Addressing the Real-World Challenges of Immunoresistance to Botulinum Neurotoxin A in Aesthetic Practice: Insights and Recommendations from a Panel Discussion in Hong Kong

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results of the Panel Discussion
2.1. Clinical and Real-World Evidence on Immunoresistance to BoNT-A in Aesthetic Practice
2.2. Consumer Awareness and Perspectives on Diminishing BoNT-A Treatment Efficacy over Time
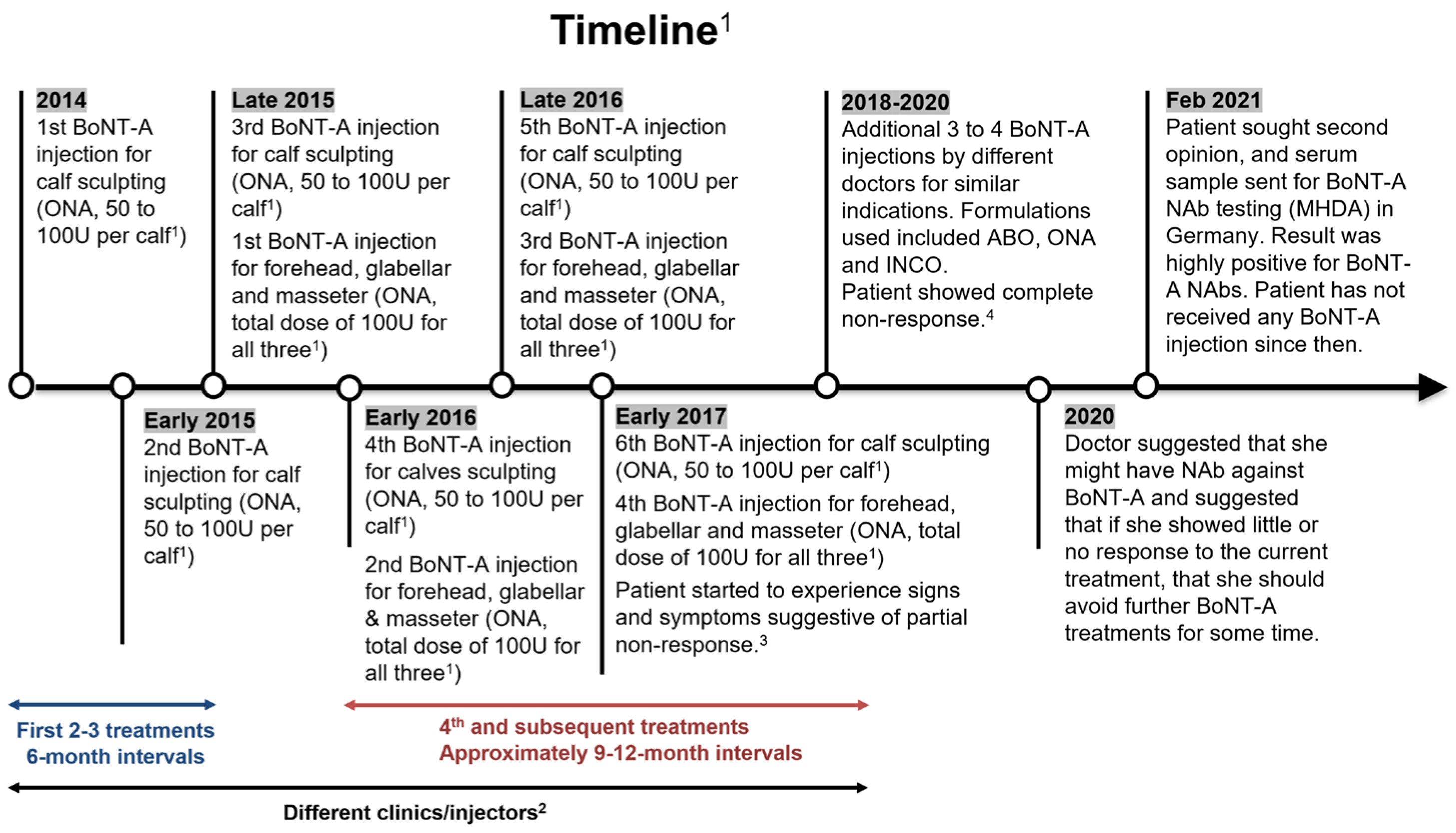
2.3. Patient Case Discussion
3. Discussion
3.1. Treatment Considerations for Best Clinical Practice
3.1.1. Be Aware of the Possibility and Long-Term Implications of BoNT-A Immunoresistance
3.1.2. Optimize Patient Journey and Consultation Process
3.1.3. Design Treatment Plan: Toxin Choice Is Important
3.1.4. Recognize and Deal with Signs of Diminishing Efficacy
3.2. The Role of Healthcare Professionals
4. Conclusions
5. Materials and Methods
5.1. Consumer Study
5.2. Panel Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Society of Plastic Surgeons. Plastic Surgery Statistics Report. 2020. Available online: https://www.plasticsurgery.org/documents/News/Statistics/2020/plastic-surgery-statistics-full-report-2020.pdf (accessed on 30 March 2023).
