
Bone Remodelling, Vitamin D Status, and Lifestyle Factors in Spanish Vegans, Lacto-Ovo Vegetarians, and Omnivores

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Anthropometry and Body Composition
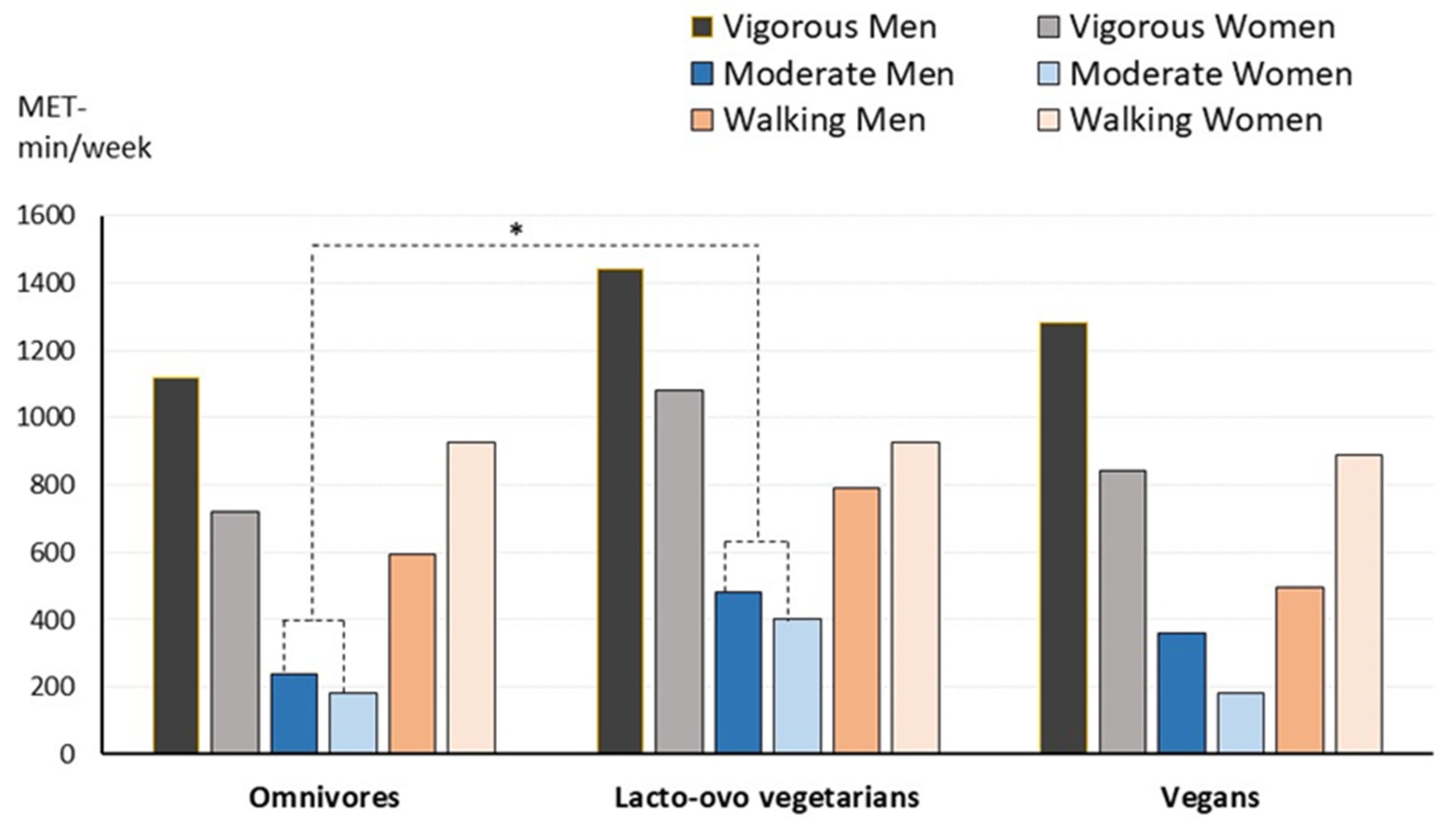
2.3. Physical Activity and Dietary Intake Assessments
2.4. Sampling and Analytical Determinations
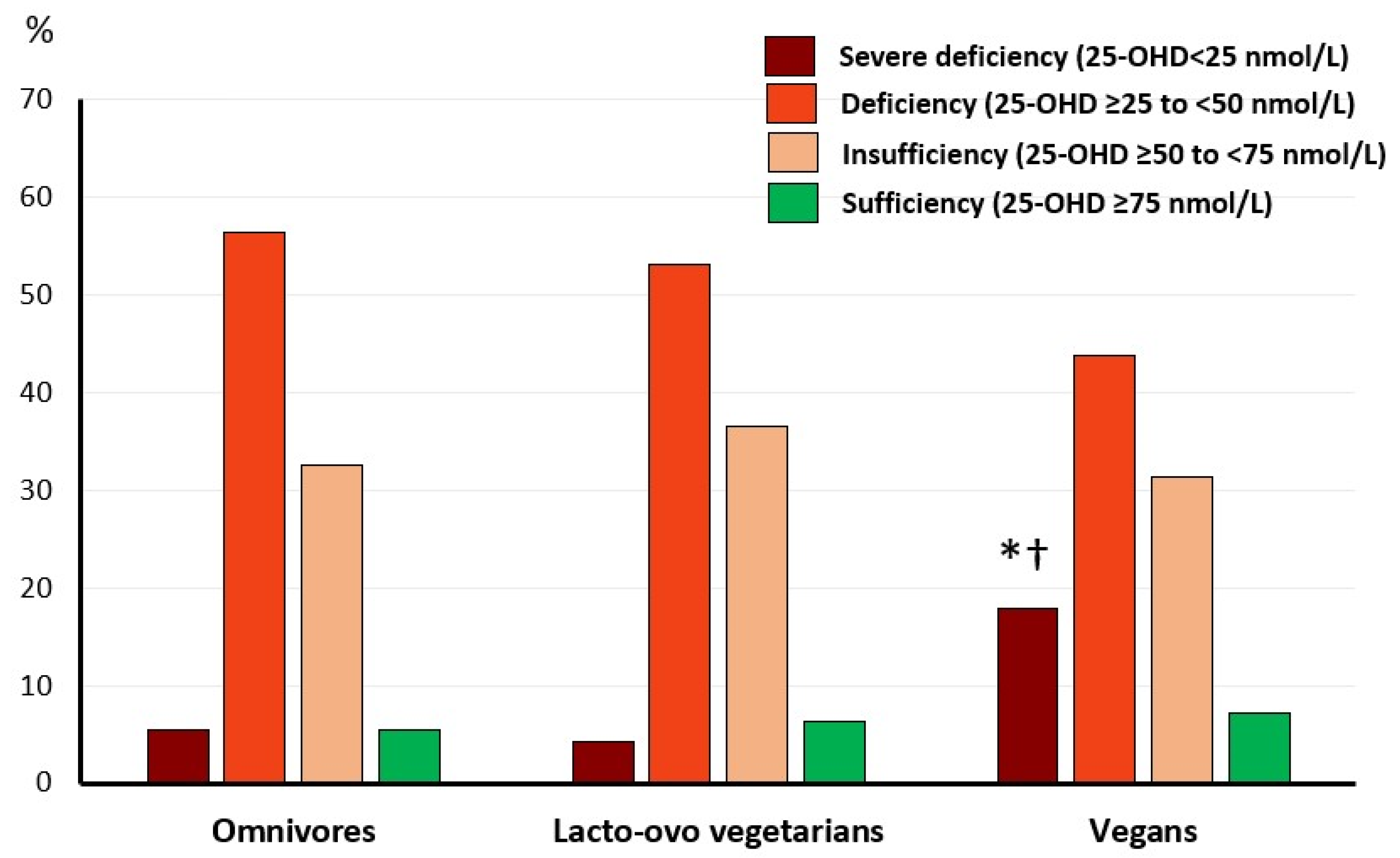
2.5. Vitamin D Status Levels
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Directions for Further Investigations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FAO; WHO. Sustainable Healthy Diets: Guiding Principles; FAO: Rome, Italy; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 11. [Google Scholar] [CrossRef]
- Kahleova, H.; Levin, S.; Barnard, N. Cardio-Metabolic Benefits of Plant-Based Diets. Nutrients 2017, 9, 848. [Google Scholar] [CrossRef]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, Vegan Diets and Multiple Health Outcomes: A Systematic Review with Meta-Analysis of Observational Studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef]
- Kim, J.; Kim, H.; Giovannucci, E.L. Plant-Based Diet Quality and the Risk of Total and Disease-Specific Mortality: A Population-Based Prospective Study. Clin. Nutr. 2021, 40, 5718–5725. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Narbón, A.; Zapatera, B.; Barrios, L.; Vaquero, M.P. Vitamin B12 and Folate Status in Spanish Lacto-Ovo Vegetarians and Vegans. J. Nutr. Sci. 2019, 8, e7. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Narbón, A.; Zapatera, B.; Vaquero, M.P. Physiological and Dietary Determinants of Iron Status in Spanish Vegetarians. Nutrients 2019, 11, 1734. [Google Scholar] [CrossRef] [PubMed]
- García-Maldonado, E.; Zapatera, B.; Alcorta, A.; Vaquero, M.P. A Microalgae Docosahexaenoic Acid Supplement Does Not Modify the Influence of Gender and Diet on Iron Status in Spanish Vegetarians or Omnivores. A Randomized Placebo-Controlled Crossover Study. Nutrition 2024, 118, 112282. [Google Scholar] [CrossRef] [PubMed]
