Novel Treatment Strategy for Patients with Venom-Induced Consumptive Coagulopathy from a Pit Viper Bite




{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Characteristics of Envenomation by a Pit Viper
3. VICC
3.1. Pathophysiology of VICC
3.2. Clinical Manifestation of VICC
3.3. Diagnosis of VICC
3.3.1. Limitations of Traditional Coagulation Tests
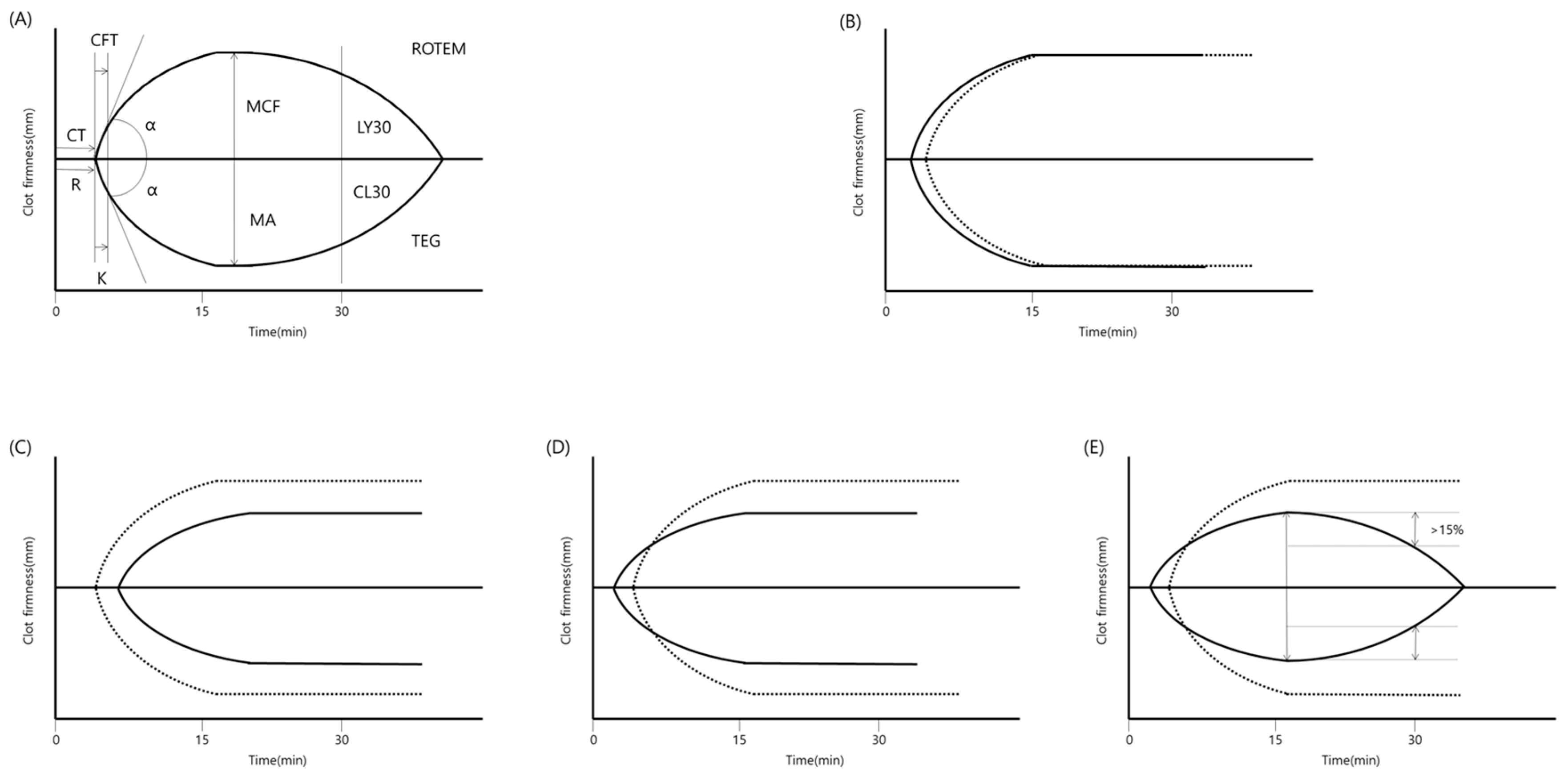
3.3.2. Thromboelastography
3.3.3. Immunological Test
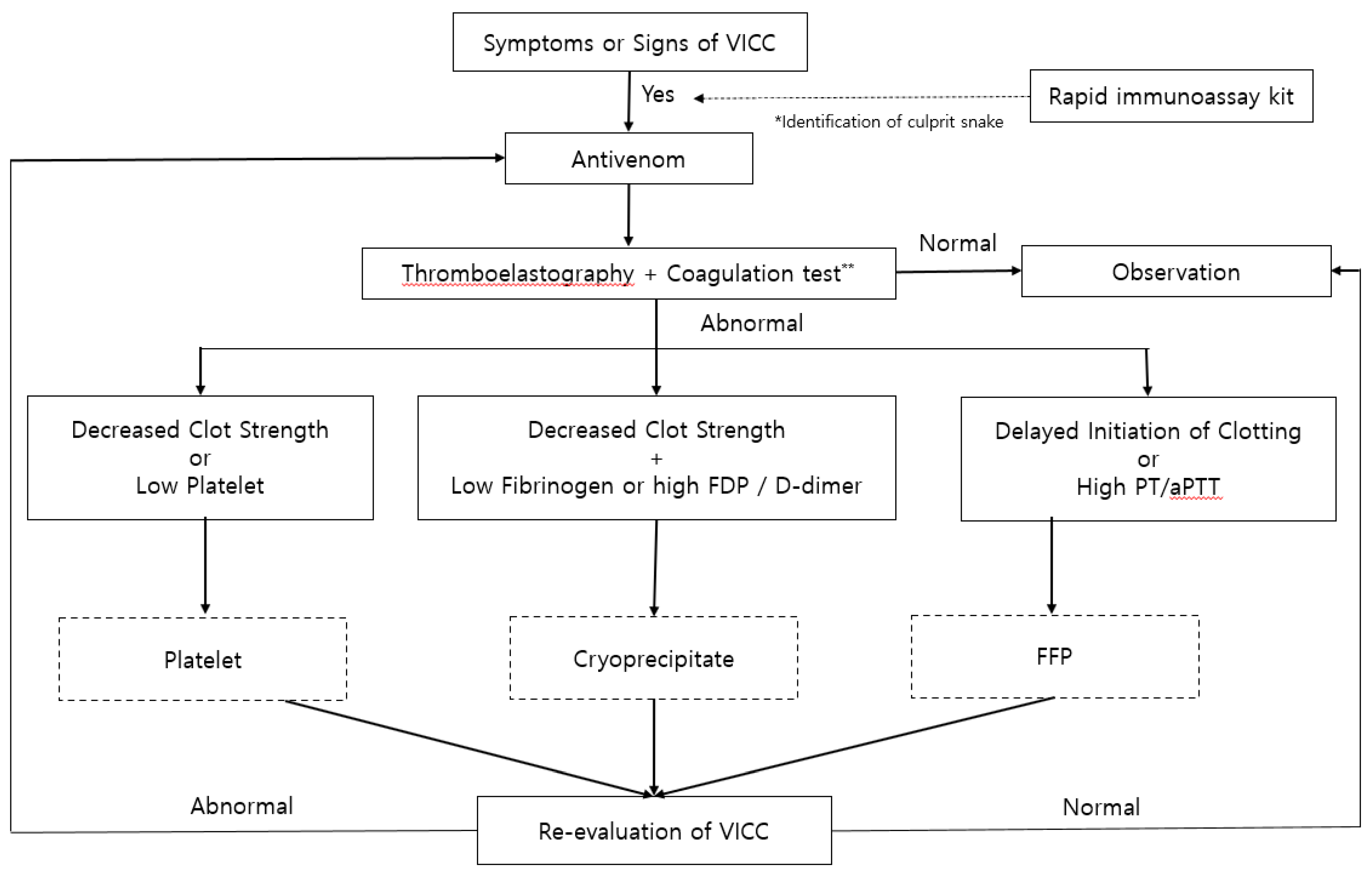
3.4. Treatment of VICC
3.4.1. Antivenom
3.4.2. Transfusion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Peterson, M.E. Snake bite: Pit vipers. Clin Tech Small Anim Pract 2006, 21, 174–182. [Google Scholar] [CrossRef] [PubMed]
- White, J. Snake venoms and coagulopathy. Toxicon. 2005, 45, 951–967. [Google Scholar] [CrossRef] [PubMed]
- Debono, J.; Bos, M.H.A.; Coimbra, F.; Ge, L.; Frank, N.; Kwok, H.F.; Fry, B.G. Basal but divergent: Clinical implications of differential coagulotoxicity in a clade of Asian vipers. Toxicology in vitro. 2019, 58, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Debono, J.; Bos, M.H.A.; Do, M.S.; Fry, B.G. Clinical implications of coagulotoxic variations in Mamushi (Viperidae: Gloydius) snake venoms. Comp. Biochem. Physiol. Toxicol. & Pharmacol. CBP 2019, 225, 108567. [Google Scholar] [CrossRef]
- Nielsen, V.G.; Frank, N.; Afshar, S. De Novo Assessment and Review of Pan-American Pit Viper Anticoagulant and Procoagulant Venom Activities via Kinetomic Analyses. Toxins 2019, 11, 94. [Google Scholar] [CrossRef] [Green Version]
- Hadley, G.P.; McGarr, P.; Mars, M. The role of thromboelastography in the management of children with snake-bite in southern Africa. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 177–179. [Google Scholar] [CrossRef]
- Nag, I.; Datta, S.S.; De, D.; Pal, P.; Das, S.K. Role of thromboelastography in the management of snake bite: A case report from India. Transfus. Apher. Sci. 2017, 56, 127–129. [Google Scholar] [CrossRef]
- Cao, D.; Domanski, K.; Hodgman, E.; Cardenas, C.; Weinreich, M.; Hutto, J.; AbdelFattah, K.R.; Chen, C. Thromboelastometry analysis of severe North American pit viper-induced coagulopathy: A case report. Toxicon 2018, 151, 29–33. [Google Scholar] [CrossRef]
