A Randomised, Cross-Over Study to Estimate the Influence of Food on the 25-Hydroxyvitamin D3 Serum Level after Vitamin D3 Supplementation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
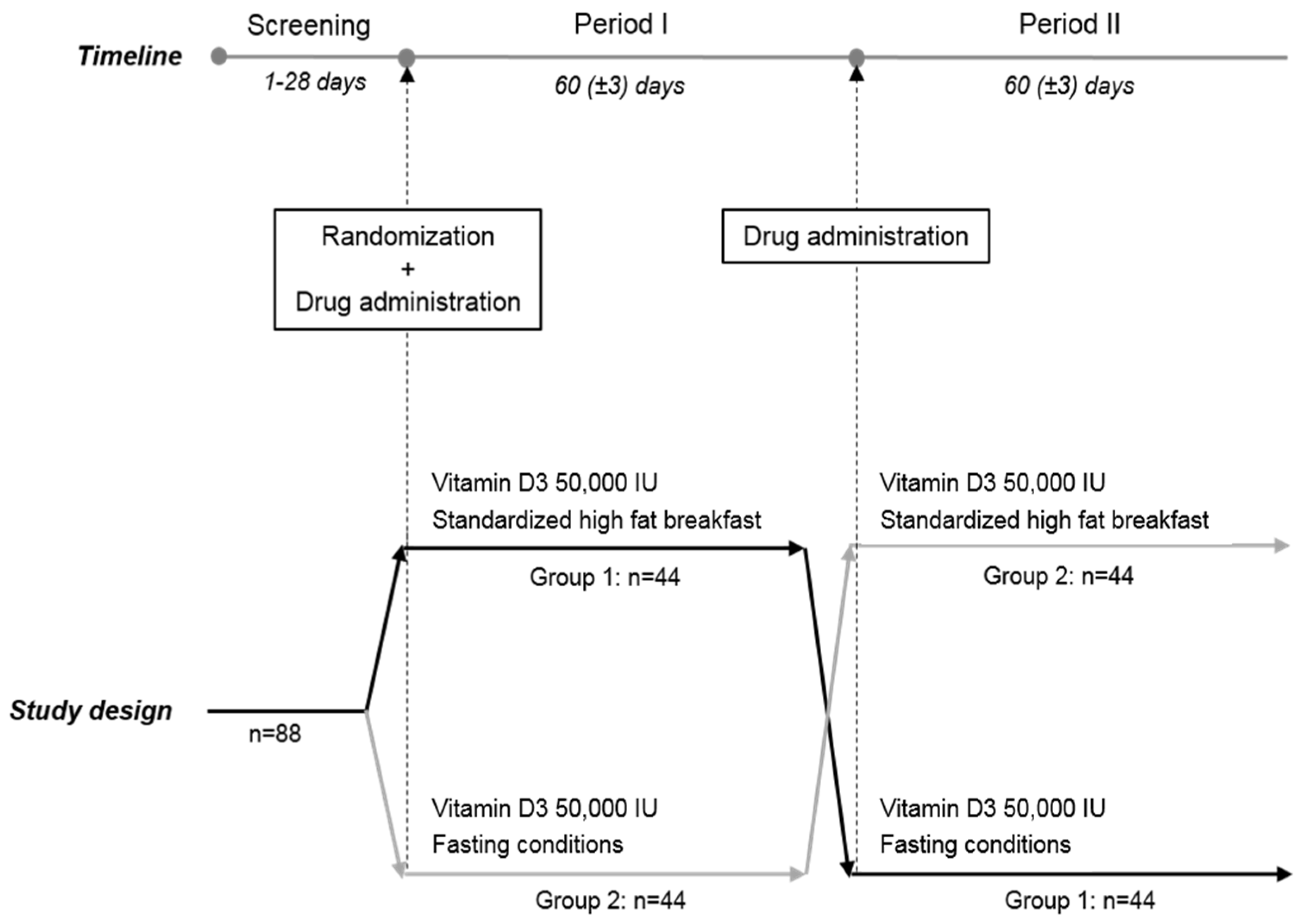
2.1. Methodoloy
2.2. Study Population
2.3. Laboratory Assessment
2.4. Statistical Methods
3. Results
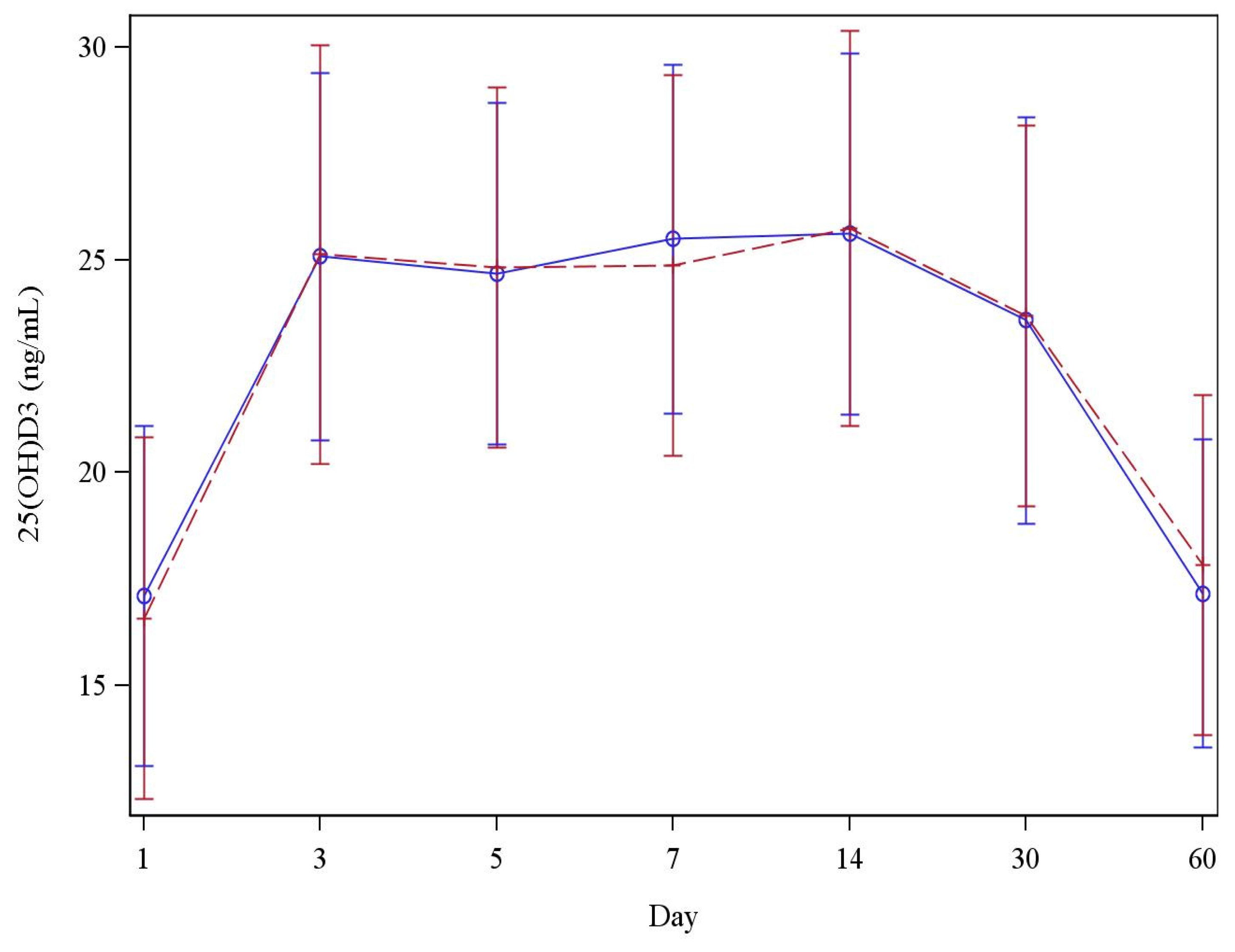
Evaluation of 25(OH)D3
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Yamshchikov, A.V.; Desai, N.S.; Blumberg, H.M.; Ziegler, T.R. Vitamin D for the treatment and prevention of infectious diseases: A systematic review of randomized controlled trials. Endocr. Pract. 2009, 5, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Judd, S.E.; Tangpricha, V. Vitamin D deficiency and risk for cardiovascular disease. Am. J. Med. Sci. 2009, 338, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Giovannucci, E.; Willett, W.C.; Dietrich, T.; Dawson-Hughes, B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am. J. Clin. Nutr. 2006, 84, 18–28. [Google Scholar] [PubMed]
- Holick, M. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Shab-Bidar, S.; Bours, S.; Geusens, P.; Kessel, G.H.; van den Bergh, J. Serum 25(OH)D response to vitamin D3 supplementation: A meta-regression analysis. Nutrition 2014, 30, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Bonham, A. A predictive equation to guide vitamin D replacement dose in patients. J. Am. Board Fam. Med. 2014, 27, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Raimundo, F.V.; Faulhaber, G.A.M.; Menegatti, P.K.; da Silva Marques, L.; Furlanetto, T.W. Effect of high- versus low-fat meal on serum 25- hydroxyvitamin D levels after a single dose of vitamin D: A single-blind, parallel, randomized trial. Int. J. Endocrinol. 