
Anti-SARS-CoV-2 Immunoglobulins in Human Milk after Coronavirus Disease or Vaccination—Time Frame and Duration of Detection in Human Milk and Factors That Affect Their Titers: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
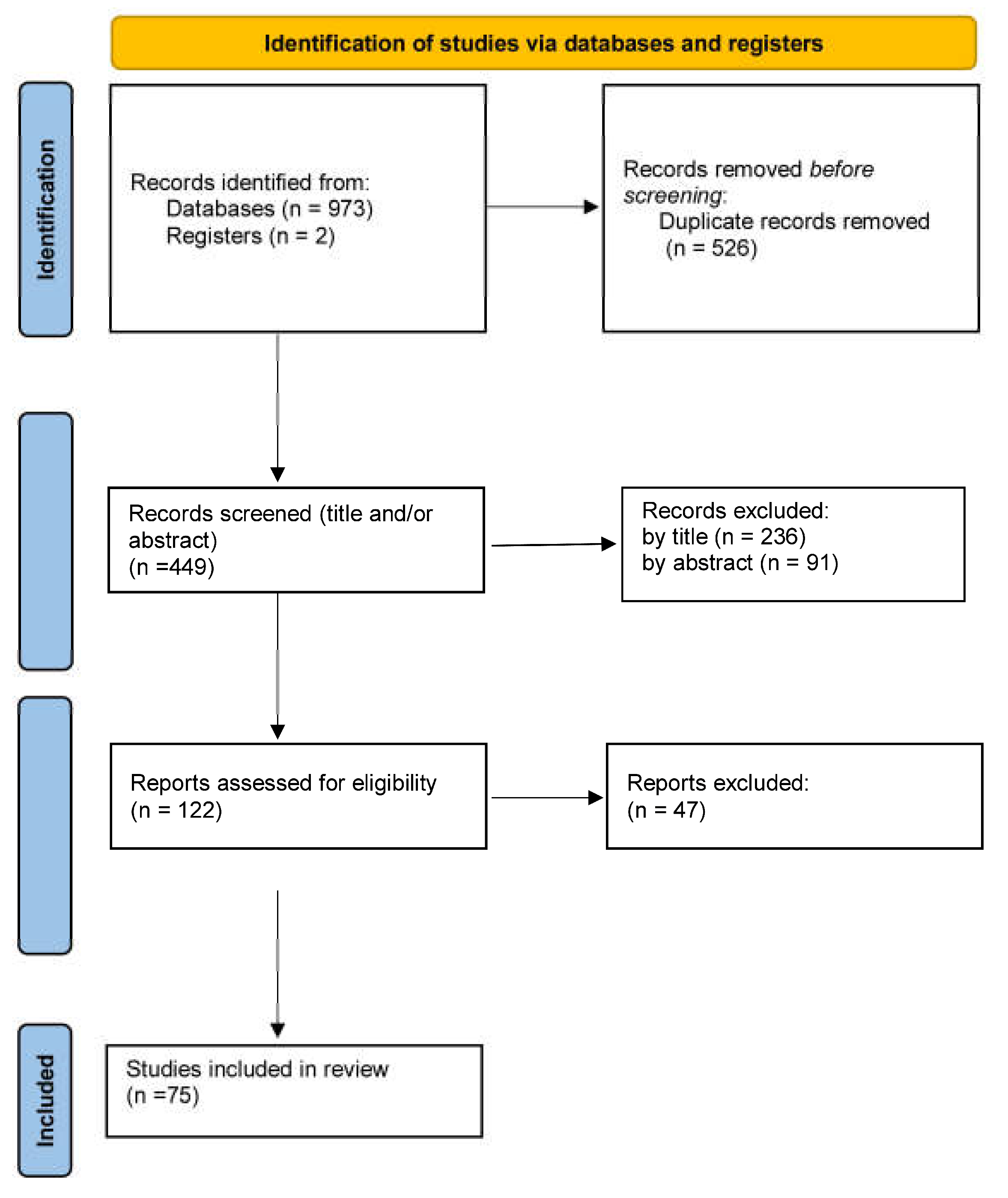
2. Materials and Methods
2.1. Study Eligibility Criteria
2.2. Data Extraction
3. Results
4. Discussion
4.1. Post Infection Immune Response
4.1.1. Anti-SARS-CoV-2 IgA Immunoglobulins
4.1.2. Anti-SARS-CoV-2 IgM Immunoglobulins
4.1.3. Anti-SARS-CoV-2 IgG Immunoglobulins
4.2. Post Vaccination Immune Response
4.2.1. Anti-SARS-CoV-2 IgG Immunoglobulins
4.2.2. Anti-SARS-CoV-2 IgA Immunoglobulins
4.2.3. Anti-SARS-CoV-2 IgM immunoglobulins
4.3. Differences in Immune Response after Infection or Vaccination
4.4. Differences in Immune Response According to Vaccine Type
4.5. Neutralizing Capacity
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 7 February 2023).
- Newborn Mortality. Available online: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-mortality-report-2021 (accessed on 7 February 2023).
- COVID-19 Vaccination for Children|CDC. Available online: https://www.cdc.gov/vaccines/covid-19/planning/children.html (accessed on 7 February 2023).
- Dimitroglou, M.; Iliodromiti, Z.; Christou, E.; Volaki, P.; Petropoulou, C.; Sokou, R.; Boutsikou, T.; Iacovidou, N. Human Breast Milk: The Key Role in the Maturation of Immune, Gastrointestinal and Central Nervous Systems: A Narrative Review. Diagnostics 2022, 12, 2208. [Google Scholar] [CrossRef] [PubMed]
- Clinical Management of COVID-19: Interim Guidance, 27 May 2020. Available online: https://apps.who.int/iris/handle/10665/332196 (accessed on 14 November 2022).
- Halasa, N.B.; Olson, S.M.; Staat, M.A.; Newhams, M.M.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Cameron, M.A.; Pannaraj, P.S.; Bline, K.E.; et al. Effectiveness of Maternal Vaccination with MRNA COVID-19 Vaccine during Pregnancy against COVID-19-Associated Hospitalization in Infants Aged. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Yang, C.; Xu, X.-F.; Xu, W.; Liu, S.-W. Structural and Functional Properties of SARS-CoV-2 Spike Protein: Potential Antivirus Drug Development for COVID-19. Acta Pharmacol. Sin. 2020, 41, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Lu, S.; Corbett, K.D. Structural Basis for SARS-CoV-2 Nucleocapsid Protein Recognition by Single-Domain Antibodies. Front. Immunol. 2021, 12, 719037. [Google Scholar] [CrossRef]
- Batra, M.; Tian, R.; Zhang, C.; Clarence, E.; Sacher, C.S.; Miranda, J.N.; De La Fuente, J.R.O.; Mathew, M.; Green, D.; Patel, S.; et al. Role of IgG against N-Protein of SARS-COV2 in COVID-19 Clinical Outcomes. Sci. Rep. 2021, 11, 3455. [Google Scholar] [CrossRef]
- Cafaro, A.; Sangster, M.; Yuan, M.; Shah, P.; Canziani, G.A.; Carter, E.P.; Chaiken, I. The Case for S2: The Potential Benefits of the S2 Subunit of the SARS-CoV-2 Spike Protein as an Immunogen in Fighting the COVID-19 Pandemic. Front. Immunol. 2021, 1, 637651. [Google Scholar] [CrossRef]
- Nicolaidou, V.; Georgiou, R.; Christofidou, M.; Felekkis, K.; Pieri, M.; Papaneophytou, C. Detection of SARS-CoV-2-Specific Antibodies in Human Breast Milk and Their Neutralizing Capacity after COVID-19 Vaccination: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 2957. [Google Scholar] [CrossRef]
- Whited, N.; Cervantes, J. Antibodies against SARS-CoV-2 in Human Breast Milk after Vaccination: A Systematic Review and Meta-Analysis. Breastfeed. Med. 2022, 17, 475–483. [Google Scholar] [CrossRef]
- Low, J.M.; Low, Y.W.; Zhong, Y.; Lee, C.Y.C.; Chan, M.; Ng, N.B.H.; Amin, Z.; Ng, Y.P.M. Titres and Neutralising Capacity of SARS-CoV-2-Specific Antibodies in Human Milk: A Systematic Review. Arch. Dis. Child. Fetal Neonatal Ed. 2022, 107, F1–F7. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Narayanaswamy, V.; Pentecost, B.; Alfandari, D.; Chin, E.; Minor, K.; Kastrinakis, A.; Lieberman, T.; Arcaro, K.F.; Leftwich, H. Humoral and Cell-Mediated Immune Response in Colostrum from Women Diagnosed Positive for SARS-CoV-2. Breastfeed. Med. 2021, 16, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Larcade, R.; DeShea, L.; Lang, G.A.; Caballero, M.T.; Ferretti, A.; Beasley, W.H.; Tipple, T.E.; Vain, N.; Prudent, L.; Lang, M.L.; et al. Maternal-Fetal Immunologic Response to SARS-CoV-2 Infection in a Symptomatic Vulnerable Population: A Prospective Cohort. J. Infect. Dis. 2021, 225, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.; Marino, J.; Amanat, F.; Krammer, F.; Hahn-Holbrook, J.; Zolla-Pazner, S.; Powell, R.L. Robust and Specific Secretory IgA against SARS-CoV-2 Detected in Human Milk. iScience 2020, 23, 101735. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wang, S.; Zeng, W.; Chen, S.; Wu, J.; Lin, X.; Liu, Y.; Sun, Z.; Feng, L. Clinical and Immunologic Features among COVID-19-Affected Mother-Infant Pairs: Antibodies to SARS-CoV-2 Detected in Breast Milk. New Microbes New Infect. 2020, 37, 100752. [Google Scholar] [CrossRef] [PubMed]
- Bobik, T.V.; Kostin, N.N.; Skryabin, G.A.; Tsabai, P.N.; Simonova, M.A.; Knorre, V.D.; Mokrushina, Y.A.; Smirnov, I.V.; Kosolapova, J.A.; Vtorushina, V.V.; et al. Epitope-Specific Response of Human Milk Immunoglobulins in COVID-19 Recovered Women. Pathogens 2021, 10, 705. [Google Scholar] [CrossRef]
- Peng, S.; Zhu, H.; Yang, L.; Cao, L.; Huang, X.; Dynes, M.; Narayan, A.; Xia, J.; Chen, Y.; Zhang, P.; et al. A Study of Breastfeeding Practices, SARS-CoV-2 and Its Antibodies in the Breast Milk of Mothers Confirmed with COVID-19. Lancet Reg. Health -West. Pacific 2020, 4, 100045. [Google Scholar] [CrossRef]
- Bäuerl, C.; Randazzo, W.; Sánchez, G.; Selma-Royo, M.; García Verdevio, E.; Martínez, L.; Parra-Llorca, A.; Lerin, C.; Fumadó, V.; Crovetto, F.; et al. SARS-CoV-2 RNA and Antibody Detection in Breast Milk from a Prospective Multicentre Study in Spain. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 107, 216–221. [Google Scholar] [CrossRef]
- Collier, A.R.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Apraku Bondzie, E.; Sellers, D.; et al. Immunogenicity of COVID-19 MRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370–2380. [Google Scholar] [CrossRef]
- Conti, M.G.; Terreri, S.; Piano Mortari, E.; Albano, C.; Natale, F.; Boscarino, G.; Zacco, G.; Palomba, P.; Cascioli, S.; Corrente, F.; et al. Immune Response of Neonates Born to Mothers Infected with SARS-CoV-2. JAMA Netw. Open 2021, 4, e2132563. [Google Scholar] [CrossRef]
- Luo, Q.Q.; Xia, L.; Yao, D.J.; Wu, M.; Wang, H.B.; Luo, M.H.; Jiang, X.; Chen, H. Breastfeeding in Mothers with COVID-19: Insights from Laboratory Tests and Follow-up from Early Outbreak of the Pandemic in China. J. Women’s Health 2021, 30, 1546–1555. [Google Scholar] [CrossRef]
- Conti, M.G.; Terreri, S.; Terrin, G.; Natale, F.; Pietrasanta, C.; Salvatori, G.; Brunelli, R.; Midulla, F.; Papaevangelou, V.; Carsetti, R.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 Infection versus Vaccination in Pregnancy: Implications for Maternal and Infant Immunity. Clin. Infect. Dis. 2022, 75, S37–S45. [Google Scholar] [CrossRef] [PubMed]
- Decenti, E.C.; Salvatore, M.A.; Mancon, A.; Portella, G.; Rocca, A.; Vocale, C.; Donati, S. A Large Series of Molecular and Serological Specimens to Evaluate Mother-to-Child SARS-CoV-2 Transmission: A Prospective Study from the Italian Obstetric Surveillance System. Int. J. Infect. Dis. 2022, 126, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Olearo, F.; Radmanesh, L.S.; Felber, N.; von Possel, R.; Emmerich, P.; Pekarek, N.; Pfefferle, S.; Nörz, D.; Hansen, G.; Diemert, A.; et al. Anti-SARS-CoV-2 Antibodies in Breast Milk during Lactation after Infection or Vaccination: A Cohort Study. J. Reprod. Immunol. 2022, 153, 103685. [Google Scholar] [CrossRef]