- Sousa, L.F.; Zdenek, C.N.; Dobson, J.S.; Op den Brouw, B.; Coimbra, F.; Gillett, A.; Del-Rei, T.H.M.; Chalkidis, H.M.; Sant’Anna, S.; Teixeira-da-Rocha, M.M.; et al. Coagulotoxicity of Bothrops (Lancehead Pit-Vipers) Venoms from Brazil: Differential Biochemistry and Antivenom Efficacy Resulting from Prey-Driven Venom Variation. Toxins 2018, 10, 411. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.; Kang, H.G.; Kim, K.H. Antivenom for snake bite in Korea. J. Korean Med. Assoc. 2013, 56, 1091–1103. [Google Scholar] [CrossRef] [Green Version]
- You, K.M.; Kwon, W.Y.; Kwon, T.H.; Shin, J.H.; Lee, H.J. Optimal Dose of Antivenin for Asymptomatic or Minor Envenomation Patient with Korean Viperidae Injuries. J. Korean Soc. Emerg. Med. 2013, 24, 420–427. [Google Scholar]
- Cha, Y.S.; Lee, K.H.; Lee, S.J.; Kwon, H.C.; Lee, J.W.; Kim, H.I.; Kim, O.H.; Cha, K.C.; Kim, H.; Hwang, S.O. Usefulness of delta neutrophil index for early prediction of overt disseminated intravascular coagulopathy in patients with venomous snakebite. Clin. Exp. Emerg. Med. 2018, 5, 76–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.J.; Hong, S.I.; Kim, H.S.; Kim, T.H.; Lee, J.H.; Kim, H.J.; Ryu, B.Y.; Kim, H.K. Hematological Features of Coagulopathy and the Efficacy of Antivenin Therapy for a Korean Snakebite. J. Korean Surg. Soc. 2007, 72, 18–26. [Google Scholar]
- Park, E.J.; Yoon, S.K.; Ahn, J.H.; Choi, S.C.; Kim, G.W.; Min, Y.G.; Lee, K.J.; Jung, H.S.; Jung, Y.S. Systemic Complications occurring after Korean Venomous Snake Bite, with focus on Hematologic and Neurologic Complications. J. Korean Soc. Clin. Toxicol. 2009, 7, 90–96. [Google Scholar]
- Marsh, N.; Williams, V. Practical applications of snake venom toxins in haemostasis. Toxicon 2005, 45, 1171–1181. [Google Scholar] [CrossRef]
- Witharana, E.; Gnanathasan, A.; Dissanayake, A.S.; Wijesinghe, S.K.J.; Kadahetti, S.C.L.; Rajapaksha, R. Sri Lankan green pit viper (Trimeresurus trigonocephalus) bites in Deniyaya: A clinico-epidemiological study. Toxicon 2019, 169, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Murthy, J.M.; Kishore, L.T.; Naidu, K.S. Cerebral infarction after envenomation by viper. J. Comput. Assist. Tomogr. 1997, 21, 35–37. [Google Scholar] [CrossRef]
