Ethnic Variability in Glycemic Response to Sucrose and Isomaltulose


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Protocol
2.3. Statistical Analysis
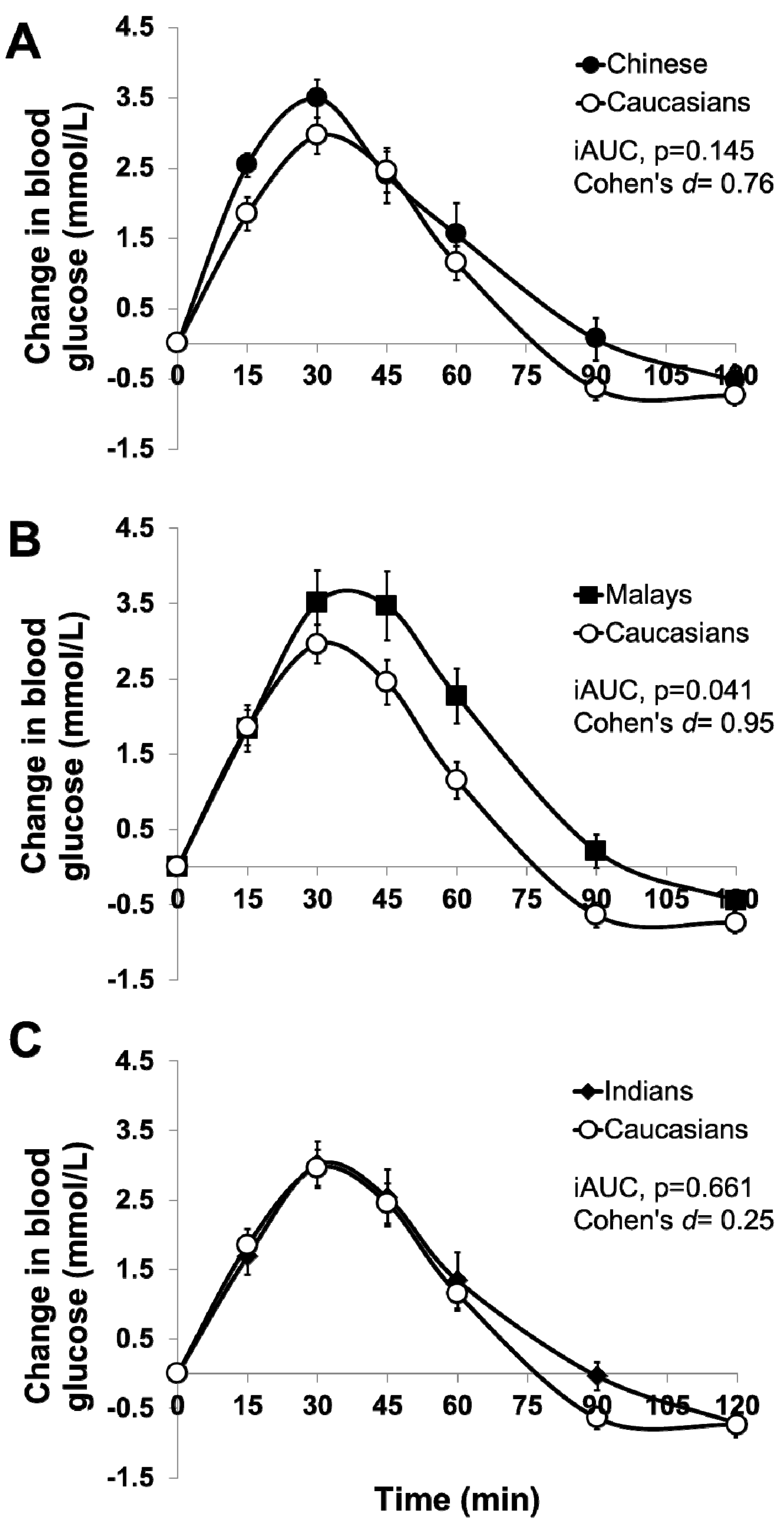
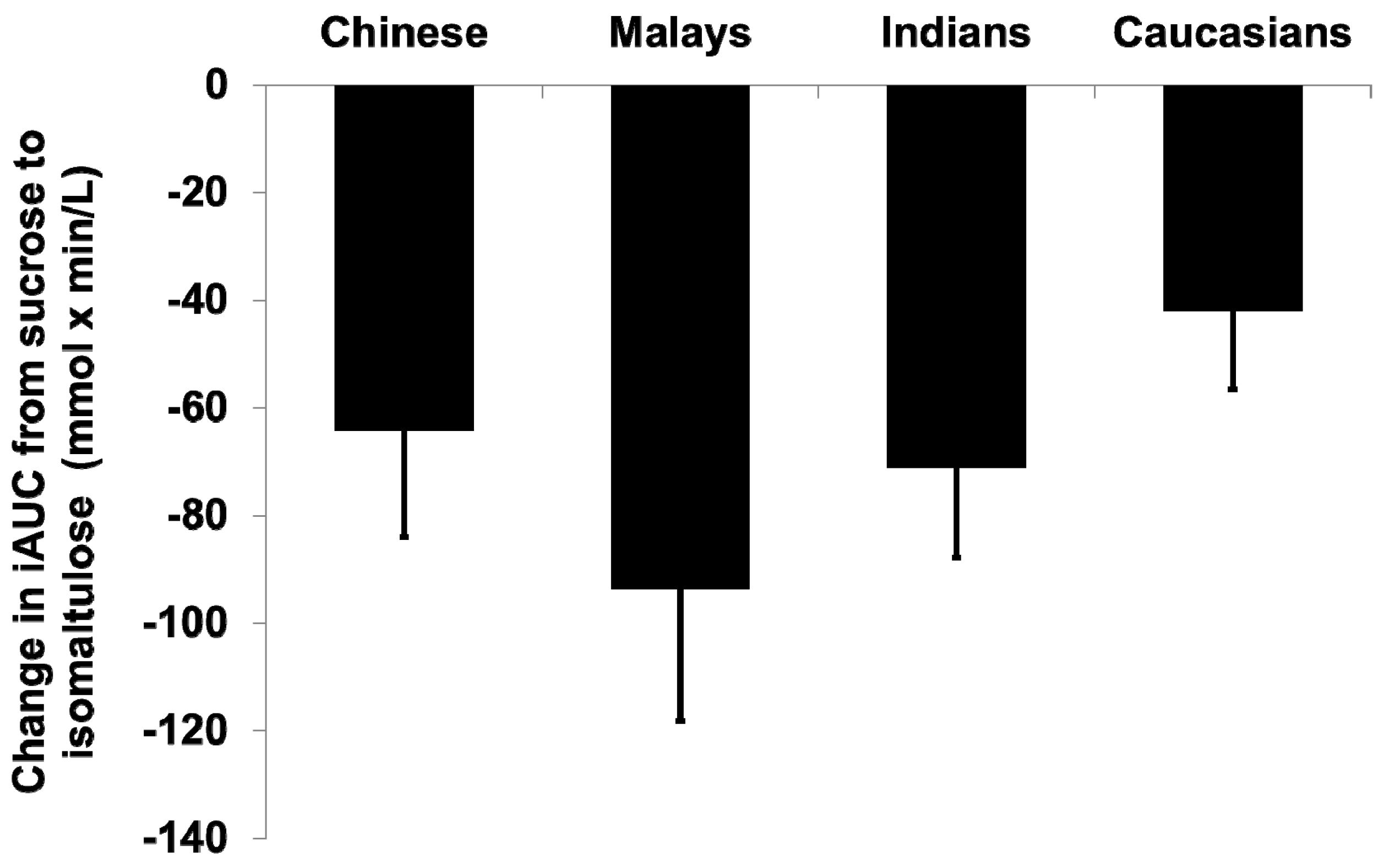
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Stratton, I.M.; Adler, A.I.; Neil, H.A.W.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. Br. Med. J. 2000, 321, 405–412. [Google Scholar] [CrossRef]
- Brand-Miller, J.; Hayne, S.; Petocz, P.; Colagiuri, S. Low-glycemic index diets in the management of diabetes. A meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef] [PubMed]
- National Health Survey 2010. Available online: https://www.moh.gov.sg/content/moh_web/home/Publications/Reports/2011/national_health_survey2010.html (accessed on 2 March 2017).
