Predictors Associated with Increase in Skeletal Muscle Mass after Sustained Virological Response in Chronic Hepatitis C Treated with Direct Acting Antivirals

Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients and Skeletal Muscle Mass Measurement
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
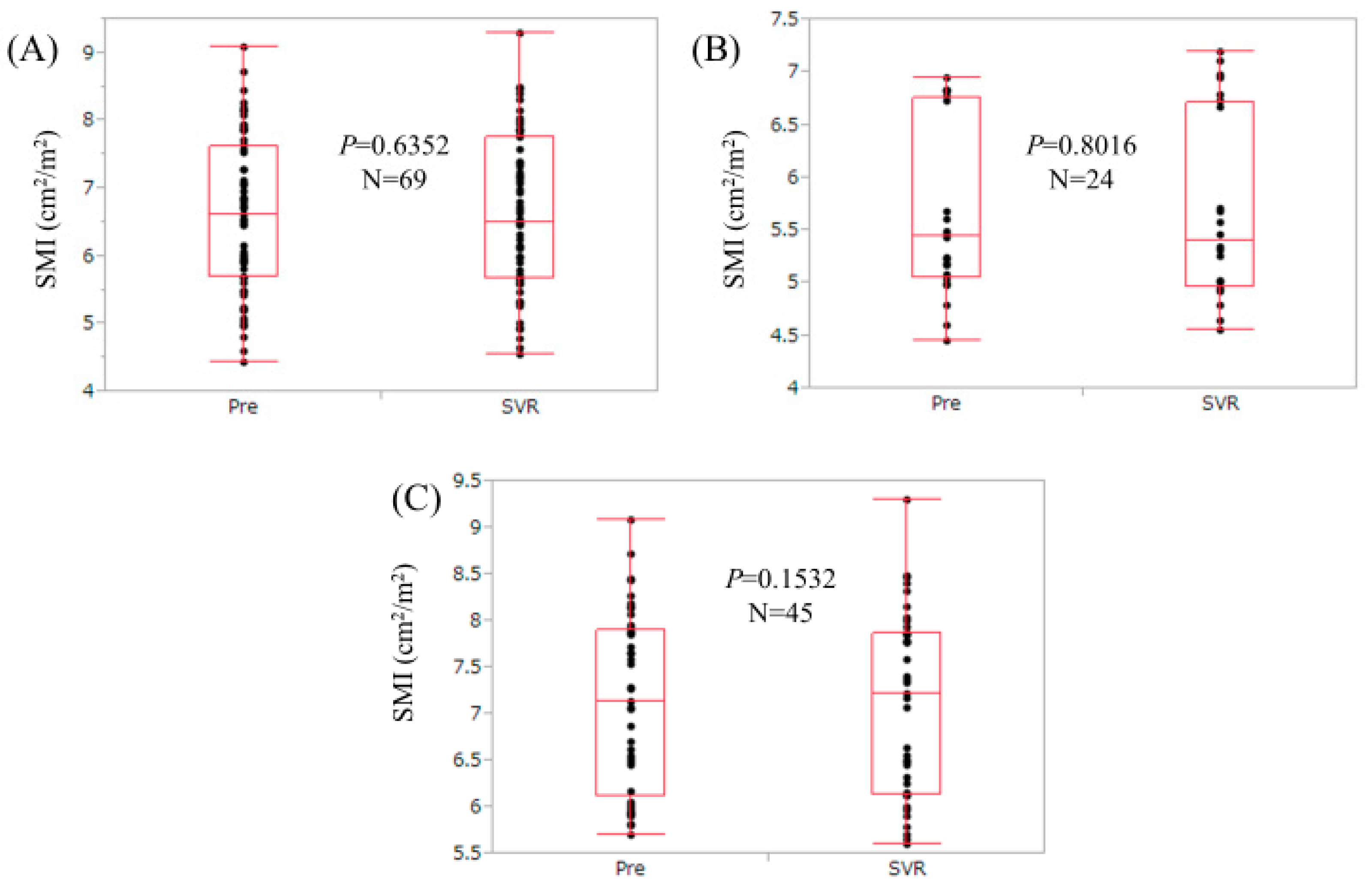
3.2. Changes in SMI for the Entire Cohort (n = 69)
3.3. Changes in SMI for Patients with Low Muscle Mass (Low SMI) at Baseline (n = 24)
3.4. Changes in SMI for Patients without Low Muscle Mass (Low SMI) at Baseline (n = 45)
3.5. Changes in SMI According to Baseline FIB-4 Index
3.6. Changes in SMI According to HCV Serotype
3.7. Changes in SMI According to HCV Viral Load
3.8. Changes in SMI According to Age
3.9. Comparison of Baseline Characteristics Between Patients with and without Increased SMI
3.10. Multivariate Analyses of Factors Linked to the Presence of Increased SMI
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CHC | chronic hepatitis C |
| HCV | hepatitis C virus |
| SVR | sustained virological response |
| DAA | direct acting antiviral |
| SMV | Simeprevir |
| Peg-IFN | pegylated interferon |
| RBV | Ribavirin |
| DCV | Daclatasvir |
| ASV | Asunaprevir |
| SOF | Sofosbuvir |
| LDV | Ledipasvir |
| SML | skeletal muscle loss |
| LC | liver cirrhosis |
| BIA | bio-impedance analysis |
| SMI | skeletal muscle index |
| BTR | branched-chain amino acid to tyrosine ratio |
References
- Wang, L.S.; D’Souza, L.S.; Jacobson, I.M. Hepatitis C—A clinical review. J. Med. Virol. 2016, 88, 1844–1855. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, A.J.; Berenguer, M. Reversion of disease manifestations after HCV eradication. J. Hepatol. 2016, 65, S95–S108. [Google Scholar] [CrossRef] [PubMed]
- Majumdar, A.; Kitson, M.T.; Roberts, S.K. Systematic review: Current concepts and challenges for the direct-acting antiviral era in hepatitis C cirrhosis. Aliment. Pharmacol. Ther. 2016, 43, 1276–1292. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, J.A.; Lawitz, E.J.; Poordad, F. Interferon-free, direct-acting antiviral therapy for chronic hepatitis C. J. Viral Hepat. 2015, 22, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, I.M. The HCV treatment revolution continues: Resistance considerations, pangenotypic efficacy, and advances in challenging populations. Gastroenterol. Hepatol. 2016, 12, 1–11. [Google Scholar]
- Welch, N.M.; Jensen, D.M. Pegylated interferon based therapy with second-wave direct-acting antivirals in genotype 1 chronic hepatitis C. Liver Int. 2015, 35, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Zeuzem, S.; Di Bisceglie, A.M.; Lim, J.K.; Pockros, P.J.; Frazier, L.M.; Kuo, A.; Lok, A.S.; Shiffman, M.L.; Ben Ari, Z. Effectiveness of ledipasvir-sofosbuvir combination in patients with hepatitis C virus infection and factors associated with sustained virologic response. Gastroenterology 2016, 151, 1131–1140. [Google Scholar] [CrossRef] [PubMed]
