Novel Anatomical Proposal for Botulinum Neurotoxin Injection Targeting Lateral Canthal Rhytids



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
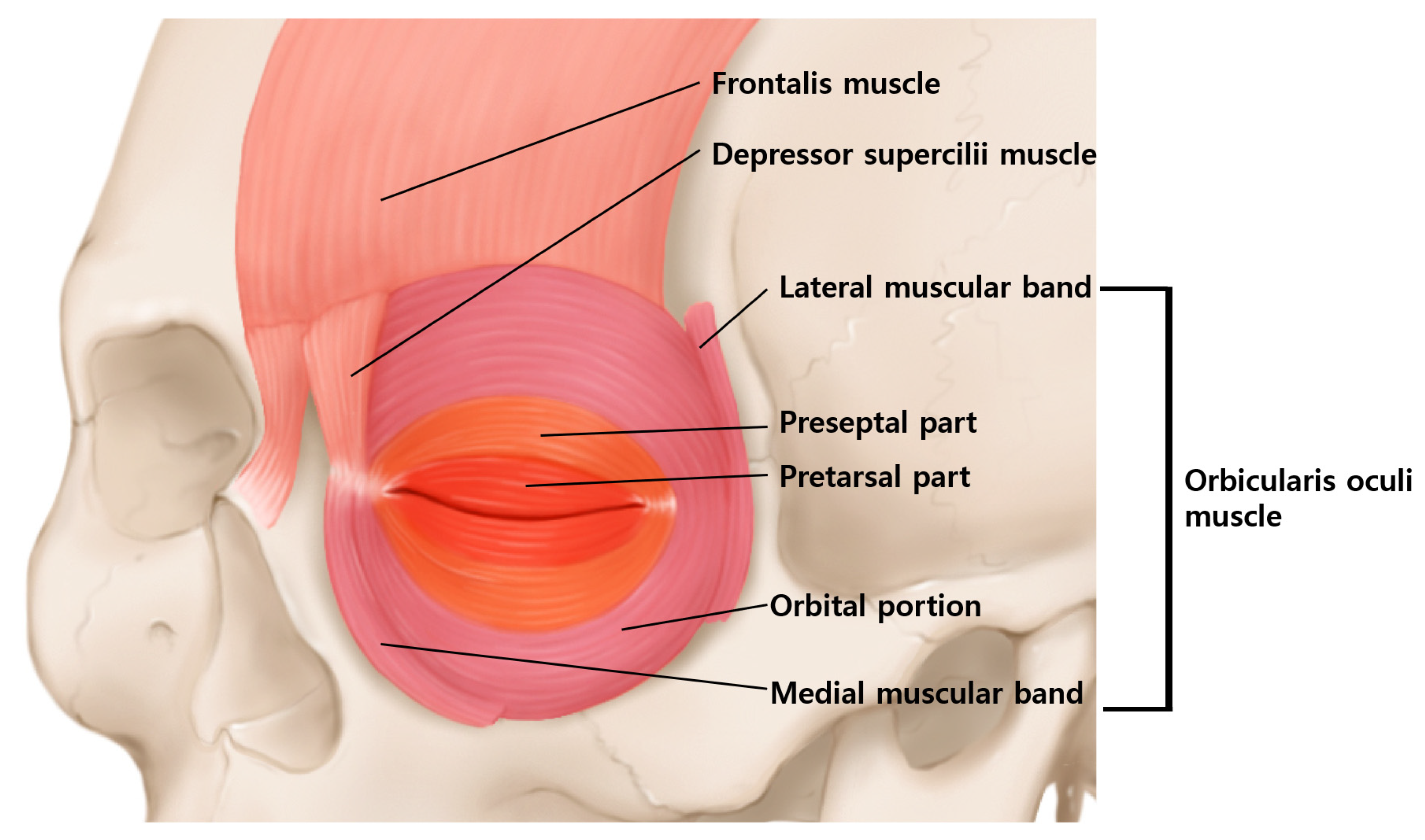
2. Anatomy of the Orbicularis Oculi Muscle
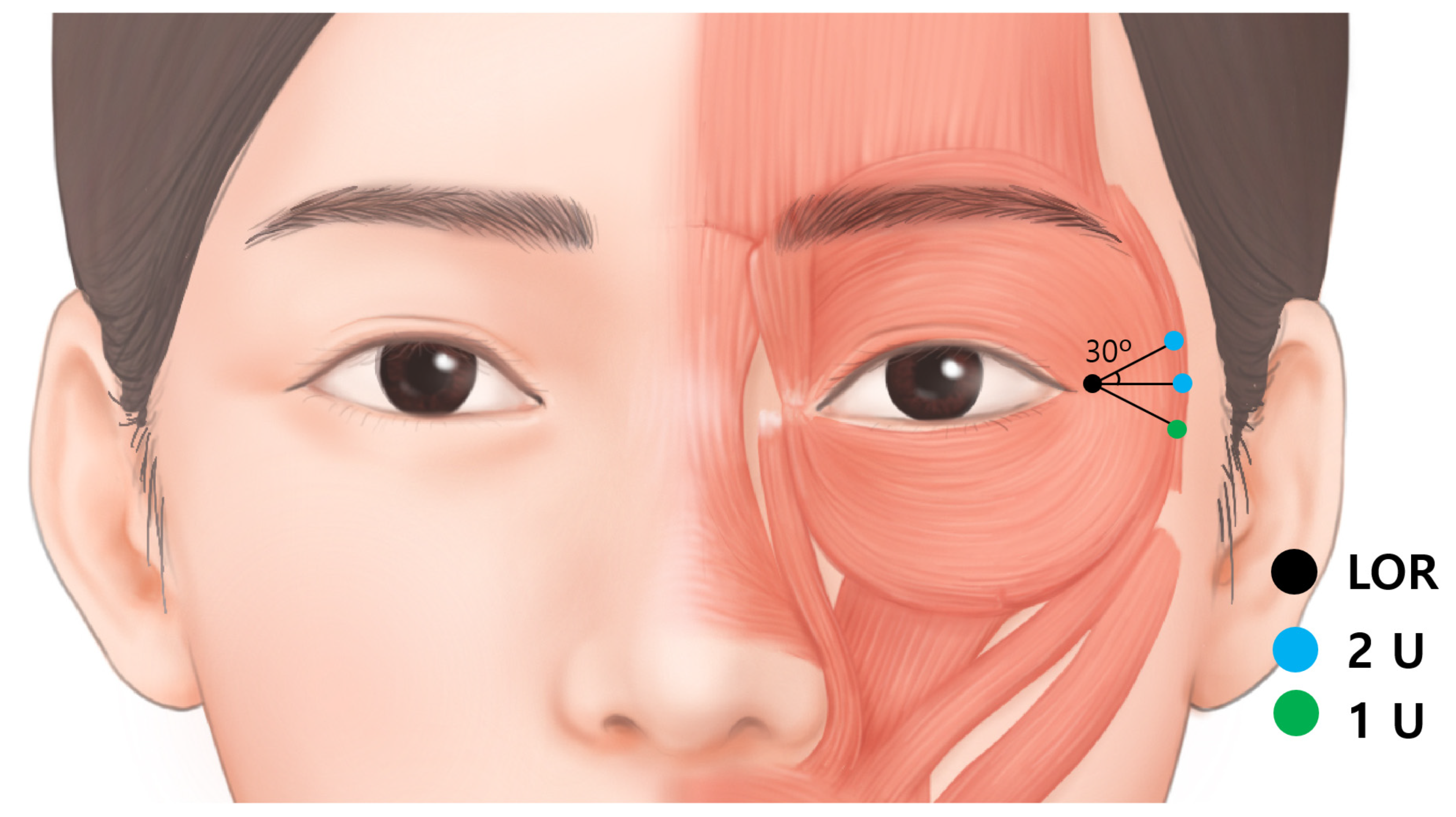
3. Injection Points for Lateral Canthal Rhytids
4. Depth
5. Medial Zygomaticotemporal Vein
6. Inferior Palpebral Vein
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dessy, L.A.; Mazzocchi, M.; Rubino, C.; Mazzarello, V.; Spissu, N.; Scuderi, N. An objective assessment of botulinum toxin A effect on superficial skin texture. Ann. Plast. Surg. 2007, 58, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Childers, M.K. Targeting the neuromuscular junction in skeletal muscles. Am. J. Phys. Med. Rehabil. 2004, 83, S38–S44. [Google Scholar] [CrossRef]
- Wutthiphan, S.; Kowal, L.; O’Day, J.; Jones, S.; Price, J. Diplopia following subcutaneous injections of botulinum A toxin for facial spasms. J. Pediatr. Ophthalmol. Strabismus 1997, 34, 229–234. [Google Scholar] [CrossRef]
- Lee, J.J.; Jeon, H.S.; Choi, H.Y. Three Cases of Esotropia after Cosmetic Botulinum Toxin A Use in the Eyelid. J. Korean Ophthalmol. Soc. 2015, 56, 799–802. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.S.; Miller, N.R. Botulinum toxin injection causing lateral rectus palsy. Br. J. Ophthalmol. 2007, 91, 843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aristodemou, P.; Watt, L.; Baldwin, C.; Hugkulstone, C. Diplopia associated with the cosmetic use of botulinum toxin a for facial rejuvenation. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Hsu, T.S.; Dover, J.S.; Arndt, K.A. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch. Dermatol. 2004, 140, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Kinnett, D. Botulinum toxin A injections in children: Technique and dosing issues. Am. J. Phys. Med. Rehabil. 2004, 83, S59–S64. [Google Scholar] [CrossRef] [PubMed]
