Non-Celiac Gluten Sensitivity Has Narrowed the Spectrum of Irritable Bowel Syndrome: A Double-Blind Randomized Placebo-Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
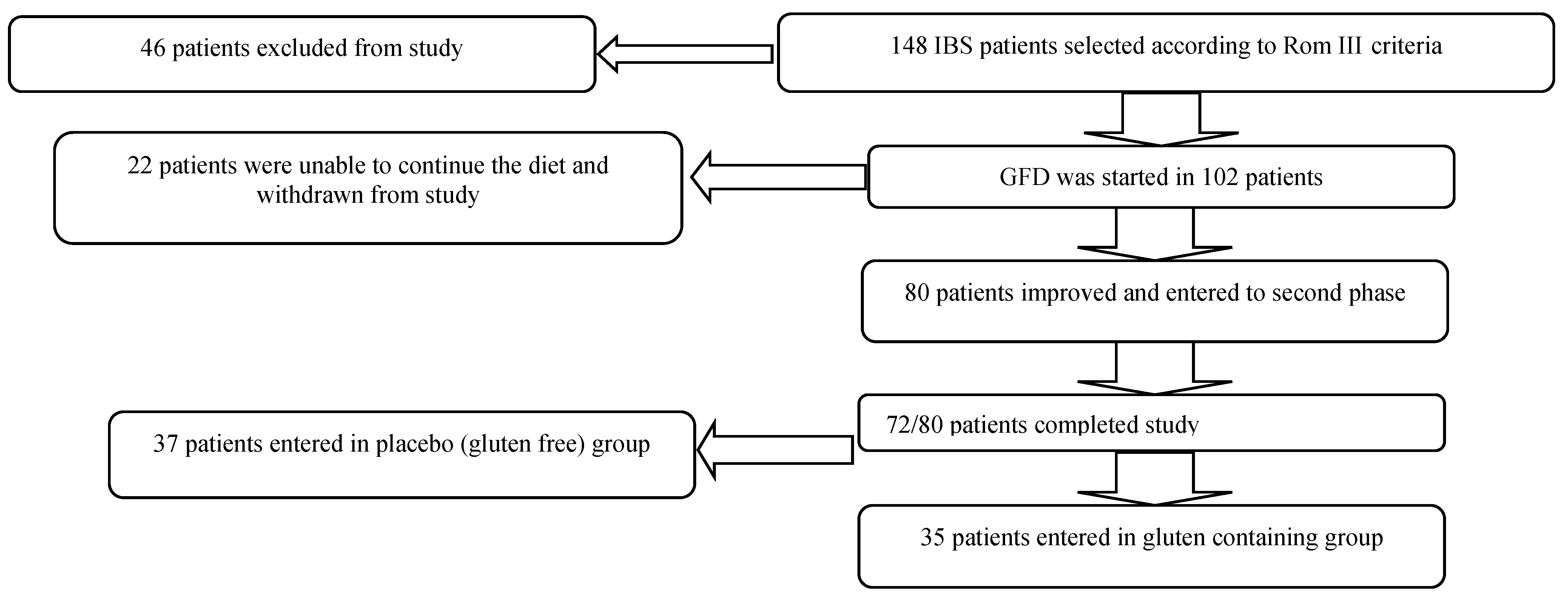
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
2.3. Clinical Trial
2.4. Assessment of Dietary Compliance

2.5. Statistical Analysis
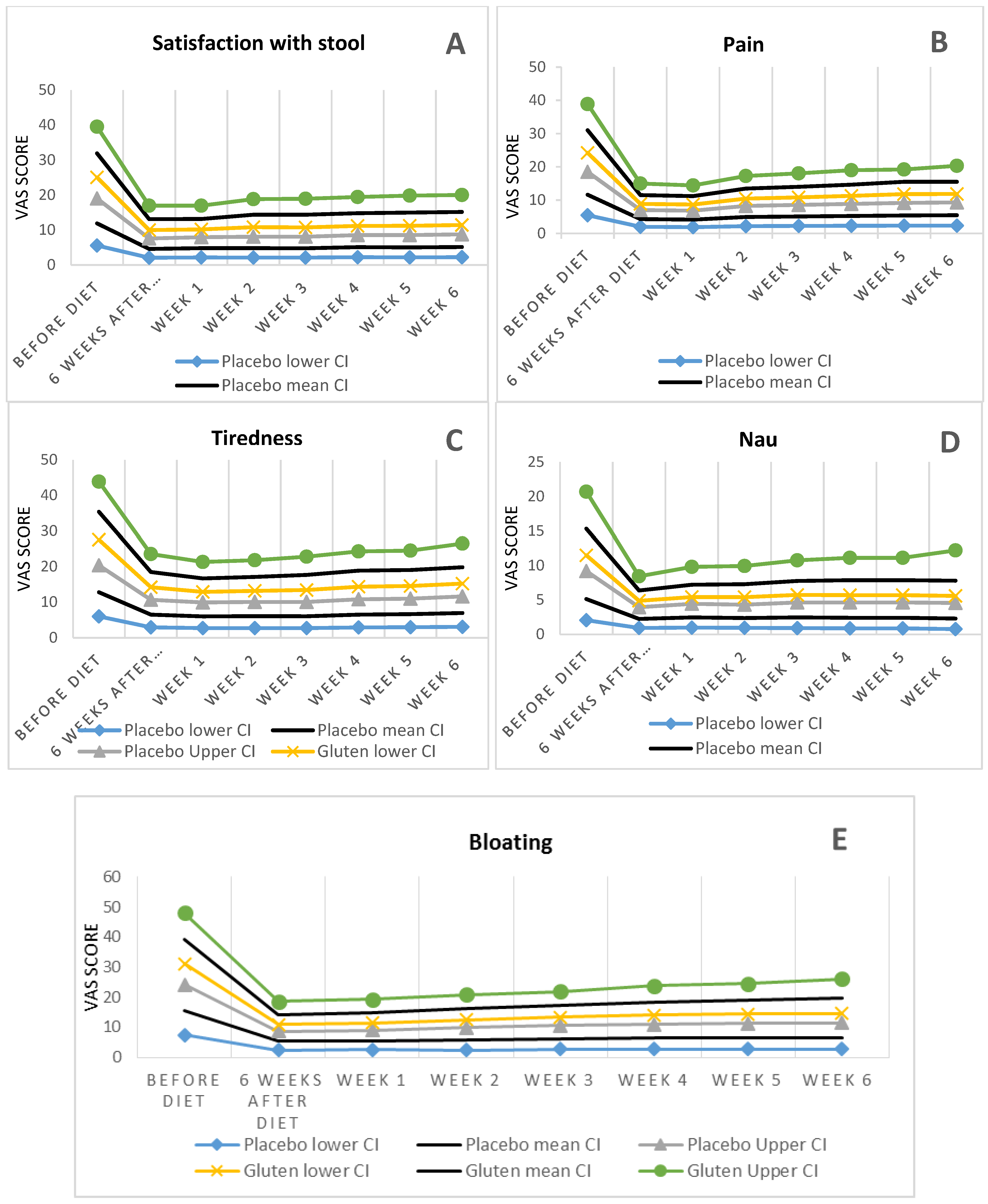
3. Results


{kind=link}
{kind=link}
{kind=link}
| Antibody | Placebo | 95% CI * | Gluten | 95% CI | p Value |
|---|---|---|---|---|---|
| Number of patients | 37 | 35 | -- | ||
| Age average | 43.2 ± 17 | 37.6–8.8 | 44.5 ± 10 | 41.11–47.89 | 0.241 |
| Frequency (%) of male gender | 13 (35.1%) | 19%–51% | 6 (17.1%) | 4%–30% | 0.083 |
| Kind of IBS | 0.089 | ||||
| Constipation | 6 (16.2%) [4%–28%] | 10 (28.6%) [13%–43%] | |||
| Diarrhea | 18 (48.6%) [32.6%–64.6%] | 19 (54.3%) [37%–71%] | |||
| Mixed | 13 (35.1%) [20%–50%] | 6 (17.1%) [5%–29%] | |||
| Tiredness | (8.8%) | (60%) | |||
| Pain | (16.2%) | (76.3%) | |||
| 1 Anti-tTG IgA | 2.3 ± 0.4 | 2.17–2.43 | 2.5 ± 0.4 | 2.37–2.63 | 0.259 |
| Anti-tTG IgG | 2 ± 0.3 | 1.02–2.98 | 2.2 ± 0.3 | 2.1–2.3 | 0.174 |
| 2 AGA IgA | 2.9 ± 1.8 | 2.31–3.49 | 2.6 ± 0.5 | 2.43–2.77 | 0.110 |
| AGA IgG | 2.6 ± 1.4 | 2.14–3.06 | 2.4 ± 0.4 | 2.27–2.53 | 0.119 |
| Positive DQ2/8 3 HLA | 23 (62.1%) | 46%–78% | 17 (48.5%) | 31%–65% | 0.792 |
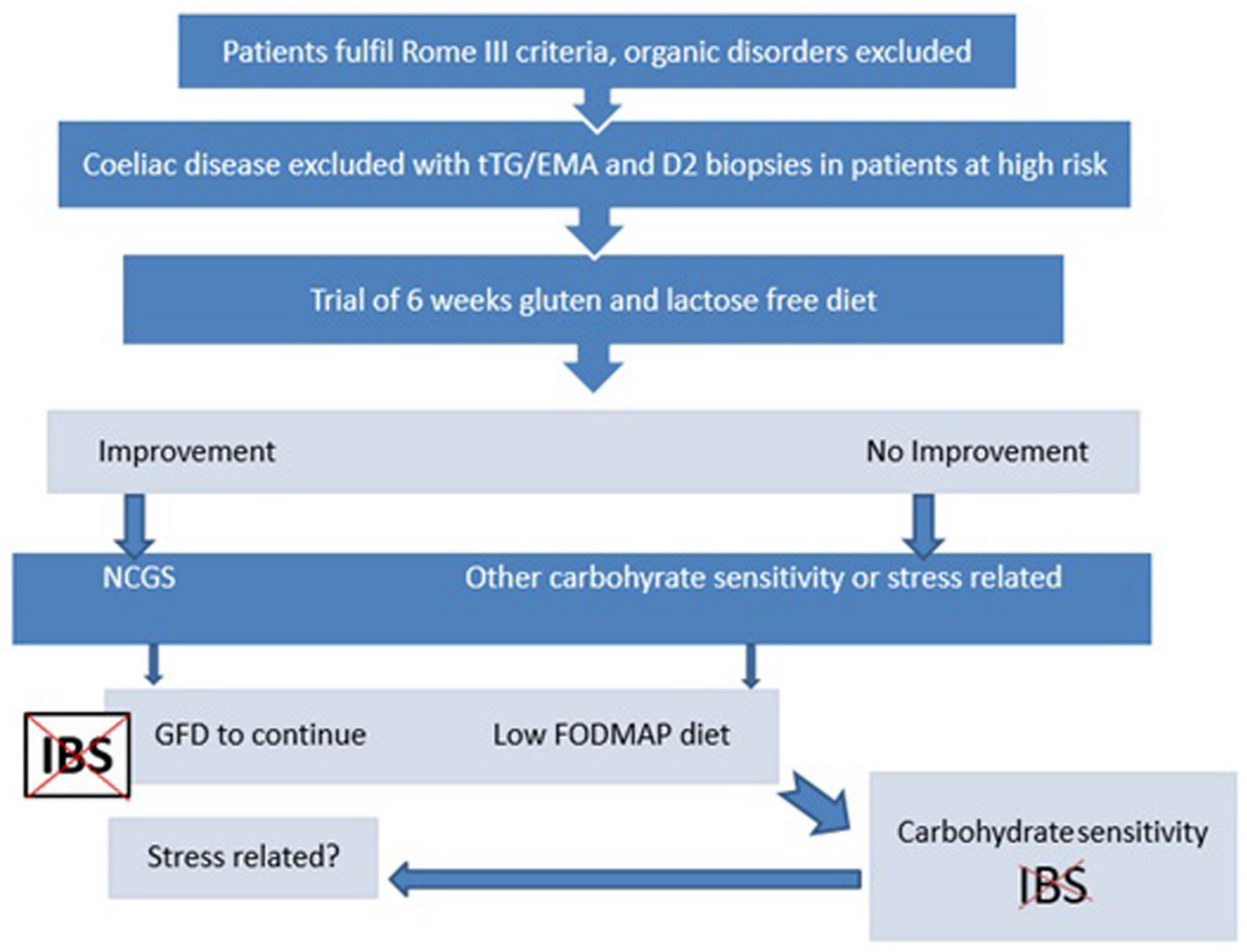
4. Discussion
5. Conclusions

Author Contributions
Conflicts of Interest
References
- Thompson, W.G.; Heaton, K.W.; Smyth, G.T.; Smyth, C. Irritable bowel syndrome in general practice: Prevalence, characteristics, and referral. Gut 2000, 46, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.F.; Salih, S.Y.; Read, A.E. Organic and functional disorders in 2000 gastroenterology outpatients. Lancet 1983, 1, 632–634. [Google Scholar] [CrossRef]