- Porath, A.; Gilon, D.; Schulchynska-Castel, H.; Shalev, O.; Keynan, A.; Benbassat, J. Risk indicators after envenomation in humans by Echis coloratus (mid-east saw scaled viper). Toxicon 1992, 30, 25–32. [Google Scholar] [CrossRef]
- Li, Q.B.; Huang, G.W.; Kinjoh, K.; Nakamura, M.; Kosugi, T. Hematological studies on DIC-like findings observed in patients with snakebite in south China. Toxicon 2001, 39, 943–948. [Google Scholar] [CrossRef]
- Maduwage, K.; Isbister, G.K.; Silva, A.; Bowatta, S.; Mendis, S.; Gawarammana, I. Epidemiology and clinical effects of hump-nosed pit viper (Genus: Hypnale) envenoming in Sri Lanka. Toxicon 2013, 61, 11–15. [Google Scholar] [CrossRef]
- Rathnayaka, R.; Ranathunga, P.; Kularatne, S.A.M. Kidney injury following envenoming by hump-nosed pit viper (Genus: Hypnale) in Sri Lanka: Proven and probable cases. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Burns, B.; Banner, W.; Roper, E. A 60-year-old male with bloody diarrhea and altered mental status secondary to a suspected intravascular crotalid envenomation. J. Okla. State Med Assoc. 2010, 103, 370–372. [Google Scholar] [PubMed]
- Lavonas, E.J.; Ruha, A.M.; Banner, W.; Bebarta, V.; Bernstein, J.N.; Bush, S.P.; Kerns, W.P.; Richardson, W.H.; Seifert, S.A.; Tanen, D.A.; et al. Unified treatment algorithm for the management of crotaline snakebite in the United States: Results of an evidence-informed consensus workshop. BMC Emerg. Med. 2011, 11, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roszko, P.J.; Kavanaugh, M.J.; Boese, M.L.; Longwell, J.J.; Earley, A.S. Rotational thromboelastometry (ROTEM) guided treatment of an Afghanistan viper envenomation at a NATO military hospital. Clin. Toxicol. 2017, 55, 229–230. [Google Scholar] [CrossRef]
- Coggins, A.; Symes, E.; Cheeseman, C.; Salter, M. Thromboelastography for the detection of acute anticoagulant coagulopathy associated with Black Snake envenomation. Emerg. Med. Australas.: EMA 2019, 31, 900–902. [Google Scholar] [CrossRef]
- Leffers, P.; Ferreira, J.; Sollee, D.; Schauben, J. Thromboelastography in the management of snakebite-induced coagulopathy: A case series and literature review. Blood Coagul. Fibrinolysis 2018, 29, 656–660. [Google Scholar] [CrossRef]
- Maduwage, K.; Scorgie, F.E.; Silva, A.; Shahmy, S.; Mohamed, F.; Abeysinghe, C.; Karunathilake, H.; Lincz, L.F.; Gnanathasan, C.A.; Isbister, G.K. Hump-nosed pit viper (Hypnale hypnale) envenoming causes mild coagulopathy with incomplete clotting factor consumption. Clin. Toxicol. 2013, 51, 527–531. [Google Scholar] [CrossRef]