- Tucker, K.L. Vegetarian Diets and Bone Status. Am. J. Clin. Nutr. 2014, 100, 329S–335S. [Google Scholar] [CrossRef]
- Falchetti, A.; Cavati, G.; Valenti, R.; Mingiano, C.; Cosso, R.; Gennari, L.; Chiodini, I.; Merlotti, D. The Effects of Vegetarian Diets on Bone Health: A Literature Review. Front. Endocrinol. 2022, 13, 899375. [Google Scholar] [CrossRef] [PubMed]
- Schüpbach, R.; Wegmüller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Menzel, J.; Abraham, K.; Stangl, G.I.; Ueland, P.M.; Obeid, R.; Schulze, M.B.; Herter-Aeberli, I.; Schwerdtle, T.; Weikert, C. Vegan Diet and Bone Health-Results from the Cross-Sectional RBVD Study. Nutrients 2021, 13, 685. [Google Scholar] [CrossRef]
- Světnička, M.; Heniková, M.; Selinger, E.; Ouřadová, A.; Potočková, J.; Kuhn, T.; Gojda, J.; El-Lababidi, E. Prevalence of iodine deficiency among vegan compared to vegetarian and omnivore children in the Czech Republic: Cross-sectional study. Eur. J. Clin. Nutr. 2023, 77, 1061–1070. [Google Scholar] [CrossRef]
- Ekmeiro-Salvador, J.E.; Storz, M.A. The Impact of Plant-Based Diets on Dietary Acid Load Metrics in Venezuela: A Cross-Sectional Study. Nutrients 2023, 15, 2745. [Google Scholar] [CrossRef]
- Appleby, P.; Roddam, A.; Allen, N.; Key, T. Comparative Fracture Risk in Vegetarians and Nonvegetarians in EPIC-Oxford. Eur. J. Clin. Nutr. 2007, 61, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Hadjidakis, D.J.; Androulakis, I.I. Bone Remodeling. Ann. N. Y. Acad. Sci. 2006, 1092, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Bolamperti, S.; Villa, I.; Rubinacci, A. Bone Remodeling: An Operational Process Ensuring Survival and Bone Mechanical Competence. Bone Res. 2022, 10, 48. [Google Scholar] [CrossRef] [PubMed]