- Rostami, K.; Rostami-Nejad, M.; Al Dulaimi, D. Post Gastroenteritis gluten intolerance. Gastroenterol. Hepatol. Bed Bench 2015, 8, 66–70. [Google Scholar] [PubMed]
- Gibson, P.R. Food intolerance in functional bowel disorders. J. Gastroenterol. Hepatol. 2011, 26, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.A.; Locke, G.R.; Talley, N.J.; Zinsmeister, A.R.; Fett, S.L.; Melton, L.J., 3rd. A comparison of the Rome and Manning criteria for case identification in epidemiological investigations of irritable bowel syndrome. Am. J. Gastroenterol. 2000, 95, 2816–2824. [Google Scholar] [CrossRef] [PubMed]
- Ruepert, L.; Quartero, A.O.; de Wit, N.J.; van der Heijden, G.J.; Rubin, G.; Muris, J.W. Bulking agents, antispasmodics and antidepressants for the treatment of irritable bowel syndrome. Cochrane Database Syst. Rev. 2011, 8. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Am. J. Gastroenterol. 2011, 106, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; Tovoli, F.; Cicola, R.; Parisi, C.; Fabbri, A.; Piscaglia, M.; Fiorini, E.; Caio, G. Serological tests in gluten sensitivity (nonceliac gluten intolerance). J. Clin. Gastroenterol. 2012, 46, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Spencer, M.; Chey, W.D.; Eswaran, S. Dietary renaissance in IBS: Has food replaced medications as a primary treatment strategy? Curr. Treat. Options Gastroenterol. 2014, 12, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef] [PubMed]
- Troncone, R.; Jabri, B. Celiac disease and gluten-sensitivity. J. Intern. Med. 2011, 269, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Sapone, A.; Bai, J.C.; Ciacci, C.; Dolinsek, J.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Rostami, K.; Sanders, D.S.; Schumann, M.; et al. Spectrum of gluten-related disorders: Consensus on new nomenclature and classification. BMC Med. 2012, 10. [Google Scholar] [CrossRef] [PubMed]
