Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Analysis
3. Results
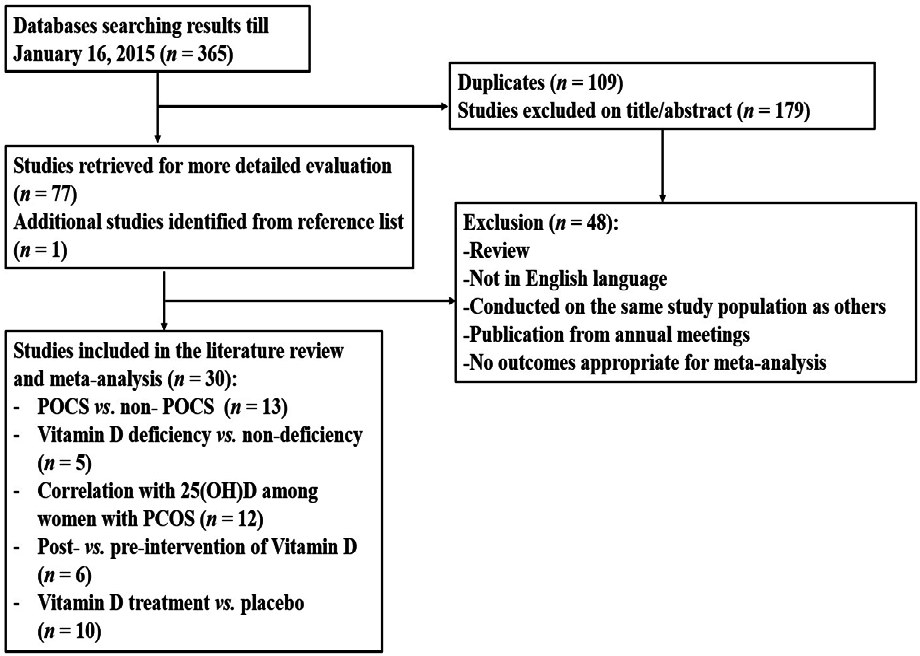
3.1. Study Selection

3.2. Characteristics of Included Studies
3.3. Differences in Vitamin D Levels between PCOS Patients and Controls
3.4. Comparison in Metabolic and Endocrine Indices in PCOS between VDD and Non-VDD Women

{kind=link}
{kind=link}
| Author (Year) | Location | Diagnosis | Participants (n) | Variables | |
|---|---|---|---|---|---|
| Comparison between PCOS Patients and Control Women | |||||
| Panidis et al., (2005) [41] | Greece | ESHRE/ASRM | PCOS,(291); healthy CTRL,(109) | 25(OH)D; 1,25(OH)2D | |
| Mahmoudi et al., (2010) [52] | Iran | NIH | PCOS, (85); CTRL, (115) | 25(OH)D; 1,25(OH)2D | |
| Li et al., (2011) [53] | UK | ESHRE/ASRM | PCOS, (25); CTRL, (27) | 25(OH)D | |
| Savastano et al., (2011) [50] | Italy | ESHRE/ASRM | PCOS, (90); Healthy CTRL, (40) | 25(OH)D | |
| Hassan et al., (2012) [48] | Egypt | ESHRE/ASRM | PCOS, (30); CTRL, (15) | 25(OH)D | |
| Lin et al., (2012) [54] | Taiwan | ESHRE/ASRM | PCOS, (188); CTRL, (143) | 25(OH)D | |
| Mazloomi et al., (2012) [55] | Iran | ESHRE/ASRM | PCOS, (103); healthy CTRL, (103) | 25(OH)D | |
| Nestler et al., (2012) [51] | USA | NIH | Obese PCOS, (8); Obese CTRL, (9) | 25(OH)D; 1,25(OH)2D | |
| Tsakova et al., (2012) [56] | Bulgaria | ESHRE/ASRM | Obese PCOS, (20); Obese CTRL, (33) | 25(OH)D | |
| El-Shal et al., (2013) [57] | Egypt | ESHRE/ASRM | PCOS, (150); CTRL, (150) | 25(OH)D | |
| Guducu et al., (2014) [58] | Turkey | ESHRE/ASRM | PCOS, (58); CTRL, (38) | 25(OH)D | |
| Ghadimi et al. (2014) [59] | Iran | ESHRE/ASRM | PCOS, (104); CTRL, (88) | 25(OH)D | |
| Sahin et al. (2014) [60] | Turkey | ESHRE/ASRM | Lean PCOS, (50); CTRL (40) | 25(OH)D | |
| Comparison between Vitamin D Deficient and Non-Deficient PCOS Patients | |||||
| Wehr et al., (2009) [22] | Austria | ESHRE/ASRM | PCOS, (206) | FG; HOMA-IR; HOMA-β; QUICKI; FI; TC; TG; HDL-C; LDL-C; CRP; TT; FT; SHBG; FAI | |
| Li et al., (2011) [53] | UK | ESHRE/ASRM | PCOS, (25) | FG; FI; HOMA-IR; HOMA-β; QUICKI; TC; HDL-C; LDL-C; TG; CRP; TT; SHBG; FAI | |
| Patra et al., (2012) [61] | India | ESHRE/ASRM | PCOS, (60) | HOMA-IR | |
| Bhattacharya et al., (2013) [62] | India | ESHRE/ASRM | PCOS, (93) | TT; SHBG; FAI; FG; FI | |
| Velija-Asimi et al., (2014) [63] | Bosnia and Herzegovina | ESHRE/ASRM | PCOS, (60) | TC; TG; CRP; FG; FI; TT; HOMA-IR; SHBG | |
| Correlation between 25(OH)D and Metabolic and Endocrine Parameters among Women with PCOS | |||||
| Hahn et al., (2006) [64] | Germany | NIH | PCOS, (120) | HOMA-IR; HOMA-β; QUICKI; TG; HDL-C; LDL-C; FG; TT;FAI; SHBG; DHEAS | |
| Wehr et al., (2009) [22] | Austria | ESHRE/ASRM | PCOS, (206) | FG; HOMA-IR; FI; TC; TG; HDL-C; LDL-C; CRP; TT; FT; SHBG; FAI | |
| Yildizhan et al., (2009) [65] | Turkey | ESHRE/ASRM | PCOS, (100) | HOMA-IR; TC; TG; TT; DHEAS; | |
| Li et al., (2011) [53] | UK | ESHRE/ASRM | PCOS, (25) | FG; FI; HOMA-IR; HOMA-β; QUICKI; TC; HDL-C; LDL-C; TG; CRP; TT; SHBG; FAI | |
| Savastano et al., (2011) [50] | Italy | ESHRE/ASRM | PCOS, (90) | HOMA-IR; FI; FAI | |
| Bonakdaran et al., (2012) [66] | Iran | ESHRE/ASRM | PCOS, (51) | DHEAS | |
| Patra et al., (2012) [61] | India | ESHRE/ASRM | PCOS, (60) | HOMA-IR; FG | |
| El-Shal et al., (2013) [57] | Egypt | ESHRE/ASRM | PCOS, (150) | TC; TG; HDL-C; LDL-C; FG; FI; HOMA-IR; HOMA-β; QUICKI; TT; FT; SHBG; DHEAS | |
| Guducu et al., (2014) [58] | Turkey | ESHRE/ASRM | PCOS, (58) | FI | |
| Kozakowski et al. (2014) [67] | Poland | ESHRE/ASRM | Obese PCOS, (60) | TC; HDL-C; LDL-C; TG; FG; FI; TT; DHEAS; FAI; SHBG | |
| Ghadimi et al. (2014) [59] | Iran | ESHRE/ASRM | PCOS, (104) | HOMA-IR | |
| Sahin et al. (2014) [60] | Turkey | ESHRE/ASRM | Lean PCOS, (50) | HOMA-IR | |
