1. Introduction
The preschool period is a crucial time in a person’s life when long-term dietary habits are established. These habits play a pivotal role in shaping the person’s healthy eating patterns later in life [
1]. Picky eating is one of the common dietary behaviors in young children [
2] and is considered a barrier to healthy eating behaviors [
3]. The prevalence of picky eating has been estimated to range from 5.6% to 47%, and this variation in prevalence is due to differences in assessment methods, children’s ages, and the countries in which studies have been conducted [
4,
5]. A universally accepted definition of picky eating is not yet available, and consensus regarding the most effective tool for identifying it has yet to be reached [
6]. Picky eating behaviors include a child’s refusal to eat both familiar and unfamiliar foods, their reluctance to try new foods, and the development of strong preferences for certain foods [
7].
Picky eating can lead to a reduction in dietary variety, potentially resulting in an unhealthy diet or one lacking adequate nutrition [
6]. Compared with non-picky eaters, picky eaters consume a narrower range of food items [
8]. Such limited variety can result in poor growth, being underweight [
9,
10] or overweight [
3], or developing eating disorders [
11]. Also, picky eaters may experience constipation due to inadequate intake of dietary fiber, commonly resulting from low fruit and vegetable consumption [
12]. The causes of picky eating include early feeding challenges, delayed introduction of textured foods during weaning, external pressure to eat certain foods, and early signs of selective food preferences [
13].
Preferences and eating habits established during childhood often persist into adolescence and may even endure into adulthood [
14]. In addition, a longitudinal generational study found that children who exhibited picky eating behaviors at 3 years of age tended to continue these behaviors until the ages of 10 and 13 years [
15]. Some children who exhibit persistent picky eating tendencies may encounter developmental challenges and may be prone to thinness during adolescence or the development of eating disorders, including picky eating, in adulthood [
16]. Another study reported that, compared with children with normal weights, those who were overweight or obese had significantly higher scores for picky eating and food neophobia [
3]. Furthermore, a separate study indicated that individuals who were picky eaters as children were more likely to maintain selective eating patterns and emotional undereating in young adulthood, being less likely to consume a nutritious diet in adulthood. These trends highlight the prolonged effect of childhood eating behaviors on one’s diet and body weight, underscoring the importance of early intervention in promoting healthy eating habits [
17]. In summary, establishing healthy eating habits in early childhood is crucial.
Picky eating in children can result in a variety of outcomes related to parenting, including parental concerns regarding the child’s growth and health, mealtime conflicts, and parental guilt. Parents often perceive food pickiness as a manifestation of opposition and assertiveness in their children [
18]. Thus, picky eating behaviors in young children can cause considerable stress, anxiety, and strain in family relationships [
19]. Parents and primary caregivers, being the primary providers of food for young children, play a crucial role in establishing children’s dietary preferences. Strategies and behaviors used by parents and primary caregivers to achieve specific dietary goals for their children are known as food parenting practices [
20]. Food behaviors and feeding strategies adopted by parents are the most pivotal factors affecting a child’s eating behaviors and food preferences. Parents serve as key role models by introducing their children to diverse nutritious food choices. Through various feeding practices, parents and primary caregivers can influence the dietary behaviors of young children and guide them toward the achievement of specific dietary objectives [
21].
The importance of family mealtimes, routines, and nutritious meals is typically agreed on by couples. However, disagreements can arise during discussions of strategies to restrict unhealthy foods and establish a harmonious atmosphere during family mealtimes [
22]. Such disputes are often related to problems such as access to energy-dense, nutrient-poor snacks and the introduction of dietary variety [
23].
Parents use effective strategies to address or alleviate picky eating in their children, including repeatedly exposing them to unfamiliar foods, modeling healthy eating behaviors, co-preparing meals, and fostering positive social experiences during mealtimes. However, counterproductive strategies, such as offering rewards for eating, have also been observed. These findings indicate that parents could benefit from higher-quality information regarding the nature of food pickiness and proven strategies for managing it [
18]. One study focused on maternal feeding practices, dietary intake, and BMI in 5 year-olds in a multiethnic Asian population. That study determined that higher levels of maternal role modeling, encouragement of a diverse and balanced diet, and instruction regarding nutritional knowledge were associated with higher levels of vegetable and whole grain intake in children [
24]. A positive and encouraging approach, such as rewarding children for trying new foods, is more effective in promoting a preference for and acceptance of healthy foods compared with strict or forceful methods [
20].
Extensive evidence indicates the crucial roles of both coparenting quality and food-related parenting practices in shaping children’s behavioral outcomes. However, whether coparenting quality affects food-related parenting practices remains unclear [
25]. In particular, in Taiwan, few studies have simultaneously explored the relations among dietary coparenting, parenting strategies, and young children’s picky eating behaviors. Accordingly, the findings of this study provide insights into picky eating behaviors and cultural differences among eating behaviors. The present study examined the relations among dietary coparenting, parenting strategies, and children’s picky eating behaviors in children aged 3–6 years in northern Taiwan.
