Micronutrient Status in 153 Patients with Anorexia Nervosa

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Patients Selection
2.2. Clinical Data
2.3. Biological Data
2.4. Body Composition
2.5. Statistical Analysis
3. Results
3.1. Anthropometric Data
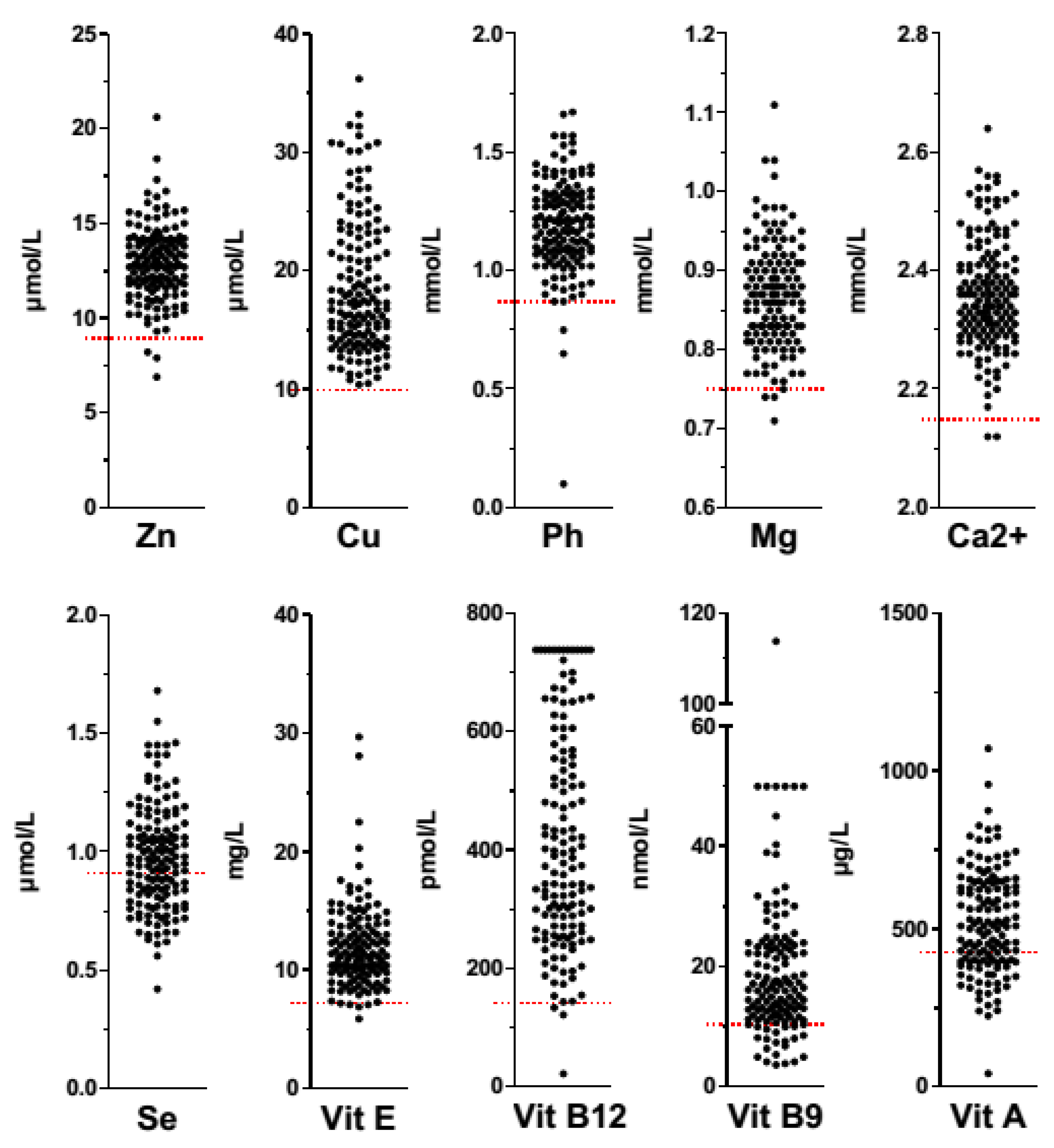
3.2. Biological Parameters
3.3. Body Composition
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Battle, D.E. Diagnostic and Statistical Manual of Mental Disorders (DSM). Codas 2013, 25, 191–192. [Google Scholar] [CrossRef] [PubMed]
- Smink, F.R.; van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 2013, 14, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.C.; Barraclough, B. Excess mortality of mental disorder. Br. J. Psychiatry 1998, 173, 11–53. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, D.; Pennacchio, H.; Bizeul, C.; Reveillard, V.; Verges, B. Outcome in AN adult patients: A 13-year follow-up in 484 patients. Diabetes Metab. 2011, 37, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Anderluh, M.B.; Tchanturia, K.; Rabe-Hesketh, S.; Treasure, J. Childhood obsessive-compulsive personality traits in adult women with eating disorders: Defining a broader eating disorder phenotype. Am. J. Psychiatry 2003, 160, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Godart, N.T.; Flament, M.F.; Lecrubier, Y.; Jeammet, P. Anxiety disorders in anorexia nervosa and bulimia nervosa: Co-morbidity and chronology of appearance. Eur. Psychiatry 2000, 15, 38–45. [Google Scholar] [CrossRef]
- Miller, K.K.; Grinspoon, S.K.; Ciampa, J.; Hier, J.; Herzog, D.; Klibanski, A. Medical findings in outpatients with anorexia nervosa. Arch. Intern. Med. 2005, 165, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Agh, T.; Kovacs, G.; Supina, D.; Pawaskar, M.; Herman, B.K.; Voko, Z.; Sheehan, D.V. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat. Weight Disord. 2016, 21, 353–364. [Google Scholar] [CrossRef] [PubMed]
- Fetissov, S.O.; Dechelotte, P. The new link between gut-brain axis and neuropsychiatric disorders. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Jean, A.; Conductier, G.; Manrique, C.; Bouras, C.; Berta, P.; Hen, R.; Charnay, Y.; Bockaert, J.; Compan, V. Anorexia induced by activation of serotonin 5-HT4 receptors is mediated by increases in CART in the nucleus accumbens. Proc. Natl. Acad. Sci. USA 2007, 104, 16335–16340. [Google Scholar] [CrossRef] [PubMed]
- Humphries, L.; Vivian, B.; Stuart, M.; McClain, C.J. Zinc deficiency and eating disorders. J. Clin. Psychiatry 1989, 50, 456–459. [Google Scholar] [PubMed]
- McClain, C.J.; Stuart, M.A.; Vivian, B.; McClain, M.; Talwalker, R.; Snelling, L.; Humphries, L. Zinc status before and after zinc supplementation of eating disorder patients. J. Am. Coll. Nutr. 1992, 11, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Casper, R.C.; Kirschner, B.; Sandstead, H.H.; Jacob, R.A.; Davis, J.M. An evaluation of trace metals, vitamins, and taste function in anorexia nervosa. Am. J. Clin. Nutr. 1980, 33, 1801–1808. [Google Scholar] [PubMed]
