An Evaluation of the Pea Pod System for Assessing Body Composition of Moderately Premature Infants

Abstract
:1. Introduction
2. Materials and Methods
2.1. Infants
2.2. Protocol
2.3. Total Body Water
2.4. Pea Pod
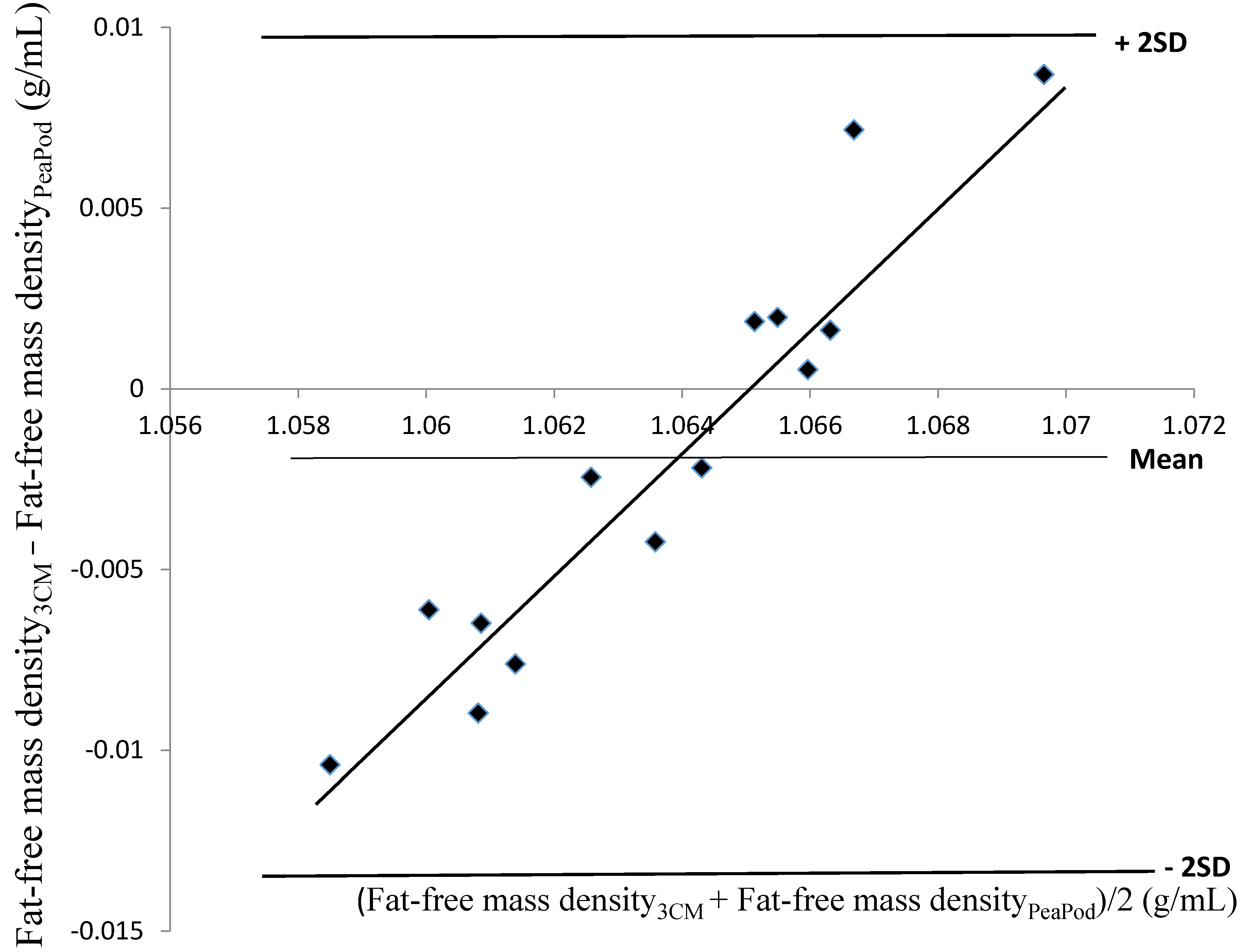
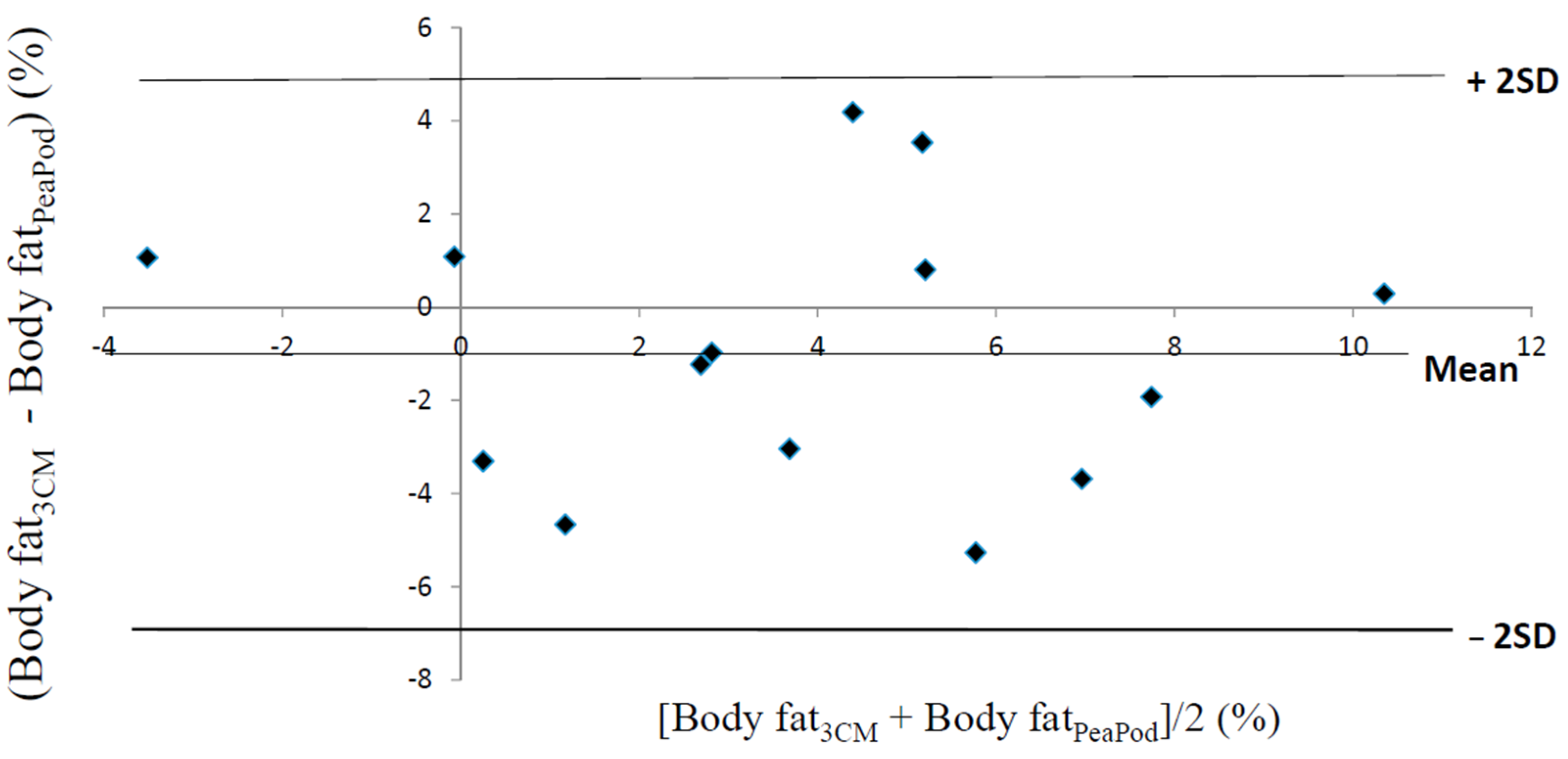
2.5. Fat-Free Mass Density and Hydration and Body Fat Calculated Using a Three-Component Model
2.6. Biological Variability of Fat-Free Mass Density
2.7. Statistics
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| 3CM | Three-component model |
| f | fraction of fat in the bodyl |
References
- Friis-Hansen, B. Water distribution in the foetus and newborn infant. Acta Paediatr. Scand. 1983, 72, 7–11. [Google Scholar] [CrossRef]
- Yeung, M.Y. Postnatal growth, neurodevelopment and altered adiposity after preterm birth-from a clinical nutrition perspective. Acta Paediatr. 2006, 95, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.J.; Wootton, S.A.; Leaf, A.A.; Jackson, A.A. Preterm birth and body composition at term equivalent age: A systematic review and meta-analysis. Pediatrics 2012, 130, e640–e649. [Google Scholar] [CrossRef] [PubMed]
- Ellis, K.J.; Yao, M.; Shypailo, R.J.; Urlando, A.; Wong, W.W.; Heird, W.C. Body-composition assessment in infancy: Air-displacement plethysmography compared with a reference 4-compartment model. Am. J. Clin. Nutr. 2007, 85, 90–95. [Google Scholar] [PubMed]
- Roggero, P.; Gianni, M.L.; Amato, O.; Piemontese, P.; Morniroli, D.; Wong, W.W.; Mosca, F. Evaluation of air-displacement plethysmography for body composition assessment in preterm infants. Pediatr. Res. 2012, 72, 316–320. [Google Scholar] [CrossRef] [PubMed]
- International Atomic Energy Agency. Assessment of Body Composition and Total Energy Expenditure in Humans Using Stable Isotope Techniques; IAEA Human Health Series No. 3; International Atomic Energy Agency: Vienna, Austria, 2009. [Google Scholar]