- Szczygioł, P.; Łukianowski, B.; Kościelska-Kasprzak, K.; Jakuszko, K.; Bartoszek, D.; Krajewska, M.; Królak-Olejnik, B. Antibodies in the Breastmilk of COVID-19 Recovered Women. BMC Pregnancy Childbirth 2022, 22, 635. [Google Scholar] [CrossRef] [PubMed]
- Nir, O.; Schwartz, A.; Toussia-Cohen, S.; Leibovitch, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Lustig, Y.; et al. Maternal-Neonatal Transfer of SARS-CoV-2 Immunoglobulin G Antibodies among Parturient Women Treated with BNT162b2 Messenger RNA Vaccine during Pregnancy. Am. J. Obstet. Gynecol. MFM 2022, 4, 100492. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Belfort, M.B.; Pace, C.D.; Lackey, K.A.; Gogel, A.C.; Nguyen-Contant, P.; Kanagaiah, P.; Fitzgerald, T.; et al. COVID-19 and Human Milk: SARS-CoV-2, Antibodies, and Neutralizing Capacity. medRxiv Prepr. Serv. Health Sci. 2020, 12. [Google Scholar] [CrossRef]
- van Keulen, B.J.; Romijn, M.; Bondt, A.; Dingess, K.A.; Kontopodi, E.; van der Straten, K.; Den Boer, M.A.; Burger, J.A.; Poniman, M.; Bosch, B.J.; et al. Human Milk from Previously COVID-19-Infected Mothers: The Effect of Pasteurization on Specific Antibodies and Neutralization Capacity. Nutrients 2021, 13, 1645. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; Hakansson, A.P.; Hall, S.; Lavangnananda, S.; Fels, S.; Medo, E. Functional Antibodies against SARS-CoV-2 Receptor Binding Domain Variants with Mutations N501Y or E484K in Human Milk from COVID-19-Vaccinated, -Recovered, and -Unvaccinated Women. Breastfeed. Med. 2022, 17, 163–172. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; DaPra, C.; Fels, S.; Medo, E. Receptor-Binding Domain Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibodies in Human Milk from Mothers with Coronavirus Disease 2019 Polymerase Chain Reaction or with Symptoms Suggestive of Coronavirus Disease 2019. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 125–128. [Google Scholar] [CrossRef]
- Juncker, H.G.; Romijn, M.; Loth, V.N.; Ruhé, E.J.M.; Bakker, S.; Kleinendorst, S.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; et al. Antibodies against SARS-CoV-2 in Human Milk: Milk Conversion Rates in the Netherlands. J. Hum. Lact. 2021, 37, 469–476. [Google Scholar] [CrossRef]
- Pullen, K.M.; Atyeo, C.; Collier, A.R.Y.; Gray, K.J.; Belfort, M.B.; Lauffenburger, D.A.; Edlow, A.G.; Alter, G. Selective Functional Antibody Transfer into the Breastmilk after SARS-CoV-2 Infection. Cell Rep. 2021, 37, 109959. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Belfort, M.B.; Pace, C.D.W.; Lackey, K.A.; Gogel, A.C.; Nguyen-Contant, P.; Kanagaiah, P.; Fitzgerald, T.; et al. Characterization of SARS-CoV-2 RNA, Antibodies, and Neutralizing Capacity in Milk Produced by Women with COVID-19. MBio 2021, 12, e03192-20. [Google Scholar] [CrossRef] [PubMed]
- Demers-Mathieu, V.; Dapra, C.; Medo, E. Comparison of Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibodies’ Binding Capacity between Human Milk and Serum from Coronavirus Disease 2019-Recovered Women. Breastfeed. Med. 2021, 16, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; Seppo, A.E.; Diaz, N.; Rosen-Carole, C.; Nowak-Wegrzyn, A.; Cruz Vasquez, J.M.; Ferri-Huerta, R.; Nguyen-Contant, P.; Fitzgerald, T.; Sangster, M.Y.; et al. Association of Human Milk Antibody Induction, Persistence, and Neutralizing Capacity with SARS-CoV-2 Infection vs. MRNA Vaccination. JAMA Pediatr. 2021, 176, 159. [Google Scholar] [CrossRef] [PubMed]
- Juncker, H.G.; Romijn, M.; Loth, V.N.; Caniels, T.G.; de Groot, C.J.M.; Pajkrt, D.; van Gils, M.J.; van Goudoever, J.B.; van Keulen, B.J. Human Milk Antibodies against SARS-CoV-2: A Longitudinal Follow-up Study. J. Hum. Lact. 2021, 37, 485–491. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Meehan, C.L.; Martin, M.A.; Ley, S.H.; Barbosa-Leiker, C.; Andres, A.; Yeruva, L.; Belfort, M.B.; et al. Milk from Women Diagnosed with COVID-19 Does Not Contain SARS-CoV-2 RNA but Has Persistent Levels of SARS-CoV-2-Specific IgA Antibodies. Front. Immunol. 2021, 12, 801797. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; Dapra, C.; Mathijssen, G.; Sela, D.A.; Järvinen, K.M.; Seppo, A.; Fels, S.; Medo, E. Human Milk Antibodies against S1 and S2 Subunits from SARS-CoV-2, HCoV-OC43, and HCoV-229E in Mothers with a Confirmed COVID-19 PCR, Viral SYMPTOMS, and Unexposed Mothers. Int. J. Mol. Sci. 2021, 22, 1749. [Google Scholar] [CrossRef]
- Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; Bijl, T.P.L.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. Comparison of SARS-CoV-2-Specific Antibodies in Human Milk after MRNA-Based COVID-19 Vaccination and Infection. Vaccines 2021, 9, 1475. [Google Scholar] [CrossRef]
- Fox, A.; Marino, J.; Amanat, F.; Oguntuyo, K.Y.; Hahn-Holbrook, J.; Lee, B.; Zolla-Pazner, S.; Powell, R.L. The IgA in Milk Induced by SARS-CoV-2 Infection Is Comprised of Mainly Secretory Antibody That Is Neutralizing and Highly Durable over Time. PLoS ONE 2022, 17, e0249723. [Google Scholar] [CrossRef]
- Leung, H.Y.H.; Leung, B.W.; Gil, M.M.; Rolle, V.; Moungmaithong, S.; Wang, C.C.; Poon, L.C. SARS-CoV-2-specific Antibodies and Neutralization Capacity in Breast Milk Following Infection vs. Vaccination. Ultrasound Obstet. Gynecol. 2022, 60, 425. [Google Scholar] [CrossRef]
- Marshall, N.E.; Blanton, M.B.; Doratt, B.M.; Malherbe, D.C.; Rincon, M.; True, H.; Mcdonald, T.; Beauregard, C.; Adatorwovor, R.; Messaoudi, I. SARS-CoV-2 Vaccine Booster Elicits Robust Prolonged Maternal Antibody Responses and Passive Transfer via the Placenta and Breastmilk. bioRxiv 2022, 11, 518385. [Google Scholar] [CrossRef] [PubMed]
- Longueira, Y.; Ojeda, D.S.; Battistelli, R.B.A.; Sanchez, L.; Oviedo Rouco, S.; Albano, D.; Guevara, E.; Valls, V.; Pando, M.A.; Gamarnik, A.V. SARS-CoV-2-Specific IgG and IgA Response in Maternal Blood and Breastmilk of Vaccinated Naïve and Convalescent Lactating Participants. Front. Immunol. 2022, 13, 5514. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Young, B.E.; Li, D.; Seppo, A.E.; Zhou, Q.; Wiltse, A.; Nowak-Wegrzyn, A.; Murphy, K.; Widrick, K.; Diaz, N.; et al. Broad cross-Reactive IgA and IgG against Human Coronaviruses in Milk Induced by COVID-19 Vaccination and Infection. medRxiv Prepr. Serv. Health Sci. 2022, 10, 980. [Google Scholar] [CrossRef] [PubMed]
- Esteve-Palau, E.; Gonzalez-Cuevas, A.; Guerrero, M.E.; Garcia-Terol, C.; Alvarez, M.C.; Garcia, G.; Moreno, E.; Medina, F.; Casadevall, D.; Diaz-Brito, V. Quantification and Progress over Time of Specific Antibodies against Severe Acute Respiratory Syndrome Coronavirus 2 in Breast Milk of Lactating Women Vaccinated with BNT162b2 Pfizer-BioNTech Coronavirus Disease 2019 Vaccine (LacCOVID). Open Forum Infect. Dis. 2022, 9, ofac239. [Google Scholar] [CrossRef]
- Low, J.M.; Gu, Y.; Ng, M.S.F.; Wang, L.W.; Amin, Z.; Zhong, Y.; Macary, P.A. Human Milk Antibodies after BNT162b2 Vaccination Exhibit Reduced Binding against SARS-CoV-2 Variants of Concern. Vaccines 2022, 10, 225. [Google Scholar] [CrossRef]
- Narayanaswamy, V.; Pentecost, B.T.; Schoen, C.N.; Alfandari, D.; Schneider, S.S.; Baker, R.; Arcaro, K.F. Neutralizing Antibodies and Cytokines in Breast Milk after Coronavirus Disease 2019 (COVID-19) MRNA Vaccination. Obstet. Gynecol. 2022, 139, 181–191. [Google Scholar] [CrossRef]