- Verdu, E.F.; Armstrong, D.; Murray, J.A. Between celiac disease and irritable bowel syndrome: The “no man’s land” of gluten sensitivity. Am. J. Gastroenterol. 2009, 104, 1587–1594. [Google Scholar] [CrossRef] [PubMed]
- Verdu, E.F.; Huang, X.; Natividad, J.; Lu, J.; Blennerhassett, P.A.; David, C.S.; McKay, D.M.; Murray, J.A. Gliadin-dependent neuromuscular and epithelial secretory responses in gluten-sensitive HLA-DQ8 transgenic mice. Am. J. Physiol. Gastrointest. Liver. Physiol. 2008, 294, G217–G225. [Google Scholar] [CrossRef] [PubMed]
- Natividad, J.M.; Huang, X.; Slack, E.; Jury, J.; Sanz, Y.; David, C.; Denou, E.; Yang, P.; Murray, J.; McCoy, K.D.; et al. Host responses to intestinal microbial antigens in gluten-sensitive mice. PLoS ONE 2009, 4, e6472. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I.; Sanders, D.S. The irritable bowel syndrome-celiac disease connection. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 623–637. [Google Scholar] [CrossRef] [PubMed]
- Carroccio, A.; Mansueto, P.; Iacono, G.; Soresi, M.; D’Alcamo, A.; Cavataio, F.; Brusca, I.; Florena, A.M.; Ambrosiano, G.; Seidita, A.; et al. Non-celiac wheat sensitivity diagnosed by double-blind placebo-controlled challenge: Exploring a new clinical entity. Am. J. Gastroenterol. 2012, 107, 1898–1906. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, L.; Blanco, I.; Bobes, J.; de Serres, F.J. Effect of one year of a gluten-free diet on the clinical evolution of irritable bowel syndrome plus fibromyalgia in patients with associated lymphocytic enteritis: A case control study. Arthritis. Res. Ther. 2014, 16. [Google Scholar] [CrossRef]