- Padda, I.S.; Tadi, P. Botulinum Toxin. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557387/ (accessed on 30 March 2023).
- The Aesthetic Society. Aesthetic Plastic Surgery National Databank Statistics 2020–2021. Available online: https://cdn.surgery.org/media/statistics/2021-TheAestheticSocietyStatistics.pdf (accessed on 30 June 2023).
- Sundaram, H.; Huang, P.H.; Hsu, N.J.; Huh, C.H.; Wu, W.T.; Wu, Y.; Cassuto, D.; Kerscher, M.J.; Seo, K.K.; Pan-Asian Aesthetics Toxin Consensus Group. Aesthetic Applications of Botulinum Toxin A in Asians: An International, Multidisciplinary, Pan-Asian Consensus. Plast. Reconstr. Surg. Glob. Open 2016, 4, e872. [Google Scholar] [CrossRef]
- Ho, W.W.S.; Albrecht, P.; Calderon, P.E.; Corduff, N.; Loh, D.; Martin, M.U.; Park, J.Y.; Suseno, L.S.; Tseng, F.W.; Vachiramon, V.; et al. Emerging Trends in Botulinum Neurotoxin A Resistance: An International Multidisciplinary Review and Consensus. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4407. [Google Scholar] [CrossRef]
- Phan, K.; Younessi, S.; Dubin, D.; Lin, M.J.; Khorasani, H. Emerging off-label esthetic uses of botulinum toxin in dermatology. Dermatol. Ther. 2022, 35, e15205. [Google Scholar] [CrossRef]
- Campanati, A.; Martina, E.; Giuliodori, K.; Consales, V.; Bobyr, I.; Offidani, A. Botulinum Toxin Off-Label Use in Dermatology: A Review. Ski. Appendage Disord. 2017, 3, 39–56. [Google Scholar] [CrossRef] [Green Version]
- Rho, N.K.; Han, K.H.; Kim, H.S. An Update on the Cosmetic Use of Botulinum Toxin: The Pattern of Practice among Korean Dermatologists. Toxins 2022, 14, 329. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, J.H.; Lee, K.; Hu, H.W.; Lee, H.J.; Kim, H.J. Anatomical Proposal for Botulinum Neurotoxin Injection Targeting the Platysma Muscle for Treating Platysmal Band and Jawline Lifting: A Review. Toxins 2022, 14, 868. [Google Scholar] [CrossRef] [PubMed]
- Torres, S.; Hamilton, M.; Sanches, E.; Starovatova, P.; Gubanova, E.; Reshetnikova, T. Neutralizing antibodies to botulinum neurotoxin type A in aesthetic medicine: Five case reports. Clin. Cosmet. Investig. Dermatol. 2014, 7, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Bellows, S.; Jankovic, J. Immunogenicity Associated with Botulinum Toxin Treatment. Toxins 2019, 11, 491. [Google Scholar] [CrossRef] [Green Version]
- Center for Drug Evaluation and Research; Center for Biologics Evaluation and Research. FDA Guidance for Industry—Immunogenicity Assessments for Therapeutic Protein Products. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/immunogenicity-assessment-therapeutic-protein-products (accessed on 30 March 2023).
