The Five-Year Prospective Study of Quality of Life in Hemifacial Spasm Treated with Abo-Botulinum Toxin A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
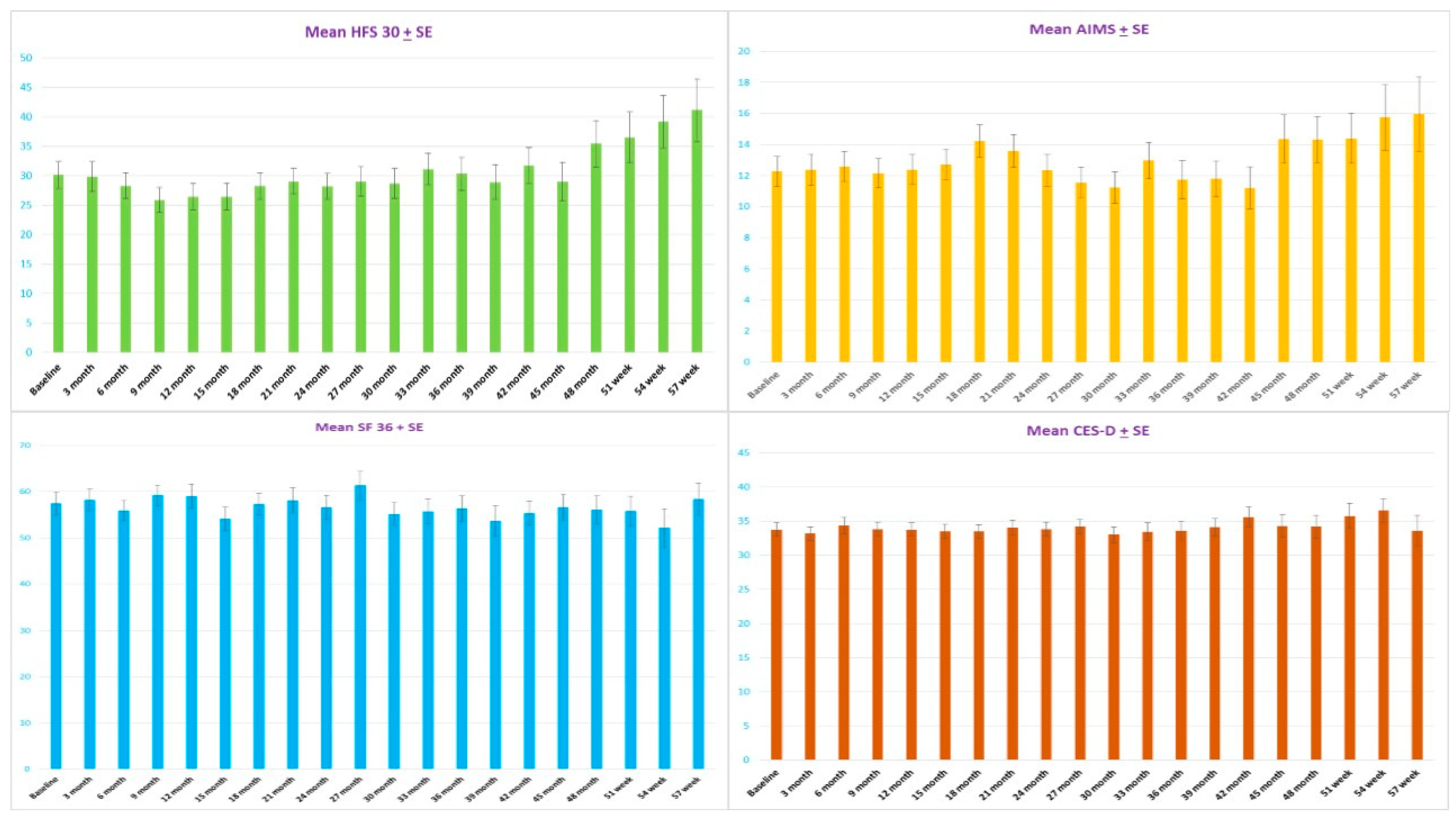
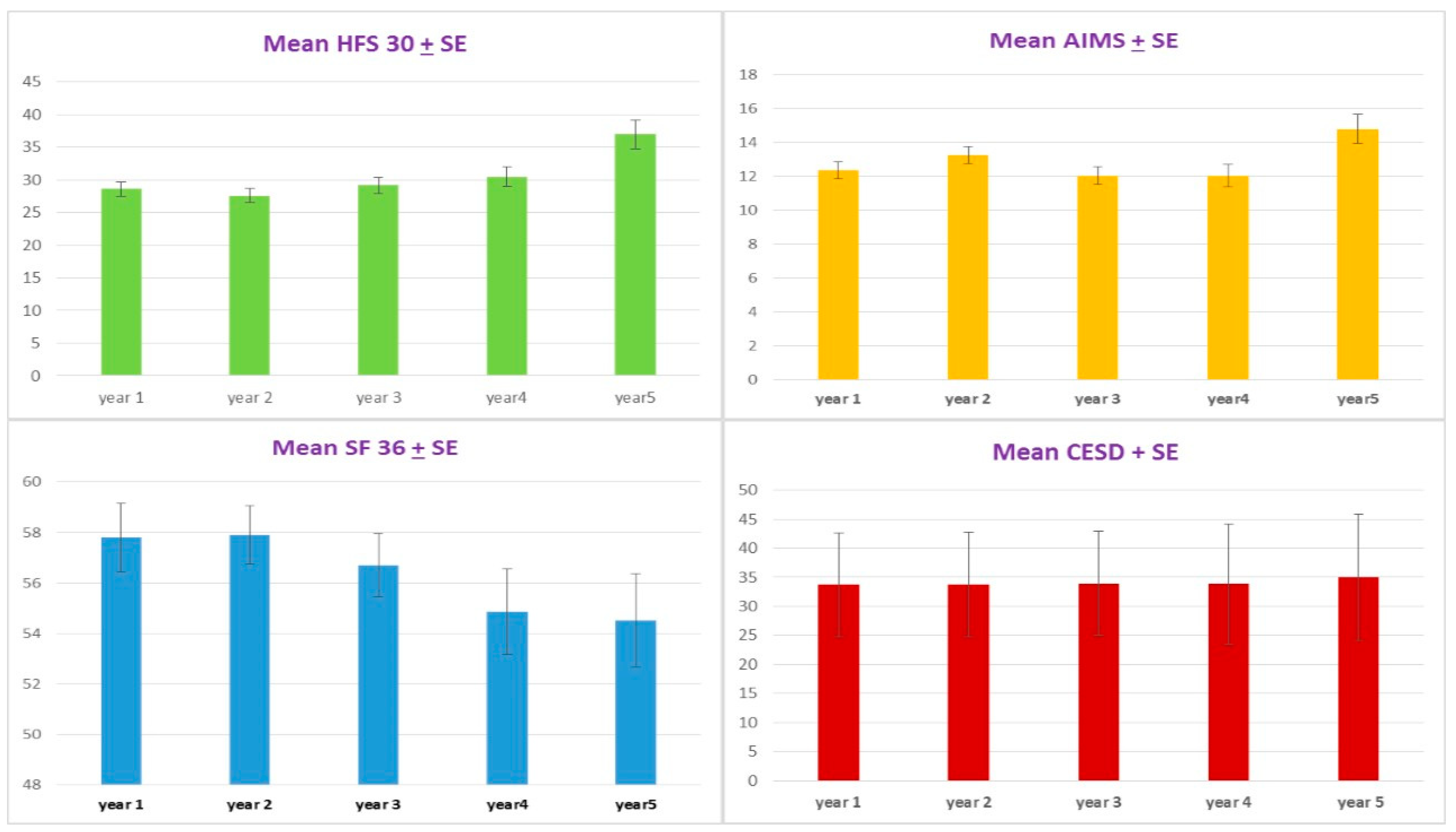
2.1. The Disease-Specific HRQoL
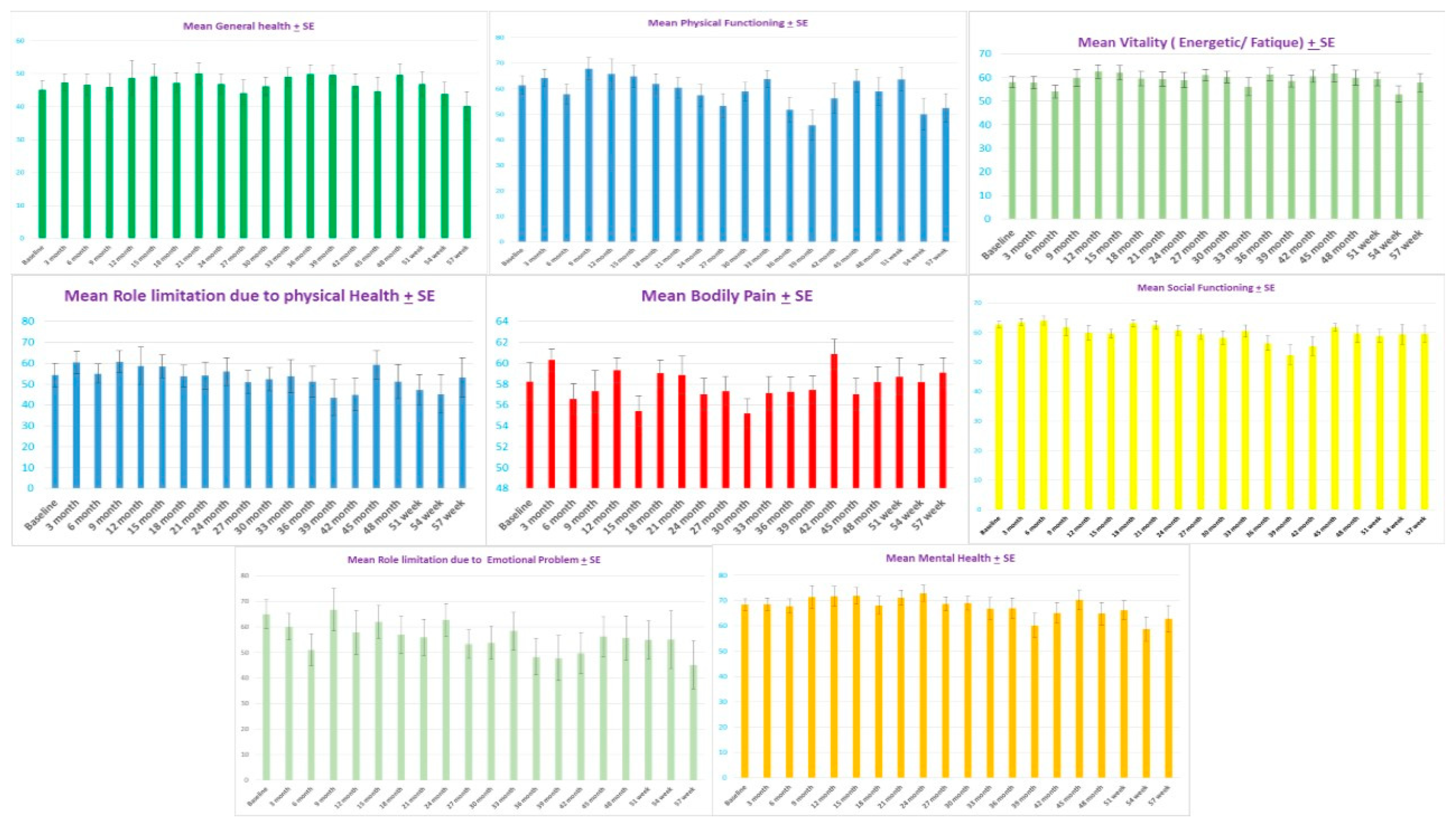
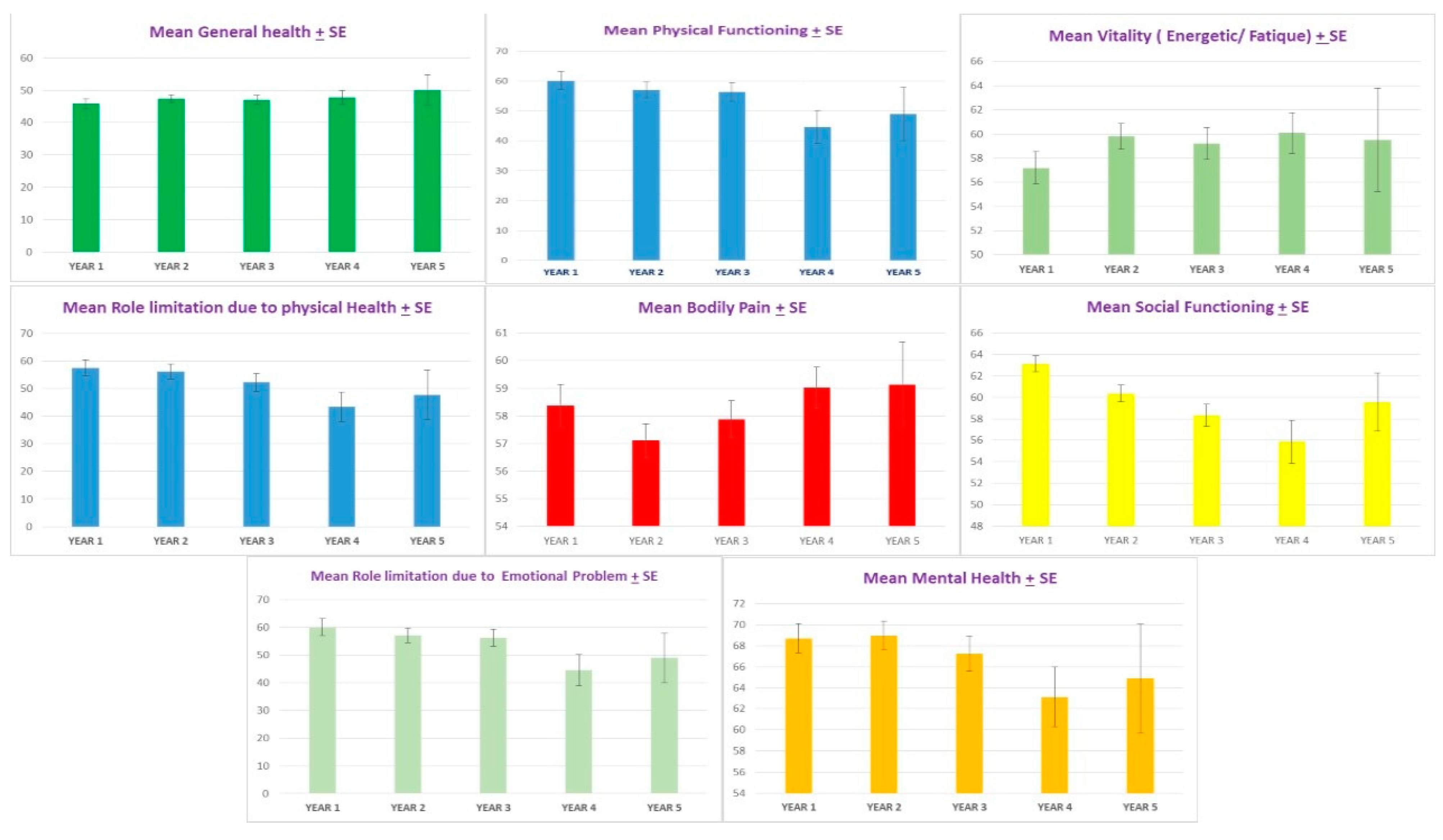
2.2. The general HRQoL
2.3. The CES-D Scores
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Medication
5.2. Assessments
5.3. Efficacy Measurement
5.3.1. The Disease-Specific HRQoL Questionnaire
5.3.2. Abnormal Involuntary Movement Scale (AIMS) (Thai Version)
5.3.3. The General HRQoL Questionnaire
5.3.4. Depression Screening Questionnaire
5.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, A.; Jankovic, J. Hemifacial spasm: Clinical findings and treatment. Muscle Nerve 1998, 21, 1740–1747. [Google Scholar] [CrossRef]
- Tan, N.C.; Chan, L.L.; Tan, E.K. Hemifacial spasm and involuntary facial movements. QJM 2002, 95, 493–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nimmannitya, P. Hemifacial spasm and surgical treatment (microvascular decompression). Thammasat Med J. 2015, 15, 291–302. [Google Scholar]