- Wouters, M.M. Histamine antagonism and postinflammatory visceral hypersensitivity. Gut 2014, 63, 1836–1837. [Google Scholar] [CrossRef] [PubMed]
- Rostami, K. From microenteropathy to villous atrophy: What is treatable? Dig. Liver. Dis. 2003, 35, 758–759. [Google Scholar] [CrossRef]
- Ohman, L.; Simren, M. Pathogenesis of IBS: Role of inflammation, immunity and neuroimmune interactions. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; Stanghellini, V.; de Giorgio, R.; Cremon, C.; Cottrell, G.S.; Santini, D.; Pasquinelli, G.; Morselli-Labate, A.M.; Grady, E.F.; Bunnett, N.W.; et al. Activated mast cells in proximity to colonic nerves correlate with abdominal pain in irritable bowel syndrome. Gastroenterology 2004, 126, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Buhner, S.; Li, Q.; Berger, T.; Vignali, S.; Barbara, G.; de Giorgio, R.; Stanghellini, V.; Schemann, M. Submucous rather than myenteric neurons are activated by mucosal biopsy supernatants from irritable bowel syndrome patients. Neurogastroenterol. Motil. 2012, 24, e1134–e1572. [Google Scholar] [CrossRef] [PubMed]
- Bodinier, M.; Brossard, C.; Triballeau, S.; Morisset, M.; Guérin-Marchand, C.; Pineau, F.; de Coppet, P.; Moneret-Vautrin, D.A.; Blank, U.; Denery-Papini, S. Evaluation of an in vitro mast cell degranulation test in the context of food allergy to wheat. Int. Arch. Allergy. Immunol. 2008, 146, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Rostami, K.; Aldulaimi, D.; Holmes, G.; Johnson, M.W.; Robert, M.; Srivastava, A.; Fléjou, J.F.; Sanders, D.S.; Volta, U.; Derakhshan, M.H.; et al. Microscoppic enteritisis: Bucharest consensus. World J. Gastroenterol. 2015, 21, 2593–2604. [Google Scholar] [CrossRef] [PubMed]