2011, 2011, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Raimundo, F.V.; Lang, M.A.B.; Scopel, L.; Marcondes, N.A.; Araùjo, M.G.A.; Faulhaber, G.A.M.; Furlanetto, T.W. Effect of fat on serum 25-hydroxyvitamin D3 levels after a single oral dose of vitamin D in young healthy adults: A double-blind randomized placebo-controlled study. Eur. J. Nutr. 2014, 54, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, G.B.; Licata, A. Taking vitamin D with the largest meal improves absorption and results in higher serum levels of 25-hydroxyvitamin D3. J. Bone Miner. Res. 2010, 25, 928–930. [Google Scholar] [CrossRef] [PubMed]
- Niramitmahapanya, S.; Harris, S.S.; Dawson-Hughes, B. Type of dietary fat is associated with the 25-hydroxyvitamin D increment in response to vitamin D supplementation. J. Clin. Endocrinol. Metab. 2011, 96, 3170–3174. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Hughes, B.; Harris, S.S.; Lichtenstein, A.H.; Dolnikowsky, G.; Palermo, N.J. Dietary fat increases vitamin-D-3 Absorption. J. Acad. Diet. 2015, 115, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, R.; Tangpricha, V. Evaluation of vehicle substances on vitamin D bioavailability: A systematic review. Mol. Nutr. Food Res. 2010, 54, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Cavalier, E.; Lukas, P.; Crine, Y.; Peeters, S.; Carlisi, A.; Le Goff, C.; Gadisseur, R.; Delanaye, P.; Souberbielle, J.C. Evaluation of automated immunoassays for 25(OH)-vitamin D determination in different critical populations before and after