- Tan, E.K.; Fook-Chong, S.; Lum, S.Y.; Lim, E. Botulinum toxin improves quality of life in hemifacial spasm: Validation of a questionnaire (HFS-30). J. Neurol. Sci. 2004, 219, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Setthawatcharawanich, S.; Aui-aree, N.; Limapichart, K.; Satirapunya, P.; Phabphal, K. The validation of the disease-specific questionnaire for health-related quality of life in Thai patients with hemifacial spasm. J. Med. Assoc. Thai 2008, 91, 1691–1697. [Google Scholar] [PubMed]
- Huang, Y.C.; Fan, J.Y.; Ro, L.S.; Lyu, R.K.; Chang, H.S.; Chen, S.T.; Hsu, W.C.; Chen, C.M.; Wu, Y.R. Validation of a Chinese version of disease specific quality of life scale (HFS-36) for hemifacial spasm in Taiwan. Health Qual. Life Outcomes 2009, 7, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kongsengdao, S.; Kritalukkul, S. Quality of life in hemifacial spasm patient after treatment with botulinum toxin A; a 24-week, double-blind, randomized, cross-over comparison of Dysport and Neuronox study. J. Med. Assoc. Thai 2012, 95 (Suppl. 3), S48–S54. [Google Scholar] [PubMed]