- Witham, W.R.; McNeill, C.; Patel, S. Rebound coagulopathy in patients with snakebite presenting with marked initial coagulopathy. Wilderness & Environ. Med. 2015, 26, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Boyer, L.V.; Seifert, S.A.; Clark, R.F.; McNally, J.T.; Williams, S.R.; Nordt, S.P.; Walter, F.G.; Dart, R.C. Recurrent and persistent coagulopathy following pit viper envenomation. Arch. Intern. Med. 1999, 159, 706–710. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.D.; Young, M.C.; DeMott, M.C.; Ly, B.T.; Clark, R.F. Recurrent coagulopathy and thrombocytopenia in children treated with crotalidae polyvalent immune fab: A case series. Pediatr. Emerg. Care 2010, 26, 576–582. [Google Scholar] [CrossRef]
- Olives, T.D.; Topeff, J.M.; Willhite, L.A.; Kubic, V.L.; Keyler, D.E.; Cole, J.B. Complete clinical course of envenomation by Protobothrops mangshanensis: Delayed coagulopathy and response to Trimeresurus albolabris antivenom. Clin. Toxicol. 2016, 54, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Pongpit, J.; Limpawittayakul, P.; Juntiang, J.; Akkawat, B.; Rojnuckarin, P. The role of prothrombin time (PT) in evaluating green pit viper (Cryptelytrops sp) bitten patients. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Bolliger, D.; Gorlinger, K.; Tanaka, K.A. Pathophysiology and treatment of coagulopathy in massive hemorrhage and hemodilution. Anesthesiol. 2010, 113, 1205–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortner, G.A.; Devlin, J.J.; McGowan, A.J.; Boboc, M.; Natarajan, R.; Zarow, G.J. Comparison of thromboelastography versus conventional coagulation tests in simulated Crotalus atrox envenomation using human blood. Toxicon 2020, 175, 19–27. [Google Scholar] [CrossRef]
- Bolliger, D.; Seeberger, M.D.; Tanaka, K.A. Principles and practice of thromboelastography in clinical coagulation management and transfusion practice. Transfus. Med. Rev. 2012, 26, 1–13. [Google Scholar] [CrossRef]
- da Luz, L.T.; Nascimento, B.; Rizoli, S. Thrombelastography (TEG(R)): Practical considerations on its clinical use in trauma resuscitation. Scand. J. Trauma. Resusc. Emerg. Med. 2013, 21, 29. [Google Scholar] [CrossRef] [Green Version]
