Gestational Vitamin 25(OH)D Status as a Risk Factor for Receptive Language Development: A 24-Month, Longitudinal, Observational Study

Abstract
:1. Introduction
2. Materials and Methods
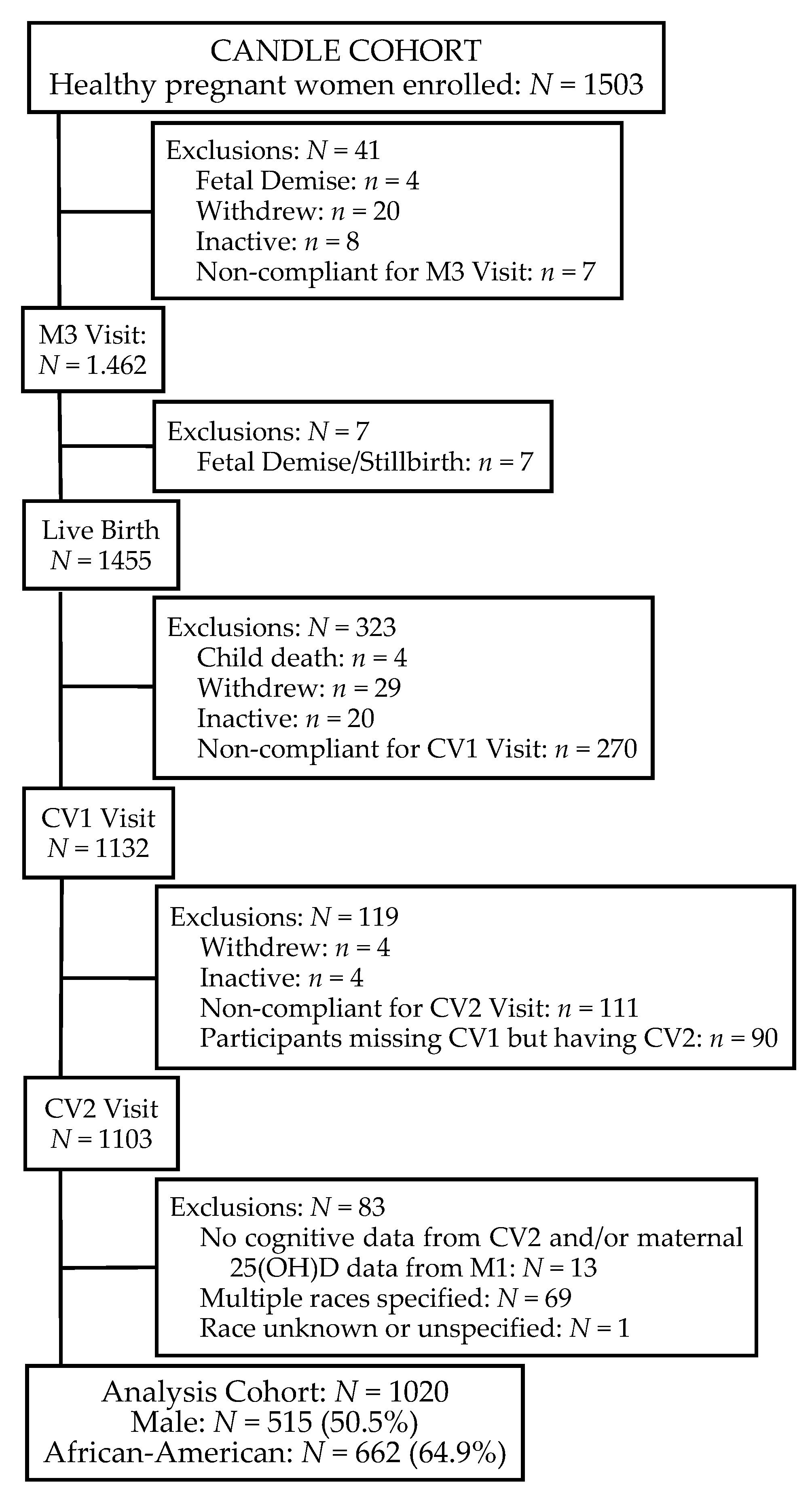
2.1. Study Population

2.2. Maternal Measures
2.3. Child Measures
2.4. Vitamin 25(OH)D Measurement
2.5. Data Analysis
3. Results
3.1. Description of the Study Participants

{kind=link}
| n | % | |
|---|---|---|
| Insurance | ||
| Other Insurance | 489 | 47.9 |
| Medicaid, Medicare | 531 | 52.1 |
| Education | ||
| HS diploma or lower | 567 | 55.6 |
| College or higher degree | 453 | 44.4 |
| Marital Status | ||
| Cohabitation | 601 | 58.9 |
| Single | 419 | 41.1 |
| Pre-Pregnancy BMI, kg/m2 | ||
| Underweight | 45 | 4.4 |
| Normal | 397 | 38.9 |
| Overweight | 240 | 23.5 |
| Obese | 338 | 33.1 |
| Alcohol Use, Yes | 86 | 8.4 |
| Tobacco Use, Yes | 85 | 8.3 |
| Total Pregnancies 1 | ||
| 1 | 309 | 30.3 |
| 2–5 | 594 | 58.2 |
| >5 | 117 | 11.5 |
| Gestational 25(OH)D | ||
| <20 ng/dL | 425 | 41.7 |
| 20.00–29.99 ng/dL | 440 | 43.1 |
| ≥30 ng/dL | 155 | 15.2 |
| Mean | SD | |
| Weeks of Gestation | 38.9 | 1.7 |
| 25(OH)D, ng/dL | 22.3 | 8.5 |
| Maternal Age, years | 26.6 | 5.5 |
| Maternal Total IQ | 96.2 | 16.4 |
| Birth Weight, Z-score | 0.05 | 0.95 |
| Birth Length, Z-score | 0.53 | 1.28 |
| Head Circumference, Z-score | −0.03 | 1.34 |
| Child Age at CV2 Assessment, months | 25.0 | 1.5 |
| Cognitive Scaled Score 2 | 9.6 | 2.6 |
| Receptive Language Scaled Score 2 | 9.5 | 2.9 |
| Expressive Language Scaled Score 2 | 9.9 | 2.7 |
3.2. Associations between Select Characteristics and Cognitive and Language Scaled Scores
| Cognitive | Receptive Language | Expressive Language | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | p 1 | Mean | SD | p 1 | Mean | SD | p 1 | |
| Race | <0.0001 | <0.0001 | <0.0001 | ||||||
| African-American | 8.8 | 2.2 | 8.6 | 2.3 | 9.3 | 2.3 | |||
| European-American | 11.0 | 2.7 | 11.1 | 3.1 | 11.0 | 3.1 | |||
| Insurance | <0.0001 | <0.0001 | <0.0001 | ||||||
| Other Insurance | 10.4 | 2.8 | 10.5 | 3.1 | 10.7 | 3.0 | |||
| Medicaid, Medicare | 8.8 | 2.1 | 8.6 | 2.3 | 9.2 | 2.2 | |||
| Education | <0.0001 | <0.0001 | <0.0001 | ||||||
| HS diploma or lower | 8.9 | 2.1 | 8.7 | 2.4 | 9.3 | 2.2 | |||
| College or higher degree | 10.4 | 2.8 | 10.5 | 3.1 | 10.7 | 3.0 | |||
| Marital Status | <0.0001 | <0.0001 | <0.0001 | ||||||
| Cohabitation | 10.1 | 2.7 | 10.1 | 3.0 | 10.3 | 2.9 | |||
| Single | 8.8 | 2.2 | 8.6 | 2.3 | 9.3 | 2.3 | |||
| Pre-Pregnancy BMI, kg/m2 | 0.0001 | 0.0001 | 0.0001 | ||||||
| Under weight | 9.7 | 2.2 | 9.9 | 2.9 | 9.9 | 2.6 | |||
| Normal | 9.9 | 2.7 | 9.9 | 3.1 | 10.4 | 2.9 | |||
| Overweight | 9.5 | 2.3 | 9.4 | 2.7 | 10.0 | 2.6 | |||
| Obese | 9.2 | 2.6 | 9.0 | 2.7 | 9.4 | 2.4 | |||
| Alcohol Use | 0.0024 | 0.002 | 0.007 | ||||||
| No | 9.5 | 2.5 | 9.4 | 2.8 | 9.8 | 2.6 | |||
| Yes | 10.3 | 3.0 | 10.7 | 3.6 | 10.6 | 3.1 | |||