- Song, L. Chapter One—Calcium and Bone Metabolism Indices. In Advances in Clinical Chemistry; Makowski, G.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2017; Volume 82, pp. 1–46. [Google Scholar] [CrossRef]
- Toxqui, L.; Perez-Granados, A.; Blanco-Rojo, R.; Wright, I.; de la Piedra, C.; Vaquero, M.P. Low Iron Status as a Factor of Increased Bone Resorption and Effects of an Iron and Vitamin D-Fortified Skimmed Milk on Bone Remodelling in Young Spanish Women. Eur. J. Nutr. 2014, 53, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Papakitsou, E.; Paspati, I.; Rizou, S.; Lyritis, G.P. Bone metabolism subgroups identified as hip fracture patients via clustering. Hormones 2021, 20, 545–555. [Google Scholar] [CrossRef]
- Spencer, E.A.; Appleby, P.N.; Davey, G.K.; Key, T.J. Diet and Body Mass Index in 38 000 EPIC-Oxford Meat-Eaters, Fish-Eaters, Vegetarians and Vegans. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2003, 27, 728–734. [Google Scholar] [CrossRef]
- García-Maldonado, E.; Zapatera, B.; Alcorta, A.; Vaquero, M.P. Metabolic and Nutritional Biomarkers in Adults Consuming Lacto-Ovo Vegetarian, Vegan and Omnivorous Diets in Spain. A Cross-Sectional Study. Food Funct. 2023, 14, 1608–1616. [Google Scholar] [CrossRef]
- Jedut, P.; Glibowski, P.; Skrzypek, M. Comparison of the Health Status of Vegetarians and Omnivores Based on Biochemical Blood Tests, Body Composition Analysis and Quality of Nutrition. Nutrients 2023, 15, 3038. [Google Scholar] [CrossRef]
- García-Morant, A.; Cortés-Castell, E.; Palazón-Bru, A.; Martínez-Amorós, N.; Gil-Guillén, V.F.; Rizo-Baeza, M.M. Macronutrients and Micronutrients in Spanish Adult Vegans (Mediterranean Population). Nutr. Hosp. 2020, 37, 549–558. [Google Scholar]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- ISO 9001:2015; Quality Management Systems Requirements. International Organization for Standardization: Geneva, Switzerland, 2015. Available online: https://www.iso.org/standard/62085.html (accessed on 11 December 2023).