- Afshari, A.; Wikkelso, A.; Brok, J.; Moller, A.M.; Wetterslev, J. Thrombelastography (TEG) or thromboelastometry (ROTEM) to monitor haemotherapy versus usual care in patients with massive transfusion. Cochrane. Database. Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Isbister, G.K.; Buckley, N.A.; Page, C.B.; Scorgie, F.E.; Lincz, L.F.; Seldon, M.; Brown, S.G.; Investigators, A.S.P. A randomized controlled trial of fresh frozen plasma for treating venom-induced consumption coagulopathy in cases of Australian snakebite (ASP-18). J. Thromb. Haemost. 2013, 11, 1310–1318. [Google Scholar] [CrossRef]
- Theakston, R.D.; Laing, G.D. Diagnosis of snakebite and the importance of immunological tests in venom research. Toxins 2014, 6, 1667–1695. [Google Scholar] [CrossRef] [Green Version]
- Dhananjaya, B.L.; Menon, J.C.; Joseph, J.K.; Raveendran, D.K.; Oommen, O.V. Snake venom detection kit (SVDK): update on current aspects and challenges. In Clinical Toxinology in Asia Pacific and Africa; Gopalakrishna kone, G., Faiz, A., Fernando, R., Gnanathasan, C.A., Eds.; Springer: Dordrecht, The Netherlands, 2015; Volume 2, pp. 379–400. [Google Scholar]
- Steuten, J.; Winkel, K.; Carroll, T.; Williamson, N.A.; Ignjatovic, V.; Fung, K.; Purcell, A.W.; Fry, B.G. The molecular basis of cross-reactivity in the Australian Snake Venom Detection Kit (SVDK). Toxicon 2007, 50, 1041–1052. [Google Scholar] [CrossRef]
- Kang, S.; Moon, J.; Chun, B. Does the traditional snakebite severity score correctly classify envenomated patients? Clin. Exp. Emerg. Med. 2016, 3, 34–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, S.G.; Caruso, N.; Borland, M.L.; McCoubrie, D.L.; Celenza, A.; Isbister, G.K. Clotting factor replacement and recovery from snake venom-induced consumptive coagulopathy. Intensive. Care. Med. 2009, 35, 1532–1538. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K.; Maduwage, K.; Page, C.B. Antivenom cross neutralisation in a suspected Asian pit viper envenoming causing severe coagulopathy. Toxicon 2014, 90, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.H.; Liew, J.L.; Tan, N.H.; Ismail, A.K.; Maharani, T.; Khomvilai, S.; Sitprija, V. Cross reactivity and lethality neutralization of venoms of Indonesian Trimeresurus complex species by Thai Green Pit Viper Antivenom. Toxicon 2017, 140, 32–37. [Google Scholar] [CrossRef]