- Bender, J.M.; Lee, Y.; Cheng, W.A.; Marentes Ruiz, C.J.; Pannaraj, P.S. Coronavirus Disease 2019 Vaccine Booster Effects Are Seen in Human Milk Antibody Response. Front. Nutr. 2022, 9, 898849. [Google Scholar] [CrossRef]
- Selma-Royo, M.; Bäuerl, C.; Mena-Tudela, D.; Aguilar-Camprubí, L.; Pérez-Cano, F.J.; Parra-Llorca, A.; Lerin, C.; Martínez-Costa, C.; Collado, M.C. Anti-SARS-CoV-2 IgA and IgG in Human Milk after Vaccination Is Dependent on Vaccine Type and Previous SARS-CoV-2 Exposure: A Longitudinal Study. Genome Med. 2022, 14, 42. [Google Scholar] [CrossRef]
- Pietrasanta, C.; Darwich, A.; Ronchi, A.; Crippa, B.; Spada, E.; Mosca, F.; Pugni, L.; Rescigno, M. Humoral Response to Anti-SARS-CoV-2 Vaccine in Breastfeeding Mothers and Mother-to-Infant Antibody Transfer through Breast Milk. NPJ Vaccines 2022, 7, 63. [Google Scholar] [CrossRef]
- Ricciardi, A.; Zelini, P.; Cassaniti, I.; Avanzini, M.A.; Colaneri, M.; De Silvestri, A.; Baldanti, F.; Bruno, R. Serum and Breastmilk SARS-CoV-2 Specific Antibodies Following BNT162b2 Vaccine: Prolonged Protection from SARS-CoV-2 in Newborns and Older Children. Int. J. Infect. Dis. 2022, 122, 905. [Google Scholar] [CrossRef]
- Pieri, M.; Maniori, M.A.; Shahabian, L.; Kanaan, E.; Paphiti-Demetriou, I.; Pipis, S.; Felekkis, K.; Nicolaidou, V.; Papaneophytou, C. Survival of Vaccine-Induced Human Milk SARS-CoV-2 IgG, IgA and SIgA Immunoglobulins across Simulated Human Infant Gastrointestinal Digestion. Nutrients 2022, 14, 3368. [Google Scholar] [CrossRef] [PubMed]
- Stafford, L.; Valcarce, V.; Henry, M.; Neu, J.; Parker, L.; Martina, M.; Vicuna, V.; Gowen, T.; Cato, E.; Kosik, I.; et al. Detection of SARS-CoV-2 IgA and IgG in Human Milk and Breastfeeding Infant Stool 6 Months after Maternal COVID-19 Vaccination. J. Perinatol. 2023, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Trofin, F.; Nastase, E.V.; Iancu, L.S.; Constantinescu, D.; Cianga, C.M.; Lunca, C.; Ursu, R.G.; Cianga, P.; Dorneanu, O.S. Anti-RBD IgA and IgG Response and Transmission in Breast Milk of Anti-SARS-CoV-2 Vaccinated Mothers. Pathogens 2022, 11, 286. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Fox, A.; Decarlo, C.; Norris, C.; Griffin, S.; Wedekind, S.; Flanagan, J.M.; Shenker, N.; Powell, R.L. Comparative Profiles of SARS-CoV-2 Spike-Specific Human Milk Antibodies Elicited by MRNA-and Adenovirus-Based COVID-19 Vaccines. In Breastfeeding Medicine; Mary Ann Liebert, Inc.: New York, NY, USA, 2022; Volume 17, pp. 638–646. [Google Scholar] [CrossRef]
- Guida, M.; Terracciano, D.; Cennamo, M.; Aiello, F.; La Civita, E.; Esposito, G.; Gargiulo, V.; Maruotti, G.M.; Portella, G.; Sarno, L. COVID-19 Vaccine MRNABNT162b2 Elicits Human Antibody Response in Milk of Breastfeeding Women. Vaccines 2021, 9, 785. [Google Scholar] [CrossRef] [PubMed]
- Valcarce, V.; Stafford, L.S.; Neu, J.; Cacho, N.; Parker, L.; Mueller, M.; Burchfield, D.J.; Li, N.; Larkin, J. Detection of SARS-CoV-2-Specific IgA in the Human Milk of COVID-19 Vaccinated Lactating Health Care Workers. Breastfeed. Med. 2021, 16, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Lechosa-Muñiz, C.; Paz-Zulueta, M.; Mendez-Legaza, J.M.; Irure-Ventura, J.; González, R.C.; Montes, J.C.; López-Hoyos, M.; Llorca, J.; Cabero-Pérez, M.J. Induction of SARS-CoV-2-Specific IgG and IgA in Serum and Milk with Different SARS-CoV-2 Vaccines in Breastfeeding Women: A cross-Sectional Study in Northern Spain. Int. J. Environ. Res. Public Health 2021, 18, 8831. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.E.; Luna Centeno, L.D.; Cheng, W.A.; Marentes Ruiz, C.J.; Lee, Y.; Congrave-Wilson, Z.; Powell, R.L.; Stellwagen, L.; Pannaraj, P.S. Human Milk SARS-CoV-2 Antibodies up to 6 Months after Vaccination. Pediatrics 2022, 149, e2021054260. [Google Scholar] [CrossRef]
- Golan, Y.; Prahl, M.; Cassidy, A.G.; Gay, C.; Wu, A.H.B.; Jigmeddagva, U.; Lin, C.Y.; Gonzalez, V.J.; Basilio, E.; Warrier, L.; et al. COVID-19 MRNA Vaccination in Lactation: Assessment of Adverse Events and Vaccine Related Antibodies in Mother-Infant Dyads. Front. Immunol. 2021, 12, 4596. [Google Scholar] [CrossRef] [PubMed]
- Jakuszko, K.; Kościelska-Kasprzak, K.; Żabińska, M.; Bartoszek, D.; Poznański, P.; Rukasz, D.; Kłak, R.; Królak-Olejnik, B.; Krajewska, M. Immune Response to Vaccination against COVID-19 in Breastfeeding Health Workers. Vaccines 2021, 9, 663. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2-Specific Antibodies in Breast Milk after COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef]
- Low, J.M.; Gu, Y.; Ng, M.S.F.; Amin, Z.; Lee, L.Y.; Ng, Y.P.M.; Shunmuganathan, B.D.; Niu, Y.; Gupta, R.; Tambyah, P.A.; et al. Codominant IgG and IgA Expression with Minimal Vaccine MRNA in Milk of BNT162b2 Vaccinees. NPJ Vaccines 2021, 6, 105. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. COVID-19 Vaccine Response in Pregnant and Lactating Women: A Cohort Study. medRxiv 2021, preprint. [Google Scholar] [CrossRef]
- Baird, J.K.; Jensen, S.M.; Urba, W.J.; Fox, B.A.; Baird, J.R. SARS-CoV-2 Antibodies Detected in Mother’s Milk Post-Vaccination. J. Hum. Lact. 2021, 37, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, D.S.R.; Perez, M.M.L.; Perez, M.C.; Hernandez, M.I.S.; Pulido, S.M.; Villacampa, L.P.; Vilar, A.M.F.; Falero, M.R.; Carretero, P.G.; Millan, B.R.; et al. SARS-CoV-2 Antibodies in Breast Milk after Vaccination. Pediatrics 2021, 148, e2021052286. [Google Scholar] [CrossRef]
- Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. The Levels of SARS-CoV-2 Specific Antibodies in Human Milk Following Vaccination. J. Hum. Lact. 2021, 37, 477–484. [Google Scholar] [CrossRef]
- Rosenberg-Friedman, M.; Kigel, A.; Bahar, Y.; Werbner, M.; Alter, J.; Yogev, Y.; Dror, Y.; Lubetzky, R.; Dessau, M.; Gal-Tanamy, M.; et al. BNT162b2 MRNA Vaccine Elicited Antibody Response in Blood and Milk of Breastfeeding Women. Nat. Commun. 2021, 12, 6222. [Google Scholar] [CrossRef]
- Scrimin, F.; Campisciano, G.; Comar, M.; Ragazzon, C.; Davanzo, R.; Quadrifoglio, M.; Giangreco, M.; Stabile, G.; Ricci, G. IgG and IgA Antibodies Post SARS-CoV-2 Vaccine in the Breast Milk and Sera of Breastfeeding Women. Vaccines 2022, 10, 125. [Google Scholar] [CrossRef]
- Charepe, N.; Gonçalves, J.; Juliano, A.M.; Lopes, D.G.; Canhão, H.; Soares, H.; Serrano, E.F. COVID-19 MRNA Vaccine and Antibody Response in Lactating Women: A Prospective Cohort Study. BMC Pregnancy Childbirth 2021, 21, 632. [Google Scholar] [CrossRef]
- Gonçalves, J.; Juliano, A.M.; Charepe, N.; Alenquer, M.; Athayde, D.; Ferreira, F.; Archer, M.; Amorim, M.J.; Serrano, F.; Soares, H. Secretory IgA and T Cells Targeting SARS-CoV-2 Spike Protein Are Transferred to the Breastmilk upon MRNA Vaccination. Cell Rep. Med. 2021, 2, 100468. [Google Scholar] [CrossRef]
- Esteve-Palau, E.; Gonzalez-Cuevas, A.; Guerrero, M.E.; Garcia-Terol, C.; Alvarez, M.C.; Casadevall, D.; Diaz-Brito, V. Quantification of Specific Antibodies against SARS-CoV-2 in Breast Milk of Lactating Women Vaccinated with an MRNA Vaccine. JAMA Netw. Open 2021, 4, e2120575. [Google Scholar] [CrossRef]