- Winston, A.P.; Jamieson, C.P.; Madira, W.; Gatward, N.M.; Palmer, R.L. Prevalence of thiamin deficiency in anorexia nervosa. Int. J. Eat. Disord. 2000, 28, 451–454. [Google Scholar] [CrossRef]
- Boland, B.; Beguin, C.; Zech, F.; Desager, J.P.; Lambert, M. Serum beta-carotene in anorexia nervosa patients: A case-control study. Int. J. Eat. Disord. 2001, 30, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Curran-Celentano, J.; Erdman, J.W., Jr.; Nelson, R.A.; Grater, S.J. Alterations in vitamin A and thyroid hormone status in anorexia nervosa and associated disorders. Am. J. Clin. Nutr. 1985, 42, 1183–1191. [Google Scholar] [PubMed]
- Mira, M.; Stewart, P.M.; Abraham, S.F. Vitamin and trace element status of women with disordered eating. Am. J. Clin. Nutr. 1989, 50, 940–944. [Google Scholar] [PubMed]
- Misra, M.; Stewart, P.M.; Abraham, S.F. Nutrient intake in community-dwelling adolescent girls with anorexia nervosa and in healthy adolescents. Am. J. Clin. Nutr. 2006, 84, 698–706. [Google Scholar] [PubMed]
- Sachs, K.; Andersen, D.; Sommer, J.; Winkelman, A.; Mehler, P.S. Avoiding medical complications during the refeeding of patients with anorexia nervosa. Eat. Disord. 2015, 23, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Solmi, M.; Veronese, N.; Luchini, C.; Manzato, E.; Sergi, G.; Favaro, A.; Santonastaso, P.; Correll, C.U. Oxidative Stress and Antioxidant Levels in Patients with Anorexia Nervosa after Oral Re-alimentation: A Systematic Review and Exploratory Meta-analysis. Eur. Eat. Disord. Rev. 2016, 24, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Verdich, C.; Barbe, P.; Petersen, M.; Grau, K.; Ward, L.; Macdonald, I.; Sorensen, T.I.; Oppert, J.M. Changes in body composition during weight loss in obese subjects in the NUGENOB study: Comparison of bioelectrical impedance vs. dual-energy X-ray absorptiometry. Diabetes Metab. 2011, 37, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Jesus, P.; Achamrah, N.; Grigioni, S.; Charles, J.; Rimbert, A.; Folope, V.; Petit, A.; Dechelotte, P.; Coeffier, M. Validity of predictive equations for resting energy expenditure according to the body mass index in a population of 1726 patients followed in a Nutrition Unit. Clin. Nutr. 2015, 34, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, V.; Gaudiani, J.L.; Mehler, P.S. Serum albumin levels may not correlate with weight status in severe anorexia nervosa. Eat. Disord. 2009, 17, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Nova, E.; Lopez-Vidriero, I.; Varela, P.; Toro, O.; Casas, J.J.; Marcos, A.A. Indicators of nutritional status in restricting-type anorexia nervosa patients: A 1-year follow-up study. Clin. Nutr. 2004, 23, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.; Robinson, P.H.; Fleck, A. Serum albumin distribution in early treated anorexia nervosa. Nutrition 1996, 12, 677–684. [Google Scholar] [CrossRef]
