The Reproducibility and Relative Validity of a Mexican Diet Quality Index (ICDMx) for the Assessment of the Habitual Diet of Adults

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
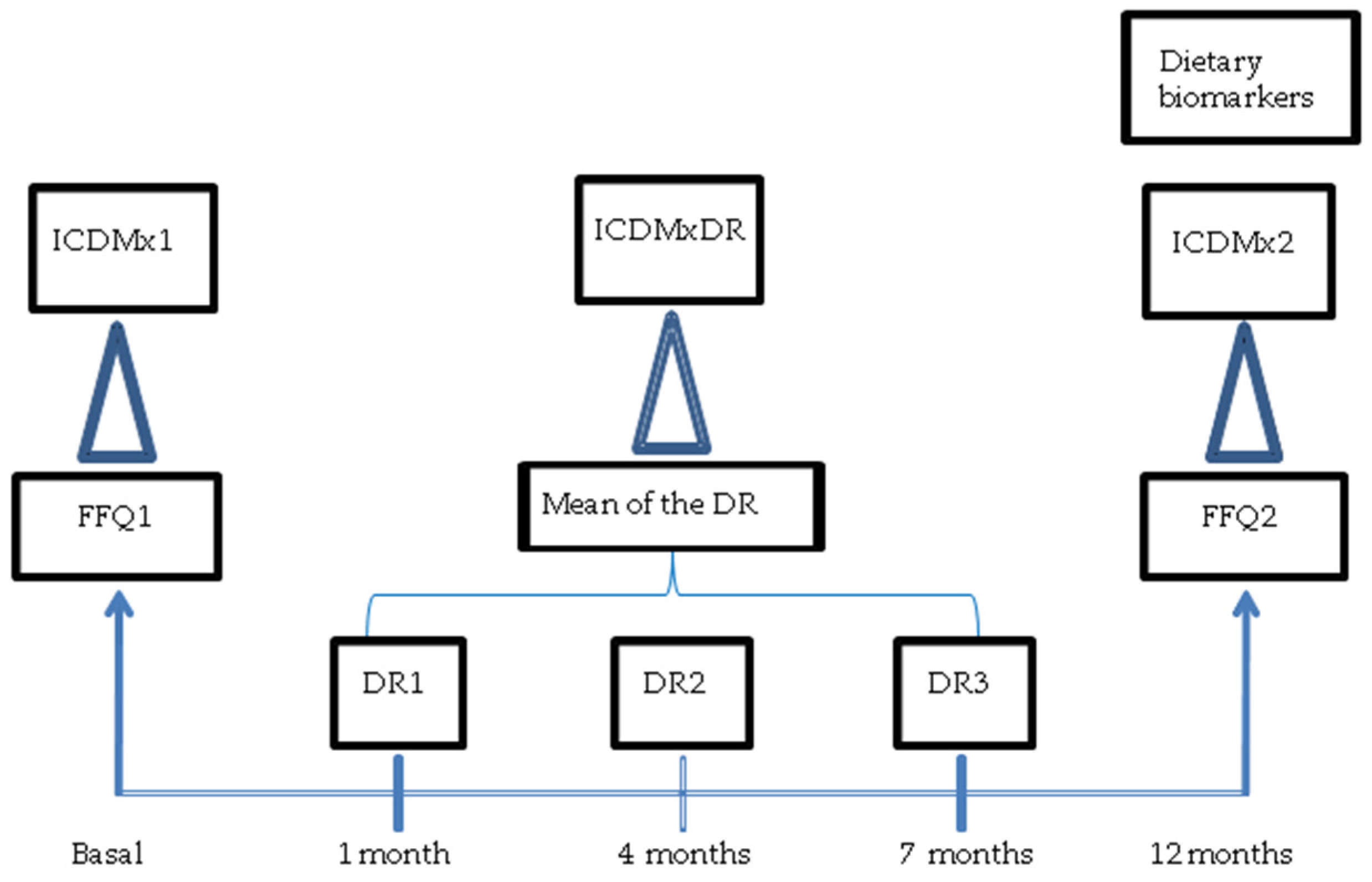
2.1. Study Population and Design
2.2. Design and Calculation of the ICDMx
2.3. Statistical Analysis
3. Results
3.1. Reproducibility of the ICDMx
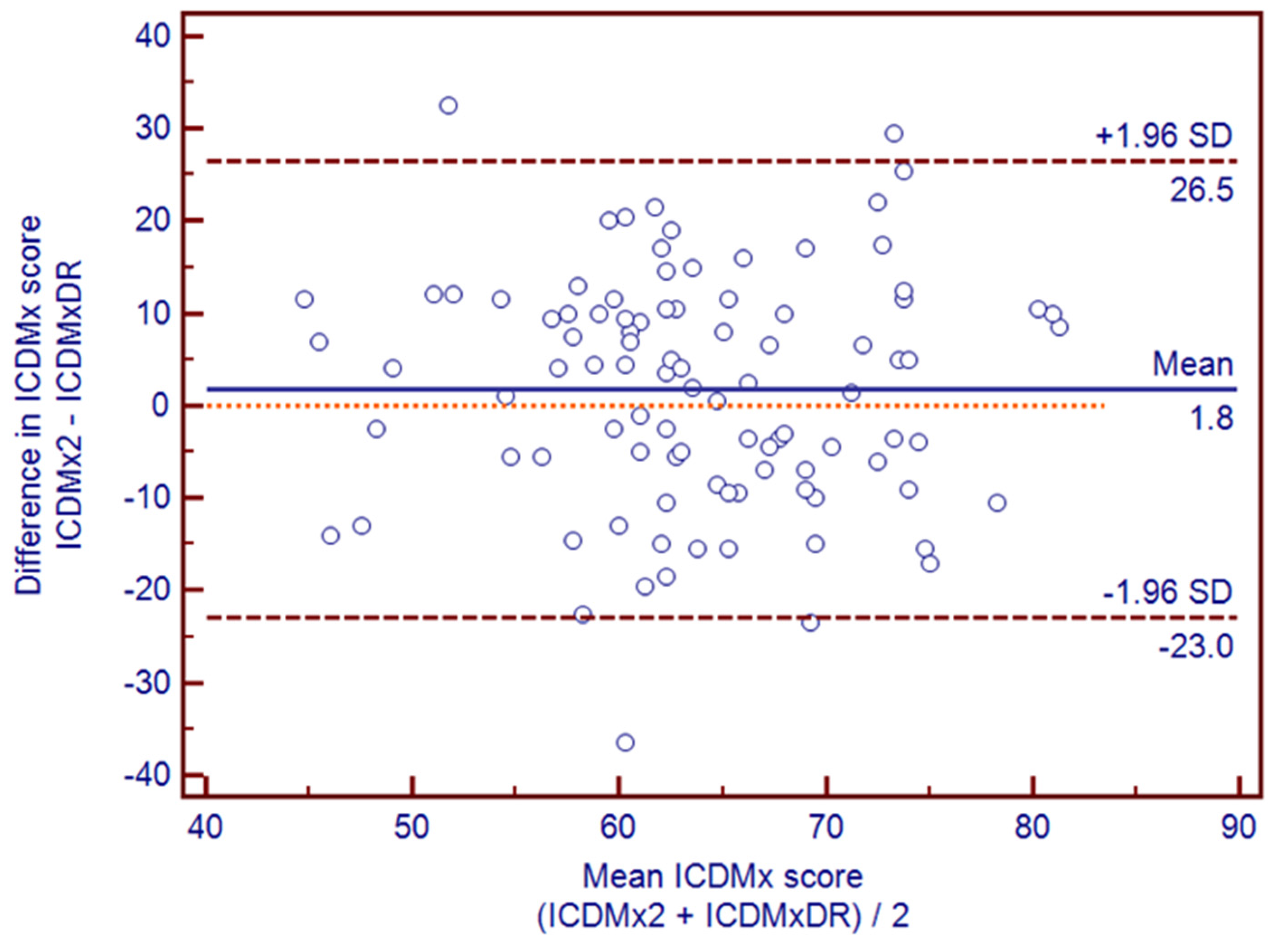
3.2. Relative Validity of ICDMx
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| DGI-CA | Dietary Guideline Index for Children and Adolescents |
| DQI-R | Revised Diet Quality Index |
| DRAI | Dietary Risk Assessment Index |
| DRs | Dietary Records |
| FFI | Food Frequency Index |
| FFQ | Food Frequency Questionnaire |
| HDL | High Density Lipoprotein |
| ICC | Intraclass Correlation Coefficients |
| ICDMx | Mexican Diet Quality Index |
| ICDMx1 | ICDMx from basal FFQ |
| ICDMx2 | ICDMx from second FFQ (1 year later) |
| ICDMxDR | ICDMx from DRs |
| IR | Intake Recommendations |
| LDL | Low Density Lipoprotein |
| MDS | Mediterranean Diet Score |
| NS | Not significant |
| US | United States |
References
- GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 5, 2287–2323. [Google Scholar]