- Mir, F.; Kahveci, A.S.; Ibdah, J.A.; Tahan, V. Sofosbuvir/velpatasvir regimen promises an effective pan-genotypic hepatitis C virus cure. Drug Des. Dev. Ther. 2017, 11, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis-aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol. Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Petta, S.; Ciminnisi, S.; Di Marco, V.; Cabibi, D.; Cammà, C.; Licata, A.; Marchesini, G.; Craxì, A. Sarcopenia is associated with severe liver fibrosis in patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2016, 45, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S.; Merli, M. Sarcopenia from mechanism to diagnosis and treatment in liver disease. J. Hepatol. 2016, 65, 1232–1244. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S. Consilience in sarcopenia of cirrhosis. J. Cachexia Sarcopenia Muscle 2012, 3, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the international sarcopenia initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Lattanzi, B.; Torrisi, S.; Greco, F.; Farcomeni, A.; Gioia, S.; Merli, M.; Riggio, O. Sarcopenia is risk factor for development of hepatic encephalopathy after transjugular intrahepatic portosysthemic shunt placement. Clin. Gastroenterol. Hepatol. 2017, 15, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Kalafateli, M.; Mantzoukis, K.; Choi Yau, Y.; Mohammad, A.O.; Arora, S.; Rodrigues, S.; de Vos, M.; Papadimitriou, K.; Thorburn, D.; O’Beirnr, J. Malnutrition and sarcopenia predict post-liver transplantation outcomes independently of the Model for End-stage Liver Disease score. J. Cachexia Sarcopenia Muscle 2017, 8, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Michitaka, K.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; Yamago, H.; Suga, Y.; Tomida, H.; et al. Sarcopenia and two types of presarcopenia in Japanese patients with chronic liver disease. Eur. J. Gastroenterol. Hepatol. 2016, 28, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, L.; Cyrino, E.S.; Antunes, M.; Santos, D.A.; Sardinha, L.B. Sarcopenia and physical independence in older adults: The independent and synergic role of muscle mass and muscle function. J. Cachexia Sarcopenia Muscle 2017, 8, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Corriere, M.; Ferrucci, L. Age-related and disease-related muscle loss: The effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2014, 2, 819–829. [Google Scholar] [CrossRef]
