Efficacy of Synbiotics in Patients with Slow Transit Constipation: A Prospective Randomized Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Issues
2.2. Patients
2.3. Study Design
2.4. Outcomes
2.5. Safety Assessments
2.6. Sample Size
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Primary and Secondary Efficacy Endpoints
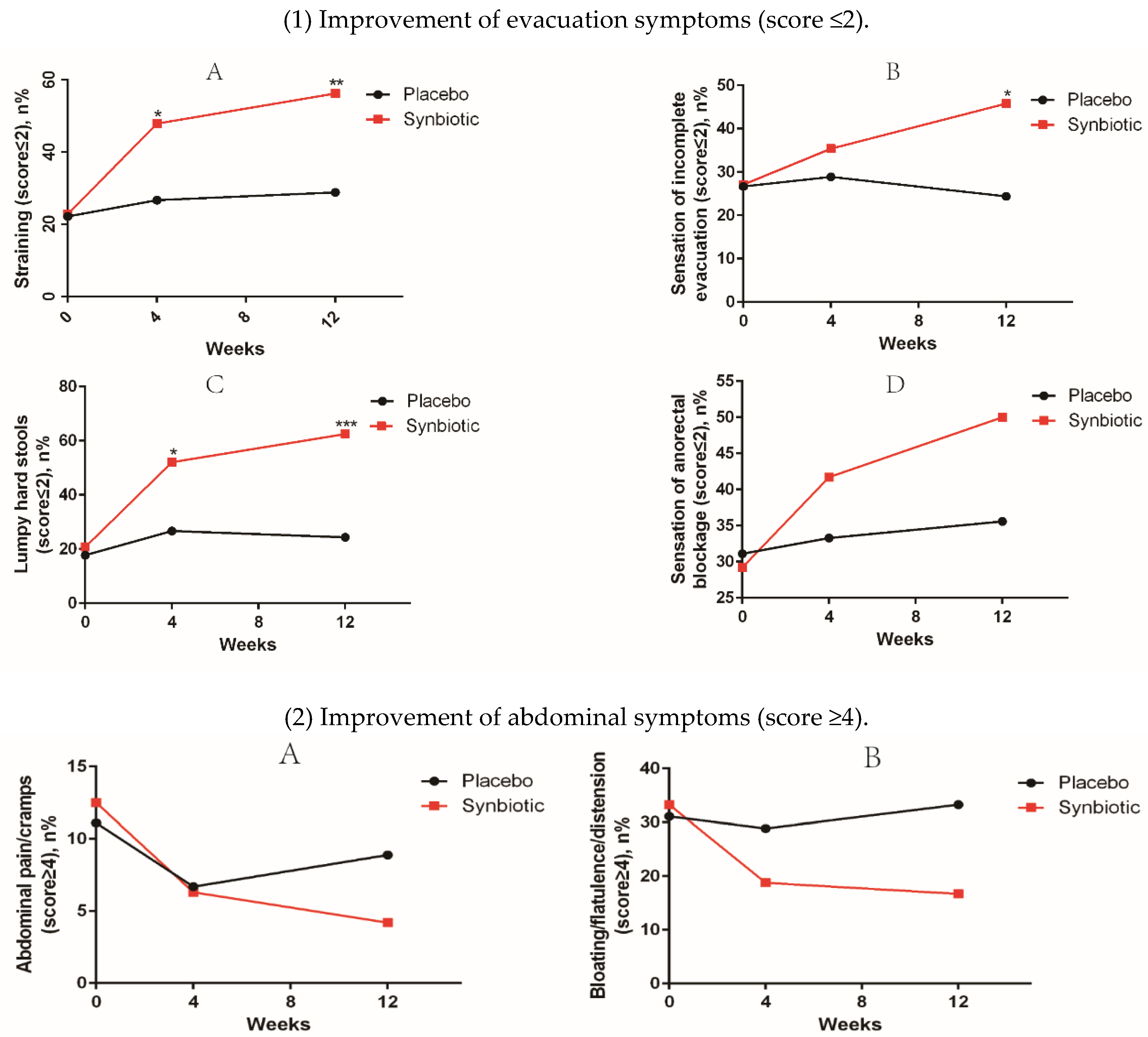
3.3. Other Efficacy Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nelson, A.D.; Camilleri, M.; Chirapongsathorn, S.; Vijayvargiya, P.; Valentin, N.; Shin, A.; Erwin, P.J.; Wang, Z.; Murad, M.H. Comparison of efficacy of pharmacological treatments for chronic idiopathic constipation: A systematic review and network meta-analysis. Gut 2016. [Google Scholar] [CrossRef] [PubMed]
- Higgins, P.D.; Johanson, J.F. Epidemiology of constipation in north america: A systematic review. Am. J. Gastroenterol. 2004, 99, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Mugie, S.M.; Benninga, M.A.; Di Lorenzo, C. Epidemiology of constipation in children and adults: A systematic review. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.S.; Rattanakovit, K.; Patcharatrakul, T. Diagnosis and management of chronic constipation in adults. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Bharucha, A.E.; Pemberton, J.H.; Locke, G.R., III. American gastroenterological association technical review on constipation. Gastroenterology 2013, 144, 218–238. [Google Scholar] [CrossRef] [PubMed]
- American Gastroenterological Association; Bharucha, A.E.; Dorn, S.D.; Lembo, A.; Pressman, A. American gastroenterological association medical position statement on constipation. Gastroenterology 2013, 144, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Suares, N.C. Effect of laxatives and pharmacological therapies in chronic idiopathic constipation: Systematic review and meta-analysis. Gut 2011, 60, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Kerstens, R.; Rykx, A.; Vandeplassche, L. A placebo-controlled trial of prucalopride for severe chronic constipation. N. Engl. J. Med. 2008, 358, 2344–2354. [Google Scholar] [CrossRef] [PubMed]
- Sajid, M.S.; Hebbar, M.; Baig, M.K.; Li, A.; Philipose, Z. Use of prucalopride for chronic constipation: A systematic review and meta-analysis of published randomized, controlled trials. J. Neurogastroenterol. Motil. 2016, 22, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.H.; Chen, C.L.; Wang, J.D.; Yang, Y.J.; Cun, Y.; Wu, J.B.; Liu, Y.H.; Dan, H.L.; Jian, Y.T.; Chen, X.Q. Effects of probiotic on intestinal mucosa of patients with ulcerative colitis. World J. Gastroenterol. 2004, 10, 1521–1525. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarczyk, M.M.; Miller, M.J.; Freund, G.G. The health benefits of dietary fiber: Beyond the usual suspects of type 2 diabetes mellitus, cardiovascular disease and colon cancer. Metabolism 2012, 61, 1058–1066. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.; Bruggeman, G.; van den Berg, M.; Borewicz, K.; Scheurink, A.J.; Bruininx, E.; de Vos, P.; Smidt, H.; Schols, H.A.; Gruppen, H. Effects of pectin on fermentation characteristics, carbohydrate utilization and microbial community composition in the gastrointestinal tract of weaning pigs. Mol. Nutr. Food Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Voderholzer, W.A.; Schatke, W.; Muhldorfer, B.E.; Klauser, A.G.; Birkner, B.; Muller-Lissner, S.A. Clinical response to dietary fiber treatment of chronic constipation. Am. J. Gastroenterol. 1997, 92, 95–98. [Google Scholar] [PubMed]
