Neutrophil Gelatinase–Associated Lipocalin Acts as a Robust Early Diagnostic Marker for Renal Replacement Therapy in Patients with Russell’s Viper Bite–Induced Acute Kidney Injuries

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
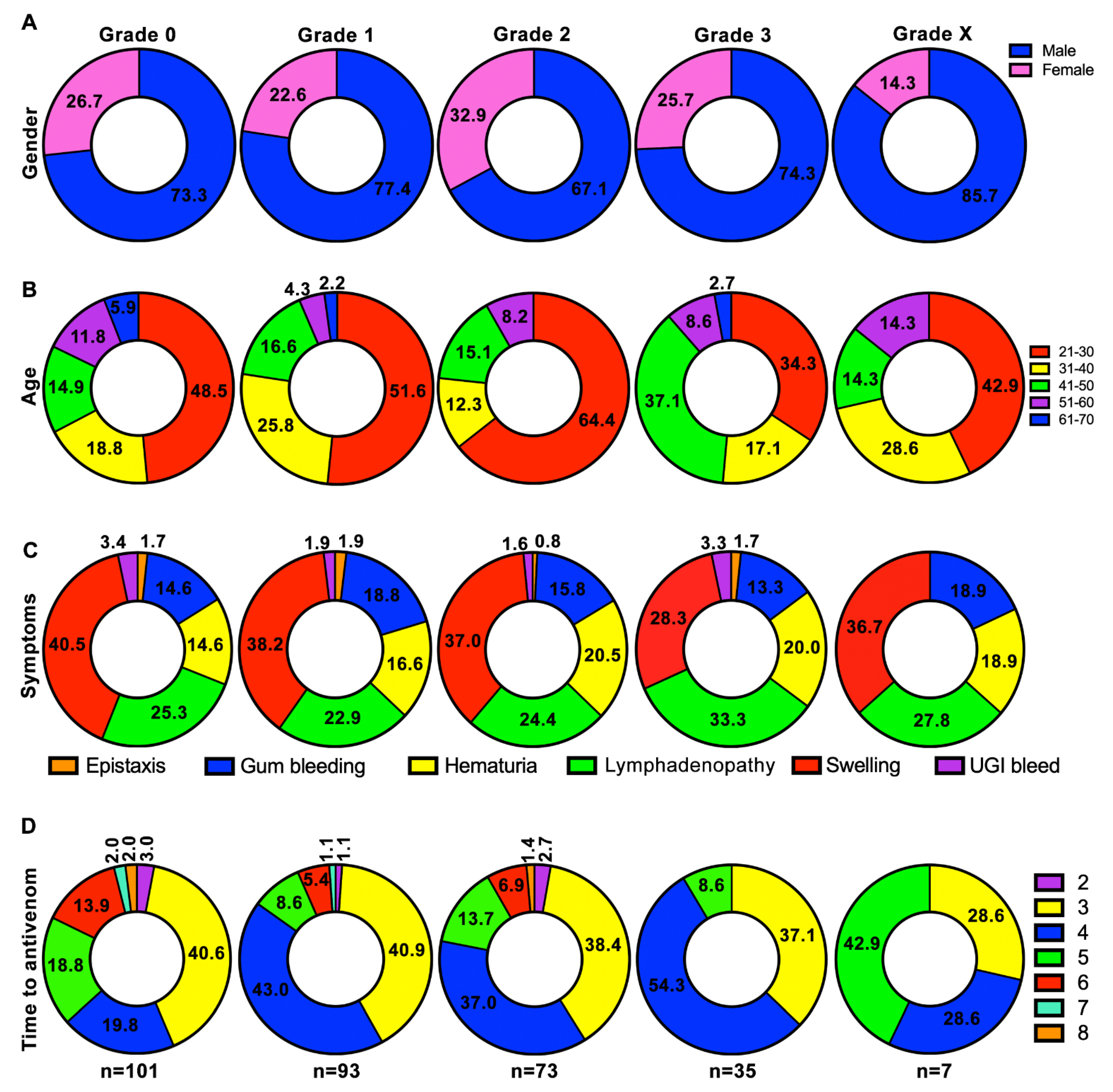
2.1. Males and Working-Age Groups Are Largely Affected by Russell’s Viper Bites
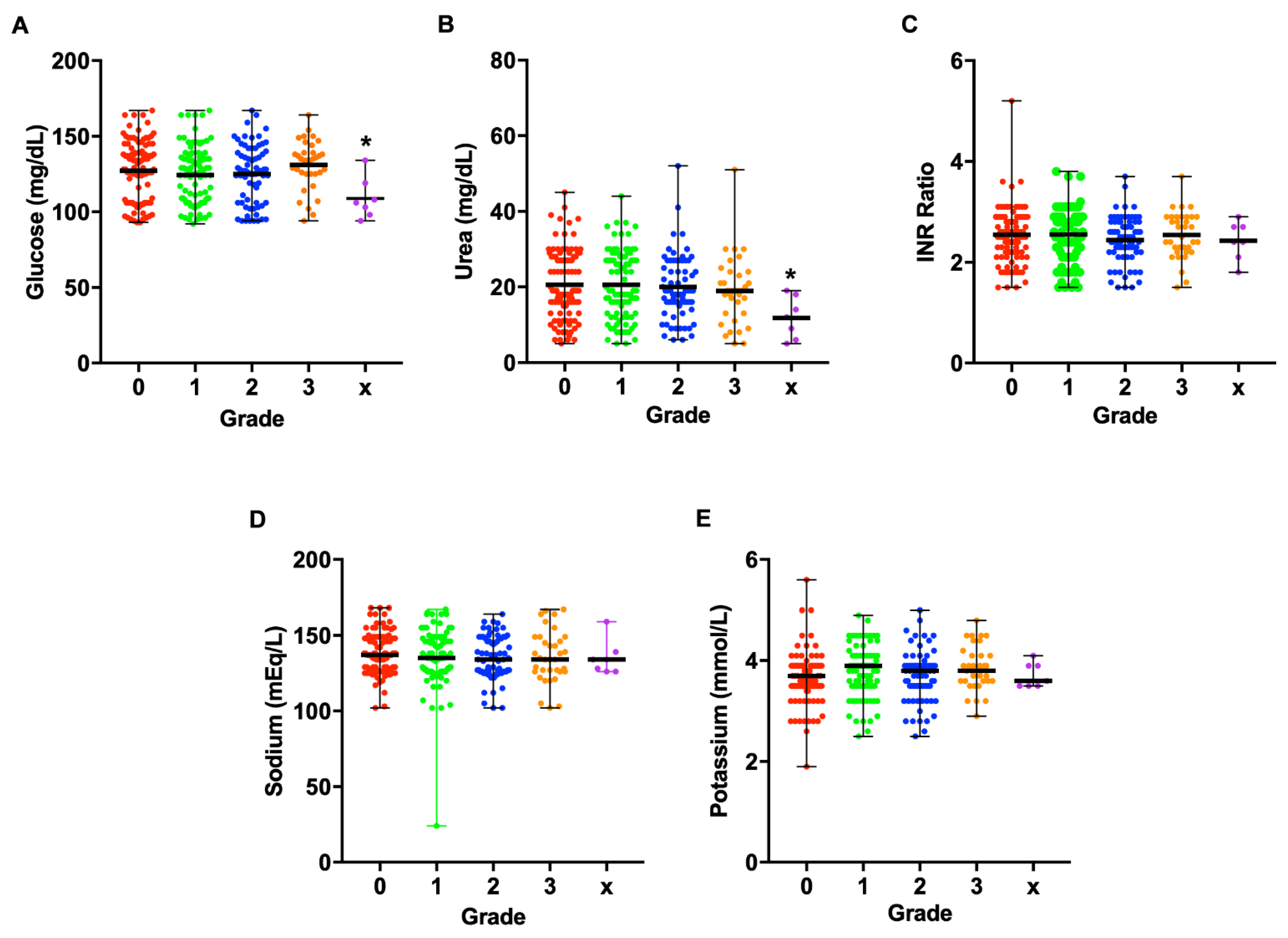
2.2. Creatinine Levels Are Significantly Increased over Time in Grades 1–3
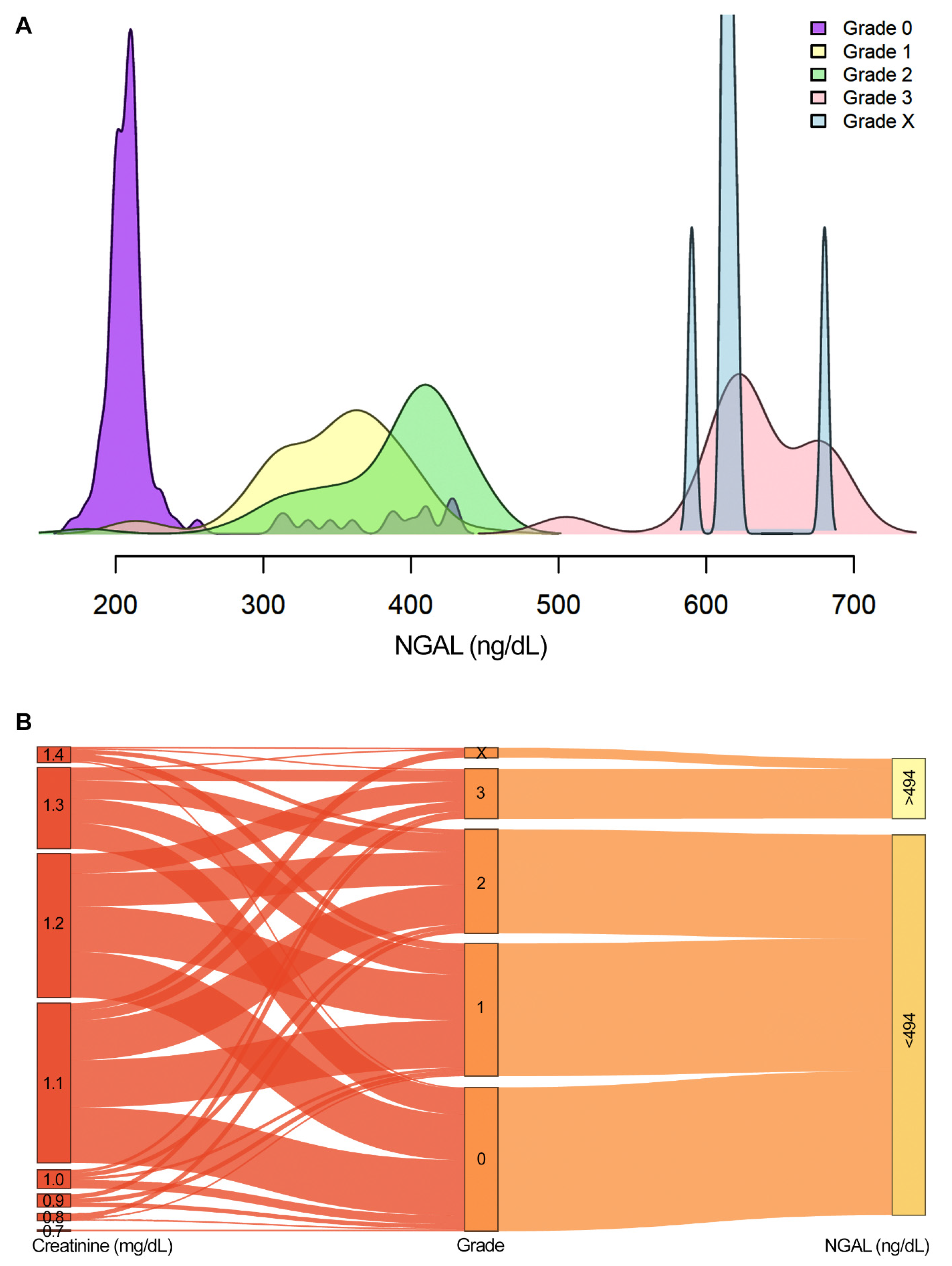
2.3. NGAL Acts as a Robust Biomarker for Grades 3 and X
3. Discussion
4. Methods
4.1. Study Design
4.2. Data Collection
4.3. Classification of Patient Groups
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kasturiratne, A.; Wickremasinghe, A.R.; de Silva, N.; Gunawardena, N.K.; Pathmeswaran, A.; Premaratna, R.; Savioli, L.; Lalloo, D.G.; de Silva, H.J. The global burden of snakebite: A literature analysis and modelling based on regional es-timates of envenoming and deaths. PLoS Med. 2008, 5, e218. [Google Scholar] [CrossRef] [Green Version]
- Williams, H.F.; Layfield, H.J.; Vallance, T.; Patel, K.; Bicknell, A.B.; Trim, S.A.; Vaiyapuri, S. The Urgent Need to Develop Novel Strategies for the Diagnosis and Treatment of Snakebites. Toxins 2019, 11, 363. [Google Scholar] [CrossRef] [Green Version]
- Samuel, S.P.; Chinnaraju, S.; Williams, H.F.; Pichamuthu, E.; Subharao, M.; Vaiyapuri, M.; Arumugam, S.; Vaiyapuri, R.; Baksh, M.F.; Patel, K.; et al. Venomous snakebites: Rapid action saves lives-A multifaceted community education programme increases awareness about snakes and snakebites among the rural population of Tamil Nadu, India. PLoS Negl. Trop. Dis. 2020, 14, e0008911. [Google Scholar] [CrossRef] [PubMed]
- Vaiyapuri, S.; Vaiyapuri, R.; Ashokan, R.; Ramasamy, K.; Nattamaisundar, K.; Jeyaraj, A.; Chandran, V.; Gajjeraman, P.; Baksh, M.F.; Gibbins, J.M.; et al. Snakebite and its socio-economic impact on the rural population of Tamil Nadu, India. PLoS ONE 2013, 8, e80090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohapatra, B.; Warrell, D.A.; Suraweera, W.; Bhatia, P.; Dhingra, N.; Jotkar, R.M.; Rodriguez, P.S.; Mishra, K.; Whitaker, R.; Jha, P.; et al. Snakebite Mortality in India: A Nationally Representative Mortality Survey. PLOS Negl. Trop. Dis. 2011, 5, e1018. [Google Scholar] [CrossRef]