- Yeo, K.T.; Chia, W.N.; Tan, C.W.; Ong, C.; Yeo, J.G.; Zhang, J.; Poh, S.L.; Lim, A.J.M.; Sim, K.H.Z.; Sutamam, N.; et al. Neutralizing Activity and SARS-CoV-2 Vaccine MRNA Persistence in Serum and Breastmilk after BNT162b2 Vaccination in Lactating Women. Front. Immunol. 2022, 12, 5793. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.; Nir, O.; Toussia-Cohen, S.; Leibovich, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Levin, E.G.; et al. Presence of SARS-CoV-2 Antibodies in Lactating Women and Their Infants Following BNT162b2 Messenger RNA Vaccine. Am. J. Obstet. Gynecol. 2021, 225, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.C.; Carter, E.B.; Raghuraman, N.; Nolan, L.S.; Gong, Q.; Lewis, A.N.; Good, M. Anti–Severe Acute Respiratory Syndrome Coronavirus 2 Antibodies Induced in Breast Milk after Pfizer-BioNTech/BNT162b2 Vaccination. Am. J. Obstet. Gynecol. 2021, 225, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Scaggs Huang, F. Are SARS-CoV-2 Antibodies Detectable in Human Milk after Vaccination against COVID-19? J. Pediatric Infect. Dis. Soc. 2022, 11, 126. [Google Scholar] [CrossRef]
- Agostinis, C.; Toffoli, M.; Balduit, A.; Mangogna, A.; Yasmin, H.; Ragazzon, C.; Pegoraro, S.; Campisciano, G.; Stabile, G.; Zito, G.; et al. Anti-Spike Antibodies Present in the Milk of SARS-CoV-2 Vaccinated Mothers Are Complement-Activating. Int. J. Mol. Sci. 2023, 24, 4395. [Google Scholar] [CrossRef]
- Gu, Y.; Low, J.M.; Tan, J.S.Y.; Ng, M.S.F.; Ng, L.F.P.; Shunmuganathan, B.; Gupta, R.; MacAry, P.A.; Amin, Z.; Lee, L.Y.; et al. Immune and Pathophysiologic Profiling of Antenatal Coronavirus Disease 2019 in the GIFT Cohort: A Singaporean Case-Control Study. Front. Pediatr. 2022, 10, 949756. [Google Scholar] [CrossRef]
- Martin-Vicente, M.; Carrasco, I.; Muñoz-Gomez, M.J.; Lobo, A.H.; Mas, V.; Vigil-Vázquez, S.; Vázquez, M.; Manzanares, A.; Cano, O.; Alonso, R.; et al. Antibody Levels to SARS-CoV-2 Spike Protein in Mothers and Children from Delivery to Six Months Later. Birth 2022. [Google Scholar] [CrossRef]
- Dutra, L.V.; Silva, M.H.; Lebrão, C.W.; Affonso-Fonseca, F.L.; Suano-Souza, F.I. Impact of the Presence Anti-SARS-CoV-2 IgA in the Colostrum of Women Infected by COVID-19 During the Pregnancy in Neonatal Clinical Outcomes: A cross-Sectional Study. Matern. Child Health J. 2023, 27, 737. [Google Scholar] [CrossRef]
- Wachman, E.M.; Snyder-Cappione, J.; Devera, J.; Boateng, J.; Dhole, Y.; Clarke, K.; Yuen, R.R.; Parker, S.E.; Hunnewell, J.; Ferraro, R.; et al. Maternal, Infant, and Breast Milk Antibody Response Following COVID-19 Infection in Early versus Late Gestation. Pediatr. Infect. Dis. J. 2023, 42, e70–e76. [Google Scholar] [CrossRef]
- Calabretto, M.; D’Alisa, R.; Faraone, S.; Mazzuti, L.; Pecorini, F.; Turriziani, O. Detection of SARS-CoV-2 RNA and Antibodies in Breast Milk of Infected Mothers. J. Med. Virol. 2023, 95, e28142. [Google Scholar] [CrossRef]
- Narayanaswamy, V.; Pentecost, B.T.; Telfer, J.C.; Burnside, A.S.; Schneider, S.S.; Alfandari, D.; Baker, R.L.; Saiju, A.; Nodiff, S.; Arcaro, K.F. Durable Antibody and Effector Memory T Cell Responses in Breastmilk from Women with SARS-CoV-2. Front. Immunol. 2022, 13, 985226. [Google Scholar] [CrossRef] [PubMed]
- Bode, L.; Bertrand, K.; Najera, J.A.; Furst, A.; Honerkamp-Smith, G.; Shandling, A.D.; Chambers, C.D.; Camerini, D.; Campo, J.J. Characterization of SARS-CoV-2 Antibodies in Human Milk from 21 Women with Confirmed COVID-19 Infection. Pediatr. Res. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lechosa-Muñiz, C.; Paz-Zulueta, M.; Irure-Ventura, J.; Mendez-Legaza, J.M.; Cuesta González, R.; Gómez-Acebo, I.; López-Hoyos, M.; Llorca, J.; Cabero-Pérez, M.J. Development of SARS-CoV-2 Specific IgG and IgA Antibodies in Serum and Milk with Different SARS-CoV-2 Vaccines in Lactating Women. Int. Breastfeed. J. 2023, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Demers-Mathieu, V.; Huston, R.K.; Markell, A.M.; McCulley, E.A.; Martin, R.L.; Dallas, D.C. Antenatal Influenza A-Specific IgA, IgM, and IgG Antibodies in Mother’s Own Breast Milk and Donor Breast Milk, and Gastric Contents and Stools from Preterm Infants. Nutrients 2019, 11, 1567. [Google Scholar] [CrossRef] [Green Version]
- Demers-Mathieu, V.; Underwood, M.A.; Beverly, R.L.; Dallas, D.C. Survival of Immunoglobulins from Human Milk to Preterm Infant Gastric Samples at 1, 2, and 3 Hours Postprandial. Neonatology 2018, 114, 242. [Google Scholar] [CrossRef]
- Thai, J.D.; Gregory, K.E. Bioactive Factors in Human Breast Milk Attenuate Intestinal Inflammation during Early Life. Nutrients 2020, 12, 581. [Google Scholar] [CrossRef] [Green Version]
- Hurley, W.L.; Theil, P.K. Perspectives on Immunoglobulins in Colostrum and Milk. Nutrients 2011, 3, 442–474. [Google Scholar] [CrossRef] [Green Version]
- Goldman, A.S.; Chheda, S.; Keeney, S.E.; Schmalstieg, F.C. Immunology of Human Milk and Host Immunity. Fetal Neonatal Physiol. 2020, 2011, 1690–1701. [Google Scholar] [CrossRef]
- Yaugel-Novoa, M.; Bourlet, T.; Paul, S. Role of the Humoral Immune Response during COVID-19: Guilty or Not Guilty? Mucosal Immunol. 2022, 15, 1170–1180. [Google Scholar] [CrossRef]
- Michaud, E.; Mastrandrea, C.; Rochereau, N.; Paul, S. Human Secretory IgM: An Elusive Player in Mucosal Immunity. Trends Immunol. 2020, 41, 141–156. [Google Scholar] [CrossRef]
- Van de Perre, P.; Simonon, A.; Karita, E.; Butera, J.B.; Hitimana, D.G.; Mukamabano, B.; Van Goethem, C.; Lepage, P.; Dabis, F.; Msellati, P. Infective and Anti-Infective Properties of Breastmilk from HIV-1-Infected Women. Lancet 1993, 341, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG Subclasses and Allotypes: From Structure to Effector Functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales-Núñez, J.J.; Muñoz-Valle, J.F.; Torres-Hernández, P.C.; Hernández-Bello, J. Overview of Neutralizing Antibodies and Their Potential in COVID-19. Vaccines 2021, 9, 1376. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year, Country) | Duration of Study | Pregnant Women (N) | Diagnostic Test | Time of Sample HM Collection | Studied Immunoglobulins | Antibody Measurement Method | Outcome/Results |
|---|---|---|---|---|---|---|---|
| Gao X. et al. (2020, China) [18] | 20 days | 12 | PCR or serology test | Within 7 days postpartum | Anti-SARS-CoV-2 antibodies (IgM and IgG) | CLIA commercial kit/NAL | Neutralizing antibodies present in 3 samples of HM. SARS-CoV-2 virus was not detected in any sample. |
| Narayanaswamy V. et al. (2021, USA) [15] | 5 months | 15 | PCR test | Within 48 hours postpartum | Anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA | Present antibodies in colostrum (IgA in 73%, IgG in 73% and IgM in 33% of the samples). |
| Larcade R. et al. (2022, Argentina) [16] | 2.5 months | 58 | PCR test | Within 96 h postpartum | Anti-RBD antibodies (IgA) | Homemade ELISA | Antibodies present in the HM of 87% of participants. No significant correlation with time of infection. Positive correlation between serum IgG titers and IgA titers in HM. |
| Bobik T.V. et al. (2021, Switzerland) [19] | NA | 41 | PCR test | Postpartum | Anti-S and anti-N antibodies (sIgA) | Homemade ELISA | Anti-RBD antibodies detected even in the HM of women infected during the first trimester. |
| Peng S. et al. (2020, China) [20] | NA | 19 | PCR test | Days 3,7,14,21, 28,42,56,70 postpartum | Anti-SARS-CoV-2 antibodies (IgM and IgG) | ELISA commercial kit | IgM present in the HM of 47% of participants. IgG was not detected in any sample. SARS-CoV-2 virus was not detected in any sample. |
| Bäuerl C. et al. (2021, Spain) [21] | 8 months | 60 | PCR or serology test | Postpartum | Anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA | Antibodies present in about 85% of samples. IgA titers remained stable in high titers over time. IgG titers were rising over time. Positive correlation between total IgA titers and anti-RBD IgA titers in HM. |
| Collier-ARY. et al. (2021, USA) [22] | 1 year | 22 | PCR test | Postpartum | Anti-RBD antibodies (IgA and IgG) | Homemade ELISA | Antibodies present in HM. |