- Patterson, R.; Pietinen, P. Evaluación del estado nutricional en individuos y poblaciones. In Nutrición y Salud Pública; Gibney, J., Margetts, B., Kearney, J., Arab, L., Eds.; Acribia: Zaragoza, Spain, 2006; pp. 73–91. [Google Scholar]
- Freisling, H.; Elmadfa, I.; Schuh, W.; Wagner, K.-H. Development and validation of a food frequency index using nutritional biomarkers in a sample of middle-aged and older adults. JHND 2009, 22, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Burrows, T.; Collins, C.E. Systematic review of diet quality indices and their associations with health-related outcomes in children and adolescents. J. Hum. Nutr. Diet. 2014, 27, 577–598. [Google Scholar] [CrossRef] [PubMed]
- Hendrie, G.A.; Viner Smith, E.; Golley, R.K. The reliability and relative validity of a diet index score for 4–11-year-old children derived from a parent-reported short food survey. Public Health Nutr. 2013, 17, 1486–1497. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.J.; Vogt, T.M.; Gerrior, S.A. Healthy Eating Index scores are associated with blood nutrient concentrations in the third National Health and Nutrition Examination Survey. J. Am. Diet. Assoc. 2004, 104, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Benitez-Arciniega, A.A.; Mendez, M.A.; Baena-Diez, J.M.; Schroder, H. Concurrent and construct validity of Mediterranean diet scores as assessed by an FFQ. Public Health Nutr. 2011, 14, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Torheim, L.E.; Barikmo, I.; Parr, C.L.; Hatløy, A.; Ouattara, F.; Oshaug, A. Validation of food variety as an indicator of diet quality assessed with a food frequency questionnaire for Western Mali. Eur. J. Clin. Nutr. 2003, 57, 1283–1291. [Google Scholar] [CrossRef] [PubMed]
- Jilcott, S.B.; Keyserling, T.C.; Samuel-Hodge, C.D.; Johnston, L.F.; Gross, M.D.; Ammerman, A.S. Validation of a brief dietary assessment to guide counseling for cardiovascular disease risk reduction in an underserved population. J. Am. Diet. Assoc. 2007, 107, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Burrows, T.L.; Rollo, M.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Hutchesson, M.J. The Comparative Validity and Reproducibility of a Diet Quality Index for Adults: The Australian Recommended Food Score. Nutrients 2015, 7, 785–798. [Google Scholar] [CrossRef] [PubMed]
- NOM-043-SSA2-2012, Servicios Básicos de Salud. Promoción y Educación Para la Salud en Materia Alimentaria. Criterios Para Brindar Orientación. Available online: http://www.dof.gob.mx/nota_detalle.php?codigo=5285372&fecha=22/01/2013 (accessed on 9 March 2015).
