A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Assessment of Risk of Bias and Quality of Evidence
2.5. Statistical Analysis
3. Results
3.1. Study Selection
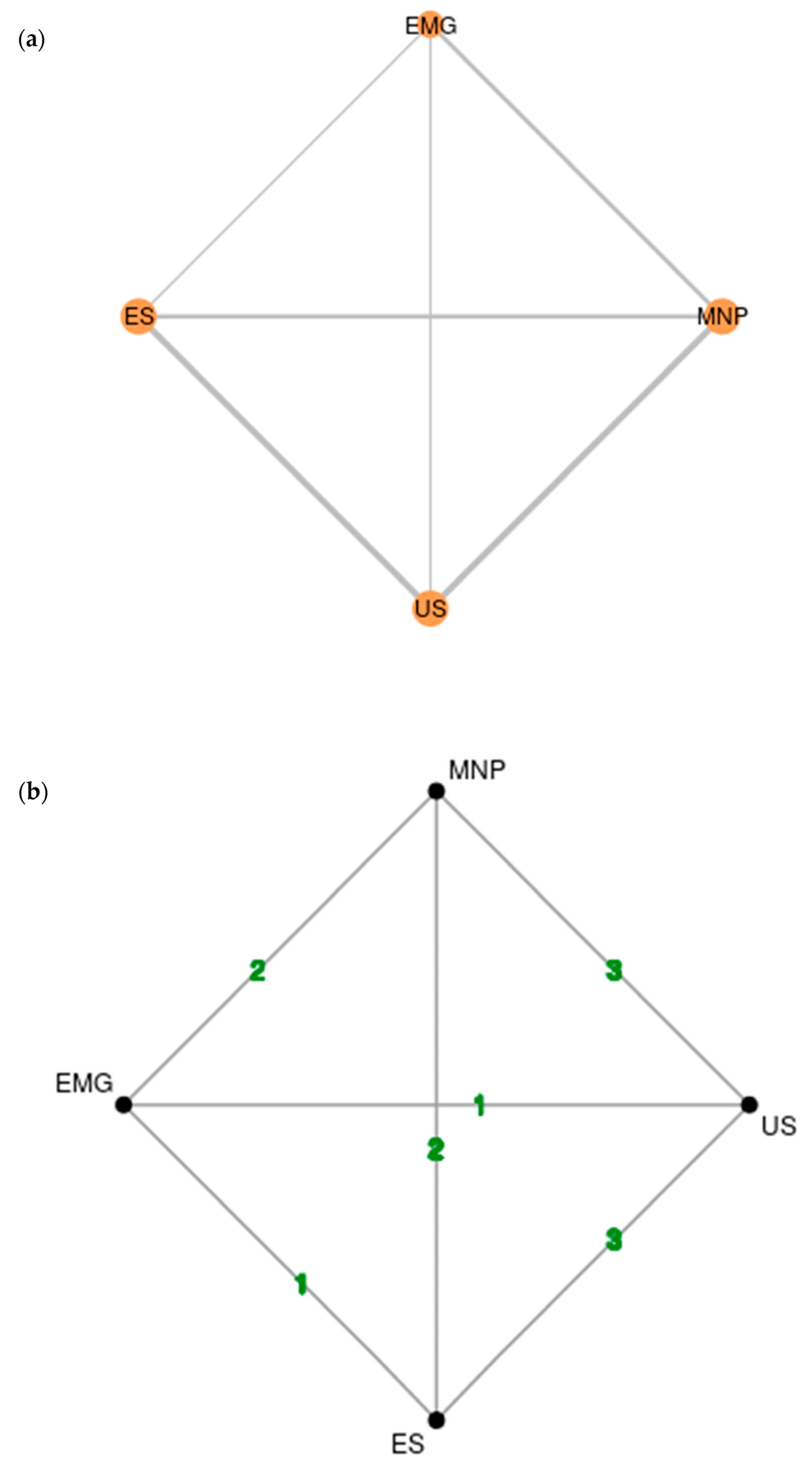
3.2. Network Structure and Geometry
3.3. Characteristics and Quality Assessment of Individual Studies
3.4. Bayesian Network Meta-Analysis Results
3.5. Assessment of Heterogeneity, Consistency and Transitivity
3.6. Assessment of Model Convergence and Measures of Fit
3.7. Additional Analyses
4. Discussion
5. Recommendations for Clinicians
6. Future Perspectives
7. Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AS | Ashworth Scale |
| BoNT | botulinum neurotoxin |
| DAS | Disability Assessment Scale |
| Dbar | posterior mean of the residual deviance |
| DIC | Deviance Information Criterion |
| EQ-5D | Quality-of-Life Scale |
| EMG | electromyography |
| ES | electrical stimulation |
| f | female |
| GRADE | Grading of Recommendations Assessment, Development and Evaluation |
| m | male |
| MAS | Modified Ashworth Scale |
| MCMC | Markov Chain Monte Carlo |
| MD | mean difference |
| MNP | manual needle placement |
| n | number |
| NA | not available |
| NMA | Network meta-analysis model |
| pD | effective degrees of freedom |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROM | ankle passive dorsiflexion range of motion |
| RCT | Randomized controlled trial |
| RoB 2 tool | revised Cochrane risk-of-bias tool for randomized studies |
| RMS-EMG | root mean square of surface electromyographic activity during the Ashworth maneuver |
| RT | Randomized trial |
| sd/SD | standard deviation |
| SUCRA | surface under the cumulative ranking curve |
| TCA | Tardieu catch angle |
| TSA | Tardieu spasticity angle |
| U | units |
| UME | unrelated mean effect |
| US | ultrasound |
| w | week |
| 10 mWT | 10 m walking test |
| 95% CrI | Credible interval |
References
- Lim, E.C.; Seet, R.C. Use of botulinum toxin in the neurology clinic. Nat. Rev. Neurol. 2010, 6, 624–636. [Google Scholar] [CrossRef]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice Guideline Update Summary: Botulinum Neurotoxin for the Treatment of Blepharospasm, Cervical Dystonia, Adult Spasticity, and Headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [Green Version]
- Dressler, D.; Bhidayasiri, R.; Bohlega, S.; Chahidi, A.; Chung, T.M.; Ebke, M.; Jacinto, L.J.; Kaji, R.; Koçer, S.; Kanovsky, P.; et al. Botulinum Toxin Therapy for Treatment of Spasticity in Multiple Sclerosis: Review and Recommendations of the IAB Interdisciplinary Working Group for Movement Disorders Task Force. J. Neurol. 2017, 264, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Schulte-Mattler, W.J. Use of botulinum toxin A in adult neurological disorders: Efficacy, tolerability and safety. CNS Drugs. 2008, 22, 725–738. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, C.F. Injection techniques for botulinum toxin using electromyography and electrical stimulation. Muscle Nerve Suppl. 1997, 6, S176–S180. [Google Scholar] [CrossRef]