| Conti MG. et al. (2021, Italy) [23] | 6 months | 28 | PCR test | 2 days and 2 months postpartum | Anti-S antibodies (IgA and IgG) | ELISA commercial kit | IgA present in all samples. Higher titers in 48 h compared to 2 months post delivery. IgG titers remain low and stable over time. |
| Luo QQ. et al. (2021, China) [24] | 43 days | 4 | PCR test | 1 week postpartum | Anti-SARS-CoV-2 antibodies (IgM and IgG) | Homemade ELISA | IgM present in all samples of confirmed disease. Positive correlation between IgM titers in HM and in serum. IgG was not detected in any sample. SARS-CoV-2 virus was not detected in any sample. |
| Conti, M. G. et al. (2022, USA) [25] | 2 months | 28 | PCR test | 5 days and 2 months after infection | Anti-S antibodies (IgA and IgG) | ELISA commercial kit | IgA present in higher titers than IgG in HM. No correlation between IgA titers in HM and in serum. |
| Decenti, E. C. et al. (2022, Italy) [26] | 16 months | 141 | PCR test | Postpartum | Anti-SARS-CoV-2 antibodies (IgM and IgG) | CLIA, ELISA, ECLIA, CMIA commercial kits | IgG present in 3.0% and IgM in 7.5% of HM. |
| Gu, Y. et al. (2022, Singapore) [81]. | NA | 8 | PCR test | 1–3 months postpartum | Anti-S and anti-RBD antibodies (IgA and IgG) | Homemade ELISA | Antibodies present in minimal levels 0–3 months postpartum. |
| Leung, H. Y. H. et al. (2022, China) [44] | NA | 18 | Laboratory-confirmed | 3–192 days post infection (median = 45 days) | Anti-RBD antibodies (IgA) | Homemade ELISA/BA-Nabs |
Antibody titers wane over time.
Neutralizing antibodies present in HM. Positive correlation between antibody titers and binding capacity. |
| Martin-Vicente, M. et al. (2022, Spain) [82] | NA | 46 | PCR or serology test | Postpartum | Anti-S antibodies (IgA, IgM and IgG) | Homemade ELISA/NAA | Antibodies’ titers correlate positively with neutralizing capacity. IgA detected in higher titers than IgM and IgG. |
| Olearo, F. et al. (2022, Germany) [27] | 6 months | 9 | PCR test | Monthly for 6 months postpartum | Anti-S antibodies (IgA) and anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA/NAA | Presence of neutralizing antibodies in HM. |
| Szczygioł, P. et al. (2022, Poland) [28] | 2.5 months | 72 | PCR test | 1–229 days after infection (median 68) | Anti-RBD antibodies (IgA and IgG) | ELISA commercial kit | No correlation between antibody titers and severity of disease or time of infection. |
| Nir O. et al. (2022, Israel) [29] | 2 months | 11 | PCR test | Postpartum | Anti-RBD antibodies (IgG) | Homemade ELISA | Positive correlation between IgG titers in HM and serum. |
| Fox, A. et al. (2022, USA) [43] | 10 months | 74 | PCR test | 4–6 weeks after infection and 4–10 months after infection | Anti-S antibodies (IgA and IgG) | Homemade ELISA/PNA | Detectable IgA in 89% of samples 4–6 weeks after infection. Detectable IgG in 75% of samples 4–6 weeks after infection. Detectable IgA even 4–10 months after infection. Increased neutralizing capacity of HM after infection. |
| Dutra LV. et al. (2023, Brazil) [83] | 1 year | 165 | PCR test | 1–2 days postpartum | Anti-S antibodies (IgA and IgG) | ELISA commercial kit | Detectable IgA in about 70% of participants. Negative correlation between IgA titers in colostrum and neonatal symptoms. |
| Wachman EM. et al. (2023, USA) [84] | 1 year | 31 | PCR test | At delivery and 6 weeks postpartum | Anti-RBD and anti-N antibodies (IgA, IgM and IgG) | Homemade ELISA | Higher titers of anti-RBD IgA in the HM of women infected during first or second trimester. Positive correlation between IgG titer in maternal HM and serum. |
| Clabretto M. et al. (2023, Italy) [85] | 8 months | 12 | PCR test | Postpartum | Anti-N antibodies (IgA) and anti-S antibodies (IgM and IgG) | CLIA and ELISA commercial kits | Presence of IgA in 66% of samples. Presence of IgM and IgG in no sample. |
| Author (Year, Country) | Duration of Study | Lactating Women (N) | Diagnostic Test | Time of Sample HM Collection | Studied Immunoglobulins | Antibody Measurement Method | Outcome/Results |
|---|---|---|---|---|---|---|---|
| Pace R.M. et al. (2020, Moscow) [30] | NA | 18 | PCR test | 12.0 ± 8.9 days after infection | Anti-SARS-CoV-2 antibodies (IgA and IgG) | Homemade ELISA/MNA | Antibodies present in HM samples. Positive correlation between anti-RBD antibodies’ titers and neutralizing capacity. SARS-CoV-2 virus was not detected in any sample. |
| van Keulen, BJ. (2021, Switzerland) [31] | ΝA | 19 | PCR test | 5.9 (SD = 2.6) weeks after infection | Anti-S antibodies (IgA and IgG), anti-RDB and anti-N antibodies (IgA, IgM, IgG) | Homemade ELISA/PNA | Antibodies present in the HM of 83% of participants. No correlation between antibody titers and neutralizing capacity. |
| Demers-Mathieu V. (2021, USA) [32] | NA | 10 | PCR test | 63 ± 40 days after infection | Anti-RBD antibodies (sIgA/IgA, sIgM/IgM and IgG) | Homemade ELISA/PNA | Antibodies present in HM. Higher inhibiting capacity against binding RBD to its receptor in women with previous COVID-19 infection compared to controls. |
| Demers-Mathieu V. et al. (2021, USA) [33] | NA | 8 | PCR test | 2 months after infection | Anti-RBD antibodies (sIgA/IgA, sIgM/IgM and IgG) | Homemade ELISA | Antibodies present in HM. |
| Junker H.G. et al. (2021, the Netherlands) [34] | 3.5 months | 165 | PCR test | 8 weeks (mean time) after infection | Anti-SARS-CoV-2 antibodies (IgA) | Homemade ELISA | Detectable antibodies in HM even 10 months after infection. |
| Pullen K.M. (2021, USA) [35] | NA | 20 | PCR test | 66 days (mean time) after infection | Anti-SARS-CoV-2 antibodies (IgA, IgM and IgG) | Systems serology | Antibodies present in HM. IgG detected in significantly lower titers. IgG functionally attenuated. Positive correlation between IgG titers in HM and serum. No correlation between IgA titers in HM and serum. |
| Pace, R.M. et al. (2021, USA) [36] | NA | 18 | PCR test | 12 ± 8,9 days after infection | Anti-RBD, anti-S2, anti-N (IgA and IgG) | Homemade ELISA/MNA | IgA present in 76% of samples and IgG in 80% of samples. Total of 62% of samples had neutralization capacity. SARS-CoV-2 virus was not detected in any sample. |
| Demers-Mathieu V. et al. (2021, USA) [37] | NA | 7 | PCR test | 3 ± 2 months after infection | Anti-RBD antibodies (sIgA/IgA, sIgM/IgM and IgG) | Homemade ELISA | Positive correlation between sIgA/IgA titers and time from infection. No correlation detected between antibody titers and maternal age, infant gender and severity of symptoms. |
| Young BE. et al. (2021, USA) [38] | 5 months | 47 | PCR test | 0, 3, 7, 10, 28 and 90 days after infection | Anti-RBD antibodies (IgA and IgG) | Homemade ELISA/MNA | IgA-dominant response. Detectable IgA in almost-stable titers even 3 months after infection. Increased neutralizing capacity of HM after infection. SARS-CoV-2 virus was not detected in any sample. |
| Juncker HG. et al. (2021, the Netherlands) [39] | 3 months | 29 | PCR test | 1,2,3,4 and 5 months after infection | Anti-S antibodies (IgA) | Homemade ELISA | Antibodies present even 5 months after infection. Not significant decrease in antibody titers over time. |
| Pace RM. et al. (2021, the Netherlands) [40] | 8 months | 64 | PCR test | 1,2,3,4 and 8 weeks after infection | Anti-RBD antibodies (IgA) | Homemade ELISA | Maximum IgA concentration was higher in symptomatic women. SARS-CoV-2 virus was not detected in any sample. |
| Demers-Mathieu V. et al. (2021, USA) [41] | NA | 7 | PCR test | 47 +/− 24 days after infection | Anti-S1 or S2 subunit antibodies (sIgA/IgA, sIgM/IgM and IgG) | ELISA | Present anti-S2 IgA antibodies. |