| Tobacco Use | <0.0006 | <0.0006 | <0.0006 | ||||||
| No | 9.6 | 2.6 | 9.6 | 2.9 | 10.0 | 2.7 | |||
| Yes | 8.7 | 2.0 | 8.5 | 2.7 | 8.8 | 2.6 | |||
| Total Pregnancies | 0.0006 | 0.029 | 0.0028 | ||||||
| 1 | 10.0 | 2.9 | 9.8 | 3.0 | 10.3 | 2.7 | |||
| 2–5 | 9.5 | 2.4 | 9.5 | 2.9 | 9.8 | 2.8 | |||
| >5 | 8.8 | 2.2 | 8.8 | 2.3 | 9.4 | 2.2 | |||
| Gestational Diabetes | 0.10 | 0.22 | 0.14 | ||||||
| Missing | 8.3 | 2.1 | 9.7 | 2.5 | 9.7 | 1.2 | |||
| No | 9.5 | 2.6 | 9.5 | 2.9 | 9.9 | 2.7 | |||
| Yes | 10.0 | 2.6 | 9.9 | 3.0 | 10.3 | 2.9 | |||
| Pre-eclampsia | 0.067 | 0.023 | 0.19 | ||||||
| Missing | 9.0 | 2.2 | 9.6 | 2.5 | 9.8 | 1.6 | |||
| No | 9.6 | 2.6 | 9.6 | 2.9 | 10.0 | 2.7 | |||
| Yes | 9.1 | 2.2 | 8.8 | 2.4 | 9.5 | 2.6 | |||
| Delivery | 0.0021 | 0.102 | 0.024 | ||||||
| Pre-Term | 8.8 | 2.2 | 8.9 | 2.9 | 9.3 | 2.8 | |||
| Full Term | 9.6 | 2.6 | 9.5 | 2.9 | 10.0 | 2.7 | |||
| Gestational 25(OH)D | <0.0001 | <0.0001 | <0.0001 | ||||||
| <20 ng/dL | 9.1 | 2.4 | 8.9 | 2.5 | 9.4 | 2.4 | |||
| 20.00–29.99 ng/dL | 9.8 | 2.8 | 9.7 | 3.0 | 10.2 | 2.9 | |||
| ≥30 ng/dL | 10.1 | 2.4 | 10.5 | 3.2 | 10.4 | 2.6 | |||
3.3. Modeling of Gestational 25(OH)D with Cognitive and Language Assessments at Age 2
| Scaled Score n = 1020 | Unadjusted Estimate | Unadjusted p | Adjusted Estimate | SE | Adjusted R2 | Adjusted p |
|---|---|---|---|---|---|---|
| Cognitive | 0.51 | <0.001 | 0.07 2 | 0.01 | 0.23 | 0.45 |
| Receptive Language | 0.71 | <0.001 | 0.24 3 | 0.10 | 0.21 | 0.017 |
| Expressive Language | 0.45 | <0.001 | 0.12 4 | 0.09 | 0.13 | 0.22 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
References
- Bryan, J.; Osendarp, S.; Hughes, D.; Calvaresi, E.; Baghurst, K.; van Klinken, J.W. Nutrients for cognitive development in school-aged children. Nutr. Rev. 2004, 62, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Bourre, J.M. Effects of nutrients (in food) on the structure and function of the nervous system: Update on dietary requirements for brain. Part 1: Micronutrients. J. Nutr. Health Aging 2006, 10, 377–385. [Google Scholar] [PubMed]
- Lozoff, B.; Smith, J.B.; Kaciroti, N.; Clark, K.M.; Guevara, S.; Jimenez, E. Functional significance of early-life iron deficiency: Outcomes at 25 years. J. Pediatr. 2013, 163, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Palfrey, J.S.; Hauser-Cram, P.; Bronson, M.B.; Warfield, M.E.; Sirin, S.; Chan, E. The Brookline Early Education Project: A 25-year follow-up study of a family-centered early health and development intervention. Pediatrics 2005, 116, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.J.; Temple, J.A.; Ou, S.R.; Robertson, D.L.; Mersky, J.P.; Topitzes, J.W.; Niles, M.D. Effects of a school-based, early childhood intervention on adult health and well-being: A 19-year follow-up of low-income families. Arch. Pediatr. Adolesc. Med. 2007, 161, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Sniadecki, J. Dziela; Warszawa, Poland, 1840; Volume 1, pp. 273–274. (In Polish) [Google Scholar]