- Biesiekierski, J.R.; Peters, S.L.; Newnham, E.D.; Rosella, O.; Muir, J.G.; Gibson, P.R. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology. 2013, 145, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Valerii, M.C.; Ricci, C.; Spisni, E.; di Silvestro, R.; de Fazio, L.; Cavazza, E.; Lanzini, A.; Campieri, M.; Dalpiaz, A.; Pavan, B.; et al. Responses of peripheralblood mononucleated cells from non-celiac gluten sensitive patients to variouscereal sources. Food Chem. 2015, 176, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; Magistris, L.D.; Dolinsek, J.; et al. How the diagnosis of non celiac gluten sensitivity (NCGS) should be confirmed: The Salerno experts’ criteria. Nutrients 2015. submitted. [Google Scholar]
- Sengupta, S.; Muir, J.G.; Gibson, P.R. Does butyrate protect from colorectal cancer? J. Gastroenterol. Hepatol. 2006, 21, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, H.M.; Lomer, M.C.; Anderson, J.L.; Barrett, J.S.; Muir, J.G.; Irving, P.M.; Whelan, K. Fermentable carbohydrate restriction reduces luminal bifidobacteria and gastrointestinal symptoms in patients with irritable bowel syndrome. J. Nutr. 2012, 142, 1510–1518. [Google Scholar] [CrossRef] [PubMed]
- Di Cagno, R.; de Angelis, M.; de Pasquale, I.; Ndagijimana, M.; Vernocchi, P.; Ricciuti, P.; Gagliardi, F.; Laghi, L.; Crecchio, C.; Guerzoni, M.E.; et al. Duodenal and faecal microbiota of celiac children: Molecular, phenotype andmetabolome characterization. BMC Microbiol. 2011, 11. [Google Scholar] [CrossRef] [PubMed]
- Kopecný, J.; Mrázek, J.; Fliegerová, K.; Frühauf, P.; Tucková, L. The intestinal microflora of childhood patients with indicated celiac disease. Folia Microbiol. (Praha) 2008, 53, 214–216. [Google Scholar] [CrossRef] [PubMed]
