5-Fluorouracil as a Tumor-Treating Field-Sensitizer in Colon Cancer Therapy

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Results
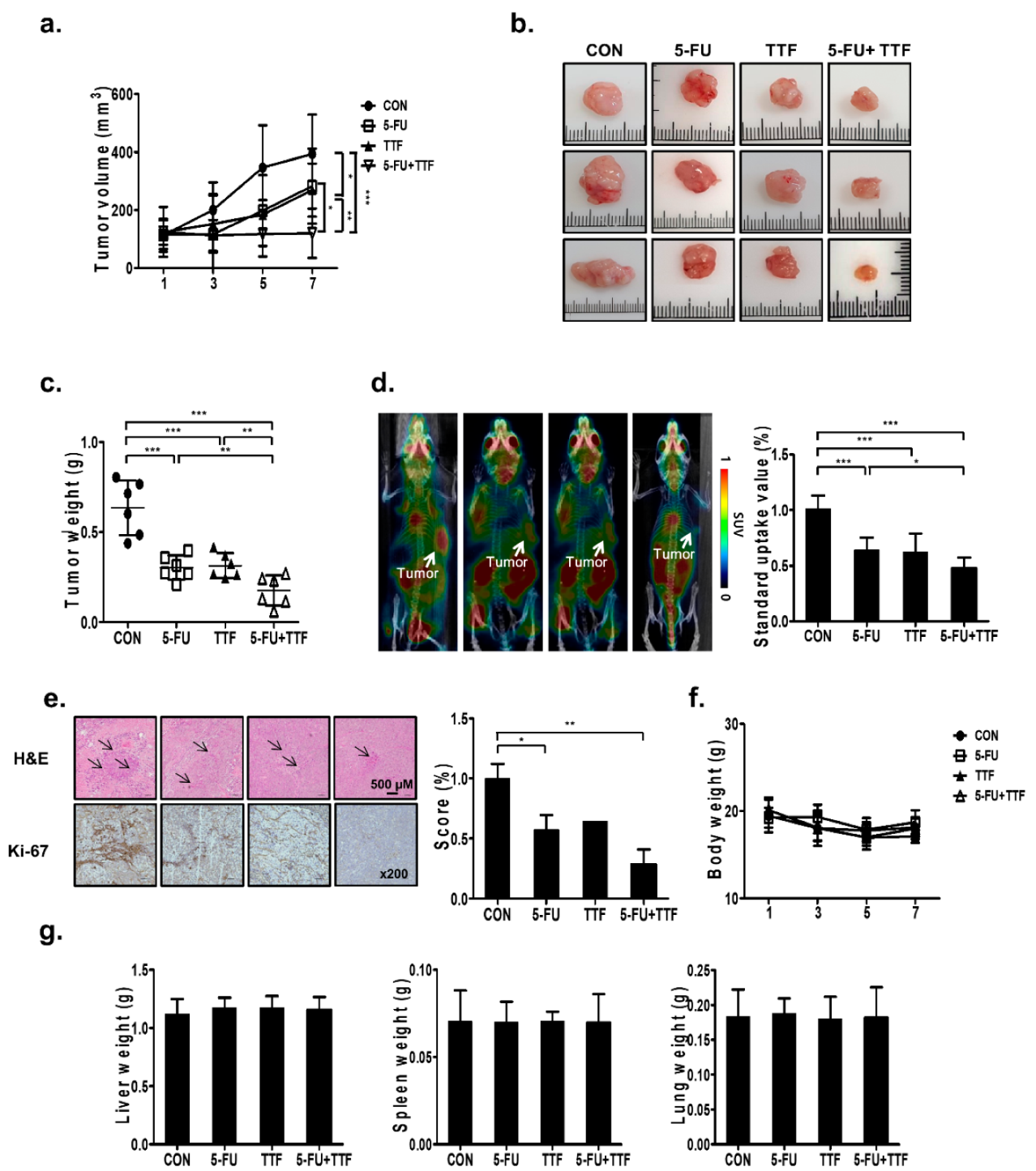
2.1. 5-FU Promoted TTFields-Sensitivity In Vivo
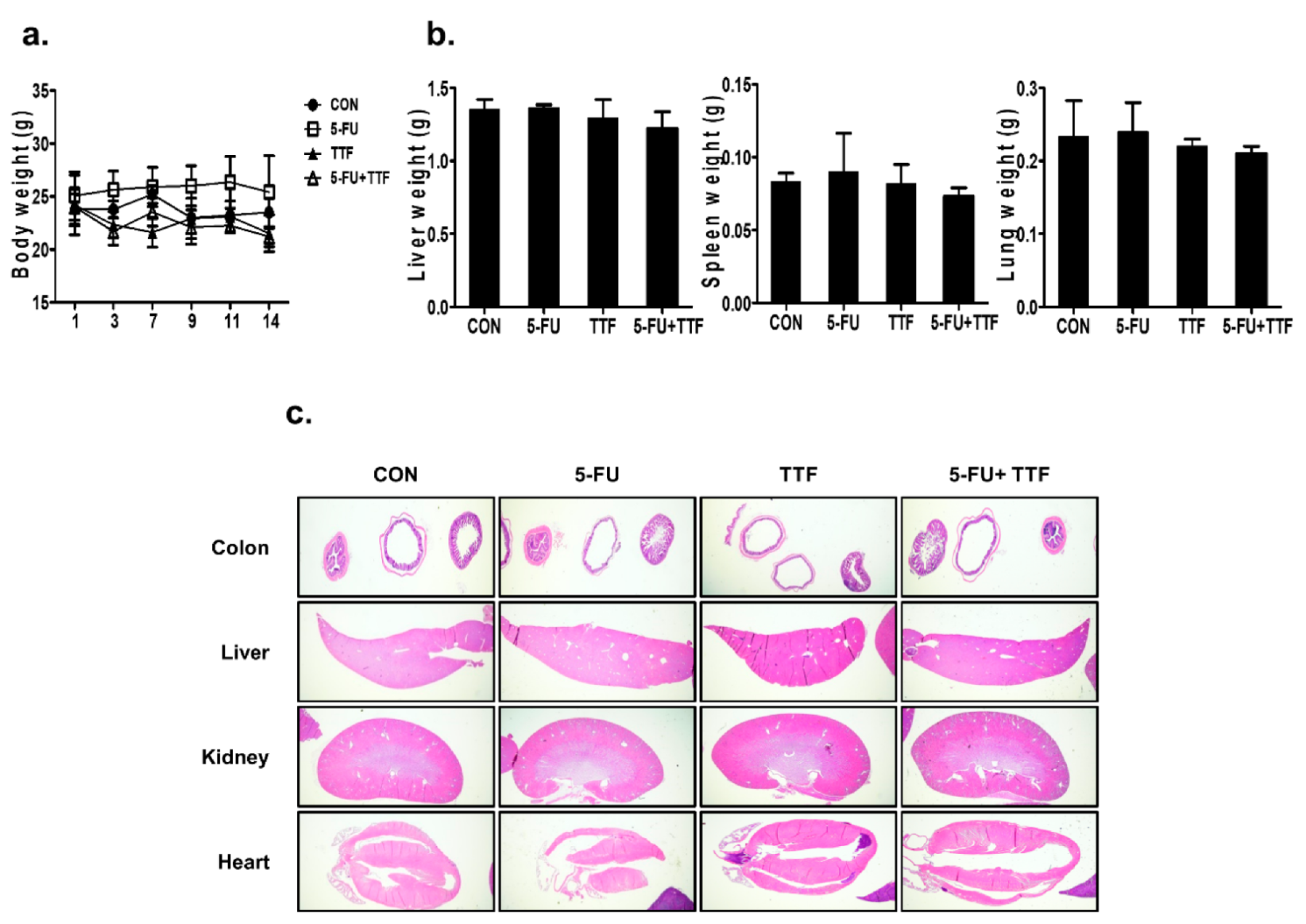
2.2. TTFields Treatment Does Not Result in Any Observable Pathologic Abnormalities in Normal Tissues