- Montecucco, C.; Schiavo, G. Mechanism of action of tetanus and botulinum neurotoxins. Mol. Microbiol. 1994, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. How Do I Inject Botulinum Toxin Into the Lateral and Medial Pterygoid Muscles? Mov. Disord. Clin. Pract. 2016, 4, 285. [Google Scholar] [CrossRef] [Green Version]
- Sconfienza, L.M.; Perrone, N.; Lacelli, F.; Lentino, C.; Serafini, G. Ultrasound-guided injection of botulinum toxin A in the treatment of iliopsoas spasticity. J. Ultrasound. 2008, 11, 113–117. [Google Scholar] [CrossRef] [Green Version]
- Mashayekh, A.; Christo, P.J.; Yousem, D.M.; Pillai, J.J. CT-guided injection of the anterior and middle scalene muscles: Technique and complications. AJNR Am. J. Neuroradiol. 2011, 32, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Lim, E.C.; Seet, R.C.; Cheah, A.E.; Lim, A.Y. Injection of botulinum toxin to the extensor carpi radialis brevis for tennis elbow. J. Hand Surg. Eur. Vol. 2010, 35, 425–426. [Google Scholar] [CrossRef]
- Lance, J.W. The control of muscle tone, reflexes, and movement: Robert Wartenberg Lecture. Neurology 1980, 30, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Gracies, J.M. Pathophysiology of spastic paresis. II: Emergence of muscle overactivity. Muscle Nerve 2005, 31, 552–571. [Google Scholar] [CrossRef] [PubMed]
- Lackritz, H.; Parmet, Y.; Frenkel-Toledo, S.; Baniña, M.C.; Soroker, N.; Solomon, J.M.; Liebermann, D.G.; Levin, M.F.; Berman, S. Effect of post-stroke spasticity on voluntary movement of the upper limb. J. Neuroeng. Rehabil. 2021, 18, 81. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, H.J.; Lee, J.H.; Lee, K.L.; Kim, H.J. Effective botulinum neurotoxin injection in treating iliopsoas spasticity. Clin. Anat. 2021, 34, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, J.H.; Lee, D.K.; Hu, H.W.; Seo, K.K.; Kim, H.J. Anatomical locations of the motor endplates of sartorius muscle for botulinum toxin injections in treatment of muscle spasticity. Surg. Radiol. Anat. 2021, 43, 2025–2030. [Google Scholar] [CrossRef]
- Lim, E.C.; Quek, A.M.; Seet, R.C. Accurate targeting of botulinum toxin injections: How to and why. Parkinsonism Relat. Disord. 2011, 17 (Suppl. S1), S34–S39. [Google Scholar] [CrossRef]
- Kaplan, J.B. Consideration of Muscle Depth for Botulinum Toxin Injections: A Three-Dimensional Approach. Plast. Surg. Nurs. 2019, 39, 52–58. [Google Scholar] [CrossRef]
- Gervasio, A.; D’Orta, G.; Mujahed, I.; Biasio, A. Sonographic anatomy of the neck: The suprahyoid region. J. Ultrasound. 2011, 14, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Crowner, B.E.; Torres-Russotto, D.; Carter, A.R.; Racette, B.A. Systemic weakness after therapeutic injections of botulinum toxin a: A case series and review of the literature. Clin. Neuropharmacol. 2010, 33, 243–247. [Google Scholar] [CrossRef]
- Yang, E.J.; Rha, D.W.; Yoo, J.K.; Park, E.S. Accuracy of manual needle placement for gastrocnemius muscle in children with cerebral palsy checked against ultrasonography. Arch. Phys. Med. Rehabil. 2009, 90, 741–744. [Google Scholar] [CrossRef]