- Cashman, K.D. 100 Years of Vitamin D: Global Differences in Vitamin D Status and Dietary Intake: A Review of the Data. Endocr. Connect. 2022, 11, e210282. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D Deficiency 2.0: An Update on the Current Status Worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Menal-Puey, S.; Morán del Ruste, M.; Marques-Lopes, I. Nutritional Composition of Common Vegetarian Food Portions. Nutr. Hosp. 2016, 33, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Davey, G.K.; Spencer, E.A.; Appleby, P.N.; Allen, N.E.; Knox, K.H.; Key, T.J. EPIC–Oxford:Lifestyle Characteristics and Nutrient Intakes in a Cohort of 33 883 Meat-Eaters and 31 546 Non Meat-Eaters in the UK. Public Health Nutr. 2003, 6, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Steur, M.; Allen, N.E.; Appleby, P.N.; Travis, R.C.; Key, T.J. Plasma Concentrations of 25-Hydroxyvitamin D in Meat Eaters, Fish Eaters, Vegetarians and Vegans: Results from the EPIC–Oxford Study. Public Health Nutr. 2011, 14, 340–346. [Google Scholar] [CrossRef]
- Manios, Y.; Moschonis, G.; Lambrinou, C.-P.; Tsoutsoulopoulou, K.; Binou, P.; Karachaliou, A.; Breidenassel, C.; Gonzalez-Gross, M.; Kiely, M.; Cashman, K.D. A Systematic Review of Vitamin D Status in Southern European Countries. Eur. J. Nutr. 2018, 57, 2001–2036. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific opinion on dietary reference values for vitamin D. EFSA J. 2016, 14, e04547. [Google Scholar] [CrossRef]
- Blanco-Rojo, R.; Perez-Granados, A.; Toxqui, L.; Zazo, P.; de la Piedra, C.; Vaquero, M.P. Relationship between Vitamin D Deficiency, Bone Remodelling and Iron Status in Iron-Deficient Young Women Consuming an Iron-Fortified Food. Eur. J. Nutr. 2013, 52, 695–703. [Google Scholar] [CrossRef]
- Hansen, T.H.; Madsen, M.T.B.; Jørgensen, N.R.; Cohen, A.S.; Hansen, T.; Vestergaard, H.; Pedersen, O.; Allin, K.H. Bone turnover, calcium homeostasis, and vitamin D status in Danish vegans. Eur. J. Clin. Nutr. 2018, 72, 1046–1054. [Google Scholar] [CrossRef]
- Alexy, U.; Fischer, M.; Weder, S.; Längler, A.; Michalsen, A.; Sputtek, A.; Keller, M. Nutrient Intake and Status of German Children and Adolescents Consuming Vegetarian, Vegan or Omnivore Diets: Results of the VeChi Youth Study. Nutrients 2021, 13, 1707. [Google Scholar] [CrossRef]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2021, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.P.; Bucca, G.; Penson, S.; Chope, G.; Hyppönen, E.; Berry, J.; Vieth, R.; et al. Comparison of Vitamin D2 and Vitamin D3 Supplementation in Raising Serum 25-Hydroxyvitamin D Status: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef]