- Defazio, G.; Abbruzzese, G.; Girlanda, P.; Vacca, L.; Currà, A.; De Salvia, R.; Marchese, R.; Raineri, R.; Roselli, F.; Livrea, P.; et al. Botulinum toxin A treatment for primary hemifacial spasm: A 10-year multicenter study. Arch. Neurol. 2002, 59, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Jitpimolmard, S.; Tiamkao, S.; Laopaiboon, M. Long term results of botulinum toxin type A (Dysport) in the treatment of hemifacial spasm: A report of 175 cases. J. Neurol. Neurosurg. Psychiatry 1998, 64, 751–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, J.; Espírito-Santo, C.; Borges, A.; Ferreira, J.J.; Coelho, M.; Moore, P.; Sampaio, C. Botulinum toxin type A therapy for hemifacial spasm. Cochrane Database Syst. Rev. 2005, 2005, Cd004899. [Google Scholar] [CrossRef]
- Cheng, J.; Lei, D.; Hui, X.; Zhang, H. Improvement of Quality of Life in Patients with Hemifacial Spasm after Microvascular Decompression: A Prospective Study. World Neurosurg. 2017, 107, 549–553. [Google Scholar] [CrossRef]
- Xu, X.L.; Zhen, X.K.; Yuan, Y.; Liu, H.J.; Liu, J.; Xu, J.; Li, X.B.; Zhang, L.; Yu, Y.B. Long-Term Outcome of Repeat Microvascular Decompression for Hemifacial Spasm. World Neurosurg. 2018, 110, e989–e997. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Adib Saberi, F. Botulinum toxin: Mechanisms of action. Eur. Neurol. 2005, 53, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.E., Jr. SF-36 health survey update. Spine (Phila Pa 1976) 2000, 25, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- Leurmarnkul, W.; Meetam, P. Properties testing of the retranslated SF36 (Thai Version). Thai J. Pharm. Sci. 2005, 29, 69–88. [Google Scholar]
- Tan, E.K.; Fook-Chong, S.; Lum, S.Y.; Thumboo, J. Validation of a short disease specific quality of life scale for hemifacial spasm: Correlation with SF-36. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1707–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trangkasombat, U.; Larpboonsarp, V.; Havanond, P. CES-D