- Suraweera, W.; Warrell, D.; Whitaker, R.; Menon, G.; Rodrigues, R.; Fu, S.H.; Begum, R.; Sati, P.; Piyasena, K.; Bhatia, M.; et al. Trends in snakebite deaths in India from 2000 to 2019 in a nationally representative mortality study. eLife 2020, 9, e54076. [Google Scholar] [CrossRef]
- Harshavardhan, L.; Lokesh, A.J.; Tejeshwari, H.L.; Halesha, B.R.; Siddharama, S. A study on the acute kidney injury in snake bite victims in a tertiary care centre. J. Clin. Diagn. Res. 2013, 7, 853–856. [Google Scholar] [CrossRef]
- Alfred, S.; Bates, D.; White, J.; Mahmood, M.A.; Warrell, D.A.; Thwin, K.T.; Thein, M.M.; Sint San, S.S.; Myint, Y.L.; Swe, H.K.; et al. Acute Kidney Injury Following Eastern Russell’s Viper (Daboia siamensis) Snakebite in Myanmar. Kidney Int. Rep. 2019, 4, 1337–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratnayake, I.; Mohamed, F.; Buckley, N.A.; Gawarammana, I.B.; Dissanayake, D.M.; Chathuranga, U.; Munasinghe, M.; Maduwage, K.; Jayamanne, S.; Endre, Z.H.; et al. Early identification of acute kidney injury in Russell’s viper (Daboia russelii) envenoming using renal biomarkers. PLoS Negl. Trop. Dis. 2019, 13, e0007486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priyamvada, P.S.; Jaswanth, C.; Zachariah, B.; Haridasan, S.; Parameswaran, S.; Swaminathan, R.P. Prognosis and long-term outcomes of acute kidney injury due to snake envenomation. Clin. Kidney J. 2019, 13, 564–570. [Google Scholar] [CrossRef]
- Sarkar, S.; Sinha, R.; Chaudhury, A.R.; Maduwage, K.; Abeyagunawardena, A.; Bose, N.; Pradhan, S.; Bresolin, N.L.; Garcia, B.A.; McCulloch, M. Snake bite associated with acute kidney injury. Pediatric. Nephrol. 2021. [Google Scholar] [CrossRef]