- Rigaud, D.; Sogni, P.; Hammel, P.; Melchior, J.C.; Angel, L.; Rozen, R.; Labarre, C.; Mignon, M.; Apfelbaum, M. Anorexia nervosa: Absence of sensitivity to nutritional protein markers. Study of 23 patients and comparison to a paired group with colonic Crohn’s disease. Ann. Med. Interne 1989, 140, 86–90. [Google Scholar]
- Caregaro, L.; Di Pascoli, L.; Favaro, A.; Nardi, M.; Santonastaso, P. Sodium depletion and hemoconcentration: Overlooked complications in patients with anorexia nervosa? Nutrition 2005, 21, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Waterlow, J.C. On serum albumin in anorexia nervosa. Nutrition 1996, 12, 720–721. [Google Scholar] [CrossRef]
- Hadigan, C.M.; Anderson, E.J.; Miller, K.K.; Hubbard, J.L.; Herzog, D.B.; Klibanski, A.; Grinspoon, S.K. Assessment of macronutrient and micronutrient intake in women with anorexia nervosa. Int. J. Eat. Disord. 2000, 28, 284–292. [Google Scholar] [CrossRef]
- Thibault, L.; Roberge, A.G. The nutritional status of subjects with anorexia nervosa. Int. J. Vitam. Nutr. Res. 1987, 57, 447–452. [Google Scholar] [PubMed]
- Duntas, L.H.; Benvenga, S. Selenium: An element for life. Endocrine 2015, 48, 756–775. [Google Scholar] [CrossRef] [PubMed]
- Agnello, E.; Malfi, G.; Costantino, A.M.; Massarenti, P.; Pugliese, M.; Fortunati, N.; Catalano, M.G.; Palmo, A. Tumour necrosis factor alpha and oxidative stress as maintaining factors in the evolution of anorexia nervosa. Eat. Weight Disord. 2012, 17, e194–e199. [Google Scholar] [CrossRef] [PubMed]
- Zenger, F.; Russmann, S.; Junker, E.; Wuthrich, C.; Bui, M.H.; Lauterburg, B.H. Decreased glutathione in patients with anorexia nervosa. Risk factor for toxic liver injury? Eur. J. Clin. Nutr. 2004, 58, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Moyano, D.; Sierra, C.; Brandi, N.; Artuch, R.; Mira, A.; Garcia-Tornel, S.; Vilaseca, M.A. Antioxidant status in anorexia nervosa. Int. J. Eat. Disord. 1999, 25, 99–103. [Google Scholar] [CrossRef]
- Smaga, I.; Niedzielska, E.; Gawlik, M.; Moniczewski, A.; Krzek, J.; Przegalinski, E.; Pera, J.; Filip, M. Oxidative stress as an etiological factor and a potential treatment target of psychiatric disorders. Part 2. Depression, anxiety, schizophrenia and autism. Pharmacol. Rep. 2015, 67, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Oliveras-Lopez, M.J.; Ruiz-Prieto, I.; Bolanos-Rios, P.; De la Cerda, F.; Martin, F.; Jauregui-Lobera, I. Antioxidant activity and nutritional status in anorexia nervosa: Effects of weight recovery. Nutrients 2015, 7, 2193–2208. [Google Scholar] [CrossRef] [PubMed]