- Turck, D.; Bresson, J.-L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; Mangelsdorf, I.; McArdle, H.J.; Naska, A.; et al. Dietary Reference Values for Vitamin K. EFSA J. 2017, 15, e04780. [Google Scholar] [CrossRef]
- Aloia, J.F.; Feuerman, M.; Yeh, J.K. Reference Range for Serum Parathyroid Hormone. Endocr. Pract. 2006, 12, 137–144. [Google Scholar] [CrossRef]
- Arslanca, T.; Korkmaz, V.; Arslanca, S.B.; Karadag, B.; Ergün, Y. Body Iodine Status in Women with Postmenopausal Osteoporosis. Menopause 2018, 25, 320–323. [Google Scholar] [CrossRef]
- Amin, N.; Clark, C.C.T.; Taghizadeh, M.; Djafarnejad, S. Zinc Supplements and Bone Health: The Role of the RANKL-RANK Axis as a Therapeutic Target. J. Trace Elem. Med. Biol. 2020, 57, 126417. [Google Scholar] [CrossRef]
- Schiessl, H.; Frost, H.M.; Jee, W.S. Estrogen and bone-muscle strength and mass relationships. Bone 1998, 22, 1–6. [Google Scholar] [CrossRef]
- Zittermann, A.; Schmidt, A.; Haardt, J.; Kalotai, N.; Lehmann, A.; Egert, S.; Ellinger, S.; Kroke, A.; Lorkowski, S.; Louis, S.; et al. Protein intake and bone health: An umbrella review of systematic reviews for the evidence-based guideline of the German Nutrition Society. Osteoporos. Int. 2023, 34, 1335–1353. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Omnivores (n = 93) | Lacto-Ovo Vegetarians (n = 96) | Vegans (n = 112) | p Group | p Gender | ||||
|---|---|---|---|---|---|---|---|---|
| Man (n = 41) | Woman (n = 52) | Man (n = 27) | Woman (n = 69) | Man (n = 32) | Woman (n = 80) | |||
| Age | 25.8 ± 6.7 | 25.2 ± 5.1 | 27.8 ± 7.9 * | 28.8 ± 7.3 * | 30.6 ± 6.4 * | 28.1 ± 6.4 * | <0.001 | 0.482 |
| Body weight (kg) | 72.0 ± 12.2 | 58.0 ± 7.8 | 72.9 ± 12.0 | 58.8 ± 8.2 | 72.5 ± 9.7 | 58.5 ± 8.0 | 0.814 | <0.001 |
| BMI (kg/m2) | 23.2 ± 3.1 | 21.7 ± 2.3 | 23.3 ± 3.7 | 22.3 ± 3.4 | 23.3 ± 3.1 | 21.9 ± 2.9 | 0.765 | <0.001 |
| Waist perimeter (cm) | 82.6 ± 8.5 | 73.7 ± 6.4 | 84.6 ± 11.2 | 76.2 ± 8.5 | 84.2 ± 8.5 | 75.7 ± 8.1 | 0.193 | <0.001 |
| Hip perimeter (cm) | 94.9 ± 7.4 | 94.7 ± 6.4 | 95.6 ± 6.5 | 96.1 ± 7.1 | 94.9 ± 5.6 | 95.2 ± 6.2 | 0.809 | 0.627 |
| Bone mass (kg) # | 3.0 (2.9, 3.3) | 2.2 (2.2, 2.3) | 3.1 (2.8, 3.3) | 2.2 (2.2, 2.3) | 3.0 (2.9, 3.2) | 2.2 (2.2, 2.3) | 0.970 | <0.001 |
| Muscle mass (kg) | 57.6 ± 7.9 | 41.7 ± 3.5 | 58.3 ± 8.0 | 40.9 ± 3.3 | 58.3 ± 6.2 | 41.1 ± 3.6 | 0.994 | <0.001 |
| Water (%) | 59.6 ± 10.2 | 56.4 ± 4.4 | 61.1 ± 5.6 | 54.6 ± 4.3 | 60.9 ± 4.7 | 54.9 ± 4.4 | 0.952 | <0.001 |