- Vikrant, S.; Jaryal, A.; Parashar, A. Clinicopathological spectrum of snake bite-induced acute kidney injury from India. World J. Nephrol. 2017, 6, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.R.; Uraiya, D.; Kumar, A.; Tripathi, N. Early demographic and clinical predictors of developing acute kidney injury in snake bite patients: A retrospective controlled study from an Indian tertiary care hospital in North Eastern Uttar Pradesh India. Indian J. Crit. Care Med. 2016, 20, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, V.S.; Ferguson, M.A.; Bonventre, J.V. Biomarkers of acute kidney injury. Annu. Rev. Pharm. Toxicol. 2008, 48, 463–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagshaw, S.M.; Gibney, R.T. Conventional markers of kidney function. Crit. Care Med. 2008, 36, S152–S158. [Google Scholar] [CrossRef]
- Endre, Z.H.; Pickering, J.W. Biomarkers and creatinine in AKI: The trough of disillusionment or the slope of enlightenment? Kidney Int. 2013, 84, 644–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endre, Z.H.; Pickering, J.W.; Walker, R.J. Clearance and beyond: The complementary roles of GFR measurement and injury biomarkers in acute kidney injury (AKI). Am. J. Physiol. Ren. Physiol. 2011, 301, F697–F707. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; Donato, V.; Coppolino, G.; Campo, S.; Buemi, A.; Lacquaniti, A.; Buemi, M. Neutrophil gelatinase-associated lipocalin (NGAL) as a marker of kidney damage. Am. J. Kidney Dis. 2008, 52, 595–605. [Google Scholar] [CrossRef]
- Senthilkumaran, S.; Thirumalaikolundusubramanian, P.; Elangovan, N. Neutrophil gelatinase-associated lipocalin as an early diagnostic biomarker of acute kidney injury in snake bite. J. Emergencies Trauma Shock 2019, 12, 260–262. [Google Scholar] [CrossRef]
- Snthilkumaran, S.; Manimaran, D.; Thirumalaikolundusubramanian, P.; Elangovan, N. Neutrophil Gelatinase-Associated Lipocalin as an Early Marker of Acute Kidney Injury in Snake Bites Victims. Int. J. Theor. Appl. Sci. 2017, 9, 178–180. [Google Scholar]