- Schnitzler, A.; Roche, N.; Denormandie, P.; Lautridou, C.; Parratte, B.; Genet, F. Manual needle placement: Accuracy of botulinum toxin A injections. Muscle Nerve 2012, 46, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Elovic, E.P.; Esquenazi, A.; Alter, K.E.; Lin, J.L.; Alfaro, A.; Kaelin, D.L. Chemodenervation and nerve blocks in the diagnosis and management of spasticity and muscle overactivity. PM R 2009, 1, 842–851. [Google Scholar] [CrossRef]
- Walter, U.; Dressler, D. Ultrasound-guided botulinum toxin injections in neurology: Technique, indications and future perspectives. Expert. Rev. Neurother. 2014, 14, 923–936. [Google Scholar] [CrossRef] [PubMed]
- Schramm, A.; Bäumer, T.; Fietzek, U.; Heitmann, S.; Walter, U.; Jost, W.H. Relevance of sonography for botulinum toxin treatment of cervical dystonia: An expert statement. J. Neural. Transm. 2015, 122, 1457–1463. [Google Scholar] [CrossRef] [Green Version]
- Esquenazi, A.; Alfaro, A.; Ayyoub, Z.; Charles, D.; Dashtipour, K.; Graham, G.D.; McGuire, J.R.; Odderson, I.R.; Patel, A.T.; Simpson, D.M. OnabotulinumtoxinA for Lower Limb Spasticity: Guidance From a Delphi Panel Approach. PM R 2017, 9, 960–968. [Google Scholar] [CrossRef] [Green Version]
- McGuire, J.; Heath, K.; O’Dell, M.W. Should Ultrasound Be Used Routinely to Guide Botulinum Toxin Injections for Spasticity? PM R 2016, 8, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Xue, F.; Chang, W.; Lian, Y.; Zheng, Y.; Xie, N.; Zhang, L.; Chen, C. Botulinum toxin type A with or without needle electromyographic guidance in patients with cervical dystonia. Springerplus 2016, 5, 1292. [Google Scholar] [CrossRef] [Green Version]
- Kreisler, A.; Djelad, S.; Simonin, C.; Baille, G.; Mutez, E.; Degardin, A.; Defebvre, L.; Labreuche, J.; Cailliau, E.; Duhamel, A. Does ultrasound-guidance improve the outcome of botulinum toxin injections in cervical dystonia? Rev. Neurol 2022, 178, 591–602. [Google Scholar] [CrossRef]
- Comella, C.L.; Buchman, A.S.; Tanner, C.M.; Brown-Toms, N.C.; Goetz, C.G. Botulinum toxin injection for spasmodic torticollis: Increased magnitude of benefit with electromyographic assistance. Neurology 1992, 42, 878–882. [Google Scholar] [CrossRef]
- Grigoriu, A.I.; Dinomais, M.; Rémy-Néris, O.; Brochard, S. Impact of Injection-Guiding Techniques on the Effectiveness of Botulinum Toxin for the Treatment of Focal Spasticity and Dystonia: A Systematic Review. Arch. Phys. Med. Rehabil. 2015, 96, 2067–2078. [Google Scholar] [CrossRef]
- Alter, K.E.; Karp, B.I. Ultrasound Guidance for Botulinum Neurotoxin Chemodenervation Procedures. Toxins 2017, 10, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, H.W.; Lee, M.Y.; Bahroo, L.B.; Hedera, P.; Charles, D. Botulinum toxin injection techniques for the management of adult spasticity. PM R 2015, 7, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.K.; Finlayson, H.; Mills, P.B. Does the method of botulinum neurotoxin injection for limb spasticity affect outcomes? A systematic review. Clin. Rehabil. 2017, 31, 713–721. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.T.; Zhang, C.; Liu, Y.; Magat, E.; Verduzco-Gutierrez, M.; Francisco, G.E.; Zhou, P.; Zhang, Y.; Li, S. The Effects of Botulinum Toxin Injections on Spasticity and Motor Performance in Chronic Stroke with Spastic Hemiplegia. Toxins 2020, 12, 492. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 4 January 2023).