- Lepage, D.; Parratte, B.; Tatu, L.; Vuiller, F.; Monnier, G. Extra- and intramuscular nerve supply of the muscles of the anterior antebrachial compartment: Applications for selective neurotomy and for botulinum toxin injection. Surg. Radiol. Anat. 2005, 27, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Pingel, J.; Nielsen, M.S.; Lauridsen, T.; Rix, K.; Bech, M.; Alkjaer, T.; Andersen, I.T.; Nielsen, J.B.; Feidenhansl, R. Injection of high dose botulinum-toxin A leads to impaired skeletal muscle function and damage of the fibrilar and non-fibrilar structures. Sci. Rep. 2017, 7, 14746. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.-H.; Lee, J.-H.; Hu, H.-W.; Kim, H.-J. Novel Anatomical Guidelines on Botulinum Neurotoxin Injection for Wrinkles in the Nose Region. Toxins 2022, 14, 342. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, J.H.; Hu, H.W.; Kim, H.J. Anatomical Proposal for Botulinum Neurotoxin Injection for Glabellar Frown Lines. Toxins 2022, 14, 268. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Seo, K.K.; Lee, H.; Kim, J. Clinical anatomy of the face for filler and botulinum toxin injection. Turk Derm. Derg. 2016, 10, 135. [Google Scholar]
- Park, J.T.; Youn, K.H.; Hur, M.S.; Hu, K.S.; Kim, H.J.; Kim, H.J. Malaris muscle, the lateral muscular band of orbicularis oculi muscle. J. Craniofac. Surg. 2011, 22, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Borodic, G.E.; Ferrante, R.; Pearce, L.B.; Smith, K. Histologic assessment of dose-related diffusion and muscle fiber response after therapeutic botulinum A toxin injections. Mov. Disord. 1994, 9, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Castaneda, J.; Jankovic, J.; Comella, C.; Dashtipour, K.; Fernandez, H.H.; Mari, Z. Diffusion, spread, and migration of botulinum toxin. Mov. Disord. 2013, 28, 1775–1783. [Google Scholar] [CrossRef] [PubMed]