- Kaido, T.; Tamai, Y.; Hamaguchi, Y.; Okumura, S.; Kobayashi, A.; Shirai, H.; Yagi, S.; Kamo, N.; Hammad, A.; Inagaki, N.; et al. Effects of pretransplant sarcopenia and sequential changes in sarcopenic parameters after living donor liver transplantation. Nutrition 2017, 33, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Giusto, M.; Lucidi, C.; Giannelli, V.; Pentassuglio, I.; Di Gregorio, V.; Lattanzi, B.; Riggio, O. Muscle depletion increases the risk of overt and minimal hepatic encephalopathy: Results of a prospective study. Metab. Brain Dis. 2013, 28, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Kalafateli, M.; Konstantakis, C.; Thomopoulos, K.; Triantos, C. Impact of muscle wasting on survival in patients with liver cirrhosis. World J. Gastroenterol. 2015, 21, 7357–7361. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Suzuki, K.; Koizumi, K.; Ichimura, H.; Oka, S.; Takada, H.; Kuwayama, H. Measurement of serum branched-chain amino acids to tyrosine ratio level is useful in a prediction of a change of serum albumin level in chronic liver disease. Hepatol. Res. 2008, 38, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Takata, R.; Hasegawa, K.; Nakano, C.; et al. Development of a simple predictive model for decreased skeletal muscle mass in patients with compensated chronic liver disease. Hepatol. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, F.; Matsumoto, Y.; Momoki, C.; Yuikawa, M.; Okada, G.; Hamakawa, E.; Kawamura, E.; Hagihara, A.; Toyama, M.; Fujii, H.; et al. Physical inactivity and insufficient dietary intake are associated with the frequency of sarcopenia in patients with compensated viral liver cirrhosis. Hepatol. Res. 2013, 43, 1264–1275. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Osaki, Y. Clinical significance of therapy using branched-chain amino acid granules in patients with liver cirrhosis and hepatocellular carcinoma. Hepatol. Res. 2014, 44, 149–158. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number or Median (Range) |
|---|---|
| Age (years) | 63 (25–83) |
| Gender, male/female | 31/38 |
| Body mass index (kg/m2) | 22.1 (15.7–32.8) |
| Skeletal muscle index (cm2/m2), male | 7.65 (6.73–9.08) |
| Skeletal muscle index (cm2/m2), female | 5.81 (4.45–7.27) |
| Total bilirubin (mg/dL) | 0.8 (0.3–3.0) |
| Serum albumin (g/dL) | 4.1 (2.8–4.9) |
| Prothrombin time (%) | 83.4 (61.1–119.4) |
| Platelets (×104/mm3) | 15.5 (3.3–27.8) |
| Serum sodium (mmol/L) | 140 (129–144) |
| eGFR (mL/min/1.73 m2) | 84 (33–142) |
| Total cholesterol (mg/dL) | 159 (110–234) |
| Triglyceride (mg/dL) | 88 (33–779) |
| AST (IU/L) | 37 (15–140) |
| ALT (IU/L) | 37 (11–155) |
| Fasting blood glucose (mg/dL) | 94 (74–187) |
| HbA1c (NSGP) | 5.5 (4.1–9.7) |
| BTR | 4.94 (2.13–9.09) |
| Alpha-fetoprotein (ng/mL) | 4.2 (1.3–224.9) |
| Hyaluronic acid (ng/mL) | 103 (9–699) |
| FIB-4 index | 2.46 (0.66–20.04) |
| HCV genotype, 1/2 | 55/14 |
| HCV viral load (log IU/L) | 6.2 (5.0–7.7) |
| Variables | I-SMI (n = 36) | Non-I-SMI (n = 33) | p Value |
|---|---|---|---|
| Age (years) | 59 (25–78) | 65 (39–83) | 0.0392 |
| Gender, male/female | 18/18 | 13/20 | 0.4693 |
| Serum albumin (g/dL) | 4.1 (3.3–4.9) | 4.1 (2.8–4.6) | 0.6883 |
| Total bilirubin (mg/dL) | 0.8 (0.3–2.5) | 0.7 (0.4–3.0) | 0.3416 |
| Prothrombin time (%) | 84.05 (67–108.4) | 82.8 (61.1–119.4) | 0.4161 |