- Cannon, R.; Ruha, A.M.; Kashani, J. Acute hypersensitivity reactions associated with administration of crotalidae polyvalent immune Fab antivenom. Ann. Emerg. Med. 2008, 51, 407–411. [Google Scholar] [CrossRef]
- LoVecchio, F.; Klemens, J.; Roundy, E.B.; Klemens, A. Serum sickness following administration of Antivenin (Crotalidae) Polyvalent in 181 cases of presumed rattlesnake envenomation. Wilderness Environ. Med. 2003, 14, 220–221. [Google Scholar]
- Isbister, G.K.; Brown, S.G.; Page, C.B.; McCoubrie, D.L.; Greene, S.L.; Buckley, N.A. Snakebite in Australia: A practical approach to diagnosis and treatment. Med. J. Aust. 2013, 199, 763–768. [Google Scholar] [CrossRef] [Green Version]
- Ledgerwood, A.M.; Blaisdell, W. Coagulation challenges after severe injury with hemorrhagic shock. J. Trauma. Acute. Care Surg. 2012, 72, 1714–1718. [Google Scholar] [CrossRef]
- Kaseer, H.; Sanghavi, D. Aminocaproic Acid. StatPearls, Aminocaproic Acid. 2020. [Google Scholar]
- Larsen, O.H.; Fenger-Eriksen, C.; Christiansen, K.; Ingerslev, J.; Sørensen, B. Diagnostic performance and therapeutic consequence of thromboelastometry activated by kaolin versus a panel of specific reagents. Anesthesiol. 2011, 115, 294–302. [Google Scholar] [CrossRef] [Green Version]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, E.J.; Choi, S.; Kim, H.-H.; Jung, Y.S. Novel Treatment Strategy for Patients with Venom-Induced Consumptive Coagulopathy from a Pit Viper Bite. Toxins 2020, 12, 295. https://doi.org/10.3390/toxins12050295
Park EJ, Choi S, Kim H-H, Jung YS. Novel Treatment Strategy for Patients with Venom-Induced Consumptive Coagulopathy from a Pit Viper Bite. Toxins. 2020; 12(5):295. https://doi.org/10.3390/toxins12050295
Chicago/Turabian StylePark, Eun Jung, Sangchun Choi, Hyuk-Hoon Kim, and Yoon Seok Jung. 2020. "Novel Treatment Strategy for Patients with Venom-Induced Consumptive Coagulopathy from a Pit Viper Bite" Toxins 12, no. 5: 295. https://doi.org/10.3390/toxins12050295
APA StylePark, E. J., Choi, S., Kim, H. -H., & Jung, Y. S. (2020). Novel Treatment Strategy for Patients with Venom-Induced Consumptive Coagulopathy from a Pit Viper Bite. Toxins, 12(5), 295. https://doi.org/10.3390/toxins12050295