| Comparison between Post- and Pre-Intervention of Vitamin D | |||||
| Kotsa et al., (2009) [68] | Greece | ESHRE/ASRM | Obese PCOS, (15) | TC; TG; HDL-C; LDL-C | |
| Selimoglu et al., (2010) [69] | Turkey | ESHRE/ASRM | PCOS, (11) | FG; FI; HOMA-IR; 25/(OH)D; TT; FT; SHBG; DHEAS | |
| Wehr et al., (2011) [70] | Austria | ESHRE/ASRM | PCOS, (52) | FG; FI; HOMA-IR; HOMA-β; TC; TG; HDL-C; LDL-C; FT; SHBG; TT; FAI; 25(OH)D | |
| Ardabili et al., 2012 [71] | Iran | ESHRE/ASRM | PCOS and vitamin D deficiency, (50) | FG; FI; HOMA-IR; HOMA-β; QUICKI | |
| Bonakdaran et al., (2012) [66] | Iran | ESHRE/ASRM | PCOS, (51) | FG; FI; HOMA-IR; TT; DHEAS; 25(OH)D | |
| Pal et al., (2012) [72] | USA | ESHRE/ASRM | Overweight PCOS, (12) | FG; FI; QUICKI; TT; SHBG; FAI; 25(OH)D | |
| Rahimi-Ardabili et al., (2013) [73] | Iran | ESHRE/ASRM | PCOS and vitamin D deficiency, (50) | TC; TG; HDL-C; LDL-C; 25(OH)D | |
| Asemi et al. (2014) [74] | Iran | ESHRE/ASRM | Overweight or obese PCOS, (52) | 25(OH)D; FG; FI; HOMA-IR; QUICKI; TG; TC; LDL-C; HDL-C | |
| Raja-Khan et al., (2014) [75] | USA | NIH | PCOS, (28) | FG; FI; QUICKI; HOMA-IR; TC; HDL-C; LDL-C; TG; TT; FT; 25(OH)D | |
| Tehrani et al. (2014) [76] | Iran | NIH | PCOS, (40) | 25(OH)D | |
| Post-Intervention of Vitamin D Compared to Post-Intervention of Placebo | |||||
| Ardabili et al., 2012[71] | Iran | ESHRE/ASRM | PCOS and vitamin D deficiency, (50) | FG; FI; HOMA-IR; HOMA-β; QUICKI | |
| Bonakdaran et al., (2012) [66] | Iran | ESHRE/ASRM | PCOS, (51) | FG; FI; HOMA-IR; TT; DHEAS; 25(OH)D | |
| Rahimi-Ardabili et al., (2013) [73] | Iran | ESHRE/ASRM | PCOS and vitamin D deficiency, (50) | TC; TG; HDL-C; LDL-C; 25(OH)D | |
| Asemi et al. (2014) [74] | Iran | ESHRE/ASRM | Overweight or obese PCOS, (52) | 25(OH)D; FG; FI; HOMA-IR; QUICKI; TG; LDL-C; HDL-C | |
| Raja-Khan et al., (2014) [75] | USA | NIH | PCOS, (28) | FG; FI; QUICKI; HOMA-IR; TC; HDL-C; LDL-C; TG; TT; FT; 25(OH)D | |
| Tehrani et al. (2014) [76] | Iran | NIH | PCOS, (40) | 25(OH)D | |

3.5. Correlation of 25(OH)D with Metabolic and/or Endocrine Parameters
3.6. Comparison between Post- and Pre-Intervention of Vitamin D Supplementation
3.7. Post-Intervention of Vitamin D Compared to Post-Intervention of Placebo
| Outcome | No. of Studies | No. of Observations | SMD (95%CI) ‡ | Heterogeneity Test | Publication Bias | |
|---|---|---|---|---|---|---|
| p-Value | I2 (%) | p-Value | ||||
| Comparison between Vitamin D Deficient and Non-Deficient PCOS Patients | ||||||
| Fasting glucose | 4 | 5 | 0.31 (0.10, 0.53) | 0.429 | 0.0 | 0.254 |
| Fasting insulin | 4 | 5 | 0.63 (0.42, 0.85) | 0.146 | 41.3 | 0.077 |
| HOMA-IR | 4 | 5 | 1.11 (0.51, 1.71) | 0.002 | 76.5 | 0.130 |
| HOMA-β | 2 | 3 | 0.43 (0.15, 0.71) | 0.183 | 41.1 | 0.613 |
| QUICKI | 2 | 3 | −0.63 (−1.28, 0.03) | 0.069 | 62.6 | 0.207 |
| Total cholesterol | 3 | 4 | −0.14 (−0.67, 0.40) | 0.026 | 67.7 | 0.767 |
| HDL-C | 2 | 3 | −0.58 (−0.86, −0.30) | 0.379 | 0.0 | 0.673 |
| LDL-C | 2 | 3 | −0.11 (−0.39, 0.16) | 0.101 | 56.3 | 0.658 |
| Triglycerides | 3 | 4 | −0.17 (−1.33, 0.99) | <0.001 | 92.7 | 0.657 |
| CRP | 3 | 4 | 0.12 (−0.67, 0.92) | <0.001 | 85.2 | 0.757 |
| Total testosterone | 4 | 4 | 0.08 (−0.28, 0.60) | 0.075 | 56.5 | 0.576 |
| SHBG | 4 | 4 | 0.16 (−0.28, 0.60) | 0.018 | 70.1 | 0.656 |
| FAI | 3 | 3 | 0.25 (0.01, 0.48) | 0.385 | 0.0 | 0.281 |
| Correlation between 25(OH)D and Metabolic and Endocrine Parameters among Women with PCOS | ||||||
| Fasting glucose | 6 | 6 | −0.23 (−0.38, −0.07) | 0.009 | 67.2 | 0.287 |
| Fasting insulin | 6 | 6 | −0.29 (−0.37, −0.21) | 0.274 | 21.2 | 0.410 |
| HOMA-IR | 9 | 10 | −0.52 (−0.23, 0.72) | <0.001 | 95.9 | 0.153 |
| HOMA-β | 3 | 3 | −0.01 (−0.13, 0.11) | 0.351 | 4.4 | 0.335 |
| QUICKI | 3 | 3 | 0.19 (0.07, 0.30) | 0.467 | 0.0 | 0.036 |