- Tian, L.; Scholte, J.; Borewicz, K.; Bogert, B.V.; Smidt, H.; Scheurink, A.J.; Gruppen, H.; Schols, H.A. Effects of pectin supplementation on the fermentation patterns of different structural carbohydrates in rats. Mol. Nutr. Food Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.O.; Leung, G.; Tong, T.; Wong, N.Y. Increasing dietary fiber intake in terms of kiwifruit improves constipation in chinese patients. World J. Gastroenterol. 2007, 13, 4771–4775. [Google Scholar] [CrossRef] [PubMed]
- Eswaran, S.; Muir, J.; Chey, W.D. Fiber and functional gastrointestinal disorders. Am. J. Gastroenterol. 2013, 108, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Soret, R.; Chevalier, J.; De Coppet, P.; Poupeau, G.; Derkinderen, P.; Segain, J.P.; Neunlist, M. Short-chain fatty acids regulate the enteric neurons and control gastrointestinal motility in rats. Gastroenterology 2010, 138, 1772–1782. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, S.; Tatewaki, M.; Yamada, T.; Fujimiya, M.; Mantyh, C.; Voss, M.; Eubanks, S.; Harris, M.; Pappas, T.N.; Takahashi, T. Short-chain fatty acids stimulate colonic transit via intraluminal 5-ht release in rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 284, R1269–R1276. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Quigley, E.M.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.; Moayyedi, P. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: Systematic review and meta-analysis. Am. J. Gastroenterol. 2014, 109, 1547–1561. [Google Scholar] [CrossRef] [PubMed]
- Morelli, L.; Zonenschain, D.; Callegari, M.L.; Grossi, E.; Maisano, F.; Fusillo, M. Assessment of a new synbiotic preparation in healthy volunteers: Survival, persistence of probiotic strains and its effect on the indigenous flora. Nutr. J. 2003, 2, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drossman, D.A. The functional gastrointestinal disorders and the rome iii process. Gastroenterology 2006, 130, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Emmanuel, A.; Cools, M.; Vandeplassche, L.; Kerstens, R. Prucalopride improves bowel function and colonic transit time in patients with chronic constipation: An integrated analysis. Am. J. Gastroenterol. 2014, 109, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Agachan, F.; Chen, T.; Pfeifer, J.; Reissman, P.; Wexner, S.D. A constipation scoring system to simplify evaluation and management of constipated patients. Dis. Colon Rectum 1996, 39, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Ge, X.; Tian, H.; Ding, C.; Gu, L.; Wei, Y.; Gong, J.; Zhu, W.; Li, N.; Li, J. Fecal microbiota transplantation in combination with soluble dietary fiber for treatment of slow transit constipation: A pilot study. Arch. Med. Res. 2016, 47, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.; Kleinman, L.; Farup, C.; Taylor, L.; Miner, P., Jr. Psychometric validation of a constipation symptom assessment questionnaire. Scand. J. Gastroenterol. 1999, 34, 870–877. [Google Scholar] [PubMed]