- Ponce, X.; Rodriguez-Ramirez, S.; Mundo-Rosas, V.; Shamah, T.; Barquera, S.; González de Cossio, T. Dietary quality indices vary with sociodemographic variables and anthropometric status among Mexican adults: A cross-sectional study. Results from the 2006 National Health and Nutrition Survey. Public Health Nutr. 2013, 17, 1717–1728. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M.; Reeve, B.B. Evaluation of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1854–1864. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Sampson, L.; Willett, W.C. The association between a nutritional quality index and risk of chronic disease. Am. J. Prev. Med. 2011, 40, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Funtikova, A.; Baena-Diez, J.M.; Koebnick, C.; Gomez, S.F.; Covas, M.I.; Goday, A.; Schröder, H. Validity of a short diet-quality index to predict changes in anthropometric and cardiovascular risk factors: A simulation study. Eur. J. Clin. Nutr. 2012, 66, 1369–1371. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Huang, Y.C.; Su, H.H.; Lee, M.-Z.; Wahlqvist, M.L. A simple food quality index predicts mortality in elderly Taiwanese. J. Nutr. Health Aging 2011, 15, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Hu, F.B.; Rimm, E.B.; Smith-Warner, S.A.; Feskanich, D.; Sampson, L.; Willett, W.C. Reproducibility and validity of the Diet Quality Index Revised as assessed by use of a food-frequency questionnaire. Am. J. Clin. Nutr. 2003, 78, 941–949. [Google Scholar] [PubMed]
- Macedo-Ojeda, G.; Vizmanos-Lamotte, B.; Marquez-Sandoval, Y.F.; Rodríguez-Rocha, N.P.; López-Uriarte, P.J.; Fernández-Ballart, J.D. Validation of a semi-quantitative food frequency questionnaire to assess food groups and nutrient intake. Nutr. Hosp. 2013, 28, 2212–2220. [Google Scholar] [PubMed]
- Willett, W.; Lenart, E. Reproducibility and validity of food-frequency questionnaires. In Nutritional Epidemiology, 3rd ed.; Willett, W., Ed.; Oxford University Press: New York, NY, USA, 2013; pp. 96–141. [Google Scholar]
- Burrows, T.L.; Williams, R.; Rollo, M.; Wood, L.; Garg, M.L.; Jensen, M.; Collins, C.E. Plasma carotenoid levels as biomarkers of dietary carotenoid consumption: A systematic review of the validation studies. JNIM 2015, 2, 15–64. [Google Scholar] [CrossRef]
- Valencia, M. Energía. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas. Energía, Proteínas, Lípidos, Hidratos de Carbono y Fibra; Bourges, H., Casanueva, E., Rosado, J.L., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2008; pp. 57–95. [Google Scholar]
- Rivera-Dommarco, J.; Hotz, C.; Rodríguez-Ramírez, S.; García-Guerra, A.; Pérez-Expósito, A.B.; Martínez, H.; González-Unzaga, M.A. Hierro. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas; Bourges, H., Casanueva, E., Rosado, J., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2005; pp. 245–264. [Google Scholar]
- DeSantiago, S.; Frenk, S.; Bourges, H. Calcio y Fosfato. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas; Bourges, H., Casanueva, E., Rosado, J., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2005; pp. 215–230. [Google Scholar]
- Rosado, J. Fibra Dietética. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas. Energía, Proteínas, Lípidos, Hidratos de Carbono Y Fibra; Bourges, H., Casanueva, E., Rosado, J.L., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2008; pp. 159–169. [Google Scholar]
- Recomendaciones para Población Mexicana. Consumo de Bebidas Para Una Vida Saludable. Available online: http://www.slan.org.mx/docs/bebidas.pdf (accessed on 9 March 2015).
- Bourges, H.; Casanueva, E.; Rosado, J. Apéndice 4. Distribución de sustratos energéticos. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas. Energía, Proteínas, Lípidos, Hidratos de Carbono y Fibra; Bourges, H., Casanueva, E., Rosado, J., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2008; p. 191. [Google Scholar]
- Aguilar-Salinas, C.A.; Kaufer-Horwitz, M. Lípidos. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas. Energía, Proteínas, Lípidos, Hidratos de Carbono y Fibra; Bourges, H., Casanueva, E., Rosado, J.L., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2008; pp. 127–143. [Google Scholar]
- Vega-Franco, L.; Iñárritu-Pérez, M. Hidratos de Carbono. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas. Energía, Proteínas, Lípidos, Hidratos de Carbono y Fibra; Bourges, H., Casanueva, E., Rosado, J.L., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2008; pp. 147–157. [Google Scholar]
- Dieta, Nutrición y Prevención de Enfermedades Crónicas. Informe de una Consulta Mixta de Expertos OMS/FAO Ginebra. Avaliable online: http://www.who.int/nutrition/publications/obesity/WHO_TRS_916_spa.pdf (accessed on 11 March 2015).
- Fundación Campo Educación y Salud. Programa cinco por día. Avaliable online: http://cincopordia.com.mx/wpcinco/ (accessed on 9 March 2015).