- Cvetko, E. A case of an unusual arrangement of numerous tributaries to the middle temporal vein and its fenestration. Surg Radiol. Anat. 2013, 35, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Nestor, M.S.; Han, H.; Gade, A.; Fischer, D.; Saban, Y.; Polselli, R. Botulinum toxin-induced blepharoptosis: Anatomy, etiology, prevention, and therapeutic options. J. Cosmet. Dermatol. 2021, 20, 3133–3146. [Google Scholar] [CrossRef]
- Kwon, K.H.; Shin, K.S.; Yeon, S.H.; Kwon, D.G. Application of botulinum toxin in maxillofacial field: Part II. Wrinkle, intraoral ulcer, and cranio-maxillofacial pain. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 42. [Google Scholar] [CrossRef]
- Seo, K.K. Botulinum Toxin for Asians; Springer: Singapore, 2017. [Google Scholar]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, K.-H.; Lee, J.-H.; Kim, G.-Y.; Yoon, S.-W.; Oh, W.; Kim, H.-J. Novel Anatomical Proposal for Botulinum Neurotoxin Injection Targeting Lateral Canthal Rhytids. Toxins 2022, 14, 462. https://doi.org/10.3390/toxins14070462
Yi K-H, Lee J-H, Kim G-Y, Yoon S-W, Oh W, Kim H-J. Novel Anatomical Proposal for Botulinum Neurotoxin Injection Targeting Lateral Canthal Rhytids. Toxins. 2022; 14(7):462. https://doi.org/10.3390/toxins14070462
Chicago/Turabian StyleYi, Kyu-Ho, Ji-Hyun Lee, Ga-Young Kim, Seong-Wook Yoon, Wook Oh, and Hee-Jin Kim. 2022. "Novel Anatomical Proposal for Botulinum Neurotoxin Injection Targeting Lateral Canthal Rhytids" Toxins 14, no. 7: 462. https://doi.org/10.3390/toxins14070462
APA StyleYi, K. -H., Lee, J. -H., Kim, G. -Y., Yoon, S. -W., Oh, W., & Kim, H. -J. (2022). Novel Anatomical Proposal for Botulinum Neurotoxin Injection Targeting Lateral Canthal Rhytids. Toxins, 14(7), 462. https://doi.org/10.3390/toxins14070462