- Eypasch, E.; Williams, J.I.; Wood-Dauphinee, S.; Ure, B.M.; Schmulling, C.; Neugebauer, E.; Troidl, H. Gastrointestinal quality of life index: Development, validation and application of a new instrument. Br. J. Surg. 1995, 82, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Waitzberg, D.L.; Logullo, L.C.; Bittencourt, A.F.; Torrinhas, R.S.; Shiroma, G.M.; Paulino, N.P.; Teixeira-da-Silva, M.L. Effect of synbiotic in constipated adult women—A randomized, double-blind, placebo-controlled study of clinical response. Clin. Nutr. 2013, 32, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Jiang, J.; Feng, X.; Ding, W.; Liu, J.; Li, J. Long-term follow-up of the jinling procedure for combined slow-transit constipation and obstructive defecation. Dis. Colon Rectum 2013, 56, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.A. Functional gastrointestinal disorders: History, pathophysiology, clinical features and Rome IV. Gastroenterology 2016, 150, 1262–1279. [Google Scholar] [CrossRef] [PubMed]
- Parthasarathy, G.; Chen, J.; Chen, X.F.; Chia, N.; O'Connor, H.M.; Wolf, P.G.; Gaskins, H.R.; Bharucha, A.E. Relationship between microbiota of the colonic mucosa vs feces and symptoms, colonic transit, and methane production in female patients with chronic constipation. Gastroenterology 2016, 150, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Liu, W.; Alkhouri, R.; Baker, R.D.; Bard, J.E.; Quigley, E.M.; Baker, S.S. Structural changes in the gut microbiome of constipated patients. Physiol. Genom. 2014, 46, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Vandeputte, D.; Falony, G.; Vieira-Silva, S.; Tito, R.Y.; Joossens, M.; Raes, J. Stool consistency is strongly associated with gut microbiota richness and composition, enterotypes and bacterial growth rates. Gut 2016, 65, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Ding, C.; Gong, J.; Ge, X.; McFarland, L.V.; Gu, L.; Wei, Y.; Chen, Q.; Zhu, W.; Li, J.; et al. Treatment of slow transit constipation with fecal microbiota transplantation: A pilot study. J. Clin. Gastroenterol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Christodoulides, S.; Dimidi, E.; Fragkos, K.C.; Farmer, A.D.; Whelan, K.; Scott, S.M. Systematic review with meta-analysis: Effect of fibre supplementation on chronic idiopathic constipation in adults. Aliment. Pharmacol. Ther. 2016, 44, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Suares, N.C.; Ford, A.C. Systematic review: The effects of fibre in the management of chronic idiopathic constipation. Aliment. Pharmacol. Ther. 2011, 33, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Dongowski, G.; Lorenz, A.; Proll, J. The degree of methylation influences the degradation of pectin in the intestinal tract of rats and in vitro. J. Nutr. 2002, 132, 1935–1944. [Google Scholar] [PubMed]