4. Discussion
In this study, similar to some previous studies [
31,
32], we classified children with an average score of three (indicating “sometimes”) or higher as picky eaters, where the average score refers to the assessment of young children’s preferences for different types of food. Based on this criterion, we calculated the proportion of children exhibiting picky eating behaviors. We observed that 31.6% of the young children in our study exhibited picky eating behaviors. This proportion was slightly lower than those reported in previous studies [
33,
34,
35]. For example, one study indicated that 42.2% of young children aged between 1 and 5 years were picky eaters [
33]. A study conducted in Taiwan reported a prevalence of 54% for picky eating among young children [
35]. Variations in the definitions of picky eating and differences in assessment methods may have contributed to the wide range of the reported prevalence rates.
This study analyzed the distribution of various forms of picky eating. The results revealed that 15.5% of the young children in our study did not like to eat vegetables. Vegetables often have bitter or strong flavors after cooking, which may be a reason for why many children do not eat them [
2]. In addition, picky eaters were significantly more likely to dislike eating vegetables, fruits, meat, and seafood than non-picky eaters were. This finding is consistent with those of other studies, indicating that a common pattern among picky eaters is a lower intake of vegetables and, to a lesser extent, fruits than that of non-picky eaters [
36,
37,
38]. Understanding the distribution of picky eating behaviors can provide insights into young children’s eating patterns and nutritional status and reveal possible research directions for future studies. For example, a meta-analysis of studies on parent-targeted home-based interventions indicated that higher exposure to different tastes substantially improved vegetable intake among children [
39].
In this research, coparenting was divided into two types, namely supportive and undermining coparenting, and we evaluated the relations between these two types and young children’s picky eating behaviors. The significant, negative direct effect of supportive coparenting on picky eating behaviors highlights the key role of supportive coparenting in shaping young children’s eating behaviors. Our study also revealed that undermining coparenting had a significant, positive direct effect on picky eating behaviors in young children. These findings emphasize the different roles of supportive and undermining coparenting in shaping young children’s eating behaviors. This result is consistent with those of previous studies showing that coparenting was particularly beneficial for young children’s diets when the parents had cohesive dietary choices and collaborated to foster healthy eating habits, which increased the likelihood of their children adopting and maintaining such habits [
40]. Lower coparenting agreement and support were associated with increased parenting stress, specifically stress related to challenges in managing disruptive behaviors during meals [
41]. These studies corroborate our finding of the role of supportive coparenting being associated with lower picky eating behaviors and emphasize the need for a holistic approach that considers coparenting and parenting education programs, along with interventions, to promote healthy eating habits in children.
Our research is consistent with previous studies demonstrating the importance of positive parenting strategies in improving children’s diets [
21,
24]. For example, higher levels of maternal role modeling, encouragement with respect to having a diverse and balanced diet, and instruction regarding nutritional information were determined to be associated with increased vegetable and whole grain intake among children in a multiethnic Asian population [
24]. Our findings indicate that the parents were most effective in encouraging and enabling their children to try new foods, with these activities scoring significantly higher than the others. This result indicates that parenting education should prioritize guiding, modeling, and teaching fun and engaging methods for introducing children to new foods, indicating their potential effectiveness in fostering healthier eating habits [
28,
42]. Addressing these aspects can guide parents aimed at promoting healthy eating behaviors among young children, and it can provide a practical foundation for parenting education to ensure young children receive well-rounded nutrition and foster their overall growth and development.