- Dickinson, S.; Colagiuri, S.; Faramus, E.; Petocz, P.; Brand-Miller, J.C. Postprandial hyperglycemia and insulin sensitivity differ among lean young adults of different ethnicities. J. Nutr. 2002, 132, 2574–2579. [Google Scholar] [PubMed]
- Henry, C.J.; Lightowler, H.J.; Newens, K.; Sudha, V.; Radhika, G.; Sathya, R.M.; Mohan, V. Glycaemic index of common foods tested in the UK and India. Br. J. Nutr. 2008, 99, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Venn, B.S.; Williams, S.M.; Mann, J.I. Comparison of postprandial glycaemia in Asians and Caucasians. Diabet. Med. 2010, 27, 1205–1208. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Snehalatha, C.; Shetty, A.S.; Nanditha, A. Trends in prevalence of diabetes in Asian countries. World J. Diabetes 2012, 3, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Mather, H.M.; Keen, H. The southall diabetes survey: Prevalence of known diabetes in Asians and Europeans. Br. Med. J. 1985, 291, 1081–1084. [Google Scholar] [CrossRef]
- Schulze, M.B.; Liu, S.; Rimm, E.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Glycemic index, glycemic load, and dietary fiber intake and incidence of type 2 diabetes in younger and middle-aged women. Am. J. Clin. Nutr. 2004, 80, 348–356. [Google Scholar] [PubMed]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J.H. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S. The glycemic index: Physiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA 2002, 287, 2414–2423. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. Postprandial hyperglycemia and diabetes complications. Is it time to treat? Diabetes 2005, 54, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Yoshikawa, H.; Murayama, Y.; Okuda, Y.; Yamashita, K. Usefulness of palatinose as a caloric sweetener for diabetic patients. Horm. Metab. Res. 1989, 21, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Bharath Kumar, S.; Prabhasankar, P. Low glycemic index ingredients and modified starches in wheat based food processing: A review. Trends Food Sci. Technol. 2014, 35, 32–41. [Google Scholar] [CrossRef]
- Holub, I.; Gostner, A.; Theis, S.; Nosek, L.; Kudlich, T.; Melcher, R.; Scheppach, W. Novel findings on the metabolic effects of the low glycaemic carbohydrate isomaltulose (palatinose™). Br. J. Nutr. 2010, 103, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Lina, B.A.R.; Jonker, D.; Kozianowski, G. Isomaltulose (palatinose®): A review of biological and toxicological studies. Food Chem. Toxicol. 2002, 40, 1375–1381. [Google Scholar] [CrossRef]
- Van Can, J.G.; van Loon, L.J.; Brouns, F.; Blaak, E.E. Reduced glycaemic and insulinaemic responses following trehalose and isomaltulose ingestion: Implications for postprandial substrate use in impaired glucose-tolerant subjects. Br. J. Nutr. 2012, 108, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Brouns, F.; Bjorck, I.; Frayn, K.N.; Gibbs, A.L.; Lang, V.; Slama, G.; Wolever, T.M.S. Glycaemic index methodology. Nutr. Res. Rev. 2005, 18, 145–171. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization; World Health Organization. Carbohydrates in Human Nutrition: Report of a Joint FAO/WHO Expert Consultation; FAO: Rome, Italy, 1998. [Google Scholar]