| Total cholesterol | 5 | 6 | −0.05 (−0.30, 0.21) | <0.001 | 84.4 | 0.812 |
| HDL-C | 5 | 5 | 0.35 (0.22, 0.47) | 0.079 | 52.2 | 0.955 |
| LDL-C | 5 | 5 | −0.06 (−0.33, 0.21) | <0.001 | 86.4 | 0.762 |
| Triglycerides | 6 | 7 | −0.69 (−0.91, −0.16) | <0.001 | 98.4 | 0.272 |
| CRP | 3 | 3 | −0.28 (−0.37, −0.18) | 0.550 | 0.0 | 0.530 |
| Total testosterone | 5 | 6 | −0.65 (−0.94, 0.18) | <0.001 | 98.8 | 0.422 |
| SHBG | 5 | 5 | 0.31 (0.23, 0.39) | 0.179 | 36.4 | 0.815 |
| FAI | 5 | 5 | −0.22 (−0.31, −0.12) | 0.099 | 48.8 | 0.406 |
| Free testosterone | 2 | 2 | −0.14 (−0.41, −0.15) | 0.007 | 86.1 | NA |
| DHEAS | 5 | 6 | −0.68 (−0.90, −0.17) | <0.001 | 97.6 | 0.259 |
| Comparison between Post- and Pre-Intervention of Vitamin D | ||||||
| Fasting glucose | 7 | 7 | −0.14 (−0.37, 0.09) | 0.285 | 19.0 | 0.101 |
| Fasting insulin | 7 | 7 | −0.02 (−0.25, 0.21) | 0.838 | 0.0 | 0.722 |
| HOMA-IR | 6 | 6 | −0.05 (−0.29, 0.19) | 0.692 | 0.0 | 0.644 |
| HOMA-β | 3 | 3 | 0.16 (−0.12, 0.44) | 0.767 | 0.0 | 0.953 |
| QUICKI | 4 | 4 | −0.07 (−0.39, 0.26) | 0.762 | 0.0 | 0.579 |
| Total cholesterol | 5 | 5 | 0.01 (−0.24, 0.26) | 0.374 | 5.7 | 0.643 |
| HDL-C | 5 | 5 | 0.03 (−0.22, 0.27) | 0.768 | 0.0 | 0.174 |
| LDL-C | 4 | 4 | 0.10 (−0.17, 0.38) | 0.312 | 0.0 | 0.577 |
| Triglycerides | 4 | 4 | −0.45 (−0.73, −0.17) | 0.607 | 0.0 | 0.002 |
| Total testosterone | 5 | 5 | −0.07 (−0.35, 0.21) | 0.844 | 0.0 | 0.732 |
| SHBG | 3 | 3 | −0.16 (−0.49, 0.17) | 0.729 | 0.0 | 0.706 |
| FAI | 2 | 2 | −0.14 (−0.49, 0.22) | 0.429 | 0.0 | NA |
| Free testosterone | 3 | 3 | −0.17 (−0.50, 0.16) | 0.416 | 0.0 | 0.649 |
| DHEAS | 2 | 2 | 0.16 (−0.39, 0.70) | 0.492 | 0.0 | NA |
| 25(OH)D | 7 | 7 | 2.09 (1.28, 2.91) | <0.001 | 85.5 | 0.201 |
| Post-Intervention of Vitamin D Compared to Post-Intervention of Placebo | ||||||
| Fasting glucose | 4 | 4 | 0.27 (−0.04, 0.58) | 0.210 | 33.7 | 0.811 |
| Fasting insulin | 4 | 4 | 0.14 (−0.14, 0.45) | 0.116 | 49.3 | 0.513 |
| HOMA-IR | 4 | 4 | 0.25 (−0.07, 0.56) | 0.760 | 0.0 | 0.440 |
| QUICKI | 3 | 3 | −0.14 (−0.48, 0.21) | 0.710 | 0.0 | 0.254 |
| HDL-C | 3 | 4 | 0.22 (−0.22, 0.66) | 0.095 | 52.9 | 0.392 |
| LDL-C | 3 | 3 | −0.11 (0.46, 0.23) | 0.799 | 0.0 | 0.133 |
| Triglycerides | 3 | 3 | −0.04 (−0.38, 0.31) | 0.474 | 0.0 | 0.474 |
| Total testosterone | 2 | 2 | −0.09 (−0.60, 0.42) | 0.404 | 0.0 | NA |
| 25(OH)D | 5 | 5 | 2.11 (0.85, 3.37) | <0.001 | 79.5 | 0.177 |
4. Discussion
4.1. Principal Findings and Interpretations
4.2. Strengths and Limitations
5. Conclusions
Supplementary Files
Supplementary File 1Author Contributions
Conflicts of Interests
References
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (pcos). Hum. Reprod. 2004, 19, 41–47. [Google Scholar]
- Asuncion, M.; Calvo, R.M.; San Millan, J.L.; Sancho, J.; Avila, S.; Escobar-Morreale, H.F. A prospective study of the prevalence of the polycystic ovary syndrome in unselected caucasian women from spain. J. Clin. Endocrinol. Metab. 2000, 85, 2434–2438. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Kouli, C.R.; Bergiele, A.T.; Filandra, F.A.; Tsianateli, T.C.; Spina, G.G.; Zapanti, E.D.; Bartzis, M.I. A survey of the polycystic ovary syndrome in the greek island of lesbos: Hormonal and metabolic profile. J. Clin. Endocrinol. Metab. 1999, 84, 4006–4011. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Woods, K.S.; Reyna, R.; Key, T.J.; Knochenhauer, E.S.; Yildiz, B.O. The prevalence and features of the polycystic ovary syndrome in an unselected population. J. Clin. Endocrinol. Metab. 2004, 89, 2745–2749. [Google Scholar] [CrossRef] [PubMed]