standardization of the assays. Clin. Chim. Acta 2014, 431, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Cavalier, E.; Faché, W.; Souberbielle, J.C. A randomised, double-blinded, placebo-controlled, parallel study of vitamin D3 supplementation with different schemes based on multiples of 25,000 IU doses. Int. J. Endocrinol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Schleck, M.L.; Souberbielle, J.C.; Jandrain, B.; da Silva, S.; de Niet, S.; Vanderbist, F.; Scheen, A.; Cavalier, E. Randomized, double-blind, parallel study to evaluate the dose-response of three different vitamin D treatment schemes on the 25-Hydroxyvitamin D serum concentration in patients with Vitamin D deficiency. Nutrients 2015, 7, 5413–5422. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Composition | High-Fat Breakfast |
|---|---|
| Total fat | 52.7 g |
| Saturated fatty acid (SFA) | 11.4 g |
| Polyunsaturated fatty acid (PUFA) | 12.35 g |
| Monosaturated fatty acid (MUFA) | 24.25 g |
| Total carbohydrates | 48.72 g |
| Total protein | 28.95 g |
| Total calories | 782 kcal |
| Variables | All Subjects (n = 88) |
|---|---|
| Male, n (%) | 37 (42) |
| Female, n (%) | 51 (58) |
| Age, year, Mean ± SD | 31.3 ± 8.8 |
| min-max; median | 19.0–55.0; 28.0 |
| BMI, kg/m2, Mean ± SD | 22.3 ± 2.0 |
| min-max; median | 18.2–25.0; 22.2 |
| 25(OH)D3, ng/mL, Mean ± SD | 16.5 ± 2.3 |
| min-max; median | 11.0–20.0; 17.0 |
| Blood Sampling Day | Fasting (n = 88) | High Fat (n = 88) | ||
|---|---|---|---|---|
| Mean ± SD | Min–Max | Mean ± SD | Min–Max | |
| Baseline (day 1) | 17.1 ± 4.0 | 9.0–26.0 | 16.6 ± 4.2 | 6.0–26.0 |
| Day 3 | 25.1 ± 4.3 | 18.0–37.0 | 25.1 ± 4.9 | 14.0–40.0 |