- Holick, M.F. Environmental factors that influence the cutaneous production of vitamin D1–3. Am. J. Clin. Nutr. 1995, 61, 638S–645S. [Google Scholar] [PubMed]
- Brannon, P.M. Vitamin D and adverse pregnancy outcomes: Beyond bone health and growth. Proc. Nutr. Soc. 2012, 71, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; Demay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The nonskeletal effects of vitamin D: An Endocrine Society scientific statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Bioavailability of vitamin D and its metabolites in black and white adults. N. Engl. J. Med. 2013, 369, 2047–2048. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Evidence-based D-bate on health benefits of vitamin D revisited. Derm.-Endocrinol. 2012, 4, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Kritchevsky, S.B.; Tooze, J.A.; Neiberg, R.H.; Schwartz, G.G.; Hausman, D.B.; Johnson, M.A.; Bauer, D.C.; Cauley, J.A.; Shea, M.K.; Cawthon, P.M.; et al. 25-Hydroxyvitamin D, parathyroid hormone, and mortality in black and white older adults: The health ABC study. J. Clin. Endocrinol. Metab. 2012, 97, 4156–4165. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.S.; Choi, M.Y.; Longtine, M.S.; Nelson, D.M. Vitamin D effects on pregnancy and the placenta. Placenta 2010, 31, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Whitehouse, A.J.O.; Holt, B.J.; Serralha, M.; Holt, P.G.; Kusel, M.M.H.; Hart, P.H. Maternal serum vitamin D levels during pregnancy and offspring neurocognitive development. Pediatrics 2012, 129, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Weinert, L.S.; Silveiro, S.P. Maternal-fetal impact of vitamin D deficiency: A critical review. Mater. Child Health J. 2015, 19, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.; Guxens, M.; Llop, S.; Rodríguez-Bernal, C.L.; Tardón, A.; Riaño, I.; Ibarluzea, J.; Lertxundi, N.; Espada, M.; Rodriguez, A.; et al. Circulating 25-hydroxyvitamin D3 in pregnancy and infant neuropsychological development. Pediatrics 2012, 130, e913–e920. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, M.L.; Felton, S.K.; Riek, A.E.; Bernal-Mizrachi, C. Implications of vitamin D deficiency in pregnancy and lactation. Am. J. Obstet. Gynecol. 2010, 202, 429.e1–429.e9. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. The role of vitamin D in pregnancy and lactation: Insights from animal models and clinical studies. Annu. Rev. Nutr. 2012, 32, 97–123. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Simhan, H.N. Vitamin D may be a link to black-white disparities in adverse birth outcomes. Obstet. Gynecol. Surv. 2010, 65, 273–284. [Google Scholar] [CrossRef] [PubMed]