2.3. TTFields-Sensitizing Events of 5-FU on In Vitro Models of Colon Cancer
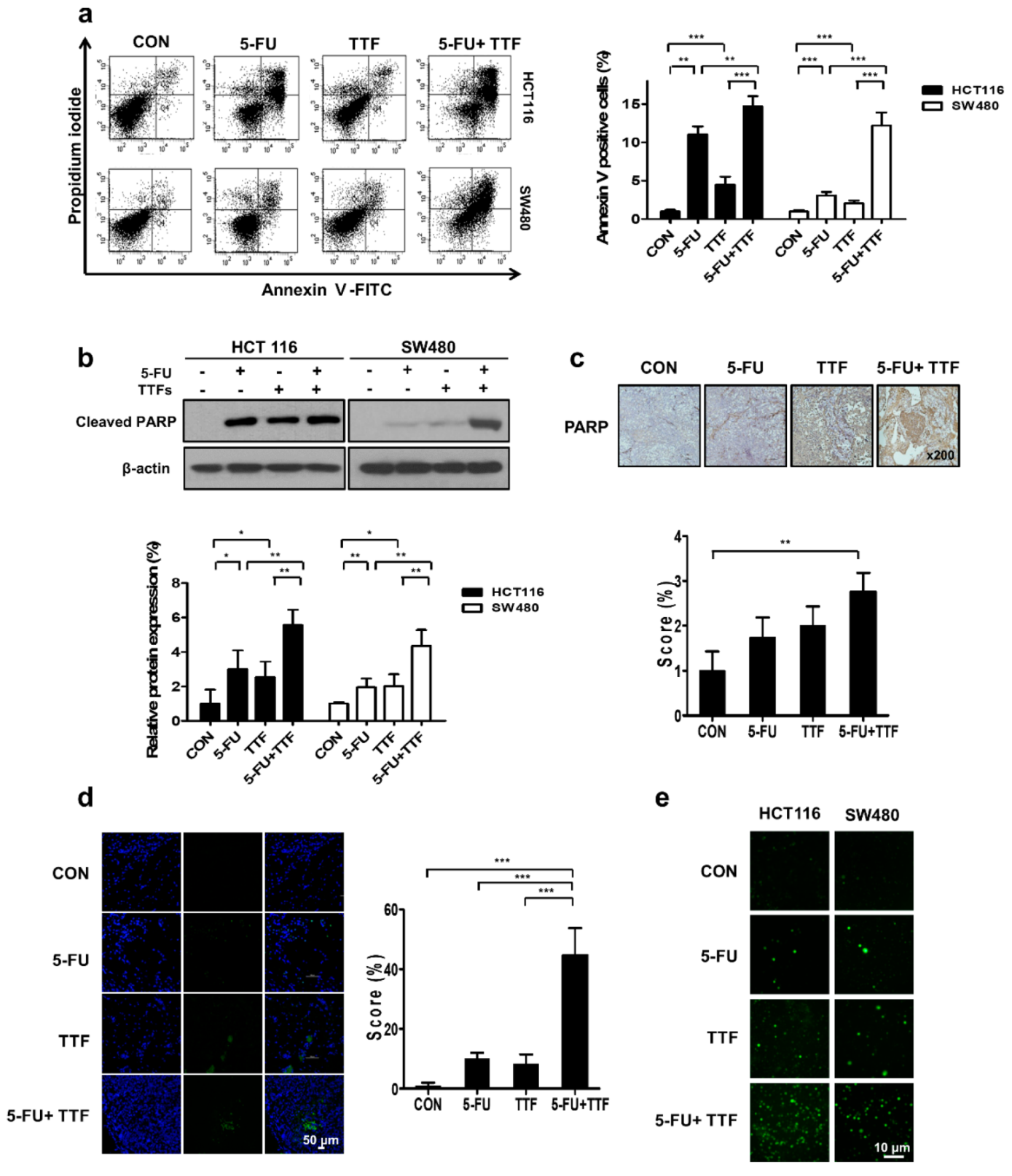
2.4. Effect of TTFields on 5-FU-Induced Apoptosis
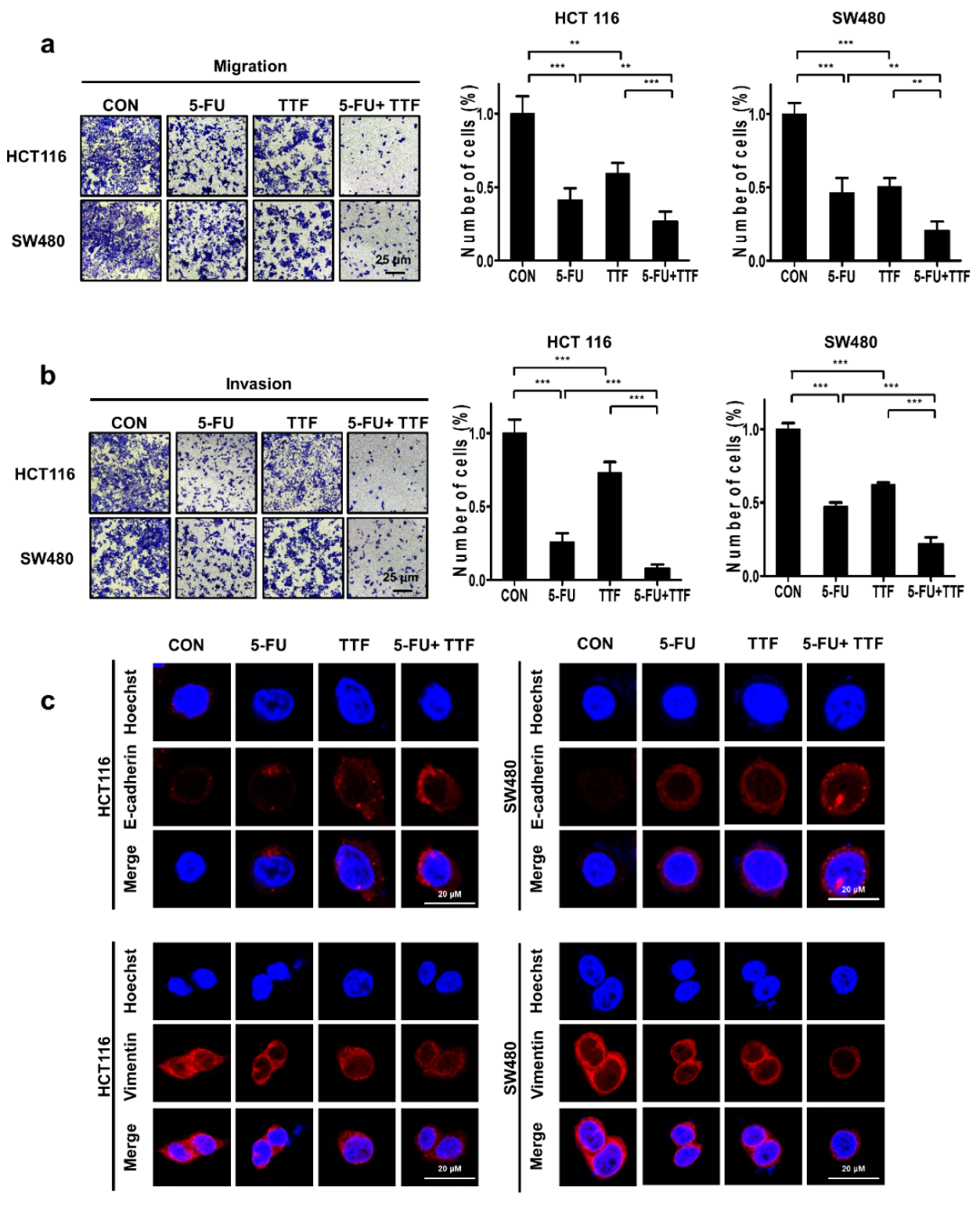
2.5. Combination Treatment Considerably Inhibited Tumor Cell Motility and Tumor Cell Invasion