- Corpeleijn, W.E.; Kouwenhoven, S.M.P.; van Goudoever, J.B. Optimal growth of preterm infants. World Rev. Nutr. Diet. 2013, 106, 149–155. [Google Scholar] [PubMed]
- Going, S.B. Hydrodensitometry and air displacement plethysmography. In Human Body Composition, 2nd ed.; Heymsfield, S.B., Lohman, T.G., Wang, Z., Going, S.B., Eds.; Human Kinetics: Champaign, IL, USA, 2005; pp. 17–33. [Google Scholar]
- Urlando, A.; (Cosmed, Concord, USA). Personal communication, 2015.
- Fomon, S.J.; Haschke, F.; Ziegler, E.E.; Nelson, S.E. Body composition of reference children from birth to age 10 years. Am. J. Clin. Nutr. 1982, 35, 1169–1175. [Google Scholar] [PubMed]
- Eriksson, B.; Löf, M.; Eriksson, O.; Hannestad, U.; Forsum, E. Fat-free mass hydration in newborns: Assessment and implications for body composition studies. Acta Paediatr. 2011, 100, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Schoeller, D.A. Hydrometry. In Human Body Composition, 2nd ed.; Heymsfield, S.B., Lohman, T.G., Wang, Z., Going, S.B., Eds.; Human Kinetics: Champaign, IL, USA, 2005; pp. 35–49. [Google Scholar]
- Eriksson, B.; Löf, M.; Forsum, E. Body composition in full-term healthy infants measured with air displacement plethysmography at 1 and 12 weeks of age. Acta Paediatr. 2010, 99, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Siri, W.E. Body composition from fluid spaces and density: Analysis of methods. Nutrition 1993, 9, 480–491. [Google Scholar] [PubMed]