| Day 5 | 24.7 ± 4.0 | 15.0–35.0 | 24.8 ± 4.2 | 15.0–35.0 |
| Day 7 | 25.5 ± 4.1 | 17.0–39.0 | 24.9 ± 4.5 | 16.0–37.0 |
| Day 14 | 25.6 ± 4.3 | 18.0–39.0 | 25.7 ± 4.6 | 16.0–37.0 |
| Day 30 | 23.6 ± 4.8 | 15.0–44.0 | 23.7 ± 4.5 | 14.0–35.0 |
| Day 30 | 17.2 ±3.6 | 11.0–26.0 | 17.8 ± 4.0 | 10.0–30.0 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavalier, E.; Jandrain, B.; Coffiner, M.; Da Silva, S.; De Niet, S.; Vanderbist, F.; Souberbielle, J.-C. A Randomised, Cross-Over Study to Estimate the Influence of Food on the 25-Hydroxyvitamin D3 Serum Level after Vitamin D3 Supplementation. Nutrients 2016, 8, 309. https://doi.org/10.3390/nu8050309
Cavalier E, Jandrain B, Coffiner M, Da Silva S, De Niet S, Vanderbist F, Souberbielle J-C. A Randomised, Cross-Over Study to Estimate the Influence of Food on the 25-Hydroxyvitamin D3 Serum Level after Vitamin D3 Supplementation. Nutrients. 2016; 8(5):309. https://doi.org/10.3390/nu8050309
Chicago/Turabian StyleCavalier, Etienne, Bernard Jandrain, Monte Coffiner, Stéphanie Da Silva, Sophie De Niet, Francis Vanderbist, and Jean-Claude Souberbielle. 2016. "A Randomised, Cross-Over Study to Estimate the Influence of Food on the 25-Hydroxyvitamin D3 Serum Level after Vitamin D3 Supplementation" Nutrients 8, no. 5: 309. https://doi.org/10.3390/nu8050309
APA StyleCavalier, E., Jandrain, B., Coffiner, M., Da Silva, S., De Niet, S., Vanderbist, F., & Souberbielle, J. -C. (2016). A Randomised, Cross-Over Study to Estimate the Influence of Food on the 25-Hydroxyvitamin D3 Serum Level after Vitamin D3 Supplementation. Nutrients, 8(5), 309. https://doi.org/10.3390/nu8050309