- Frevert, J.; Ahn, K.Y.; Park, M.Y.; Sunga, O. Comparison of botulinum neurotoxin type A formulations in Asia. Clin. Cosmet. Investig. Dermatol. 2018, 11, 327–331. [Google Scholar] [CrossRef] [Green Version]
- Carruthers, A.; Kane, M.A.; Flynn, T.C.; Huang, P.; Kim, S.D.; Solish, N.; Kaeuper, G. The convergence of medicine and neurotoxins: A focus on botulinum toxin type A and its application in aesthetic medicine—A global, evidence-based botulinum toxin consensus education initiative: Part I: Botulinum toxin in clinical and cosmetic practice. Dermatol. Surg. 2013, 39, 493–509. [Google Scholar] [CrossRef]
- Kerscher, M.; Wanitphakdeedecha, R.; Trindade de Almeida, A.; Maas, C.; Frevert, J. IncobotulinumtoxinA: A Highly Purified and Precisely Manufactured Botulinum Neurotoxin Type A. J. Drugs Dermatol. 2019, 18, 52–57. [Google Scholar]
- Park, J.Y.; Sunga, O.; Wanitphakdeedecha, R.; Frevert, J. Neurotoxin Impurities: A Review of Threats to Efficacy. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2627. [Google Scholar] [CrossRef] [PubMed]
- Bryant, A.M.; Cai, S.; Singh, B.R. Comparative immunochemical characteristics of botulinum neurotoxin type A and its associated proteins. Toxicon Off. J. Int. Soc. Toxinol. 2013, 72, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samadzadeh, S.; Ürer, B.; Brauns, R.; Rosenthal, D.; Lee, J.-I.; Albrecht, P.; Hefter, H. Clinical Implications of Difference in Antigenicity of Different Botulinum Neurotoxin Type A Preparations: Clinical Take-Home Messages from Our Research Pool and Literature. Toxins 2020, 12, 499. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, J.H.; Hu, H.; Park, H.J.; Lee, H.J.; Choi, Y.J.; Kim, H.J. Botulinum neurotoxin injection in the deltoid muscle: Application to cosmetic shoulder contouring. Surg. Radiol. Anat. 2023, 45, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, H.J.; Choi, Y.J.; Lee, K.; Lee, J.H.; Kim, H.J. Anatomical guide for botulinum neurotoxin injection: Application to cosmetic shoulder contouring, pain syndromes, and cervical dystonia. Clin. Anat. 2021, 34, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.; Sayegh, F.; Sarosi, A.; Chopra, K.; Codner, M.; Sanati-Mehrizy, P.; Taub, P.J. Millennials Are Interested in Botulinum Toxin Injections for Prevention of Facial Rhytids. Face 2021, 2, 94–98. [Google Scholar] [CrossRef]
- Michon, A. Botulinum toxin for cosmetic treatments in young adults: An evidence-based review and survey on current practice among aesthetic practitioners. J. Cosmet. Dermatol. 2023, 22, 128–139. [Google Scholar] [CrossRef]
- Chung, K.; Orme, N.; Sherber, N. “Millennial Botulinum Toxin”: A Retrospective Age-Matched Cohort Study with Onabotulinumtoxin A. Dermatol. Surg. 2021, 47, 882–884. [Google Scholar] [CrossRef]
- Kazerooni, R. Decreased Therapeutic Effect over Time Amongst Botulinum Toxin Type A Agents (1837). Neurology 2021, 96, 1837. [Google Scholar]
- Kazerooni, R. Decrease in therapeutic effect among botulinum neurotoxin type A agents: Updated analysis of the FDA Adverse Event Reporting System database. J. Am. Acad. Dermatol. 2020, 83, AB200. [Google Scholar] [CrossRef]
- Dressler, D. Clinical presentation and management of antibody-induced failure of botulinum toxin therapy. Mov. Disord. 2004, 19, S92–S100. [Google Scholar] [CrossRef]
- Albrecht, P.; Jansen, A.; Lee, J.I.; Moll, M.; Ringelstein, M.; Rosenthal, D.; Bigalke, H.; Aktas, O.; Hartung, H.P.; Hefter, H. High prevalence of neutralizing antibodies after long-term botulinum neurotoxin therapy. Neurology 2019, 92, e48–e54. [Google Scholar] [CrossRef] [PubMed]