- March, W.A.; Moore, V.M.; Willson, K.J.; Phillips, D.I.; Norman, R.J.; Davies, M.J. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum. Reprod. 2010, 25, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Grulet, H.; Hecart, A.C.; Delemer, B.; Gross, A.; Sulmont, V.; Leutenegger, M.; Caron, J. Roles of lh and insulin resistance in lean and obese polycystic ovary syndrome. Clin. Endocrinol. 1993, 38, 621–626. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Dunaif, A. New perspectives in polycystic ovary syndrome. Trends Endocrinol. Metab. 1996, 7, 267–271. [Google Scholar] [CrossRef]
- Dunaif, A.; Finegood, D.T. Beta-cell dysfunction independent of obesity and glucose intolerance in the polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 1996, 81, 942–947. [Google Scholar] [PubMed]
- Alemzadeh, R.; Kansra, A.R. New adolescent polycystic ovary syndrome perspectives. Minerva Pediatr. 2011, 63, 35–47. [Google Scholar] [PubMed]
- Legro, R.S.; Kunselman, A.R.; Dunaif, A. Prevalence and predictors of dyslipidemia in women with polycystic ovary syndrome. Am. J. Med. 2001, 111, 607–613. [Google Scholar] [CrossRef]
- Morin-Papunen, L.C.; Vauhkonen, I.; Koivunen, R.M.; Ruokonen, A.; Tapanainen, J.S. Insulin sensitivity, insulin secretion, and metabolic and hormonal parameters in healthy women and women with polycystic ovarian syndrome. Hum. Reprod. 2000, 15, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Wild, R.A.; Rizzo, M.; Clifton, S.; Carmina, E. Lipid levels in polycystic ovary syndrome: Systematic review and meta-analysis. Fertil. Steril. 2011, 95, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Forrest, K.Y.; Stuhldreher, W.L. Prevalence and correlates of vitamin d deficiency in us adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Hovsepian, S.; Amini, M.; Aminorroaya, A.; Amini, P.; Iraj, B. Prevalence of vitamin d deficiency among adult population of Isfahan city, Iran. J. Health Popul. Nutr. 2011, 29, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Tangpricha, V.; Pearce, E.N.; Chen, T.C.; Holick, M.F. Vitamin d insufficiency among free-living healthy young adults. Am. J. Med. 2002, 112, 659–662. [Google Scholar] [CrossRef]
- Thomson, R.L.; Spedding, S.; Buckley, J.D. Vitamin D in the aetiology and management of polycystic ovary syndrome. Clin. Endocrinol. 2012, 77, 343–350. [Google Scholar] [CrossRef] [PubMed]
- De Groot, P.C.; Dekkers, O.M.; Romijn, J.A.; Dieben, S.W.; Helmerhorst, F.M. Pcos, coronary heart disease, stroke and the influence of obesity: A systematic review and meta-analysis. Hum. Reprod. Update, 2011; 17, 495–500. [Google Scholar]
- Khan, H.; Kunutsor, S.; Franco, O.H.; Chowdhury, R. Vitamin D, type 2 diabetes and other metabolic outcomes: A systematic review and meta-analysis of prospective studies. Proc. Nutr. Soc. 2013, 72, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Wang, L.; Pittas, A.G.; Del Gobbo, L.C.; Zhang, C.; Manson, J.E.; Hu, F.B. Blood 25-hydroxy vitamin d levels and incident type 2 diabetes: A meta-analysis of prospective studies. Diabetes Care 2013, 36, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Schaffer, A.; Sartori, C.; Barbieri, L.; Cassetti, E.; Marino, P.; Galasso, G.; De Luca, G. Vitamin D deficiency is independently associated with the extent of coronary artery disease. Eur. J. Clin. Investig. 2014, 44, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Krul-Poel, Y.H.; Snackey, C.; Louwers, Y.; Lips, P.; Lambalk, C.B.; Laven, J.S.; Simsek, S. The role of vitamin D in metabolic disturbances in polycystic ovary syndrome: A systematic review. Eur. J. Endocrinol. 2013, 169, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Wehr, E.; Pilz, S.; Schweighofer, N.; Giuliani, A.; Kopera, D.; Pieber, T.R.; Obermayer-Pietsch, B. Association of hypovitaminosis D with metabolic disturbances in polycystic ovary syndrome. Eur. J. Endocrinol. 