- Thamarai, R.; Sivakumar, K. Plasma neutrophil gelatinase associated lipocalin as an early biomarker of acute kidney injury in snake bite. J. Evol. Med. Dent. Sci. 2014, 3, 14737–14746. [Google Scholar]
- Albuquerque, P.L.M.M.; da Silva Junior, G.B.; Meneses, G.C.; Martins, A.M.C.; Lima, D.B.; Raubenheimer, J.; Fathima, S.; Buckley, N.; Daher, E.D.F. Acute Kidney Injury Induced by Bothrops Venom: Insights into the Pathogenic Mechanisms. Toxins 2019, 11, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chippaux, J.-P. Snakebite envenomation turns again into a neglected tropical disease! J. Venom. Anim. Toxins Incl. Trop. Dis. 2017, 23, 38. [Google Scholar] [CrossRef]
- Samra, M.; Abcar, A.C. False estimates of elevated creatinine. Perm J. 2012, 16, 51–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsa, R.; Ashley, E.; Sharma, V.; Walden, A.P.; Keating, L. Plasma and urine neutrophil gelatinase-associated lipocalin in the diagnosis of new onset acute kidney injury in critically ill patients. Crit. Care 2014, 18, R137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khawaja, S.; Jafri, L.; Siddiqui, I.; Hashmi, M.; Ghani, F. The utility of neutrophil gelatinase-associated Lipocalin (NGAL) as a marker of acute kidney injury (AKI) in critically ill patients. Biomark Res. 2019, 7, 4. [Google Scholar] [CrossRef]
- Schley, G.; Köberle, C.; Manuilova, E.; Rutz, S.; Forster, C.; Weyand, M.; Formentini, I.; Kientsch-Engel, R.; Eckardt, K.-U.; Willam, C. Comparison of Plasma and Urine Biomarker Performance in Acute Kidney Injury. PLoS ONE 2015, 10, e0145042. [Google Scholar] [CrossRef] [Green Version]
- Mahmoodpoor, A.; Hamishehkar, H.; Fattahi, V.; Sanaie, S.; Arora, P.; Nader, N.D. Urinary versus plasma neutrophil gelatinase-associated lipocalin (NGAL) as a predictor of mortality for acute kidney injury in intensive care unit patients. J. Clin. Anesth 2018, 44, 12–17. [Google Scholar] [CrossRef]