- Wissel, J.; Bensmail, D.; Ferreira, J.J.; Molteni, F.; Satkunam, L.; Moraleda, S.; Rekand, T.; McGuire, J.; Scheschonka, A.; Flatau-Baque, B.; et al. Safety and efficacy of incobotulinumtoxinA doses up to 800 U in limb spasticity: The TOWER study. Neurology 2017, 88, 1321–1328. [Google Scholar] [CrossRef] [Green Version]
- Corduff, N. Sensory Symptoms Associated with Aesthetic Botulinum Toxin A Treatments. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4631. [Google Scholar] [CrossRef] [PubMed]
- Shome, D.; Kapoor, R.; Khare, S. Two different types of botulinum toxins: Is there a difference in efficacy and longevity? J. Cosmet. Dermatol. 2019, 18, 1635–1641. [Google Scholar] [CrossRef] [PubMed]
- Kerscher, M.; Roll, S.; Becker, A.; Wigger-Alberti, W. Comparison of the spread of three botulinum toxin type A preparations. Arch. Dermatol. Res. 2012, 304, 155–161. [Google Scholar] [CrossRef]
- Samizadeh, S.; De Boulle, K. Botulinum neurotoxin formulations: Overcoming the confusion. Clin. Cosmet. Investig. Dermatol. 2018, 11, 273–287. [Google Scholar] [CrossRef] [Green Version]
- Bigalke, H.; Rummel, A. Botulinum Neurotoxins: Qualitative and Quantitative Analysis Using the Mouse Phrenic Nerve Hemidiaphragm Assay (MPN). Toxins 2015, 7, 4895–4905. [Google Scholar] [CrossRef] [Green Version]
- Wilder-Kofie, T.D.; Luquez, C.; Adler, M.; Dykes, J.K.; Coleman, J.D.; Maslanka, S.E. An alternative in vivo method to refine the mouse bioassay for botulinum toxin detection. Comp. Med. 2011, 61, 235–242. [Google Scholar]
- Nestor, M.S.; Ablon, G.R. The Frontalis Activity Measurement Standard: A novel contralateral method for assessing botulinum neurotoxin type-A activity. J. Drugs Dermatol. 2011, 10, 968–972. [Google Scholar] [PubMed]
- Dressler, D.; Gessler, F.; Tacik, P.; Bigalke, H. An enzyme-linked immunosorbent assay for detection of botulinum toxin-antibodies. Mov. Disord. 2014, 29, 1322–1324. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, W.W.S.; Chan, L.; Corduff, N.; Lau, W.-T.; Martin, M.U.; Tay, C.M.; Wang, S.; Wu, R. Addressing the Real-World Challenges of Immunoresistance to Botulinum Neurotoxin A in Aesthetic Practice: Insights and Recommendations from a Panel Discussion in Hong Kong. Toxins 2023, 15, 456. https://doi.org/10.3390/toxins15070456
Ho WWS, Chan L, Corduff N, Lau W-T, Martin MU, Tay CM, Wang S, Wu R. Addressing the Real-World Challenges of Immunoresistance to Botulinum Neurotoxin A in Aesthetic Practice: Insights and Recommendations from a Panel Discussion in Hong Kong. Toxins. 2023; 15(7):456. https://doi.org/10.3390/toxins15070456
Chicago/Turabian StyleHo, Wilson W. S., Lisa Chan, Niamh Corduff, Wang-Tak Lau, Michael U. Martin, Clifton Ming Tay, Sandy Wang, and Raymond Wu. 2023. "Addressing the Real-World Challenges of Immunoresistance to Botulinum Neurotoxin A in Aesthetic Practice: Insights and Recommendations from a Panel Discussion in Hong Kong" Toxins 15, no. 7: 456. https://doi.org/10.3390/toxins15070456
APA StyleHo, W. W. S., Chan, L., Corduff, N., Lau, W. -T., Martin, M. U., Tay, C. M., Wang, S., & Wu, R. (2023). Addressing the Real-World Challenges of Immunoresistance to Botulinum Neurotoxin A in Aesthetic Practice: Insights and Recommendations from a Panel Discussion in Hong Kong. Toxins, 15(7), 456. https://doi.org/10.3390/toxins15070456