- De Sousa Moraes, L.F.; Grzeskowiak, L.M.; de Sales Teixeira, T.F.; Gouveia Peluzio Mdo, C. Intestinal microbiota and probiotics in celiac disease. Clin. Microbiol. Rev. 2014, 27, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Christophersen, C.T.; Bird, A.R.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. Diets that differ in their FODMAP content alter the colonic luminal microenvironment. Gut 2015, 64, 93–100. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shahbazkhani, B.; Sadeghi, A.; Malekzadeh, R.; Khatavi, F.; Etemadi, M.; Kalantri, E.; Rostami-Nejad, M.; Rostami, K. Non-Celiac Gluten Sensitivity Has Narrowed the Spectrum of Irritable Bowel Syndrome: A Double-Blind Randomized Placebo-Controlled Trial. Nutrients 2015, 7, 4542-4554. https://doi.org/10.3390/nu7064542
Shahbazkhani B, Sadeghi A, Malekzadeh R, Khatavi F, Etemadi M, Kalantri E, Rostami-Nejad M, Rostami K. Non-Celiac Gluten Sensitivity Has Narrowed the Spectrum of Irritable Bowel Syndrome: A Double-Blind Randomized Placebo-Controlled Trial. Nutrients. 2015; 7(6):4542-4554. https://doi.org/10.3390/nu7064542
Chicago/Turabian StyleShahbazkhani, Bijan, Amirsaeid Sadeghi, Reza Malekzadeh, Fatima Khatavi, Mehrnoosh Etemadi, Ebrahim Kalantri, Mohammad Rostami-Nejad, and Kamran Rostami. 2015. "Non-Celiac Gluten Sensitivity Has Narrowed the Spectrum of Irritable Bowel Syndrome: A Double-Blind Randomized Placebo-Controlled Trial" Nutrients 7, no. 6: 4542-4554. https://doi.org/10.3390/nu7064542
APA StyleShahbazkhani, B., Sadeghi, A., Malekzadeh, R., Khatavi, F., Etemadi, M., Kalantri, E., Rostami-Nejad, M., & Rostami, K. (2015). Non-Celiac Gluten Sensitivity Has Narrowed the Spectrum of Irritable Bowel Syndrome: A Double-Blind Randomized Placebo-Controlled Trial. Nutrients, 7(6), 4542-4554. https://doi.org/10.3390/nu7064542