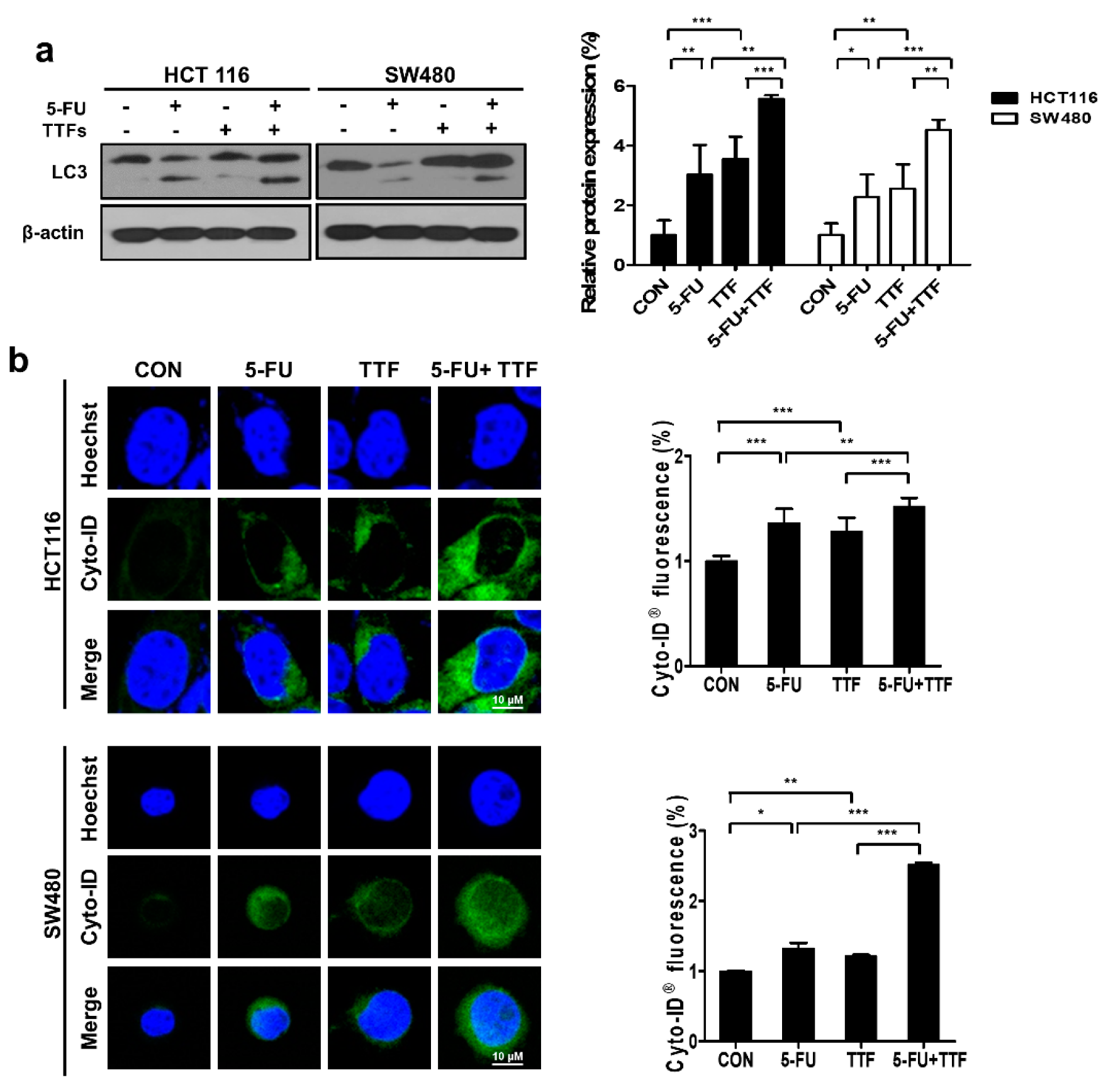
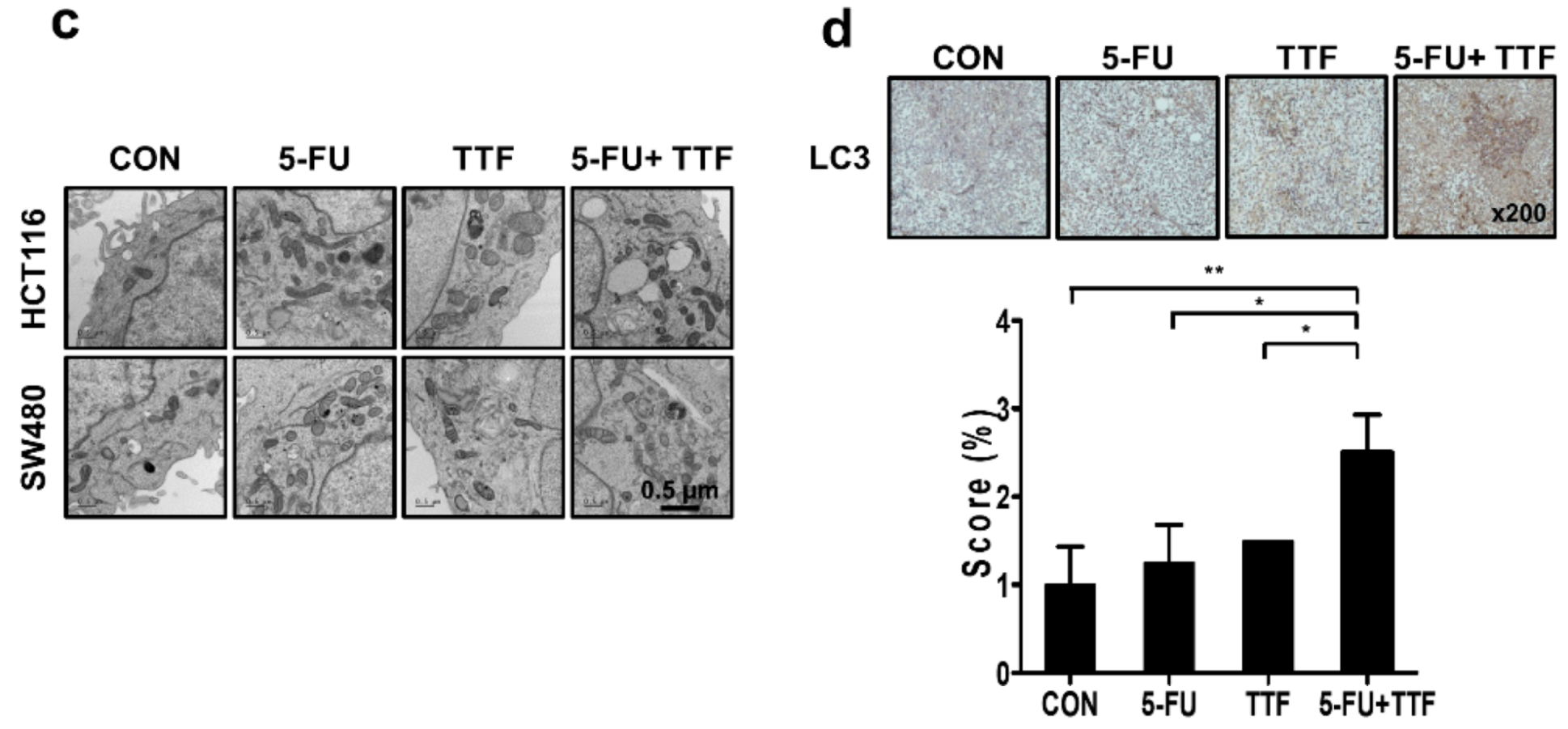
2.6. Effects of 5-FU and TTFields on Autophagic Cell Death
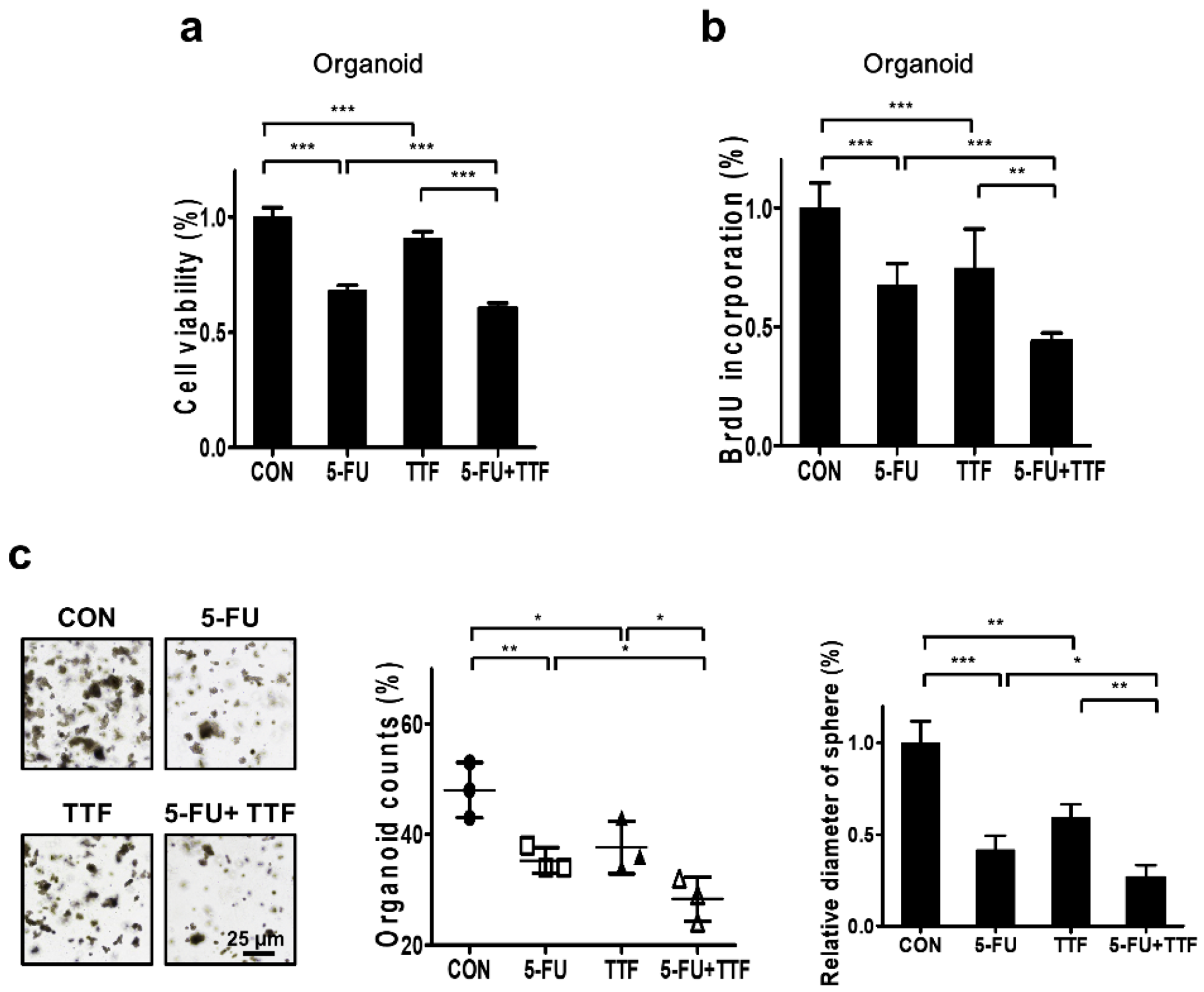
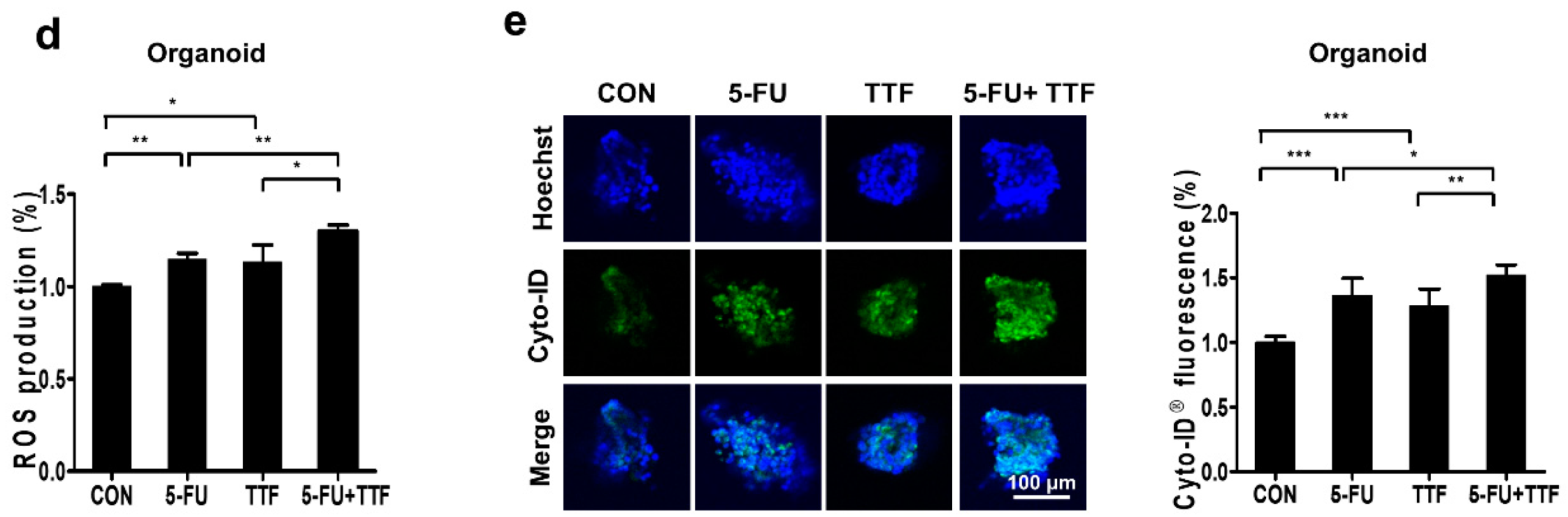
2.7. Combination of 5-FU and TTFs Augmented Cell Death in Colon Patient Organoid
3. Discussion
4. Materials and Methods