- West, A.K.; Leung, J.Y.; Chung, R.S. Neuroprotection and regeneration by extracellular metallothionein via lipoprotein-receptor-related proteins. J. Biol. Inorg. Chem. 2011, 16, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.; Bell, N.H.; Shary, J.; Shaw, S.; Greene, A.; Oexmann, M.J. Evidence that obesity does not influence the vitamin D-endocrine system in blacks. J. Bone Miner. Res. 1986, 1, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Sowers, M.; Bell, C. Serum 25-hydroxyvitamin D, diabetes, and ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes Care 2004, 27, 2813–2818. [Google Scholar] [CrossRef] [PubMed]
- Cosman, F.; Nieves, J.; Dempster, D.; Lindsay, R. Vitamin D economy in blacks. J. Bone Miner. Res. 2007, 22, V34–V38. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, L.M.; Greene, R.A.; Kearney, P.M. The effect of moderate gestational alcohol consumption during pregnancy on speech and language outcomes in children: A systematic review. Syst. Rev. 2014, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Irner, T.B.; Teasdale, T.W.; Olofsson, M. Cognitive and social development in preschool children born to women using substances. J. Addict. Dis. 2012, 31, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Maccani, J.Z.; Koestler, D.C.; Houseman, E.A.; Marsit, C.J.; Kelsey, K.T. Placental DNA methylation alterations associated with maternal tobacco smoking at the RUNX3 gene are also associated with gestational age. Epigenomics 2013, 5, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Palmer, F.B.; Anand, K.J.; Graff, J.C.; Murphy, L.E.; Qu, Y.; Völgyi, E.; Rovnaghi, C.R.; Moore, A.; Tran, Q.T.; Tylavsky, F.A. Early adversity, socioemotional development, and stress in urban 1-year-old children. J. Pediatr. 2013, 163, 1733–1739. [Google Scholar] [CrossRef] [PubMed]
- Anthopolos, R.; Edwards, S.E.; Miranda, M.L. Effects of maternal prenatal smoking and birth outcomes extending into the normal range on academic performance in fourth grade in North Carolina, USA. Paediatr. Perinat. Epidemiol. 2013, 27, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, G.; van Eijsden, M.; Vrijkotte, T.G.; Gemke, R.J. Educational inequalities in perinatal outcomes: The mediating effect of smoking and environmental tobacco exposure. PLoS ONE 2012, 7, e37002. [Google Scholar] [CrossRef] [PubMed]
- Völgyi, E.; Carroll, K.N.; Hare, M.E.; Ringwald-Smith, K.; Piyathilake, C.; Yoo, W.; Tylavsky, F.A. Dietary patterns in pregnancy and effects on nutrient intake in the Mid-South: The Conditions Affecting Neurocognitive Development and Learning in Early Childhood (CANDLE) Study. Nutrients 2013, 5, 1511–1530. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, B.N. Validity of the Wechsler Abbreviated Scale of Intelligence and other very short forms of estimating intellectual functioning. Assessment 2002, 9, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Willet, W. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- National Health and Nutrition Examination Survey. 1999–2014 Survey Content Brochure; National Center for Health Statistics: Hyattsville, MD, USA, 2014.
- Bayley, N. Bayley Scales of Infant and Toddler Development®, 3rd ed.; Harcourt Assessment, Inc.: San Antonio, TX, USA, 2006. [Google Scholar]