| Fat (%) | 15.2 ± 5.3 | 23.7 ± 6.0 | 15.0 ± 6.8 | 25.9 ± 6.1 | 14.9 ± 6.1 | 25.4 ± 6.1 | 0.536 | <0.001 |
| Omnivores (n = 88) | Lacto-Ovo Vegetarians (n = 53) | Vegans (n = 59) | p Group | p Gender | ||||
|---|---|---|---|---|---|---|---|---|
| Man (n = 39) | Woman (n = 49) | Man (n = 16) | Woman (n = 37) | Man (n = 22) | Woman (n = 37) | |||
| Energy (Kcal) | 2407 ± 101 | 1979 ± 661 | 2716 ± 756 | 2004 ± 505 | 2632 ± 619 | 1955 ± 548 | 0.306 | <0.001 |
| Proteins (%E) | 17.3 ± 4.0 | 16.5 ± 3.7 | 14.1 ± 4.2 * | 14.7 ± 4.0 * | 14.0 ± 4.2 * | 14.9 ± 4.6 * | <0.001 | 0.721 |
| CHO (%E) | 38.1 ± 7.8 | 37.6 ± 8.4 | 41.6 ± 6.0 * | 43.5 ± 6.8 * | 45.7 ± 10.4 *,† | 47.3 ± 8.4 *,† | <0.001 | 0.418 |
| Fibre (g) | 28.3 ± 14.3 | 24.6 ± 12.0 | 50.2 ± 23.6 * | 32.7 ± 12.4 * | 57.7 ± 33.2 *,† | 39.0 ± 14.0 *,† | <0.001 | <0.001 |
| Fat (%E) | 40.0 ± 8.3 | 42.1 ± 9.7 | 39.8 ± 6.8 | 37.1 ± 7.9 | 35.1 ± 9.1 *,† | 32.8 ± 9.2 *,† | <0.001 | 0.486 |
| SFA (%E) | 12.4 ± 2.9 | 12.7 ± 4.0 | 9.4 ± 3.5 * | 10.6 ± 3.9 * | 6.0 ± 1.9 *,† | 7.2 ± 3.3 *,† | <0.001 | 0.087 |
| MUFA (%E) | 16.1 ± 4.3 | 17.9 ± 6.2 | 16.4 ± 5.4 | 14.3 ± 6.0 | 15.2 ± 6.2 * | 12.8 ± 5.5 * | 0.011 | 0.297 |
| PUFA (%E) | 5.8 ± 2.9 | 6.0 ± 2.3 | 6.8 ± 2.0 | 5.9 ± 2.7 | 8.2 ± 6.5 * | 6.8 ± 3.0 * | 0.020 | 0.201 |
| Ca (mg) | 878 ± 361 | 759 ± 327 | 851 ± 352 | 703 ± 427 | 644 ± 223 *,† | 559 ± 259 *,† | <0.001 | 0.022 |
| P (g) | 1.63 ± 0.61 | 1.30 ± 0.47 | 1.68 ± 0.85 | 1.20 ± 0.48 | 1.40 ± 0.50 * | 0.95 ± 0.42 * | 0.005 | <0.001 |
| Mg (mg) | 353 ± 144 | 280 ± 106 | 519 ± 269 * | 369 ± 152 * | 512 ± 176 * | 364 ± 184 * | <0.001 | <0.001 |
| Na (g) | 2.46 ± 0.12 | 1.97 ± 0.78 | 2.22 ± 0.98 | 2.01 ± 1.03 | 2.14 ± 1.29 | 1.53 ± 0.89 | 0.090 | 0.005 |
| K (g) | 3.32 ± 0.13 | 2.78 ± 1.00 | 4.09 ± 1.56 | 3.07 ± 1.28 | 3.82 ± 1.55 | 2.92 ± 1.20 | 0.061 | <0.001 |
| I (µg) # | 100 (81, 112) | 74 (63, 88) | 43 (32, 102) * | 47 (34, 57) * | 56 (43, 68) * | 38 (32, 39) * | <0.001 | <0.001 |
| Zn (mg) # | 11.0 (10.2, 13.7) | 8.3 (7.8, 9.0) | 9.6 (7.6, 14.7) | 7.8 (6.8, 8.5) | 9.3 (7.6, 11.6) * | 6.0 (4.7, 8.2) * | 0.006 | <0.001 |
| Vit A (RE µg) | 628 (584, 716) | 705 (563, 873) | 1101 (792, 2191) * | 923 (699, 1166) * | 872 (474, 1117) † | 643 (438,873) † | 0.016 | 0.428 |
| Retinol (µg) | 337 (279, 379) | 234 (186, 292) | 267 (75, 359) * | 144 (73, 224) * | 0.85 (0.0, 10.8) *,† | 4.5 (0.4, 13.9) *,† | <0.001 | 0.540 |
| Carotenes (mg) | 1.4 (1.0, 1.8) | 2.0 (1.3, 2.6) | 3.1 (2.1, 9.3) * | 3.5 (1.5, 5.3) * | 3.7 (2.5, 6.0) * | 2.7 (2.1, 4.5) * | <0.001 | 0.597 |