- Li, Y.M.; Li, Y.; Yan, L.; Wang, H.; Wu, X.J.; Tang, J.T.; Wang, L.L.; Shi, Y.Y. Comparison of urine and blood NGAL for early prediction of delayed graft function in adult kidney transplant recipients: A meta-analysis of observational studies. BMC Nephrol. 2019, 20, 291. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Li, J.; Li, F.; Qi, X.; Zhang, J. Neutrophil gelatinase-associated lipocalin accurately predicts renal tubular injury in patients with chronic hepatitis B treated with nucleos(t)ide analogs. Hepatol. Res. 2018, 48, 144–152. [Google Scholar] [CrossRef]
- Yi, A.; Lee, C.H.; Yun, Y.M.; Kim, H.; Moon, H.W.; Hur, M. Effectiveness of Plasma and Urine Neutrophil Gelatinase-Associated Lipocalin for Predicting Acute Kidney Injury in High-Risk Patients. Ann. Lab Med. 2021, 41, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Han, J.; Liu, J.; Liang, B.; Wang, X.; Wang, C. Clinical significance of novel biomarker NGAL in early diagnosis of acute renal injury. Exp. Med. 2017, 14, 5017–5021. [Google Scholar] [CrossRef] [PubMed]
- Törnblom, S.; Nisula, S.; Petäjä, L.; Vaara, S.T.; Haapio, M.; Pesonen, E.; Pettilä, V.; Laru-Sompa, R.; Pulkkinen, A.; Saarelainen, M.; et al. Urine NGAL as a biomarker for septic AKI: A critical appraisal of clinical utility—Data from the observational FINNAKI study. Ann. Intensive Care 2020, 10, 51. [Google Scholar] [CrossRef] [PubMed]
- Glassford, N.J.; Schneider, A.G.; Xu, S.; Eastwood, G.M.; Young, H.; Peck, L.; Venge, P.; Bellomo, R. The nature and discriminatory value of urinary neutrophil gelatinase-associated lipocalin in critically ill patients at risk of acute kidney injury. Intensive Care Med. 2013, 39, 1714–1724. [Google Scholar] [CrossRef]
- Srisawat, N.; Praditpornsilpa, K.; Patarakul, K.; Techapornrung, M.; Daraswang, T.; Sukmark, T.; Khositrangsikun, K.; Fakthongyoo, A.; Oranrigsupak, P.; Praderm, L.; et al. Neutrophil Gelatinase Associated Lipocalin (NGAL) in Leptospirosis Acute Kidney Injury: A Multicenter Study in Thailand. PLoS ONE 2015, 10, e0143367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Zhao, X.; Duan, X.; Wang, X.; Wang, T.; Feng, S.; Zhang, H.; Chen, C.; Li, G. Knockout of NGAL aggravates tubulointerstitial injury in a mouse model of diabetic nephropathy by enhancing oxidative stress and fibrosis. Exp. Med. 2021, 21, 321. [Google Scholar] [CrossRef]