- Sánchez-Castillo, C.; López, P.; Pichardo-Ontiveros, E. Sodio, cloro y potasio. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas; Bourges, H., Casanueva, E., Rosado, J., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2005; pp. 193–214. [Google Scholar]
- Academy of Nutrition and Dietetics. International Dietetics & Nutrition Terminology (IDNT) Reference Manual, 4th ed.; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2013. [Google Scholar]
- Muller, R.; Buttner, P. A critical discussion of intraclass correlation coefficients. Stat. Med. 1994, 13, 2465–2476. [Google Scholar] [CrossRef] [PubMed]
- Beaton, G.H.; Milner, J.; Corey, P.; McGuire, V.; Cousins, M.; Stewart, E.; de Ramos, M.; Hewitt, D.; Grambsch, P.V.; Kassim, N.; et al. Sources of variance in 24-h dietary recall data: Implications for nutrition study design and interpretation. Am. J. Clin. Nutr. 1979, 32, 2546–2559. [Google Scholar] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S; discussion 1229S–1231S. [Google Scholar] [PubMed]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Daily Recommendation: Healthy Diet [11] | Components of the ICDMx (Maximum: 100 Points) | Scoring Criteria |
|---|---|---|
| Component 1. Sufficient (20 points) | ||
| Meets all nutritional needs, so that the adult subject has good nutrition and a healthy weight. | The diet covers 100% of energy requirements [21]. | >90% or <110% = 8 |
| >80%–90% or 110%–<120% = 7 | ||
| >70%–80% or 120%–<130% = 6 | ||
| >60%–70% or 130%–<140% = 5 | ||
| >50%–60% or 140%–<150% = 4 | ||
| >40%–50% or 150%–<160% = 3 | ||
| >30%–40% or 160%–<170% = 2 | ||
| >20%–30% or 170%–<180% = 1 | ||
| ≤20 or ≥180% = 0 | ||
| Iron intake of at least 21 mg for women or 15 mg for men [22], % RDA for age. | ≥100% = 3 | |
| 50%–<100% = 1.5 | ||
| <50% = 0 | ||
| Calcium intake of at least 1 g [23], % AI for age. | ≥100% = 3 | |
| 50%–<100% = 1.5 | ||
| <50% = 0 | ||
| Fiber intake of at least 30 g for women or 35 g for men [24], % nutritional recommendations. | ≥100% = 3 | |
| 50%–<100% = 1.5 | ||
| <50% = 0 | ||
| Water intake of at least 1500 mL [25]. | ≥1500 = 3 | |
| 1000–<1500 = 1.5 | ||
| <1000 = 0 | ||
| Component 2. Balanced (20 points) | ||
| Nutrients are consumed in balanced proportions with respect to total energy intake. | Proteins, 12%–15% of energy intake [26]. | 12%–15% = 7 |
| 10–<12% or >15%–19% = 3.5 | ||
| <10 or >19% = 0 | ||
| Lipids, 25%–<30% of energy intake [26,27]. | 25%–<30% = 7 | |
| 21%–<25% or 30%–33% = 3.5 | ||
| <21% or >33% = 0 | ||
| Carbohydrates, 55%–63% of energy intake [26,28]. | 55%–63% = 6 | |
| 51%–<55% or >63%–67% = 3 | ||
| <51% or >67% = 0 | ||
| Component 3. Complete (20 points) | ||
| Contains all nutrients. It is recommended to include foods from all three groups in each meal. | It includes at least 400 g from the vegetables and fruits group [29]. | ≥400 = 8 |
| 300–<400 = 6 | ||
| 200–<300 = 3 | ||
| <200 = 0 | ||