| Juncker HG. et al. (2021, Switzerland) [42] | 70 days | 18 | PCR test | Every 2 weeks after infection for at least 70 days | Anti-SARS-CON-2 antibodies (IgA) | Homemade ELISA | Detectable IgA antibodies even 70 days after infection. |
| Longueira, Y. et al. (2022, Argentina) [46] | 12 months | 11 | PCR test | After infection | Anti-S antibodies (IgA and IgG) | ELISA commercial kit | Antibodies present in HM. |
| Narayanaswamy, V. et al. (2022, USA) [86] | 4 months | 30 | PCR test | Every 3 days (for the 1st month after infection) and 4 months after infection | Anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA/NAA | Detectable neutralizing antibodies. Detectable IgA and IgG in the majority of participants even 4 months after infection. |
| Wang, J. et al. (2022, USA) [47] | 28 days | 45 | PCR test | 0, 3, 10, 19 and 28 days after enrolled day (within 14 days from infection) | Anti-S and anti-N antibodies (IgA and IgG) | LUMINEX assay | Antibodies present in HM. Positive correlation between IgG titers in HM and serum. No correlation between IgA titers in HM and serum. |
| L. Bode. et al. (2022, USA) [87] | 7 months | 21 | PCR test | Around infection | Anti-S, anti-RBD, anti-NTD and anti-N antibodies (IgA and IgG) | ECLIA | IgA was mainly against N protein and less against S protein. No difference was observed in IgG isotype. Heterogeneity in responses between participants. |
| Author (Year, Country) | Duration of Study | Pregnant Women (N) | Vaccine Type | Time of Sample HM collection | Studied immunoglobulins | Antibody Measurement Method | Outcome/Results |
|---|---|---|---|---|---|---|---|
| Conti, M. G. et al. (2022, USA) [25] | NA | 11 | BNT162b2 2 doses | 2 months after 2nd dose | Anti-S antibodies (IgA and IgG) | ELISA commercial kit | Higher IgG titers in vaccinated women compared to those who were infected. Positive correlation between IgG titers in HM and serum. |
| Leung, H. Y. H. et al. (2022, China) [44] | NA | 8 | COVID-19 vaccination | 0–334 days post 1st dose (median = 71 days) | Anti-RBD antibodies (IgA) | ELISA commercial kit/BA-Nabs |
Neutralizing antibodies present in HM.
Antibody titers wane over time. Higher binding capacity after infection than vaccination. Positive correlation between antibody titers and binding capacity. |
| Olearo, F. et al. (2022, Germany) [27] | 6 months | 5 | BNT162b2 2 doses | Monthly for 6 months postpartum | Anti-S antibodies (IgA) Anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA | Higher titers of antibodies compared to recovered women. |
| Nir O. et al. (2022, Israel) [29] | 2 months | 64 | BNT162b2 2 doses | Postpartum, within a few days | Anti-RBD antibodies (IgG) | Homemade ELISA |
Positive correlation between IgG titers in HM and serum.
|
| Collier-ARY. et al. (2021, USA) [22] | 4 months | 30 | mRNA-1273/BNT162b2 2 doses | Close after each dose and 2–8 weeks after 2nd dose | Anti-RBD antibodies (IgA and IgG) | Homemade ELISA | Neutralizing antibodies present in HM. |
| Marshall N.E. et al. (2022, USA) [45] | NA | 78 | mRNA-1273/BNT162b2 2 doses | Between 0–12 months postpartum | Anti-RBD antibodies (IgG) | Homemade ELISA | Half life of IgG in HM is about 2 months. Positive correlation between IgG titers in HM and serum. IgG1 and IgG3 are present in higher titers compared to IgG4. |
| Author (Year, Country) | Duration of Study | Lactating Women (N) | Vaccine Type | Time of Sample HM Collection | Studied Immunoglobulins | Antibody Measurement Method | Outcome/Results |
|---|---|---|---|---|---|---|---|
| Demers-Mathieu V. (2021, USA) [32] | NA | 19 | mRNA-1273/BNT162b2 2 doses | 37 ± 20 days after vaccination | Anti-RBD antibodies (sIgA/IgA, sIgM/IgM and IgG) | Homemade ELISA/PNA | Antibodies present in HM. Higher IgG titers in vaccinated compared to infected women. Higher neutralizing capacity in vaccinated women compared to controls. |
| Young BE. et al. (2021, USA) [38] | 5 months | 30 | mRNA-1273/BNT162b2 2 doses | Prevaccination, 18 days after 1st dose, 18 and 90 days after 2nd dose | Anti-RBD antibodies (IgA and IgG) | Homemade ELISA/MNT | IgG-dominant response. Increased IgG titers after each dose. Declined IgG titers by 3 months. Increased IgA titers only after the first dose. Increased neutralization capacity after vaccination. |
| Juncker HG. et al. (2021, Switzerland) [42] | 70 days | 26 | BNT162b2 2 doses | Prevaccination 3, 5, 7, 9, 11, 13, 15–17 days after 1st dose and 2nd dose and 70 days after 1st dose | Anti-S antibodies (IgA) | Homemade ELISA | Biphasic response of IgA antibodies. Detectable antibodies in 96% of participants after 2 doses. Detectable antibodies in about 40% of participants 70 days post vaccination. No significant difference between IgA titers in the HM of lactating women either infected or vaccinated. No severe adverse effect after vaccination. |
| Conti, M. G. et al. (2022, USA) [25] | NA | 12 | BNT162b2 2 doses | 10 days after 2nd dose | Anti-S antibodies (IgA and IgG) | ELISA commercial kit | Higher IgG titers in vaccinated women compared to the infected group. Positive correlation between IgG titers in HM and serum. |
| Esteve-Palau, E. et al. (2022, Spain) [48] | 6 months | 33 | BNT162b2 2 doses | 2 weeks after 1st dose and 2,4,12 and 24 weeks after 2nd dose | Anti-S1 and anti-N antibodies (IgG) | Serology test, commercial kit | Peak anti-S1-IgG titers 2 weeks after 2nd dose. Positive correlation between IgG titers in HM and serum. IgG titers wane over a 6 month period. |
| Longueira, Y. et al. (2022, Argentina) [46] | 12 months | 27 | Sputnik V, ChAdOx1-S or BBIBP-CorV | 21 and 65 days after first and 21, 65 and 120 days after second dose (mean time) | Anti-SARS-CoV-2 antibodies (IgA and IgG) | ELISA commercial kit | 2.8-fold increase in IgG titer after the 2nd dose. IgA remained constant between 1st and 2nd dose. 1.6-fold decrease in IgG titers, but stable levels of IgA over a 3-month period. Higher titer of IgG in participants who received adenoviral-based vaccines compared to those who received inactivated SARS-CoV-2 Sinopharm. No difference in IgA titers. |
| Low, J. M. et al. (2022, Singapore) [49] | 6 weeks | 46 | BNT162b2 2 doses | Prevaccination 3–7 days and 4–6 weeks after 2nd dose | Anti-RBD antibodies (IgA) | Homemade ELISA | Peak titers of IgA observed 3–5 days after 2nd dose. Total of 30% reduction in binding capacity of antibodies in Beta, Gamma and Delta variants compared to Wuhan-Hu-1 strain. |
| Narayanaswamy, V. et al. (2022, USA) [50] | NA | 27 | mRNA-1273/BNT162b2 2 doses | Prevaccination after 1st and 2nd dose | Anti-RBD antibodies (IgA IgM and IgG) | ELISA commercial kit/V-PLEX commercial kit | IgG-dominant immune response. No increase in IgA titers after 2nd dose. No correlation between lactation stage and antibody titers. |
| Bender, J. M. et al. (2022, USA) [51] | 10 months | 10 | mRNA-1273/BNT162b2 2 doses | Prevaccination 1, 3, 6 months after 1st dose | Anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA/sVNT | Peak antibody titers one month after the 1st dose. No significant increase in IgM titers. Positive correlation between IgG titers in serum, and IgG and IgA titers in HM. Increased neutralizing capacity after vaccination. |
| Collier-ARY et al. (2021, USA) [22] | 4 months | 16 | mRNA-1273/BNT162b2 2 doses | Close to each dose and 2–8 weeks after 2nd dose | Anti-RBD antibodies (IgA and IgG) | Homemade ELISA] | Neutralizing antibodies present in HM. |