- Salanti, G.; Del Giovane, C.; Chaimani, A.; Caldwell, D.M.; Higgins, J.P. Evaluating the quality of evidence from a network meta-analysis. PLoS ONE 2014, 9, e99682. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions; version 6.3; Cochrane: London, UK, 2022; Available online: https://training.cochrane.org/handbook (accessed on 1 February 2023).
- Rouse, B.; Chaimani, A.; Li, T. Network meta-analysis: An introduction for clinicians. Intern. Emerg. Med. 2017, 12, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Watt, J.; Del Giovane, C. Network Meta-Analysis. Methods Mol. Biol. 2022, 2345, 187–201. [Google Scholar] [CrossRef]
- Phillips, M.R.; Steel, D.H.; Wykoff, C.C.; Busse, J.W.; Bannuru, R.R.; Thabane, L.; Bhandari, M.; Chaudhary, V.; Retina Evidence Trials InterNational Alliance (R.E.T.I.N.A.) Study Group. A clinician’s guide to network meta-analysis. Eye 2022, 36, 1523–1526. [Google Scholar] [CrossRef] [PubMed]
- Owen, R.K.; Bradbury, N.; Xin, Y.; Cooper, N.; Sutton, A. MetaInsight: An interactive web-based tool for analyzing, interrogating, and visualizing network meta-analyses using R-shiny and netmeta. Res. Synth. Methods 2019, 10, 569–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackenberger, B.K. Bayesian meta-analysis now-let’s do it. Croat. Med. J. 2020, 61, 564–568. [Google Scholar] [CrossRef]
- Sadeghirad, B.; Foroutan, F.; Zoratti, M.J.; Busse, J.W.; Brignardello-Petersen, R.; Guyatt, G.; Thabane, L. Theory and practice of Bayesian and frequentist frameworks for network meta-analysis. BMJ Evid. Based. Med, 2022; Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Franchini, A.J.; Dias, S.; Ades, A.E.; Jansen, J.P.; Welton, N.J. Accounting for correlation in network meta-analysis with multi-arm trials. Res. Synth. Methods. 2012, 3, 142–160. [Google Scholar] [CrossRef]
- Dressler, D.; Altavista, M.C.; Altenmueller, E.; Bhidayasiri, R.; Bohlega, S.; Chana, P.; Chung, T.M.; Colosimo, C.; Fheodoroff, K.; Garcia-Ruiz, P.J.; et al. Consensus guidelines for botulinum toxin therapy: General algorithms and dosing tables for dystonia and spasticity. J. Neural Transm. 2021, 128, 321–335. [Google Scholar] [CrossRef]
- Wissel, J.; Ward, A.B.; Erztgaard, P.; Bensmail, D.; Hecht, M.J.; Lejeune, T.M.; Schnider, P.; Altavista, M.C.; Cavazza, S.; Deltombe, T.; et al. European consensus table on the use of botulinum toxin type A in adult spasticity. J. Rehabil. Med. 2009, 41, 13–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglione, F. Conversion Ratio between Botox®, Dysport®, and Xeomin® in Clinical Practice. Toxins 2016, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Review Manager (RevMan) [Computer Program]. Version 5.4. The Cochrane Collaboration. 2020. Available online: https://training.cochrane.org/system/files/uploads/protected_file/RevMan5.4_user_guide.pdf (accessed on 15 January 2023).