- Tan, V.M.; Wu, T.; Henry, C.J.; Lee, Y.S. Glycaemic and insulin responses, glycaemic index and insulinaemic index values of rice between three Asian ethnic groups. Br. J. Nutr. 2015, 113, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Rajadhyaksha, A.; Rodriguez, M.; Nichols, J.H. Evaluation of the hemocue glucose 201 room temperature microcuvettes. Point Care 2008, 7, 12–15. [Google Scholar] [CrossRef]
- Tey, S.L.; Van Helvoort, A.; Henry, C.J. Glycaemic responses to liquid food supplements among three Asian ethnic groups. Eur. J. Nutr. 2016, 55, 2493–2498. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Kuenen, J.; Borg, R.; Zheng, H.; Schoenfeld, D.; Heine, R.J. Translating the a1c assay into estimated average glucose values. Diabetes care 2008, 31, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Board. Report of the National Nutrition Survey 2010, Singapore; Health Promotion Board: Singapore, 2013. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Chinese (n = 10) | Malays (n = 10) | Indians (n = 10) | Caucasians (n = 10) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 24.2 (3.9) | 25.8 (4.3) | 23.6 (2.1) | 27.5 (5.2) | 0.150 |
| Weight (kg) | 59.8 (8.2) | 61.3 (13.7) | 67.1 (9.3) | 70.6 (10.9) | 0.104 |
| Height (cm) | 1.67 (0.1) | 1.62 (0.1) | 1.67 (0.1) | 1.73 (0.1) | 0.047 * |
| Body mass index (kg/m2) | 21.3 (1.3) | 23.0 (3.2) | 24.1 (3.0) | 23.6 (2.7) | 0.105 |
| Systolic blood pressure (mmHg) | 107.6 (7.7) | 110.4 (10.1) | 110.7 (7.0) | 117.6 (8.2) | 0.071 |
| Diastolic blood pressure (mmHg) | 71.4 (5.5) | 70.0 (12.1) | 69.4 (7.2) | 70.9 (6.6) | 0.946 |
| Mean fasting blood glucose (mmol/L) | 4.7 (0.3) | 4.5 (0.4) | 4.4 (0.5) | 4.8 (0.4) | 0.181 |
| Waist circumference (cm) | 71.4 (5.8) | 72.2 (10.1) | 76.1 (7.9) | 76.9 (8.8) | 0.366 |
| Hip circumference (cm) | 93.6 (4.7) | 95.8 (5.2) | 98.7 (6.5) | 97.2 (7.7) | 0.305 |
| Ethnicity | iAUC Glucose (mmol × min/L) | Difference | p-Value | |
|---|---|---|---|---|
| Sucrose (50 g) | Isomaltulose (50 g) | |||
| All (n = 40) | 160.1 (67.5) | 92.4 (42.6) | −67.7 (61.5) | <0.001 |
| Chinese (n = 10) | 174.1 (69.6) | 109.9 (27.6) | −64.1 (62.8) | 0.010 |
| Malays (n = 10) | 192.4 (82.6) a | 98.8 (52.0) | −93.6 (77.9) | 0.004 |
| Indians (n = 10) | 143.4 (60.8) | 72.3 (31.4) | −71.2 (52.9) | 0.002 |
| Caucasians (n = 10) | 130.5 (41.3) a | 88.4 (50.7) | −42.1 (45.7) | 0.017 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, W.S.K.; Tan, S.-Y.; Henry, C.J. Ethnic Variability in Glycemic Response to Sucrose and Isomaltulose. Nutrients 2017, 9, 347. https://doi.org/10.3390/nu9040347
Tan WSK, Tan S-Y, Henry CJ. Ethnic Variability in Glycemic Response to Sucrose and Isomaltulose. Nutrients. 2017; 9(4):347. https://doi.org/10.3390/nu9040347
Chicago/Turabian StyleTan, Wei Shuan Kimberly, Sze-Yen Tan, and Christiani Jeyakumar Henry. 2017. "Ethnic Variability in Glycemic Response to Sucrose and Isomaltulose" Nutrients 9, no. 4: 347. https://doi.org/10.3390/nu9040347
APA StyleTan, W. S. K., Tan, S. -Y., & Henry, C. J. (2017). Ethnic Variability in Glycemic Response to Sucrose and Isomaltulose. Nutrients, 9(4), 347. https://doi.org/10.3390/nu9040347