- Widdowson, E.M. Changes in body composition during growth. In Scientific Foundations of Paediatrics, 2nd ed.; Davis, J.A., Dobbing, J., Eds.; Heinemann Medical Books Ltd.: London, UK, 1981; pp. 330–342. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Niklasson, A.; Albertsson-Wikland, K. Continuous growth reference from 24th week of gestation to 24 months by gender. BMC Pediatr. 2008, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Urlando, A.; Dempster, P.; Aitkens, S. A new air displacement plethysmograph for the measurement of body composition in infants. Pediatr. Res. 2003, 53, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.B.; Coward, W.A.; Schlingenseipen, K.-H.; Nohria, V.; Lucas, A. Comparison of the doubly labeled water (2H218O) method with indirect calorimetry and a nutrient-balance study for simultaneous determination of energy expenditure, water intake, and metabolizable energy intake in preterm infants. Am. J. Clin. Nutr. 1986, 44, 315–322. [Google Scholar] [PubMed]
- Fields, D.A.; Wilson, G.D.; Gladden, L.B.; Hunter, G.R.; Pascoe, D.D.; Goran, M.I. Comparison of the BOD POD with the four-compartment model in adult females. Med. Sci. Sports Exerc. 2001, 33, 1605–1610. [Google Scholar] [CrossRef] [PubMed]
- Fuller, N.J.; Jebb, S.A.; Laskey, M.A.; Coward, W.A.; Elia, M. Four-component model for the assessment of body composition in humans: Comparison with alternative methods, and evaluation of the density and hydration of fat-free mass. Clin. Sci. 1992, 82, 687–693. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sex | Gestational Age at Birth Weeks + Days | Age at Investigation Days | Weight at Birth g | Weight z Score 1 | Length at Birth cm | Length z Score 1 |
|---|---|---|---|---|---|---|
| male | 33 + 1 | 7 | 1710 | −1.93 | 43 | −2.29 |
| male | 35 + 3 | 5 | 2090 | −1.77 | 45 | −1.33 |
| male | 33 + 6 | 4 | 2306 | 0.34 | 45 | −0.60 |
| male | 33 + 0 | 6 | 2370 | 0.56 | 46 | 0.85 |
| female 2 | 32 + 4 | 6 | 1805 | −1.20 | 41 | −2.36 |
| female 2 | 32 + 4 | 6 | 1780 | −1.30 | 40 | −3.07 |