- Turna, I.F.; Erhan, B.; Gunduz, N.B.; Turna, O. The effects of different injection techniques of botulinum toxin a in post-stroke patients with plantar flexor spasticity. Acta Neurol Belg. 2020, 120, 639–643. [Google Scholar] [CrossRef]
- Zeuner, K.E.; Knutzen, A.; Kühl, C.; Möller, B.; Hellriegel, H.; Margraf, N.G.; Deuschl, G.; Stolze, H. Functional impact of different muscle localization techniques for Botulinum neurotoxin A injections in clinical routine management of post-stroke spasticity. Brain Inj. 2017, 31, 75–82. [Google Scholar] [CrossRef]
- Picelli, A.; Lobba, D.; Midiri, A.; Prandi, P.; Melotti, C.; Baldessarelli, S.; Smania, N. Botulinum toxin injection into the forearm muscles for wrist and fingers spastic overactivity in adults with chronic stroke: A randomized controlled trial comparing three injection techniques. Clin. Rehabil. 2014, 28, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Ploumis, A.; Varvarousis, D.; Konitsiotis, S.; Beris, A. Effectiveness of botulinum toxin injection with and without needle electromyographic guidance for the treatment of spasticity in hemiplegic patients: A randomized controlled trial. Disabil. Rehabil. 2014, 36, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Tamburin, S.; Bonetti, P.; Fontana, C.; Barausse, M.; Dambruoso, F.; Gajofatto, F.; Santilli, V.; Smania, N. Botulinum toxin type A injection into the gastrocnemius muscle for spastic equinus in adults with stroke: A randomized controlled trial comparing manual needle placement, electrical stimulation and ultrasonography-guided injection techniques. Am. J. Phys. Med. Rehabil. 2012, 91, 957–964. [Google Scholar] [CrossRef]
- Mayer, N.H.; Whyte, J.; Wannstedt, G.; Ellis, C.A. Comparative impact of 2 botulinum toxin injection techniques for elbow flexor hypertonia. Arch. Phys. Med. Rehabil. 2008, 89, 982–987. [Google Scholar] [CrossRef]
- Lau, J.; Ioannidis, J.P.; Terrin, N.; Schmid, C.H.; Olkin, I. The case of the misleading funnel plot. BMJ 2006, 333, 597–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, S.; Ades, A.E.; Welton, N.J.; Jansen, J.P.; Sutton, A.J. Model fit, model comparison and outlier detection. In Network Meta-Anlaysis for Decision-Making; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2018; pp. 59–91. [Google Scholar]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Van Der Linde, A. Bayesian measures of model complexity and fit. J. R Stat. Soc. Series B Stat. Methodol. 2002, 64, 583–639. [Google Scholar] [CrossRef] [Green Version]
- Lannin, N.A.; Ada, L.; English, C.; Ratcliffe, J.; Faux, S.; Palit, M.; Gonzalez, S.; Olver, J.; Schneider, E.; Crotty, M.; et al. Long-term effect of additional rehabilitation following botulinum toxin-A on upper limb activity in chronic stroke: The InTENSE randomised trial. BMC Neurol. 2022, 22, 154. [Google Scholar] [CrossRef]
- Kinnear, B.Z.; Lannin, N.A.; Cusick, A.; Harvey, L.A.; Rawicki, B. Rehabilitation therapies after botulinum toxin-A injection to manage limb spasticity: A systematic review. Physical. Therapy 2014, 94, 1569–1581. [Google Scholar] [CrossRef] [Green Version]