- Antoniucci, D.M.; Black, D.M.; Sellmeyer, D.E. Serum 25-hydroxyvitamin D is unaffected by multiple freeze-thaw cycles. Clin. Chem. 2005, 51, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Lissner, D.; Mason, R.S.; Posen, S. Stability of vitamin D metabolites in human blood serum and plasma. Clin. Chem. 1981, 27, 773–774. [Google Scholar] [PubMed]
- Wagner, C.L.; Taylor, S.N.; Dawodu, A.; Johnson, D.D.; Hollis, B.W. Vitamin D and its role during pregnancy in attaining optimal health of mother and fetus. Nutrients 2012, 4, 208–230. [Google Scholar] [CrossRef] [PubMed]
- Colón-Ramos, U.; Racette, S.B.; Ganiban, J.; Nguyen, T.G.; Kocak, M.; Carroll, K.N.; Völgyi, E.; Tylavsky, F.A. Association between dietary patterns during pregnancy and birth size measures in a diverse population in Southern US. Nutrients 2015, 7, 1318–1332. [Google Scholar] [CrossRef] [PubMed]
- Hawes, J.E.; Tesic, D.; Whitehouse, A.J.; Zosky, G.R.; Smith, J.T.; Wyrwoll, C.S. Maternal vitamin D deficiency alters fetal brain development in the BALC/c mouse. Behav. Brain Res. 2015, 286, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.; Burne, T.; McGrath, J. Vitamin D in fetal brain development. Semin. Cell Dev. Biol. 2011, 22, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Strøm, M.; Halldorsson, T.I.; Hansen, S.; Granström, C.; Maslova, E.; Petersen, S.B.; Cohen, A.S.; Olsen, S.F. Vitamin D measured in maternal serum and offspring neurodevelopmental outcomes: A prospective study with long-term follow-up. Ann. Nutr. Metab. 2014, 64, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Keim, S.A.; Bodnar, L.M.; Klebanoff, M.A. Maternal and cord blood 25(OH)-vitamin D concentrations in relation to child development and behaviour. Paediatr. Perinat. Epidemiol. 2014, 28, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Zhu, P.; Tong, S.-L.; Hao, J.-H.; Tao, R.-X.; Huang, K.; Hu, W.-B.; Zhou, Q.-F.; Jiang, X.-M.; Tao, F.-B. Cord blood vitamin D and neurocognitive development are nonlinearly related in toddlers. J. Nutr. 2015, 145, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Gould, E. Childhood lead poisoning: Conservative estimates of the social and economic benefits of lead hazard control. Environ. Health Perspect. 2009, 117, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Bourre, J.M. Effects of nutrients (in food) on the structure and function of the nervous system: Update on dietary requirements for brain. Part 2: Macronutrients. J. Nutr. Health Aging 2006, 10, 386–399. [Google Scholar] [PubMed]
- Grantham-McGregor, S.; Cheung, Y.B.; Cueto, S.; Glewwe, P.; Richter, L.; Strupp, B. International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef]
- Moore, E.C.J. Family socialization and the IQ test performance of traditionally and trans-racially adopted Black children. Dev. Psychol. 1986, 22, 317–326. [Google Scholar] [CrossRef]