- Roijen, S.B.; Worsaae, U.; Zlotnik, G. Zinc in patients with anorexia nervosa. Ugeskr. Laeger 1991, 153, 721–723. [Google Scholar] [PubMed]
- Bakan, R. The role of zinc in anorexia nervosa: Etiology and treatment. Med. Hypotheses 1979, 5, 731–736. [Google Scholar] [CrossRef]
- Shay, N.F.; Mangian, H.F. Neurobiology of zinc-influenced eating behavior. J. Nutr. 2000, 130, 1493S–1499S. [Google Scholar] [PubMed]
- Hambidge, K.M.; Hambidge, C.; Jacobs, M.; Baum, J.D. Low levels of zinc in hair, anorexia, poor growth, and hypogeusia in children. Pediatr. Res. 1972, 6, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Lask, B.; Fosson, A.; Rolfe, U.; Thomas, S. Zinc deficiency and childhood-onset anorexia nervosa. J. Clin. Psychiatry 1993, 54, 63–66. [Google Scholar] [PubMed]
- Yamaguchi, H.; Arita, Y.; Hara, Y.; Kimura, T.; Nawata, H. Anorexia nervosa responding to zinc supplementation: A case report. Gastroenterol. Jpn. 1992, 27, 554–558. [Google Scholar] [PubMed]
- Birmingham, C.L.; Goldner, E.M.; Bakan, R. Controlled trial of zinc supplementation in anorexia nervosa. Int. J. Eat. Disord. 1994, 15, 251–255. [Google Scholar] [PubMed]
- Suzuki, H.; Asakawa, A.; Li, J.B.; Tsai, M.; Amitani, H.; Ohinata, K.; Komai, M.; Inui, A. Zinc as an appetite stimulator—The possible role of zinc in the progression of diseases such as cachexia and sarcopenia. Recent Pat. Food Nutr. Agric. 2011, 3, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, C.L.; Gritzner, S. How does zinc supplementation benefit anorexia nervosa? Eat. Weight Disord. 2006, 11, e109–e111. [Google Scholar] [CrossRef] [PubMed]
- Seeger, G.; Braus, D.F.; Ruf, M.; Goldberger, U.; Schmidt, M.H. Body image distortion reveals amygdala activation in patients with anorexia nervosa—A functional magnetic resonance imaging study. Neurosci. Lett. 2002, 326, 25–28. [Google Scholar] [CrossRef]
- Takano, A.; Shiga, T.; Kitagawa, N.; Koyama, T.; Katoh, C.; Tsukamoto, E.; Tamaki, N. Abnormal neuronal network in anorexia nervosa studied with I-123-IMP SPECT. Psychiatry Res. 2001, 107, 45–50. [Google Scholar] [CrossRef]
- Divasta, A.D.; Feldman, H.A.; Brown, J.N.; Giancaterino, C.; Holick, M.F.; Gordon, C.M. Bioavailability of vitamin D in malnourished adolescents with anorexia nervosa. J. Clin. Endocrinol. Metab. 2011, 96, 2575–2580. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Vasantharajan, S. Vitamin status of eating disorder patients: Relationship to clinical indices and effect of treatment. Int. J. Eat. Disord. 1995, 18, 257–262. [Google Scholar] [CrossRef]
- Castro, J.; Deulofeu, R.; Gila, A.; Puig, J.; Toro, J. Persistence of nutritional deficiencies after short-term weight recovery in adolescents with anorexia nervosa. Int. J. Eat. Disord. 2004, 35, 169–178. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| AN-R (n = 91) | AN-BP (n = 62) | t-Test (p) | |
|---|---|---|---|
| Mean age (years) | 29.42 ± 11.4 | 27.1 ± 10.4 | NS |