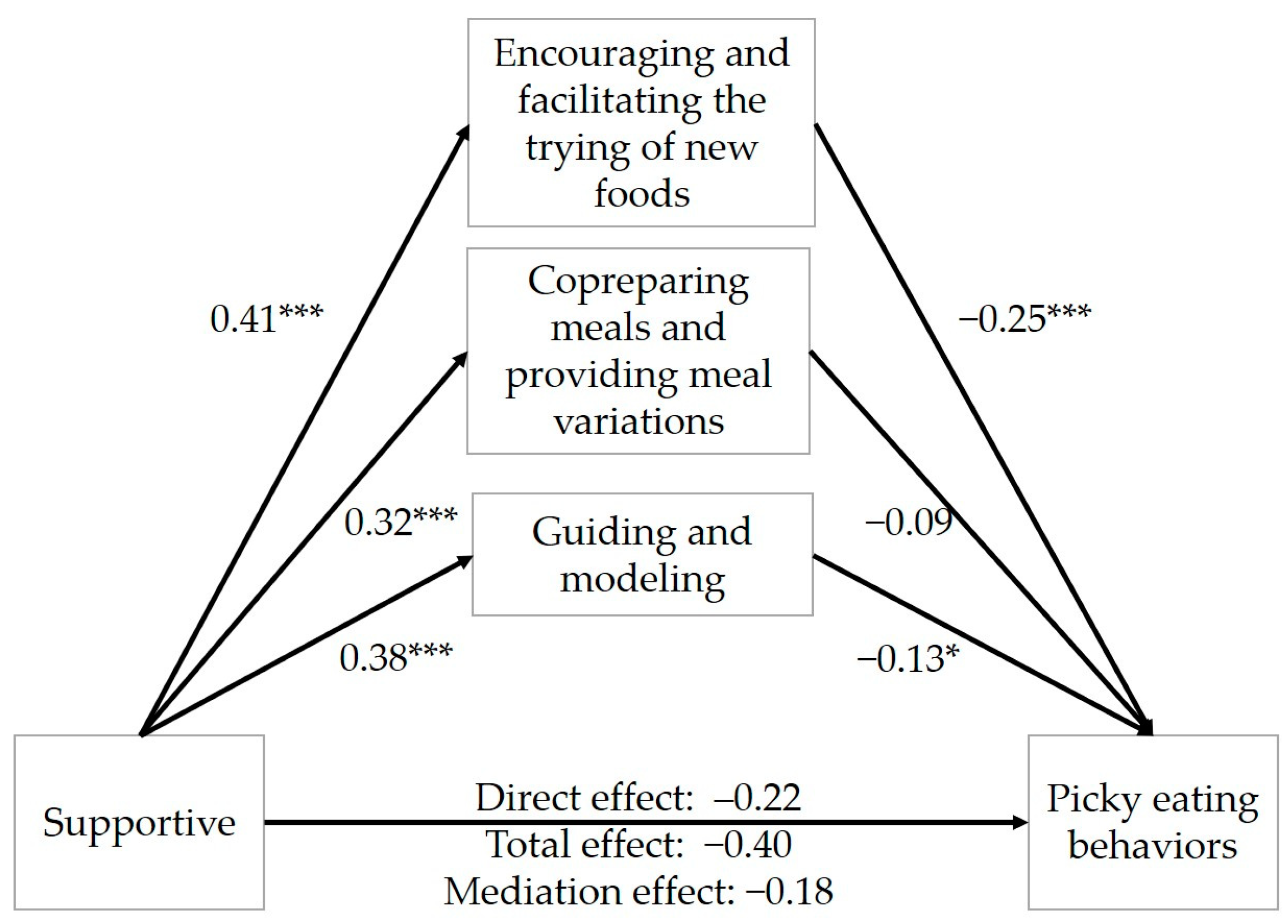
Our study explored the complex interplay between dietary coparenting, parenting strategies, and picky eating behaviors, highlighting the significant diminishing role of supportive coparenting in being associated with lower picky eating behaviors among young children. Our analysis revealed a negative association of supportive coparenting with picky eating behaviors and identified two key parenting strategies—encouraging and facilitating the trying of new foods and guiding and modeling—as significant mediators. The indirect effects of these strategies explained 45.0% (supportive) and 40.0% (undermining) of the total effect on the association between dietary coparenting, parenting strategies, and picky eating behaviors in children. One study reported that supportive coparenting did not lead to controlling feeding practices. By contrast, undermining coparenting was linked to using food for emotional regulation, offering food as a reward, and implementing weight-related restrictions but not to pressured eating or health-based dietary restrictions [
43]. In addition, our results revealed that undermining coparenting was associated with more frequent picky eating behaviors, with its influence mediated by effective parenting strategies, further emphasizing the complexity of parental influence on children’s dietary practices. Our study stands out for its simultaneous exploration of the relations among dietary coparenting, parenting strategies, and young children’s picky eating behaviors, offering novel insights into the nuanced interplay between parenting partnership, parenting, and children’s eating behaviors in the family context within a culture.
Cross-sectional designs in this study may limit causal inferences, so it is suggested that future studies could conduct longitudinal designs. We invited parents from 14 preschools across different districts, offered appropriate incentives, and ensured the participants remained anonymous. However, the recruitment approach may have caused self-selection bias. Our research highlights the need to address sample limitations and calls for future research to include a broader range of participants, encompassing paired fathers and mothers, other caregivers (e.g., grandparents), and also single-parent families, to understand the full spectrum of dietary coparenting and parenting strategies. Investigating the interactions among various caregivers and the effects of supportive coparenting, as well as effective parenting strategies, offers deeper insights into children’s picky eating behaviors. Moreover, exploring the beliefs and motivations underlying parents’ choice of strategies and the impact of the strategies on children’s eating behaviors across potential genetic predispositions and cultural and socioeconomic backgrounds would enhance our understanding of the nurture and nature factors influencing picky eating. Furthermore, exploring more strategies for dealing with pickiness may help in developing a well-established scale. Such a comprehensive approach would not only improve the generalizability of findings but also contribute to the development of tailored guidance and educational programs that foster positive dietary coparenting, parenting strategies, and picky eating behaviors in children.






{kind=link}
{kind=link}