023, 15, 1624. https://doi.org/10.3390/nu15071624
Ruiz-Cortés M, Múzquiz-Barberá P, Herrero R, Vara MD, Escrivá-Martínez T, Carcelén R, Rodilla E, Baños RM, Lisón JF. How the Presence of a Doctor Known to Patients Impacts a Web-Based Intervention to Promote Physical Activity and Healthy Eating Behaviour in Individuals with an Overweight/Obesity–Hypertension Phenotype: A Randomised Clinical Trial. Nutrients. 2023; 15(7):1624. https://doi.org/10.3390/nu15071624
Chicago/Turabian StyleRuiz-Cortés, Marta, Pedro Múzquiz-Barberá, Rocío Herrero, María Dolores Vara, Tamara Escrivá-Martínez, Raquel Carcelén, Enrique Rodilla, Rosa María Baños, and Juan Francisco Lisón. 2023. "How the Presence of a Doctor Known to Patients Impacts a Web-Based Intervention to Promote Physical Activity and Healthy Eating Behaviour in Individuals with an Overweight/Obesity–Hypertension Phenotype: A Randomised Clinical Trial" Nutrients 15, no. 7: 1624. https://doi.org/10.3390/nu15071624
APA StyleRuiz-Cortés, M., Múzquiz-Barberá, P., Herrero, R., Vara, M. D., Escrivá-Martínez, T., Carcelén, R., Rodilla, E., Baños, R. M., & Lisón, J. F. (2023). How the Presence of a Doctor Known to Patients Impacts a Web-Based Intervention to Promote Physical Activity and Healthy Eating Behaviour in Individuals with an Overweight/Obesity–Hypertension Phenotype: A Randomised Clinical Trial. Nutrients, 15(7), 1624. https://doi.org/10.3390/nu15071624