as a screen for depression in adolescents. J. Psychiatr. Assoc. Thai 1997, 42, 2–13. [Google Scholar]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kongsaengdao, S.; Maneeton, N.; Maneeton, B. The Five-Year Prospective Study of Quality of Life in Hemifacial Spasm Treated with Abo-Botulinum Toxin A. Toxins 2021, 13, 215. https://doi.org/10.3390/toxins13030215
Kongsaengdao S, Maneeton N, Maneeton B. The Five-Year Prospective Study of Quality of Life in Hemifacial Spasm Treated with Abo-Botulinum Toxin A. Toxins. 2021; 13(3):215. https://doi.org/10.3390/toxins13030215
Chicago/Turabian StyleKongsaengdao, Subsai, Narong Maneeton, and Benchalak Maneeton. 2021. "The Five-Year Prospective Study of Quality of Life in Hemifacial Spasm Treated with Abo-Botulinum Toxin A" Toxins 13, no. 3: 215. https://doi.org/10.3390/toxins13030215
APA StyleKongsaengdao, S., Maneeton, N., & Maneeton, B. (2021). The Five-Year Prospective Study of Quality of Life in Hemifacial Spasm Treated with Abo-Botulinum Toxin A. Toxins, 13(3), 215. https://doi.org/10.3390/toxins13030215