| Pieri, M. et al. (2022, Switzerland) [55] | 7 months | 43 | mRNA-1273/BNT162b2 ChAdOx1-S 2 doses | Prevaccination 1 day before the 2nd dose, 3 weeks after the 2nd | Anti-SARS-CoV-2 antibodies (sIgA/IgA and IgG) | ELISA commercial kit | Higher titers of IgG and IgA after the 2nd dose. Stable high antibody titers 3 weeks after the 2nd dose. |
| Pietrasanta, C. et al. (2022, Italy) [53] | 90 days | 24 | BNT162b2 2 doses | Prevaccination before 2nd dose and 30, 60 and 90 days after 2nd dose | Anti-S and anti-RBD antibodies (IgA, IgA1, IgA2 and IgG) | Homemade ELISA | Vaccination induced IgG and IgA (mainly IgA1) immune responses. Antibodies waned over time, but they were still in detectable titers 90 days after vaccination. No severe adverse effect after vaccination. |
| Ricciardi, A. et al. (2022, Italy) [54] | 2,5 months | 18 | BNT162b2 2 doses | Prevaccination at the 2nd dose, 3 weeks after 2nd dose and 6 months after 1st dose | Anti-S antibodies (sIgA and sIgG) | ELISA commercial kit | Increased sIgA titers after the 1st dose. Peak sIgA titers 3 weeks after the 2nd dose. Significant decrease in sIgA titers 6 months post vaccination. Peak sIgG titers 6 months after the first dose. |
| Agostinis C. et al. (2023, Italy) [80] | 6 months | 22 | BNT162b2/ ChAdOx1-S 2 doses | Post vaccination (max 75 days post vaccination) | Anti-S antibodies (IgA and IgG) | Homemade ELISA | Range of antibody titers among participants. Positive correlation between IgG titers in serum and HM. No correlation between time of sample collection and antibody titers. Presence of IgG antibodies that can activate the complement. |
| Selma-Royo, M. et al. (2022, Spain) [52] | ΝA | 75 | mRNA-1273/BNT162b2/ ChAdOx1-S 2 doses | Prevaccination 1,2,3–4 weeks after 1st and 2nd dose In ChAdOx1-S group, a sample collected before 2nd dose | Anti-RBD antibodies (IgA and IgG) | Homemade ELISA | Peaked IgG titers 2 weeks after 2nd dose. Peaked IgA titers 1 week after the 1st dose for mRNA vaccines. IgA titers did not increase further after the 2nd dose. Higher IgG and IgA titers after vaccination with mRNA vaccines compared to those vaccinated with adeno-vectored vaccine. No significant difference observed between 2 mRNA vaccines. |
| Guida M. et al. (2021, Italy) [59] | NA | 10 | BNT162b2 2 doses | 20 days after 1st dose and 7 days after 2nd dose | Anti-S antibodies (total) | ECLIA commercial kit | Higher antibody titers after 2nd dose. No correlation between total anti-S antibodies in HM and serum. |
| Stafford, L. et al. (2022, USA) [56] | 12 months | 8 | mRNA-1273/BNT162b2 2 doses Ad.26.COV2.S 1 dose | Prevaccination 15–30 after 1st dose (for mRNA-based vaccines) and 7–30 days, 60–75 days, 90–105 days and 6 months after last dose | Anti-SARS-CoV-2 antibodies (IgA and IgG) | ELISA commercial kit/PVA | Antibody titers wane over time. Detectable levels 6 months post vaccination. More significant decline in IgG titers compared to IgA titers. Positive correlation between IgG levels in serum and HM 6 months post vaccination. Increased neutralizing capacity of HM after vaccination, especially 6 months post vaccination. |
| Valcare V. et al. (2021, USA) [60] | 4 months | 22 | mRNA-1273/BNT162b2 2 doses | Prevaccination, post 1st and 2nd dose | Anti-S antibodies (IgA and IgG) | ELISA | Detectable antibodies in HM after vaccination. |
| Trofin, F. et al. (2022, Romania) [57]. | 7 months | 28 | mRNA -1273/BNT162b2 2 doses | 30 and 60 days post 2nd dose | Anti-RBD antibodies (IgA and IgG) | ELISA commercial kit | No significant decrease in antibody levels 60 days post vaccination. Positive correlation of antibodies with lactation period. Negative correlation with child parity. No correlation between antibody titers and maternal age or vaccine type. |
| Wang, J. et al. (2022, USA) [47] | 40 days | 30 | mRNA-1273/BNT162b2 2 doses | Prevaccination, 18 days after 1st and 2nd dose | Anti-Spike antibodies (IgA and IgG) | Homemade ELISA | Peak IgG titers after the 2nd dose. Peak IgA after the 1st dose. Total of 10-fold and 100-fold increase in IgA and IgG post vaccination, respectively. Detectable IgG titers even 187 days after the 2nd dose. Positive correlation between IgG titers in HM and serum. No correlation between IgA titers in HM and serum. |
| Yang, X. et al. (2022, USA and UK) [58] | NA | 54 | mRNA-1273/BNT162b2 2 doses ChAdOx1-S/Ad.26.COV2.S 2 or 1 dose | Prevaccination and 14 days or 21–35 (J&J) days post last dose | Anti-Spike antibodies (IgA and IgG) | Homemade ELISA | mRNA vaccines induce higher IgA antibody titers compared to adenovirus-vectored vaccines. Detectable IgG titers in 86–100% of mRNA-vaccinated women and in 33–38% of adenovirus-vector-vaccinated women. Detectable IgA in 52–71% of mRNA-vaccinated women and in 17–23% of adenovirus-vector-vaccinated women. Vaccination does not lead to significant increase in secretory antibody titers. (<50% of samples had specific secretory antibodies.) Moderna vaccine induces 2-fold higher levels of secretory antibodies compared with other vaccines. |
| Ramirez DSR et al. (2021, Spain) [69] | 2 months | 93 | mRNA-1273/BNT162b2 2 doses | 14 days post 2nd dose | Anti-RBD antibodies (IgA, IgM and IgG) | ELISA commercial kit/NAA commercial kit | Detectable IgG and IgA but not IgM. Positive correlation between IgG titers in HM and serum, positive correlation between IgA and IgG titers in HM. No correlation between antibody levels and maternal age and BMI. |
| Lechosa-Muñiz C. et al. (2021, Spain) [61] | 1 month | 110 | mRNA-1273/BNT162b2 2 doses ChAdOx1-S 1 dose | 30 days after the last dose | Anti-SARS-CoV-2 antibodies (IgA and IgG) | Homemade ELISA, CLIA commercial kit | Higher titers of IgA and IgG in HM after mRNA vaccine compared to adenovirus-vectored vaccine (the latter received only 1 dose). |
| Gray KJ. et al. (2021, USA) [67] | NA | 31 | mRNA-1273/BNT162b2 2 doses | At time of 1st and 2nd dose, 2–5.5 weeks post 2nd dose | Anti-S and anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA/LUMINEX | Robust IgG titers, but not IgA and IgM titers after the 2nd dose. Higher IgA titers detected to Moderna group after the 2nd dose. |
| Perez S.E. et al. (2021, USA) [62] | 14 months | 27 | mRNA-1273/BNT162b2 2 doses | Prevaccination, 1, 3 and 6 months post vaccination | Anti-SARS-CoV-2 antibodies (IgA, IgM and IgG) | Homemade ELISA/sVNT commercial kit | Detectable IgG in all samples, IgA in about 1/2 of the samples and IgM in about 1/4 of samples. IgG reached their peak levels 1 month post vaccination. Detectable IgG titers even 6 months post vaccination. Detectable IgA and IgM titers even 3 months post vaccination. Positive correlation between IgG and IgA titers in HM and IgG titers in serum. Neutralizing capacity of HM even at 6 months post vaccination. Neutralizing capacity correlates positively with IgG titers. |
| Golan Y. et al. (2021, USA) [63] | NA | 48 | mRNA-1273/BNT162b2 2 doses | Prevaccination before 2nd dose and 4–10 weeks after 2nd dose | Anti-RBD antibodies (IgA and IgG) | Homemade ELISA | Higher IgA titers after the 1st dose. No further increase after the 2nd dose. Detectable IgA titers in 75% of participants. IgG titers increase after 1st dose, with further increase in their titers after 2nd dose. No significant difference in the immune response between mRNA-based vaccines. Positive correlation between IgG titers in HM and maternal serum. No severe adverse effect after vaccination. |
| Scaggs Huang F. et al. (2021, USA) [79] | 3 months | 98 | mRNA-1273/BNT162b2 2 doses | 14 days post 2nd dose | Anti-S1 (IgA, IgM and IgG) and anti-N antibodies (IgG) | Serology test/NAA | Anti-S1 IgG and IgA antibodies present in HM. IgM antibodies were not detectable in any sample. Positive correlation between IgG titers in serum and HM. |