| male | 35 + 6 | 4 | 2685 | −0.44 | 48 | 0 |
| male | 32 + 5 | 7 | 1970 | −0.85 | 43 | −1.29 |
| male 3 | 35 + 0 | 4 | 1875 | −2.60 | 45 | −1.33 |
| male 3 | 35 + 0 | 4 | 1750 | −3.14 | 45 | −1.33 |
| male | 35 + 2 | 3 | 2520 | −0.31 | 47 | 0 |
| female | 35 + 2 | 3 | 2510 | −0.04 | 44 | −1.64 |
| female | 35 + 4 | 4 | 2680 | −0.14 | 47 | −0.20 |
| male | 32 + 3 | 5 | 1790 | −0.80 | 44 | 0.21 |
| mean | 34 + 1 | 4.9 | 2132 | −1.02 | 45 | −0.96 |
| SD | 1 + 2 | 1.4 | 367 | 1.04 | 2 | 1.06 |
| Mean ± SD | |
|---|---|
| Body weight 1, kg | 2.038 ± 0.332 |
| Body volume 2, L | 1.930 ± 0.322 |
| Total body water 3, kg | 1.630 ± 0.240 |
| Total body water 3, % | 80.30 ± 3.87 |
| Body density 4, g/mL | 1.057 ± 0.007 |
| Fat-Free Mass Density (g/mL) | Body Fat (%) | Hydration Factor (%) | |
|---|---|---|---|
| Pea Pod system | 1.0646 ± 0.0009 | 4.2 ± 3.9 | - |
| Three-component model | 1.0627 ± 0.0059 1 | 3.2 ± 3.8 1 | 83.0 ± 1.4 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsum, E.; Olhager, E.; Törnqvist, C. An Evaluation of the Pea Pod System for Assessing Body Composition of Moderately Premature Infants. Nutrients 2016, 8, 238. https://doi.org/10.3390/nu8040238
Forsum E, Olhager E, Törnqvist C. An Evaluation of the Pea Pod System for Assessing Body Composition of Moderately Premature Infants. Nutrients. 2016; 8(4):238. https://doi.org/10.3390/nu8040238
Chicago/Turabian StyleForsum, Elisabet, Elisabeth Olhager, and Caroline Törnqvist. 2016. "An Evaluation of the Pea Pod System for Assessing Body Composition of Moderately Premature Infants" Nutrients 8, no. 4: 238. https://doi.org/10.3390/nu8040238
APA StyleForsum, E., Olhager, E., & Törnqvist, C. (2016). An Evaluation of the Pea Pod System for Assessing Body Composition of Moderately Premature Infants. Nutrients, 8(4), 238. https://doi.org/10.3390/nu8040238