2009, 161, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Ramagopalan, S.V.; Heger, A.; Berlanga, A.J.; Maugeri, N.J.; Lincoln, M.R.; Burrell, A.; Handunnetthi, L.; Handel, A.E.; Disanto, G.; Orton, S.M.; et al. A chip-seq defined genome-wide map of vitamin d receptor binding: Associations with disease and evolution. Genome Res. 2010, 20, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- Dobnig, H.; Pilz, S.; Scharnagl, H.; Renner, W.; Seelhorst, U.; Wellnitz, B.; Kinkeldei, J.; Boehm, B.O.; Weihrauch, G.; Maerz, W. Independent association of low serum 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels with all-cause and cardiovascular mortality. Arch. Intern. Med. 2008, 168, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.M.; Looker, A.C.; Chang, S.C.; Graubard, B.I. Prospective study of serum vitamin D and cancer mortality in the united states. J. Natl. Cancer Inst. 2007, 99, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Schleithoff, S.S.; Tenderich, G.; Berthold, H.K.; Korfer, R.; Stehle, P. Low vitamin D status: A contributing factor in the pathogenesis of congestive heart failure? J. Am. Coll. Cardiol. 2003, 41, 105–112. [Google Scholar] [CrossRef]
- Teegarden, D.; Donkin, S.S. Vitamin D: Emerging new roles in insulin sensitivity. Nutr. Res. Rev. 2009, 22, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Plymate, S.R.; Matej, L.A.; Jones, R.E.; Friedl, K.E. Inhibition of sex hormone-binding globulin production in the human hepatoma (Hep G2) cell line by insulin and prolactin. J. Clin. Endocrinol. Metabol. 1988, 67, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Haffner, S.M.; Stern, M.P.; Mitchell, B.D.; Hazuda, H.P.; Patterson, J.K. Incidence of type II diabetes in mexican americans predicted by fasting insulin and glucose levels, obesity, and body-fat distribution. Diabetes 1990, 39, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Lehto, S.; Ronnemaa, T.; Pyorala, K.; Laakso, M. Cardiovascular risk factors clustering with endogenous hyperinsulinaemia predict death from coronary heart disease in patients with type II diabetes. Diabetologia 2000, 43, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Lillioja, S.; Mott, D.M.; Spraul, M.; Ferraro, R.; Foley, J.E.; Ravussin, E.; Knowler, W.C.; Bennett, P.H.; Bogardus, C. Insulin resistance and insulin secretory dysfunction as precursors of non-insulin-dependent diabetes mellitus. Prospective studies of pima indians. N. Engl. J. Med. 1993, 329, 1988–1992. [Google Scholar] [CrossRef] [PubMed]
- Ruige, J.B.; Assendelft, W.J.; Dekker, J.M.; Kostense, P.J.; Heine, R.J.; Bouter, L.M. Insulin and risk of cardiovascular disease: A meta-analysis. Circulation 1998, 97, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M.K.; Meigs, J.B.; Sullivan, L.M.; D’Agostino, R.B.; Wilson, P.W. Insulin resistance, the metabolic syndrome, and incident cardiovascular events in the framingham offspring study. Diabetes 2005, 54, 3252–3257. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (moose) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Hartling, L.; Milne, A.; Hamm, M.P.; Vandermeer, B.; Ansari, M.; Tsertsvadze, A.; Dryden, D.M. Testing the newcastle ottawa scale showed low reliability between individual reviewers. J. Clin. Epidemiol. 2013, 66, 982–993. [Google Scholar] [CrossRef] [PubMed]
- Juni, P.; Altman, D.G.; Egger, M. Systematic reviews in health care: Assessing the quality of controlled clinical trials. BMJ 2001, 323, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-ottawa scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis of the Behavioural Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Panidis, D.; Balaris, C.; Farmakiotis, D.; Rousso, D.; Kourtis, A.; Balaris, V.; Katsikis, I.; Zournatzi, V.; Diamanti-Kandarakis, E. Serum parathyroid hormone concentrations are increased in women with polycystic ovary syndrome. Clin. Chem. 2005, 51, 1691–1697. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: Orlando, FL, USA, 1985. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rupinski, M.T.; Dunlap, W.P. Approximating pearson product-moment correlations from kendall’s tau and spearman’s rho. Educ. Psychol. Meas. 1996, 56, 429–429. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Hassan, N.E.; El-Orabi, H.A.; Eid, Y.M.; Mohammed, N.R. Effect of 25-hydroxyvitamin D on metabolic parameters and insulin resistance in patients with polycystic ovarian syndrome. Middle East Fertil. Soc. J. 2012, 17, 176. [Google Scholar] [CrossRef]
- Zawadski, J.K.; Dunaif, A. In The Polycystic Ovary Syndrome; Givens, J.H.F., Merriman, G., Eds.; Blackwell Scientific: Cambridge, MA, USA, 1992; pp. 377–384. [Google Scholar]
- Savastano, S.; Valentino, R.; di Somma, C.; Orio, F.; Pivonello, C.; Passaretti, F.; Brancato, V.; Formisano, P.; Colao, A.; Beguinot, F.; et al. Serum 25-hydroxyvitamin D levels, phosphoprotein enriched in diabetes gene product (ped/pea-15) and leptin-to-adiponectin ratio in women with pcos. Nutr. Metab. 2011, 8, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nestler, J.E.; Reilly, E.R.; Cheang, K.I.; Bachmann, L.M.; Downs, R.W. A pilot study: Effects of decreasing serum insulin with diazoxide on vitamin D levels in obese women with polycystic ovary syndrome. Trans. Am. Clin. Climatol. Assoc. 2012, 123, 209–219. [Google Scholar] [PubMed]
- Mahmoudi, T.; Gourabi, H.; Ashrafi, M.; Yazdi, R.S.; Ezabadi, Z. Calciotropic hormones, insulin resistance, and the polycystic ovary syndrome. Fertil. Steril. 2010, 93, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- Li, H.W.; Brereton, R.E.; Anderson, R.A.; Wallace, A.M.; Ho, C.K. Vitamin D deficiency is common and associated with metabolic risk factors in patients with polycystic ovary syndrome. Metab. Clin. Exp. 2011, 60, 1475–1481. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.W.; Tsai, S.J.; Chou, P.Y.; Huang, M.F.; Sun, H.S.; Wu, M.H. Vitamin D receptor 1a promotor −1521 g/c and −1012 a/g polymorphisms in polycystic ovary syndrome. Taiwan J. Obstet. Gynecol. 2012, 51, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Mazloomi, S.; Sharifi, F.; Hajihosseini, R.; Kalantari, S.; Mazloomzadeh, S. Association between hypoadiponectinemia and low serum concentrations of calcium and vitamin D in women with polycystic ovary syndrome. ISRN Endocrinol. 2012, 2012, 949427. [Google Scholar] [CrossRef] [PubMed]
- Tsakova, A.D.; Gateva, A.T.; Kamenov, Z.A. 25(OH) vitamin D levels in premenopausal women with polycystic ovary syndrome and/or obesity. Int. J. Vitam. Nutr. Res. 2012, 82, 399–404. [Google Scholar] [CrossRef] [PubMed]
- El-Shal, A.S.; Shalaby, S.M.; Aly, N.M.; Rashad, N.M.; Abdelaziz, A.M. Genetic variation in the vitamin D receptor gene and vitamin D serum levels in egyptian women with polycystic ovary syndrome. Mol. Biol. Rep. 2013, 40, 6063–6073. [Google Scholar] [CrossRef] [PubMed]
- Guducu, N.; Gormus, U.; Kutay, S.S.; Kavak, Z.N.; Dunder, I. 25-hydroxyvitamin D levels are related to hyperinsulinemia in polycystic ovary syndrome. Gynecol. Endocrinol. 2014, 1–4. [Google Scholar]
- Ghadimi, R.; Esmaeilzadeh, S.; Firoozpour, M.; Ahmadi, A. Does vitamin D status correlate with clinical and biochemical features of polycystic ovarysyndrome in high school girls? Casp. J. Intern. Med. 2014, 5, 202–208. [Google Scholar]
- Sahin, S.; Eroglu, M.; Selcuk, S.; Turkgeldi, L.; Kozali, S.; Davutoglu, S.; Muhcu, M. Intrinsic factors rather than vitamin D deficiency are related to insulin resistance in lean women with polycystic ovary syndrome. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 2851–2856. [Google Scholar] [PubMed]