- Pandyan, A.D.; Johnson, G.R.; Price, C.I.; Curless, R.H.; Barnes, M.P.; Rodgers, H. A review of the properties and limitations of the Ashworth and modified Ashworth Scales as measures of spasticity. Clin. Rehabil. 1999, 13, 373–383. [Google Scholar] [CrossRef]
- Ansari, N.N.; Naghdi, S.; Moammeri, H.; Jalaie, S. Ashworth Scales are unreliable for the assessment of muscle spasticity. Physiother. Theory Pract. 2006, 22, 119–125. [Google Scholar] [CrossRef]
- Zurawski, E.; Behm, K.; Dunlap, C.; Koo, J.; Ismail, F.; Boulias, C.; Reid, S.; Phadke, C.P. Interrater Reliability of the Modified Ashworth Scale with Standardized Movement Speeds: A Pilot Study. Physiother. Can. 2019, 71, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, M.; van Vliet, P.; Mockett, S.P. Reliability of measurements obtained with the modified Ashworth scale in the lower extremities of people with stroke. Phys. Ther. 2002, 82, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Brashear, A.; Zafonte, R.; Corcoran, M.; Galvez-Jimenez, N.; Gracies, J.M.; Gordon, M.F.; McAfee, A.; Ruffing, K.; Thompson, B.; Williams, M.; et al. Inter- and intrarater reliability of the Ashworth Scale and the Disability Assessment Scale in patients with upper-limb poststroke spasticity. Arch. Phys. Med. Rehabil. 2002, 83, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Gregson, J.M.; Leathley, M.; Moore, A.P.; Sharma, A.K.; Smith, T.L.; Watkins, C.L. Reliability of the Tone Assessment Scale and the modified Ashworth scale as clinical tools for assessing poststroke spasticity. Arch. Phys. Med. Rehabil. 1999, 80, 1013–1016. [Google Scholar] [CrossRef] [PubMed]
- Akpinar, P.; Atici, A.; Ozkan, F.U.; Aktas, I.; Kulcu, D.G.; Sarı, A.; Durmus, B. Reliability of the Modified Ashworth Scale and Modified Tardieu Scale in patients with spinal cord injuries. Spinal. Cord. 2017, 55, 944–949. [Google Scholar] [CrossRef]
- Mehrholz, J.; Wagner, K.; Meissner, D.; Grundmann, K.; Zange, C.; Koch, R.; Pohl, M. Reliability of the Modified Tardieu Scale and the Modified Ashworth Scale in adult patients with severe brain injury: A comparison study. Clinical. Rehabil. 2005, 19, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Shu, X.; McConaghy, C.; Knight, A. Validity and reliability of the Modified Tardieu Scale as a spasticity outcome measure of the upper limbs in adults with neurological conditions: A systematic review and narrative analysis. BMJ Open 2021, 11, e050711. [Google Scholar] [CrossRef]
- Shaari, C.M.; Sanders, I. Quantifying how location and dose of botulinum toxin injections affect muscle paralysis. Muscle Nerve 1993, 16, 964–969. [Google Scholar] [CrossRef]
- Childers, M.K.; Kornegay, J.N.; Aoki, R.; Otaviani, L.; Bogan, D.J.; Petroski, G. Evaluating motor end-plate-targeted injections of botulinum toxin type A in a canine model. Muscle Nerve 1998, 21, 653–655. [Google Scholar] [CrossRef]
- Gracies, J.M.; Lugassy, M.; Weisz, D.J.; Vecchio, M.; Flanagan, S.; Simpson, D.M. Botulinum toxin dilution and endplate targeting in spasticity: A double-blind controlled study. Arch. Phys. Med. Rehabil. 2009, 90, 9–16.e2. [Google Scholar] [CrossRef]