| Disease duration (years) | 6.8 ± 7.6 | 8.4 ± 9.3 | NS |
| BMI (kg/m2) | 16.5 ± 2 | 18.8 ± 3.0 | <0.05 |
| FM (%) | 18.7 ± 6.5 | 20.8 ± 5.9 | p = 0.054 |
| FFM (%) | 80.6 ± 8.9 | 76.9 ± 12.6 | <0.05 |
| Mean Values | AN-R | AN-BP | t-Test (p) | |
|---|---|---|---|---|
| Zn (9–17 µmol/L) | 12.8 ± 1.9 | 13.04 ± 2.03 | 12.6 ± 1.7 | NS |
| Cu (10–40 µmol/) | 18.76 ± 5.8 | 18.40 ± 5.9 | 19.36 ± 5.5 | NS |
| Ph (0.87–1.50 mmol/L) | 1.19 ± 0.2 | 1.20 ± 0.17 | 1.17 ± 0.23 | NS |
| Mg (0.75–1 mmol/L) | 0.86 ± 0.64 | 0.87 ± 0.60 | 0.85 ± 0.72 | NS |
| Ca2+ (2.15–2.55 mmol/L) | 2.36 ± 0.92 | 2.35 ± 0.91 | 2.37 ± 0.09 | NS |
| Se (0.90–1.65 µmol/L) | 0.97 ± 0.21 | 0.99 ± 0.23 | 0.93 ± 0.18 | NS |
| Vit E (7–17 mg/L) | 11.89 ± 3.51 | 11.4 ± 3.07 | 12.68 ± 4.02 | <0.05 |
| B12 (141–489 pmol/L) | 413.1 ± 193.1 | 426.3 ± 183.0 | 391.46 ± 177.7 | NS |
| B9 (10.4–42.4 nmol/L) | 19.42 ± 13.07 | 19.45 ± 10.59 | 19.38 ± 16.40 | NS |
| Vit A (430–800 µg/L) | 521.6 ± 164.6 | 511.6 ± 152.4 | 537.5 ± 182.7 | NS |
| Deficiency % (n) | AN-R % (n) | AN-BP % (n) | p (Chi2) | |
|---|---|---|---|---|
| Zn (9–17 µmol/L) | 2.1 (3) | 2.2 (2) | 1.9 (1) | NS |
| Cu (10–40 µmol/L) | 0 (0) | 0 (0) | 0 (0) | - |
| Ph (0.87–1.50 mmol/L) | 3.5 (5) | 3.5 (3) | 3.6 (2) | NS |
| Mg (0.75–1 mmol/L) | 3.0 (4) | 1.2 (1) | 6.0 (3) | NS |
| Ca2+ (2.15–2.55 mmol/L) | 1.3 (2) | 1.1 (1) | 1.7 (1) | NS |
| Se (0.90–1.65 µmol/L) | 40.6 (58) | 40.0 (36) | 41.5 (22) | NS |
| Vit E (7–17 mg/L) | 1.5 (2) | 1.2 (1) | 1.9 (1) | NS |
| B12 (141–489 pmol/L) | 2.2 (3) | 2.4 (2) | 1.9 (1) | NS |
| B9 (10.4–42.4 nmol/L) | 15.9 (22) | 14.1 (12) | 18.9 (10) | NS |
| Vit A (430–800 µg/L) | 32.8 (45) | 35.7 (30) | 28.3 (15) | NS |
| At least one oligoelement deficiency | 43.7 (55) | 43.0 (34) | 44.7 (21) | NS |
| At least one vitamin deficiency | 45.7 (59) | 46.9 (38) | 43.8 (21) | NS |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Achamrah, N.; Coëffier, M.; Rimbert, A.; Charles, J.; Folope, V.; Petit, A.; Déchelotte, P.; Grigioni, S. Micronutrient Status in 153 Patients with Anorexia Nervosa. Nutrients 2017, 9, 225. https://doi.org/10.3390/nu9030225
Achamrah N, Coëffier M, Rimbert A, Charles J, Folope V, Petit A, Déchelotte P, Grigioni S. Micronutrient Status in 153 Patients with Anorexia Nervosa. Nutrients. 2017; 9(3):225. https://doi.org/10.3390/nu9030225
Chicago/Turabian StyleAchamrah, Najate, Moïse Coëffier, Agnès Rimbert, Jocelyne Charles, Vanessa Folope, André Petit, Pierre Déchelotte, and Sébastien Grigioni. 2017. "Micronutrient Status in 153 Patients with Anorexia Nervosa" Nutrients 9, no. 3: 225. https://doi.org/10.3390/nu9030225
APA StyleAchamrah, N., Coëffier, M., Rimbert, A., Charles, J., Folope, V., Petit, A., Déchelotte, P., & Grigioni, S. (2017). Micronutrient Status in 153 Patients with Anorexia Nervosa. Nutrients, 9(3), 225. https://doi.org/10.3390/nu9030225