- Patra, S.K.; Nasrat, H.; Goswami, B.; Jain, A. Vitamin D as a predictor of insulin resistance in polycystic ovarian syndrome. Diabetes Metab. Syndr. 2012, 6, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S.M.; Jha, A. Association of vitamin D3 deficiency with clinical and biochemical parameters in indian women with polycystic ovary syndrome. Int. J. Gynaecol. Obstet. 2013, 123, 74–75. [Google Scholar] [CrossRef] [PubMed]
- Velija-Asimi, Z. Evaluation of the association of vitamin D deficiency with gonadotropins and sex hormone in obese and non-obese women with polycystic ovary syndrome. Med. Glas. 2014, 11, 170–176. [Google Scholar]
- Hahn, S.; Haselhorst, U.; Tan, S.; Quadbeck, B.; Schmidt, M.; Roesler, S.; Kimmig, R.; Mann, K.; Janssen, O.E. Low serum 25-hydroxyvitamin D concentrations are associated with insulin resistance and obesity in women with polycystic ovary syndrome. Exp. Clin. Endocrinol. Diabetes 2006, 114, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Yildizhan, R.; Kurdoglu, M.; Adali, E.; Kolusari, A.; Yildizhan, B.; Sahin, H.G.; Kamaci, M. Serum 25-hydroxyvitamin D concentrations in obese and non-obese women with polycystic ovary syndrome. Arch. Gynecol. Obstet. 2009, 280, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Bonakdaran, S.; Khorasani, Z.M.; Davachi, B.; Khorasani, J.M. The effects of calcitriol on improvement of insulin resistance, ovulation and comparison with metformin therapy in pcos patients: A randomized placebo-controlled clinical trial. Iran. J. Reprod. Med. 2012, 10, 465–472. [Google Scholar] [PubMed]
- Kozakowski, J.; Kapuscinska, R.; Zgliczynski, W. Associations of vitamin D concentration with metabolic and hormonal indices in women with polycystic ovary syndrome presenting abdominal and gynoidal type of obesity. Ginekol. Pol. 2014, 85, 765–770. [Google Scholar] [PubMed]
- Kotsa, K.; Yavropoulou, M.P.; Anastasiou, O.; Yovos, J.G. Role of vitamin D treatment in glucose metabolism in polycystic ovary syndrome. Fertil. Steril. 2009, 92, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Selimoglu, H.; Duran, C.; Kiyici, S.; Ersoy, C.; Guclu, M.; Ozkaya, G.; Tuncel, E.; Erturk, E.; Imamoglu, S. The effect of vitamin D replacement therapy on insulin resistance and androgen levels in women with polycystic ovary syndrome. J. Endocrinol. Investig. 2010, 33, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Wehr, E.; Pieber, T.R.; Obermayer-Pietsch, B. Effect of vitamin D3 treatment on glucose metabolism and menstrual frequency in polycystic ovary syndrome women: A pilot study. J. Endocrinol. Investig. 2011, 34, 757–763. [Google Scholar]
- Ardabili, H.R.; Gargari, B.P.; Farzadi, L. Vitamin D supplementation has no effect on insulin resistance assessment in women with polycystic ovary syndrome and vitamin D deficiency. Nutr. Res. 2012, 32, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Pal, L.; Berry, A.; Coraluzzi, L.; Kustan, E.; Danton, C.; Shaw, J.; Taylor, H. Therapeutic implications of vitamin D and calcium in overweight women with polycystic ovary syndrome. Gynecol. Endocrinol. 2012, 28, 965–968. [Google Scholar] [CrossRef] [PubMed]
- Rahimi-Ardabili, H.; Pourghassem Gargari, B.; Farzadi, L. Effects of vitamin D on cardiovascular disease risk factors in polycystic ovary syndrome women with vitamin D deficiency. J. Endocrinol. Investig. 2013, 36, 28–32. [Google Scholar]
- Asemi, Z.; Foroozanfard, F.; Hashemi, T.; Bahmani, F.; Jamilian, M.; Esmaillzadeh, A. Calcium plus vitamin D supplementation affects glucose metabolism and lipid concentrations in overweight and obese vitamin D deficient women with polycystic ovary syndrome. Clin. Nutr. 2014. [Google Scholar] [CrossRef] [PubMed]