- Lapatki, B.G.; van Dijk, J.P.; van de Warrenburg, B.P.; Zwarts, M.J. Botulinum toxin has an increased effect when targeted toward the muscle’s endplate zone: A high-density surface EMG guided study. Clin. Neurophysiol. 2011, 122, 1611–1616. [Google Scholar] [CrossRef] [PubMed]
- Van Campenhout, A.; Molenaers, G. Localization of the motor endplate zone in human skeletal muscles of the lower limb: Anatomical guidelines for injection with botulinum toxin. Dev. Med. Child. Neurol. 2011, 53, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Boon, A.J.; Oney-Marlow, T.M.; Murthy, N.S.; Harper, C.M.; McNamara, T.R.; Smith, J. Accuracy of electromyography needle placement in cadavers: Non-guided vs. ultrasound guided. Muscle Nerve 2011, 44, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.D.; Yun, S.I.; Ryoo, D.; Chung, M.E.; Park, J. Accuracy of Ultrasound-Guided and Non-guided Botulinum Toxin Injection Into Neck Muscles Involved in Cervical Dystonia: A Cadaveric Study. Ann. Rehabil. Med. 2020, 44, 370–377. [Google Scholar] [CrossRef]
- Jordan, S.E.; Ahn, S.S.; Gelabert, H.A. Combining ultrasonography and electromyography for botulinum chemodenervation treatment of thoracic outlet syndrome: Comparison with fluoroscopy and electromyography guidance. Pain. Physician 2007, 10, 541–546. [Google Scholar] [CrossRef]
- Feng, L.; Zhang, Z.; Malam Djibo, I.; Chen, S.; Li, B.; Pan, Y.; Zhang, X.; Xu, Y.; Su, J.; Ma, H.; et al. The efficacy of single-photon emission computed tomography in identifying dystonic muscles in cervical dystonia. Nucl. Med. Commun. 2020, 41, 651–658. [Google Scholar] [CrossRef]
- Zhang, C.; Chen, Y.T.; Liu, Y.; Magat, E.; Gutierrez-Verduzco, M.; Francisco, G.E.; Zhou, P.; Li, S.; Zhang, Y. Improving Botulinum Toxin Efficiency in Treating Post-Stroke Spasticity Using 3D Innervation Zone Imaging. Int. J. Neural Syst. 2021, 31, 2150007. [Google Scholar] [CrossRef]
- Yi, K.H.; Lee, J.H.; Hur, H.W.; Lee, H.J.; Choi, Y.J.; Kim, H.J. Distribution of the intramuscular innervation of the triceps brachii: Clinical importance in the treatment of spasticity with botulinum neurotoxin. Clin. Anat. 2023; Epub ahead of print. [Google Scholar] [CrossRef]
- Won, S.Y.; Rha, D.W.; Kim, H.S.; Jung, S.H.; Park, E.S.; Hu, K.S.; Kim, H.J. Intramuscular nerve distribution pattern of the adductor longus and gracilis muscles demonstrated with Sihler staining: Guidance for botulinum toxin injection. Muscle Nerve 2012, 46, 80–85. [Google Scholar] [CrossRef]
- Cote, M.P.; Lubowitz, J.H.; Brand, J.C.; Rossi, M.J. Understanding Network Meta-analysis (NMA) Conclusions Requires Scrutiny of Methods and Results: Introduction to NMA and the Geometry of Evidence. Arthroscopy 2021, 37, 2013–2016. [Google Scholar] [CrossRef]
- Li, T.; Puhan, M.A.; Vedula, S.S.; Singh, S.; Dickersin, K. Ad Hoc Network Meta-analysis Methods Meeting Working Group Network meta-analysis-highly attractive but more methodological research is needed. BMC Med. 2011, 9, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illomei, G.; Spinicci, G.; Locci, E.; Marrosu, M.G. Muscle elastography: A new imaging technique for multiple sclerosis spasticity measurement. Neurol Sci. 2017, 38, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Rubin, J.M.; Chen, J.; O’Dell, M. Ultrasound Elastography to Assess Botulinum Toxin A Treatment for Post-stroke Spasticity: A Feasibility Study. Ultrasound Med. Biol. 2019, 45, 1094–1102. [Google Scholar] [CrossRef] [PubMed]