| Vit C (mg) | 107 (79, 166) | 99 (77, 141) | 149 (115, 239) | 134 (86, 184) | 129 (101, 182) | 122 (107, 163) | 0.032 | 0.100 |
| Vit D (µg) | 2.2 (1.9, 3.0) | 2.1 (1.1, 2.7) | 1.4 (1.0, 2.5) * | 1.1 (0.5, 1.7) * | 0.6 (0.3, 1.4) * | 0.9 (0.5, 1.4) * | <0.001 | 0.480 |
| Vit E (mg) | 8.3 (8.0, 10.7) | 9.7 (8.1, 11.7) | 14.8 (14.5, 18.4) | 9.5 (8.0, 11.3) | 12.2 (10.4, 16.3) | 11.0 (7.5, 14.2) | 0.037 | 0.001 |
| Vit K (µg) | 126 (106, 179) | 120 (100, 160) | 274 (147, 289) | 135 (90, 178) | 288 (228, 365) * | 129 (98, 261) | 0.005 | 0.002 |
| Omnivores (n = 86) | Lacto-Ovo Vegetarians (n = 44) | Vegans (n = 56) | p Group | p Gender | ||||
|---|---|---|---|---|---|---|---|---|
| Men (n = 38) | Women (n = 48) | Men (n = 15) | Women (n = 29) | Men (n = 19) | Women (n = 37) | |||
| PTH (pg/mL) | 49.2 ± 22.2 | 49.8 ± 21.0 | 57.9 ± 15.6 | 56.6 ± 20.1 | 59.4 ± 24.1 * | 65.8 ± 21.3 * | 0.003 | 0.687 |
| 25-OHD (nmol/L) | 46.6 ± 16.2 | 46.4 ± 16.2 | 42.4 ± 12.8 | 45.2 ± 15.8 | 40.7 ± 19.0 | 38.6 ± 20.3 | 0.069 | 0.908 |
| BAP (µg/L) # | 20 (18, 22) | 15 (14, 16) | 19 (12, 24) | 14 (11, 19) | 18 (14, 22) | 15 (14, 18) | 0.104 | <0.001 |
| NTx (nM/mM creatinine) # | 78 (66, 103) | 63 (56, 79) | 93 (75, 117) | 77 (66, 107) | 90 (77, 115) * | 91 (66, 108) * | 0.002 | 0.136 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Maldonado, E.; Gallego-Narbón, A.; Zapatera, B.; Alcorta, A.; Martínez-Suárez, M.; Vaquero, M.P. Bone Remodelling, Vitamin D Status, and Lifestyle Factors in Spanish Vegans, Lacto-Ovo Vegetarians, and Omnivores. Nutrients 2024, 16, 448. https://doi.org/10.3390/nu16030448
García-Maldonado E, Gallego-Narbón A, Zapatera B, Alcorta A, Martínez-Suárez M, Vaquero MP. Bone Remodelling, Vitamin D Status, and Lifestyle Factors in Spanish Vegans, Lacto-Ovo Vegetarians, and Omnivores. Nutrients. 2024; 16(3):448. https://doi.org/10.3390/nu16030448
Chicago/Turabian StyleGarcía-Maldonado, Elena, Angélica Gallego-Narbón, Belén Zapatera, Alexandra Alcorta, Miriam Martínez-Suárez, and M. Pilar Vaquero. 2024. "Bone Remodelling, Vitamin D Status, and Lifestyle Factors in Spanish Vegans, Lacto-Ovo Vegetarians, and Omnivores" Nutrients 16, no. 3: 448. https://doi.org/10.3390/nu16030448
APA StyleGarcía-Maldonado, E., Gallego-Narbón, A., Zapatera, B., Alcorta, A., Martínez-Suárez, M., & Vaquero, M. P. (2024). Bone Remodelling, Vitamin D Status, and Lifestyle Factors in Spanish Vegans, Lacto-Ovo Vegetarians, and Omnivores. Nutrients, 16(3), 448. https://doi.org/10.3390/nu16030448