- Raja-Khan, N.; Shah, J.; Stetter, C.M.; Lott, M.E.; Kunselman, A.R.; Dodson, W.C.; Legro, R.S. High-dose vitamin D supplementation and measures of insulin sensitivity in polycystic ovary syndrome: A randomized, controlled pilot trial. Fertil. Steril. 2014, 101, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Tehrani, H.G.; Mostajeran, F.; Shahsavari, S. The effect of calcium and vitamin D supplementation on menstrual cycle, body mass index and hyperandrogenism state of women with poly cystic ovarian syndrome. J. Res. Med. Sci. 2014, 19, 875–880. [Google Scholar] [PubMed]
- Carmina, E.; Lobo, R.A. Use of fasting blood to assess the prevalence of insulin resistance in women with polycystic ovary syndrome. Fertil. Steril. 2004, 82, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Dunaif, A. Insulin resistance and the polycystic ovary syndrome: Mechanism and implications for pathogenesis. Endocr. Rev. 1997, 18, 774–800. [Google Scholar] [CrossRef] [PubMed]
- Schachter, M.; Raziel, A.; Friedler, S.; Strassburger, D.; Bern, O.; Ron-El, R. Insulin resistance in patients with polycystic ovary syndrome is associated with elevated plasma homocysteine. Hum. Reprod. 2003, 18, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Misso, M.L.; Wild, R.A.; Norman, R.J. Impaired glucose tolerance, type 2 diabetes and metabolic syndrome in polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2010, 16, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.; Brennan, K.; Azziz, R. Prevalence of hyperandrogenemia in the polycystic ovary syndrome diagnosed by the national institutes of health 1990 criteria. Fertil. Steril. 2010, 93, 1938–1941. [Google Scholar] [CrossRef] [PubMed]
- Bourlon, P.M.; Billaudel, B.; Faure-Dussert, A. Influence of vitamin D3 deficiency and 1,25 dihydroxyvitamin D3 on de novo insulin biosynthesis in the islets of the rat endocrine pancreas. J. Endocrinol. 1999, 160, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.; Meigs, J.B.; Pittas, A.G.; McKeown, N.M.; Economos, C.D.; Booth, S.L.; Jacques, P.F. Plasma 25-hydroxyvitamin D is associated with markers of the insulin resistant phenotype in nondiabetic adults. J. Nutr. 2009, 139, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Mattila, C.; Knekt, P.; Mannisto, S.; Rissanen, H.; Laaksonen, M.A.; Montonen, J.; Reunanen, A. Serum 25-hydroxyvitamin D concentration and subsequent risk of type 2 diabetes. Diabetes Care 2007, 30, 2569–2570. [Google Scholar] [CrossRef] [PubMed]
- Ortlepp, J.R.; Metrikat, J.; Albrecht, M.; von Korff, A.; Hanrath, P.; Hoffmann, R. The vitamin D receptor gene variant and physical activity predicts fasting glucose levels in healthy young men. Diabetic Med. 2003, 20, 451–454. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Sowers, M.; Bell, C.; Third National, H.; Nutrition Examination, S. Serum 25-hydroxyvitamin D, diabetes, and ethnicity in the third national health and nutrition examination survey. Diabetes Care 2004, 27, 2813–2818. [Google Scholar] [CrossRef] [PubMed]
- Zeitz, U.; Weber, K.; Soegiarto, D.W.; Wolf, E.; Balling, R.; Erben, R.G. Impaired insulin secretory capacity in mice lacking a functional vitamin D receptor. FASEB J. 2003, 17, 509–511. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, C.; Lin, Z.; Robb, S.W.; Ezeamama, A.E. Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 4555-4577. https://doi.org/10.3390/nu7064555
He C, Lin Z, Robb SW, Ezeamama AE. Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis. Nutrients. 2015; 7(6):4555-4577. https://doi.org/10.3390/nu7064555
Chicago/Turabian StyleHe, Chunla, Zhoumeng Lin, Sara Wagner Robb, and Amara E. Ezeamama. 2015. "Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis" Nutrients 7, no. 6: 4555-4577. https://doi.org/10.3390/nu7064555
APA StyleHe, C., Lin, Z., Robb, S. W., & Ezeamama, A. E. (2015). Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis. Nutrients, 7(6), 4555-4577. https://doi.org/10.3390/nu7064555