Innovations in Calculating Precise Nutrient Intake of Hospitalized Patients

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. The Computer Program
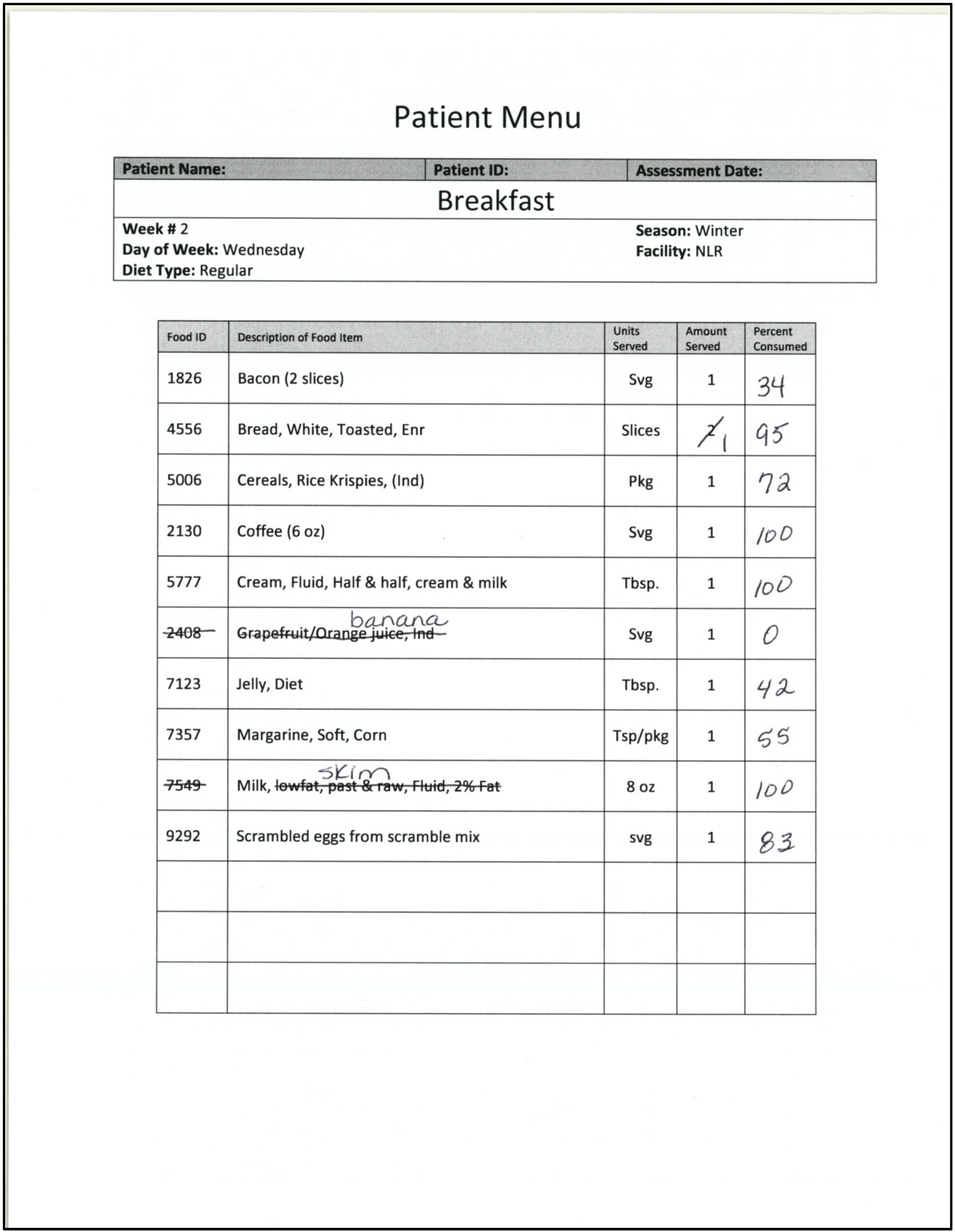
2.3. Direct Observation
2.4. Photography
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Tappenden, K.A.; Quatrara, B.; Parkhurst, M.L.; Malone, A.M.; Fanjiang, G.; Ziegler, T.R. Critical role of nutrition in improving quality of care: An interdisciplinary call to action to address adult hospital malnutrition. J. Aca. Nutr. Diet 2013, 113, 1219–1237. [Google Scholar] [CrossRef] [PubMed]
- Simmons, S.F.; Reuben, D. Nutritional intake monitoring for nursing home residents: A comparison of staff documentation, direct observation, and photography methods. J. Am. Geriatr. Soc. 2000, 48, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Boaz, M.; Rychani, L.; Barami, K.; Houri, Z.; Yosef, R.; Siag, A.; Berlovitz, Y.; Leibovitz, E. Nurses and nutrition: A survey of knowledge and attitudes regarding nutrition assessment and care of hospitalized elderly patients. J. Contin. Educ. Nurs. 2013, 44, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Kayser-Jones, J.; Schell, E.; Porter, C.; Paul, S. Reliability of percentage figures used to record the dietary intake of nursing home residents. Nurs. Home Med. 1997, 5, 69–76. [Google Scholar]
- Pokrywka, H.S.; Koffler, K.H.; Remsburg, R.; Bennett, R.G.; Roth, J.; Tayback, M.; Wright, J.E. Accuracy of patient care staff in estimating and documenting meal intake of nursing home residents. J. Am. Geriatr. Soc. 1997, 45, 1223–1227. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.H.; Patch, G.A.; Walls, R.C.; Lipschitz, D.A. Impact of nutrition status on morbidity and mortality in a select population of geriatric rehabilitation patients. Am. J. Clin. Nutr. 1990, 51, 749–758. [Google Scholar] [PubMed]
- Sullivan, D.H.; Walls, R.C.; Lipschitz, D.A. Protein-energy undernutrition and the risk of mortality within one year of hospital discharge in a select population of geriatric rehabilitation patients. Am. J. Clin. Nutr. 1991, 53, 599–605. [Google Scholar] [PubMed]
- Sullivan, D.H.; Walls, R.C. Impact of nutritional status on morbidity in a population of geriatric rehabilitation patients. J. Am. Geriatr. Soc. 1994, 42, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.L.; Compher, C.; Sullivan, D.H.; Mullin, G.E. Recognizing malnutrition in adults: Definitions and characteristics, screening, assessment, and team approach. J. Parenter. Enteral Nutr. 2013, 37, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.H.; Johnson, L.E.; Dennis, R.A.; Roberson, P.K.; Garner, K.K.; Padala, P.R.; Padala, K.P.; Bopp, M.M. Nutrient intake, peripheral edema, and weight change in elderly recuperative care patients. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Elwood, P.C.; Bird, G. A photographic method of diet evaluation. Hum. Nutr. Appl. Nutr. 1983, 37, 474–477. [Google Scholar] [PubMed]
- Bird, G.; Elwood, P.C. The dietary intakes of subjects estimated from photographs compared with a weighed record. Hum. Nutr. Appl. Nutr. 1983, 37, 470–473. [Google Scholar] [PubMed]