| It includes at least 200 g from the cereals group. | ≥200 = 6 | |
| 150–<200 = 4 | ||
| 100–<150 = 2 | ||
| <100 = 0 | ||
| It includes at least 120 g from the legumes and animal product group. | ≥120 = 6 | |
| 90–<120 = 4 | ||
| 60–<90 = 2 | ||
| <60 = 0 | ||
| Component 4. Varied (20 points) | ||
| Different foods from each group are consumed. This implies a variety of textures, colors, flavors, etc. | It includes at least four of five sub-groups (red, bluish-purple, yellowish-orange, green and white) from the vegetables and fruits group [30]. | 4 or 5 = 8 |
| 3 = 6 | ||
| 2 = 3 | ||
| <2 = 0 | ||
| It includes at least three of five sub-groups (wheat, rice, corn, whole grains and tubers) from the cereals group. | 3–5 = 6 | |
| 2 = 3 | ||
| <2 = 0 | ||
| It includes at least three of five sub-groups (legumes, poultry -including eggs-, red meat -beef and pork-, seafood, dairy products) from the legumes and animal product group. | 3–5 = 6 | |
| 2 = 3 | ||
| <2 = 0 | ||
| Component 5. Innocuous (20 points) | ||
| Its regular intake does not entail health risks because it is consumed in moderation. | Saturated fatty acids, ≤7% of energy intake [27]. | ≤7% = 5 |
| >7%–12% = 2.5 | ||
| >12% = 0 | ||
| Polyunsaturated fatty acids, 6%–10% of energy [27]. | 6%–10% = 5 | |
| >10%–15% or <6% = 2.5 | ||
| >15% = 0 | ||
| Sodium intake, 1600 mg [31]. | ≤1600 = 5 | |
| >1600–2600 = 2.5 | ||
| >2600 = 0 | ||
| Alcoholic drink intake, ≤14.4 g of ethanol (equivalent to 1 alcoholic drink) [32]. | ≤14.4 = 5 | |
| >14.4–21.6 = 2.5 | ||
| >21.6 = 0 |
| Participants (n = 97) | Non-Participants (n = 53) | |||
|---|---|---|---|---|
| Characteristics | n | % | n | % |
| Age 1 | 27.5 | 12.6 | 24.5 | 7.9 |
| BMI 1 | 24.1 | 4.1 | 24.2 | 3.1 |
| Gender 2 | ||||
| Male | 38 | 39.2 | 28 | 52.8 |
| Female | 59 | 60.8 | 25 | 47.2 |
| Physical activity 3 | ||||
| Sedentary | 43 | 44.3 | 27 | 50.9 |
| Active | 38 | 39.2 | 22 | 41.6 |
| Very active | 16 | 16.5 | 4 | 7.5 |
| Marital status 3 | ||||
| Single | 80 | 82.5 | 50 | 94.3 |
| Married | 16 | 16.5 | 3 | 5.7 |
| Divorced | 1 | 1.0 | 0 | 0 |
| Education 3 | ||||
| <10 years | 5 | 5.2 | 3 | 5.7 |
| ≥10 years | 92 | 94.8 | 50 | 94.3 |
| Occupation 3 | ||||
| Employee | 20 | 20.6 | 8 | 15.1 |
| Homemaker | 1 | 1.0 | 0 | 0 |
| Student | 72 | 74.2 | 45 | 84.9 |
| Unemployed | 4 | 4.1 | 0 | 0 |
| Component/Subcomponent | ICDMx1 | ICDMx2 | ICDMxDR | Reproducibility * | Validity * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Maximum | Mean | SD | Mean | SD | Mean | SD | r | ICC | r | ICC | |
| Component 1 Sufficient | 20 | 13.2 | 2.9 | 13.2 | 2.7 | 13.4 | 2.7 | 0.40 | 0.57 | 0.16 † | 0.28 |
| Adequate energy | 8 | 5.3 | 2.7 | 5.4 | 2.2 | 6.3 | 1.4 | 0.41 | 0.57 | −0.03 † | −0.06 † |
| Adequate iron | 3 | 2.4 | 0.8 | 2.3 | 0.8 | 2.1 | 0.8 | 0.47 | 0.63 | 0.39 | 0.57 |
| Adequate calcium | 3 | 2.4 | 0.9 | 2.2 | 0.9 | 1.9 | 0.9 | 0.58 | 0.74 | 0.41 | 0.59 |
| Adequate fiber | 3 | 1.5 | 1.0 | 1.4 | 1.1 | 1.1 | 0.9 | 0.54 | 0.69 | 0.27 | 0.42 |