- Patel, M.L.; Sachan, R.; Misra, R.; Kamal, R.; Shyam, R.; Sachan, P. Prognostic significance of urinary NGAL in chronic kidney disease. Int. J. Nephrol. Renov. Dis. 2015, 8, 139–144. [Google Scholar] [CrossRef] [Green Version]
- Castillo-Rodriguez, E.; Fernandez-Prado, R.; Martin-Cleary, C.; Pizarro-Sánchez, M.S.; Sanchez-Niño, M.D.; Sanz, A.B.; Fernandez-Fernandez, B.; Ortiz, A. Kidney Injury Marker 1 and Neutrophil Gelatinase-Associated Lipocalin in Chronic Kidney Disease. Nephron 2017, 136, 263–267. [Google Scholar] [CrossRef]
- Papadopoulou-Marketou, N.; Margeli, A.; Papassotiriou, I.; Chrousos, G.P.; Kanaka-Gantenbein, C.; Wahlberg, J. NGAL as an Early Predictive Marker of Diabetic Nephropathy in Children and Young Adults with Type 1 Diabetes Mellitus. J. Diabetes Res. 2017, 2017, 7526919. [Google Scholar] [CrossRef]
- Malyszko, J.; Bachorzewska-Gajewska, H.; Malyszko, J.S.; Pawlak, K.; Dobrzycki, S. Serum neutrophil gelatinase-associated lipocalin as a marker of renal function in hypertensive and normotensive patients with coronary artery disease. Nephrology 2008, 13, 153–156. [Google Scholar] [CrossRef]
- Ning, M.; Mao, X.; Niu, Y.; Tang, B.; Shen, H. Usefulness and limitations of neutrophil gelatinase-associated lipocalin in the assessment of kidney diseases. J. Lab. Precis. Med. 2018, 3. [Google Scholar] [CrossRef]
- Pla, D.; Sanz, L.; Quesada-Bernat, S.; Villalta, M.; Baal, J.; Chowdhury, M.A.W.; León, G.; Gutiérrez, J.M.; Kuch, U.; Calvete, J.J. Phylovenomics of Daboia russelii across the Indian subcontinent. Bioactivities and comparative in vivo neutralization and in vitro third-generation antivenomics of antivenoms against venoms from India, Bangladesh and Sri Lanka. J. Proteom. 2019, 207, 103443. [Google Scholar] [CrossRef] [PubMed]