- Dahl, L. A.; Poulsen, S.; Ernst, L.; Kaae, A.K.; Biltoft-Jensen, A.; Tetens, I. Evaluation of a digital method to assess evening meal intake in a free-living adult population. Food Nutr. Res. 2010, 54, 2010. [Google Scholar]
- Lazarte, C.E.; Encinas, M.E.; Alegre, C.; Granfeldt, Y. Validation of digital photographs, as a tool in 24-h recall, for the improvement of dietary assessment among rural populations in developing countries. Nutr. J. 2012, 11, 61. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.K.; Nicklas, T.; Gunturk, B.; Correa, J.B.; Allen, H.R.; Champagne, C. Measuring food intake with digital photography. J. Hum. Nutr. Diet. 2014, 27, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Navarro, D.A.; Singer, P.; Leibovitz, E.; Krause, I.; Boaz, M. Inter- and intra-rater reliability of digitally captured images of plate waste. Nutr. Diet. 2014, 71, 284–288. [Google Scholar] [CrossRef]
- Nelson, M.; Atkinson, M.; Darbyshire, S. Food photography II: Use of food photographs for estimating portion size and the nutrient content of meals. Br. J. Nutr. 1996, 76, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Parent, M.; Niezgoda, H.; Keller, H.H.; Chambers, L.W.; Daly, S. Comparison of visual estimation methods for regular and modified textures: Real-time vs. digital imaging. J. Acad. Nutr. Diet. 2012, 112, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Robson, P.J.; Livingstone, M.B. An evaluation of food photographs as a tool for quantifying food and nutrient intakes. Public Health Nutr. 2000, 3, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.A.; Allen, H.R.; Martin, P.D.; Alfonso, A.; Gerald, B.; Hunt, A. Digital photography: A new method for estimating food intake in cafeteria settings. Eat. Weight Disord. 2004, 9, 24–28. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Agriculture. Composition of Foods Raw, Processed, Prepared USDA National Nutrient Database for Standard Reference; United States Department of Agriculture: Beltsville, MD, USA, 1992. [Google Scholar]
- Adams, C.F. Nutritive Value of American Foods in Common Units, 1st ed.; Agricultural Research Service United States Department of Agriculture: Washington, DC, USA, 1975. [Google Scholar]
- Sullivan, S.C.; Bopp, M.M.; Roberson, P.R.; Lensing, S.; Sullivan, D.H. Validation of an innovative method for calculating precise nutrient intake of hospitalized patients. Nutrients 2016, in press. [Google Scholar]


© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sullivan, S.C.; Bopp, M.M.; Weaver, D.L.; Sullivan, D.H. Innovations in Calculating Precise Nutrient Intake of Hospitalized Patients. Nutrients 2016, 8, 412. https://doi.org/10.3390/nu8070412
Sullivan SC, Bopp MM, Weaver DL, Sullivan DH. Innovations in Calculating Precise Nutrient Intake of Hospitalized Patients. Nutrients. 2016; 8(7):412. https://doi.org/10.3390/nu8070412
Chicago/Turabian StyleSullivan, Sheila Cox, Melinda M. Bopp, Dennis L. Weaver, and Dennis H. Sullivan. 2016. "Innovations in Calculating Precise Nutrient Intake of Hospitalized Patients" Nutrients 8, no. 7: 412. https://doi.org/10.3390/nu8070412
APA StyleSullivan, S. C., Bopp, M. M., Weaver, D. L., & Sullivan, D. H. (2016). Innovations in Calculating Precise Nutrient Intake of Hospitalized Patients. Nutrients, 8(7), 412. https://doi.org/10.3390/nu8070412