| Platelet count (×104/mm3) | 17.35 (3.6–25.3) | 14.2 (3.3–27.8) | 0.3433 |
| AST (IU/L) | 29.5 (15–140) | 45 (19–120) | 0.2735 |
| ALT (IU/L) | 36.5 (11–155) | 39 (13–104) | 0.4971 |
| Serum sodium (mmol/L) | 140 (129–144) | 141 (135–143) | 0.7724 |
| Total cholesterol (mg/dL) | 158 (110–228) | 159 (126–234) | 0.5347 |
| Triglyceride (mg/dL) | 92 (33–174) | 88 (45–779) | 0.9091 |
| Fasting blood glucose (mg/dL) | 93 (74–187) | 96 (85–130) | 0.1224 |
| eGFR (mL/min/1.73 m2) | 85 (33–141) | 82 (36–142) | 0.8803 |
| HbA1c (NSGP) | 5.5 (4.7–9.7) | 5.5 (4.1–7.0) | 0.4911 |
| Body mass index (kg/m2) | 21.95 (15.7–30.8) | 22.5 (17.4–32.8) | 0.3988 |
| BTR | 5.16 (3.01–9.09) | 4.19 (2.13–8.36) | 0.0024 |
| Hyaluronic acid (ng/mL) | 80 (9–437) | 156 (17–699) | 0.0143 |
| FIB-4 index | 1.94 (0.66–20.04) | 3.53 (0.96–15.29) | 0.0656 |
| Alpha-fetoprotein (ng/mL) | 3.1 (1.9–224.9) | 7.3 (1.3–183.3) | 0.4694 |
| HCV genotype, 1/2 | 31/5 | 24/9 | 0.2331 |
| HCV-RNA (log IU/L) | 6.3 (5.1–7.2) | 6.2 (5.0–7.7) | 0.9380 |
| Variables | Multivariate Analysis | |
|---|---|---|
| OR (95% CI) | p Value | |
| Age (per one year) | 1.029 (0.977–1.089) | 0.2797 |
| Hyaluronic acid (per one ng/mL) | 1.002 (0.998–1.006) | 0.3794 |
| BTR (per one) | 0.648 (0.398–0.998) | 0.0488 |
| FIB-4 index (per one) | 0.996 (0.832–1.221) | 0.9688 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoh, K.; Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; et al. Predictors Associated with Increase in Skeletal Muscle Mass after Sustained Virological Response in Chronic Hepatitis C Treated with Direct Acting Antivirals. Nutrients 2017, 9, 1135. https://doi.org/10.3390/nu9101135
Yoh K, Nishikawa H, Enomoto H, Ishii A, Iwata Y, Miyamoto Y, Ishii N, Yuri Y, Hasegawa K, Nakano C, et al. Predictors Associated with Increase in Skeletal Muscle Mass after Sustained Virological Response in Chronic Hepatitis C Treated with Direct Acting Antivirals. Nutrients. 2017; 9(10):1135. https://doi.org/10.3390/nu9101135
Chicago/Turabian StyleYoh, Kazunori, Hiroki Nishikawa, Hirayuki Enomoto, Akio Ishii, Yoshinori Iwata, Yuho Miyamoto, Noriko Ishii, Yukihisa Yuri, Kunihiro Hasegawa, Chikage Nakano, and et al. 2017. "Predictors Associated with Increase in Skeletal Muscle Mass after Sustained Virological Response in Chronic Hepatitis C Treated with Direct Acting Antivirals" Nutrients 9, no. 10: 1135. https://doi.org/10.3390/nu9101135
APA StyleYoh, K., Nishikawa, H., Enomoto, H., Ishii, A., Iwata, Y., Miyamoto, Y., Ishii, N., Yuri, Y., Hasegawa, K., Nakano, C., Nishimura, T., Aizawa, N., Sakai, Y., Ikeda, N., Takashima, T., Takata, R., Iijima, H., & Nishiguchi, S. (2017). Predictors Associated with Increase in Skeletal Muscle Mass after Sustained Virological Response in Chronic Hepatitis C Treated with Direct Acting Antivirals. Nutrients, 9(10), 1135. https://doi.org/10.3390/nu9101135