- Faisal, T.; Tan, K.Y.; Tan, N.H.; Sim, S.M.; Gnanathasan, C.A.; Tan, C.H. Proteomics, toxicity and antivenom neutralization of Sri Lankan and Indian Russell’s viper (Daboia russelii) venoms. J. Venom. Anim. Toxins Incl. Trop. Dis. 2021, 27, e20200177. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.Y.; Tan, N.H.; Tan, C.H. Venom proteomics and antivenom neutralization for the Chinese eastern Russell’s viper, Daboia siamensis from Guangxi and Taiwan. Sci. Rep. 2018, 8, 8545. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senthilkumaran, S.; Patel, K.; Salim, A.; Vijayakumar, P.; Williams, H.F.; Vaiyapuri, R.; Savania, R.; Elangovan, N.; Thirumalaikolundusubramanian, P.; Baksh, M.F.; et al. Neutrophil Gelatinase–Associated Lipocalin Acts as a Robust Early Diagnostic Marker for Renal Replacement Therapy in Patients with Russell’s Viper Bite–Induced Acute Kidney Injuries. Toxins 2021, 13, 797. https://doi.org/10.3390/toxins13110797
Senthilkumaran S, Patel K, Salim A, Vijayakumar P, Williams HF, Vaiyapuri R, Savania R, Elangovan N, Thirumalaikolundusubramanian P, Baksh MF, et al. Neutrophil Gelatinase–Associated Lipocalin Acts as a Robust Early Diagnostic Marker for Renal Replacement Therapy in Patients with Russell’s Viper Bite–Induced Acute Kidney Injuries. Toxins. 2021; 13(11):797. https://doi.org/10.3390/toxins13110797
Chicago/Turabian StyleSenthilkumaran, Subramanian, Ketan Patel, Anika Salim, Pradeep Vijayakumar, Harry F. Williams, Rajendran Vaiyapuri, Ravi Savania, Namasivayam Elangovan, Ponniah Thirumalaikolundusubramanian, M. Fazil Baksh, and et al. 2021. "Neutrophil Gelatinase–Associated Lipocalin Acts as a Robust Early Diagnostic Marker for Renal Replacement Therapy in Patients with Russell’s Viper Bite–Induced Acute Kidney Injuries" Toxins 13, no. 11: 797. https://doi.org/10.3390/toxins13110797
APA StyleSenthilkumaran, S., Patel, K., Salim, A., Vijayakumar, P., Williams, H. F., Vaiyapuri, R., Savania, R., Elangovan, N., Thirumalaikolundusubramanian, P., Baksh, M. F., & Vaiyapuri, S. (2021). Neutrophil Gelatinase–Associated Lipocalin Acts as a Robust Early Diagnostic Marker for Renal Replacement Therapy in Patients with Russell’s Viper Bite–Induced Acute Kidney Injuries. Toxins, 13(11), 797. https://doi.org/10.3390/toxins13110797