| Water intake | 3 | 1.7 | 1.0 | 1.9 | 1.0 | 1.9 | 1.2 | 0.50 | 0.67 | 0.45 | 0.63 |
| Component 2 Balanced | 20 | 8.6 | 5.4 | 7.8 | 5.5 | 9.0 | 4.9 | 0.37 | 0.52 | 0.01 † | 0.08 † |
| Distribution of proteins | 7 | 4.8 | 2.2 | 4.7 | 2.2 | 3.0 | 2.0 | 0.20 | 0.33 | 0.28 | 0.45 |
| Distribution of lipids | 7 | 1.8 | 2.6 | 1.4 | 2.4 | 3.3 | 2.7 | 0.11 † | 0.23 † | −0.02 † | −0.15 † |
| Distribution of carbohydrates | 6 | 2.0 | 2.5 | 1.7 | 2.2 | 2.7 | 2.5 | 0.43 | 0.60 | 0.19 † | 0.33 |
| Component 3 Complete | 20 | 18.1 | 1.9 | 18.6 | 2.1 | 16.6 | 3.1 | 0.52 | 0.67 | 0.14 † | 0.22 † |
| Vegetables and fruits | 8 | 7.7 | 1.0 | 7.7 | 1.2 | 5.3 | 2.9 | 0.38 | 0.54 | 0.31 | 0.36 |
| Cereals | 6 | 5.3 | 1.4 | 5.0 | 1.7 | 5.6 | 0.9 | 0.56 | 0.71 | 0.38 | 0.50 |
| Legumes and AOF | 6 | 5.9 | 0.3 | 5.9 | 0.4 | 5.7 | 0.9 | 0.58 | 0.74 | 0.17 † | 0.22 † |
| Component 4 Varied | 20 | 14.1 | 3.6 | 13.4 | 3.9 | 10.7 | 4.5 | 0.49 | 0.66 | 0.17 † | 0.28 |
| Variety of vegetables and fruits | 8 | 6.4 | 2.2 | 6.3 | 2.2 | 2.7 | 2.7 | 0.40 | 0.57 | 0.31 | 0.47 |
| Variety of cereals | 6 | 2.4 | 2.1 | 2.3 | 2.0 | 3.2 | 2.2 | 0.39 | 0.56 | 0.21 | 0.35 |
| Variety of legumes and AOF | 6 | 5.3 | 1.4 | 4.8 | 2.0 | 4.7 | 1.9 | 0.51 | 0.65 | 0.21 | 0.35 |
| Component 5 Innocuous | 20 | 10.8 | 3.9 | 11.6 | 3.4 | 13.1 | 2.9 | 0.50 | 0.66 | 0.39 | 0.57 |
| SFA | 5 | 1.2 | 1.5 | 1.6 | 1.6 | 2.8 | 1.6 | 0.61 | 0.76 | 0.43 | 0.61 |
| PUFA | 5 | 3.3 | 1.6 | 3.3 | 1.4 | 3.3 | 1.2 | 0.30 | 0.46 | 0.05 † | 0.08 † |
| Sodium | 5 | 1.9 | 2.0 | 2.1 | 1.9 | 2.3 | 1.7 | 0.57 | 0.72 | 0.12 † | 0.26 |
| Alcohol | 5 | 4.5 | 1.5 | 4.6 | 1.2 | 4.8 | 0.9 | 0.78 | 0.87 | 0.65 | 0.79 |
| Total score of the ICDMx | 100 | 65.8 | 9.3 | 64.7 | 10.0 | 62.9 | 10.2 | 0.39 | 0.55 | 0.19 | 0.35 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macedo-Ojeda, G.; Márquez-Sandoval, F.; Fernández-Ballart, J.; Vizmanos, B. The Reproducibility and Relative Validity of a Mexican Diet Quality Index (ICDMx) for the Assessment of the Habitual Diet of Adults. Nutrients 2016, 8, 516. https://doi.org/10.3390/nu8090516
Macedo-Ojeda G, Márquez-Sandoval F, Fernández-Ballart J, Vizmanos B. The Reproducibility and Relative Validity of a Mexican Diet Quality Index (ICDMx) for the Assessment of the Habitual Diet of Adults. Nutrients. 2016; 8(9):516. https://doi.org/10.3390/nu8090516
Chicago/Turabian StyleMacedo-Ojeda, Gabriela, Fabiola Márquez-Sandoval, Joan Fernández-Ballart, and Barbara Vizmanos. 2016. "The Reproducibility and Relative Validity of a Mexican Diet Quality Index (ICDMx) for the Assessment of the Habitual Diet of Adults" Nutrients 8, no. 9: 516. https://doi.org/10.3390/nu8090516
APA StyleMacedo-Ojeda, G., Márquez-Sandoval, F., Fernández-Ballart, J., & Vizmanos, B. (2016). The Reproducibility and Relative Validity of a Mexican Diet Quality Index (ICDMx) for the Assessment of the Habitual Diet of Adults. Nutrients, 8(9), 516. https://doi.org/10.3390/nu8090516