| Jakuszko K. et al. (2021, Switzerland) [64] | 3 months | 28 | BNT162b2 2 doses | 8 ± 1, 22 ± 2, 29 ± 3 and 43 ± 4 after 1st dose | Anti-Spike antibodies (IgA, IgM and IgG) | ELISA commercial kit | Peak antibody titers 7 ± 3 days after 1st dose. Higher IgA titers in the HM of serum-positive IgA women compared to serum-negative ones. No IgM was detectable in any sample. Positive correlation between IgG titers in HM and serum. |
| Schwartz A. et al. (2021, Israel) [77] | 5 months | 61 | BNT162b2 2 doses | Post vaccination | Anti-RBD antibodies (IgA and IgG) | ELISA | IgG antibodies were detectable in all samples. Positive correlation between IgG titers in serum and HM. Neutralizing antibodies were detected in about 40% of samples. Secretory IgA was detected in 15% of samples. |
| Perl SH. et al. (2021, Israel) [65] | 8 weeks | 84 | BNT162b2 2 doses | Prevaccination 2, 3, 4, 5 and 6 weeks post 1st dose | Anti-SARS-CoV-2 antibodies (IgA and IgG) | CLIA commercial kit | Detectable IgA titers in 61.8% and 86.1% of participants at 2 and 4 weeks after the 1st dose, respectively. Increased IgA titers after the 1st and 2nd dose. Detectable IgA titers 6 weeks after the 1st dose. IgG titers increased 1 week after the 2nd dose. IgG was detectable in 97% of samples 5 and 6 weeks after the 1st dose. No severe adverse effects after vaccination. |
| Yeo KT. et al. (2021, Singapore) [76] | 4,5 months | 34 | BNT162b2 2 doses | Prevaccination 1, 3, 7, 14 and 21 days after 1st and 2nd dose | Anti-RBD antibodies (IgA, IgM and IgG) | Homemade ELISA/s-VNA commercial kit | Neutralizing antibodies in HM increased after the 2nd dose. Neutralizing antibodies in HM were detectable even 3 weeks after 2nd dose. Dominance of IgG1 response post vaccination. |
| Low JM. et al. (2021, Singapore) [66] | NA | 14 | BNT162b2 2 doses | Prevaccination 1–3 and 7–10 days post 1st dose, 3–7 days and 4–6 weeks post 2nd dose | Anti-Spike and anti-RBD antibodies (IgA and IgG) | Homemade ELISA | Presence of IgA antibodies in 93% of participants. Higher ΙgA titers 3–7 days after the 2nd dose. IgA titers waned 4–6 weeks after the 2nd dose. IgG antibodies detected in all samples. IgG titers increased after the 2nd dose. Stable high IgG titers even 4–6 weeks after the 2nd dose. No severe adverse effects in participants. |
| Baird JK. et al. (2021, USA) [68] | NA | 7 | mRNA-1273/BNT162b2 2 doses | Prevaccination 1, 4, 7 and 14 days post 1st and 2nd dose and 1 day before 2nd dose | Anti-S and anti-RBD antibodies (IgA and IgG) | Homemade ELISA | Vaccination mainly induced IgG response. No significant difference between 2 vaccines. Antibodies present even 80 days after vaccination in 1 sample collected. |
| Juncker HG. et al. (2021, the Netherlands) [70] | 1 month | 20 | BNT162b2 2 doses | Prevaccination 3, 5, 7, 9, 11, 13 and 15–17 days after 1st and 2nd doses and 1 day before 2nd dose | Anti-SARS-CoV-2 antibodies (IgA) | Homemade ELISA | Increased IgA titers 5–7 days after the 1st dose. IgA titers decreased by 50% between Day 15 and 21. IgA titers increased by 1.3 times after the 2nd dose compared to the 1st one. |
| Rosenberg-Friedman M. et al. (2021, Israel) [71] | NA | 10 | BNT162b2 2 doses | 7 and 14 days post 1st and 2nd doses | Anti-S and anti-RBD antibodies (IgA and IgG) | Homemade ELISA | IgG titers peaked 7 days after the 2nd dose. IgG titers remained high on Day 14 after the 2nd dose. Increased IgA titers 7 days post the 2nd dose. Increased neutralizing capacity observed after vaccination. |
| Scrimin F. et al. (2022, Switzerland) [72] | 6 months | 40 | mRNA-1273/BNT162b2 2 doses ChAdOx1-S 2 or 1 dose | 20–30 days, 1–2 months or 3–4 months post 2nd dose | Anti-SARS-CoV-2 antibodies (IgA and IgG) | ELISA commercial kit/NAA | IgG antibodies detected in all samples. IgG present even 4 months after the 2nd dose. No severe adverse effects in participants. |
| Marshall N.E. et al. (2022, USA) [45] | NA | 28 | mRNA-1273/BNT162b2 2 doses | Between 0–12 months postpartum | Anti-RBD antibodies (IgG) | Homemade ELISA | Half life of IgG in HM is about 2 months. Positive correlation between IgG titers in HM and serum. IgG1 and IgG3 are present in higher titers compared to IgG4 antibodies. |
| Esteve-Palau E. et al. (2021, Spain) [75] | NA | 33 | mRNA -based BNT162b2 2 doses | 2 weeks after 1st dose and 2 and 4 weeks after 2nd dose | Anti-S antibodies (IgG) | Serology test | Increased IgG titers after 2nd dose. Positive correlation between serum and HM IgG titers. |
| Gonçalves J. et al. (2021, Portugal) [74] | 7 months | 23 | mRNA-1273/BNT162b2 2 doses | Prevaccination, a median of 10 days after 1st and 2nd dose | Anti-S antibodies (sIgA/IgA, IgM and IgG) | Homemade ELISA | Antibodies present in the HM of 96% of participants. Increased IgG titers after the 2nd dose. Increased IgA titers after the 1st dose. Poorly increased IgM antibodies after vaccination. Positive correlation between IgA and IgG titers in HM. Positive correlation between IgA titers in serum and HM. Antibody titers were not correlated with maternal age. |
| Lechosa-Muniz C. et al. (2023, Spain) [88] | 6 months | 62 | mRNA-1273/BNT162b2 2 doses ChAdOx1-S 1 dose | 6 months post vaccination | Anti-S antibodies (IgA and IgG) | Homemade ELISA/CLIA commercial kit | No significant difference in antibody levels according to vaccine type. |
| Charepe N. et al. (2021, Portugal) [73] | 2 months | 14 | BNT162b2 2 doses | 1–3 weeks post 1st and 2nd dose | Anti-S antibodies (IgA, IgM and IgG) | Homemade ELISA | Increased IgG titers after the 2nd dose. IgA peaked after the 1st dose. No IgM response was observed. |
| Kelly JC. et al. (2021, USA) [78] | NA | 5 | BNT162b2 2 doses | Prevaccination within 24 h after 1st dose and a week post vaccination | Anti-S antibodies (IgA and IgG) | ELISA | Anti-S antibodies were present in HM. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimitroglou, M.; Sokou, R.; Iacovidou, N.; Pouliakis, A.; Kafalidis, G.; Boutsikou, T.; Iliodromiti, Z. Anti-SARS-CoV-2 Immunoglobulins in Human Milk after Coronavirus Disease or Vaccination—Time Frame and Duration of Detection in Human Milk and Factors That Affect Their Titers: A Systematic Review. Nutrients 2023, 15, 1905. https://doi.org/10.3390/nu15081905
Dimitroglou M, Sokou R, Iacovidou N, Pouliakis A, Kafalidis G, Boutsikou T, Iliodromiti Z. Anti-SARS-CoV-2 Immunoglobulins in Human Milk after Coronavirus Disease or Vaccination—Time Frame and Duration of Detection in Human Milk and Factors That Affect Their Titers: A Systematic Review. Nutrients. 2023; 15(8):1905. https://doi.org/10.3390/nu15081905
Chicago/Turabian StyleDimitroglou, Margarita, Rozeta Sokou, Nicoletta Iacovidou, Abraham Pouliakis, Georgios Kafalidis, Theodora Boutsikou, and Zoi Iliodromiti. 2023. "Anti-SARS-CoV-2 Immunoglobulins in Human Milk after Coronavirus Disease or Vaccination—Time Frame and Duration of Detection in Human Milk and Factors That Affect Their Titers: A Systematic Review" Nutrients 15, no. 8: 1905. https://doi.org/10.3390/nu15081905
APA StyleDimitroglou, M., Sokou, R., Iacovidou, N., Pouliakis, A., Kafalidis, G., Boutsikou, T., & Iliodromiti, Z. (2023). Anti-SARS-CoV-2 Immunoglobulins in Human Milk after Coronavirus Disease or Vaccination—Time Frame and Duration of Detection in Human Milk and Factors That Affect Their Titers: A Systematic Review. Nutrients, 15(8), 1905. https://doi.org/10.3390/nu15081905