- Mathevon, L.; Michel, F.; Decavel, P.; Fernandez, B.; Parratte, B.; Calmels, P. Muscle structure and stiffness assessment after botulinum toxin type A injection. A systematic review. Ann. Phys. Rehabil. Med. 2015, 58, 343–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Type of Study | No of Patients (m/f) | Cause of Spasticity | Assessment Scales | Post-Injection Clinical Evaluation | Guidance Technique (n) | Type of Toxin (Brand Name) | Dilution | Injection Sites/Muscle (n) |
|---|---|---|---|---|---|---|---|---|---|
| Turna et al. (2018) [52] | Prospective cohort | 40 (23/17) | Ischemic or hemorrhagic stroke | Brunnstrom stage, Barthel Index, MAS, 10 mWT | 2 w 3 m | ES (20) US (20) | Abobotulinum toxin A (Dysport®) Onabotulinum toxin A (Botox®) | 1000 U in 2.5 mL NaCL 300 U in 2 mL NaCL | NA |
| Zeuner et al. (2016) [53] | Crossover RCT | 23 (10/13) | Ischemic or hemorrhagic stroke | Barthel Index, DAS, EQ-5D, MAS | 4 w | EMG (12) MNP (11) US (12) | Onabotulinum toxin A (Botox®) | 100 U in 2mL NaCL | NA |
| Picelli et al. (2014) [54] | Parallel-group RCT | 60 (32/28) | Ischemic or hemorrhagic stroke | MAS, PROM, TSA | 4 w | ES (20) MNP (20) US (20) | Abobotulinum toxin A (Dysport®) | 500 U in 2 mL NaCL | 1 |
| Ploumis et al. (2013) [55] | Parallel-group RCT | 27 (7/20) | Stroke, traumatic brain injury, spinal cord injury, cerebral palsy, hypoxic encephalopathy | Barthel Index, MAS | 3 w 3 m | EMG (15) MNP (12) | Onabotulinum toxin A (Botox®) | 100 U in 1 mL NaCL | 1–2 |
| Picelli et al. (2012) [56] | Parallel-group RCT | 47 (31/16) | Ischemic or hemorrhagic stroke | MAS, PROM, TSA | 4 w | ES (15) MNP (15) US (17) | Onabotulinum toxin A (Botox®) | 100 U in 2 mL NaCL | 2 |
| Mayer et al. (2008) [57] | Parallel-group RT | 36 (18/18) (elbows) | Stroke, traumatic brain injury, hypoxic encephalopathy | AS *, RMS-EMG, TCA ** | 3 w | EMG (18) ES (18) | Onabotulinum toxin A (Botox®) | 60 U in 2.4 mL NaCL and 30 U in 1.2 mL NaCL | 1 site in motor point injections 4 (biceps) and 2 (brachioradialis) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asimakidou, E.; Sidiropoulos, C. A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity. Toxins 2023, 15, 256. https://doi.org/10.3390/toxins15040256
Asimakidou E, Sidiropoulos C. A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity. Toxins. 2023; 15(4):256. https://doi.org/10.3390/toxins15040256
Chicago/Turabian StyleAsimakidou, Evridiki, and Christos Sidiropoulos. 2023. "A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity" Toxins 15, no. 4: 256. https://doi.org/10.3390/toxins15040256
APA StyleAsimakidou, E., & Sidiropoulos, C. (2023). A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity. Toxins, 15(4), 256. https://doi.org/10.3390/toxins15040256