- Onumpai, C.; Kolida, S.; Bonnin, E.; Rastall, R.A. Microbial utilization and selectivity of pectin fractions with various structures. Appl. Environ. Microbiol. 2011, 77, 5747–5754. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.M.; de Souza, R.; Kendall, C.W.; Emam, A.; Jenkins, D.J. Colonic health: Fermentation and short chain fatty acids. J. Clin. Gastroenterol. 2006, 40, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Muller-Lissner, S.; Tack, J.; Feng, Y.; Schenck, F.; Specht Gryp, R. Levels of satisfaction with current chronic constipation treatment options in europe - an internet survey. Aliment. Pharmacol. Ther. 2013, 37, 137–145. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Placebo (n = 45) | Treatment (n = 48) | p Value |
|---|---|---|---|
| Sex (male/female) * | 16 (35.6)/29 (64.4) | 18 (37.5)/30 (62.5) | 0.846 |
| Age (year) † | 48.3 ± 11.3 | 47.2 ± 10.7 | 0.638 |
| BMI (kg/m2) † | 22.8 ± 1.1 | 22.6 ± 1.1 | 0.305 |
| Disease duration (year) † | 7.1 ± 4.2 | 7.4 ± 3.9 | 0.695 |
| Wexner score † | 19.8 ± 2.0 | 20.0 ± 2.2 | 0.797 |
| No. of BMs/week † | 2.1 ± 0.6 | 2.2 ± 0.7 | 0.615 |
| Stool consistency † | 2.0 ± 0.6 | 2.1 ± 0.5 | 0.366 |
| CTT (h) † | 73.0 ± 10.3 | 71.7 ± 10.8 | 0.567 |
| Smoker * | 3 (6.7) | 4 (8.3) | 0.761 |
| Alcohol consumer * | 6 (13.3) | 5 (10.4) | 0.663 |
| Regular exercise * | 12 (26.7) | 14 (29.2) | 0.788 |
| Endpoint | 4 Week | 12 Week | ||
|---|---|---|---|---|
| Placebo | Synbiotic | Placebo | Synbiotic | |
| Clinical remission rate (%) † | 6 (13.3) | 18 (37.5) ** | 8 (16.7) | 22 (45.8) ** |
| Clinical improvement rate (%) † | 11 (24.4) | 25 (52.1) ** | 14 (29.2) | 31 (64.6) ** |
| No. of BMs/week ‡ | 2.9 ± 1.1 | 4.5 ± 1.6 *** | 3.1 ± 1.4 | 5.1 ± 2.0 *** |
| Stool consistency ‡ | 2.5 ± 0.8 | 3.2 ± 1.2 *** | 2.4 ± 0.8 | 3.5 ± 1.1 *** |
| CTT (h) ‡ | 68.2 ± 11.3 | 53.8 ± 10.9 ** | 70.5 ± 12.1 | 49.3 ± 11.7 *** |
| Week | PAC-SYM † | GIQLI † | Satisfaction Score † | |||
|---|---|---|---|---|---|---|
| Placebo | Synbiotic | Placebo | Synbiotic | Placebo | Synbiotic | |
| Baseline | 1.9 ± 0.3 | 1.9 ± 0.2 | 86.3 ± 11.2 | 83.5 ± 12.6 | — | — |
| 4 weeks | 1.8 ± 0.3 | 1.4 ± 0.5 ** | 91.7 ± 12.8 | 117.8 ± 15.8 ** | 2.8 ± 1.2 | 3.5 ± 1.4 * |
| 12 weeks | 1.7 ± 0.4 | 1.2 ± 0.6 *** | 95.5 ± 15.3 | 126.9 ± 16.5 *** | 2.9 ± 1.3 | 3.8 ± 1.4 ** |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, C.; Ge, X.; Zhang, X.; Tian, H.; Wang, H.; Gu, L.; Gong, J.; Zhu, W.; Li, N. Efficacy of Synbiotics in Patients with Slow Transit Constipation: A Prospective Randomized Trial. Nutrients 2016, 8, 605. https://doi.org/10.3390/nu8100605
Ding C, Ge X, Zhang X, Tian H, Wang H, Gu L, Gong J, Zhu W, Li N. Efficacy of Synbiotics in Patients with Slow Transit Constipation: A Prospective Randomized Trial. Nutrients. 2016; 8(10):605. https://doi.org/10.3390/nu8100605
Chicago/Turabian StyleDing, Chao, Xiaolong Ge, Xueying Zhang, Hongliang Tian, Hongkan Wang, Lili Gu, Jianfeng Gong, Weiming Zhu, and Ning Li. 2016. "Efficacy of Synbiotics in Patients with Slow Transit Constipation: A Prospective Randomized Trial" Nutrients 8, no. 10: 605. https://doi.org/10.3390/nu8100605
APA StyleDing, C., Ge, X., Zhang, X., Tian, H., Wang, H., Gu, L., Gong, J., Zhu, W., & Li, N. (2016). Efficacy of Synbiotics in Patients with Slow Transit Constipation: A Prospective Randomized Trial. Nutrients, 8(10), 605. https://doi.org/10.3390/nu8100605