- Fernald, A.; Marchman, V.A.; Weisleder, A. SES differences in language processing skill and vocabulary are evident at 18 months. Dev. Sci. 2013, 16, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Gottfredson, L.S. What if the hereditarian hypothesis is true? Psychol. Public Policy Law 2005, 11, 311–319. [Google Scholar] [CrossRef]
- Lynn, R.; Vanhanen, T. IQ and the Wealth of Nations; Praeger/Greenwood: Westport, CT, USA, 2002. [Google Scholar]
- Nisbett, R.E.; Aronson, J.; Blair, C.; Dickens, W.; Flynn, J.; Halpern, D.F.; Turkheimer, E. Intelligence: New findings and theoretical developments. Am. Psychol. 2012, 67, 130–159. [Google Scholar] [CrossRef] [PubMed]
- Rushton, J.P.; Jensen, A.R. Thirty years of race differences in cognitive ability. Psychol. Public Policy Law 2005, 11, 235–294. [Google Scholar] [CrossRef]
- Rushton, J.P.; Jensen, A.R. Wanted: More race realism, less moralistic fallacy. Psychol. Public Policy Law 2005, 11, 328–336. [Google Scholar] [CrossRef]
- Dickens, W.T.; Flynn, J.R. Black Americans reduce the racial IQ gap: Evidence from standardized samples. Psychol. Sci. 2006, 7, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Nisbett, R.E. Heredity, environment, and race differences in IQ: A commentary on Rushton and Jensen. Psychol. Public Policy Law 2005, 11, 235–294. [Google Scholar] [CrossRef]
- Nisbett, R.E. Intelligence and How to Get It: Why Schools and Cultures Count; W.W. Norton & Co.: New York, NY, USA, 2009. [Google Scholar]
- Mozhui, K.; Smith, A.K.; Tylavsky, F.A. Ancestry dependent DNA methylation and influence of maternal nutrition. PLoS ONE 2015, 10, e0118466. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tylavsky, F.A.; Kocak, M.; Murphy, L.E.; Graff, J.C.; Palmer, F.B.; Völgyi, E.; Diaz-Thomas, A.M.; Ferry, R.J. Gestational Vitamin 25(OH)D Status as a Risk Factor for Receptive Language Development: A 24-Month, Longitudinal, Observational Study. Nutrients 2015, 7, 9918-9930. https://doi.org/10.3390/nu7125499
Tylavsky FA, Kocak M, Murphy LE, Graff JC, Palmer FB, Völgyi E, Diaz-Thomas AM, Ferry RJ. Gestational Vitamin 25(OH)D Status as a Risk Factor for Receptive Language Development: A 24-Month, Longitudinal, Observational Study. Nutrients. 2015; 7(12):9918-9930. https://doi.org/10.3390/nu7125499
Chicago/Turabian StyleTylavsky, Frances A., Mehmet Kocak, Laura E. Murphy, J. Carolyn Graff, Frederick B. Palmer, Eszter Völgyi, Alicia M. Diaz-Thomas, and Robert J. Ferry. 2015. "Gestational Vitamin 25(OH)D Status as a Risk Factor for Receptive Language Development: A 24-Month, Longitudinal, Observational Study" Nutrients 7, no. 12: 9918-9930. https://doi.org/10.3390/nu7125499
APA StyleTylavsky, F. A., Kocak, M., Murphy, L. E., Graff, J. C., Palmer, F. B., Völgyi, E., Diaz-Thomas, A. M., & Ferry, R. J. (2015). Gestational Vitamin 25(OH)D Status as a Risk Factor for Receptive Language Development: A 24-Month, Longitudinal, Observational Study. Nutrients, 7(12), 9918-9930. https://doi.org/10.3390/nu7125499