4.1. Experimental Setup for Electric Fields
4.2. Antibodies and Chemicals
4.3. Cell Culture
4.4. Cell Viability Assay
4.6. Colony-Forming Assay
4.7. Tumor Xenografts in Nude Mice
4.8. PET/CT Scans and Image Analysis
4.9. Detection of Apoptotic Cells via Annexin V Staining
4.10. Western Blotting
4.11. TUNEL Assays
4.12. Fluorescence-Based Quantification of Intracellular ROS
4.13. Cyto-ID® Analysis
4.14. Transmission Electron Microscopy
4.15. Immunohistochemistry
4.16. Invasion/Migration Assay
4.19. Statistical Analysis
4.20. Ethical Statement
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| 3D | Three dimensional |
| 5-FU | 5-Fluorouracil |
| CRC | Colorectal cancer |
| CT | Computed tomography |
| DCFH-DA | 2’,7’-Dichlorofluorescein diacetate |
| DMEM | Dulbecco’s modified Eagle’s medium |
| FBS | Fetal bovine serum |
| FDG | 18F-fluoro-2-deoxy-d-glucose |
| GBM | Glioblastoma multiforme |
| HEPES | 4-(2-Hydroxyethyl)-1-piperazineethanesulfonic acid |
| IR | Infrared radiation |
| MTT | 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| NSCLC | Non-small cell lung carcinoma |
| PBS | Phosphate buffered saline |
| PE | Plating efficiency |
| PET | Positron emission tomography |
| PI | Propidium iodide |
| ROI | Region of interest |
| ROS | Reactive oxygen species |
| SD | Standard deviation |
| SUV | Standard uptake value |
| TTFields | Tumor-treating fields |
| TUNEL | Terminal deoxynucleotidyl transferase-mediated dUTP nick-end labeling |
| RT | Radiotherapy |
| SF | Surviving fraction |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Saltz, L.B.; Minsky, B. Adjuvant therapy of cancers of the colon and rectum. Surg. Clin. N. Am. 2002, 82, 1035–1058. [Google Scholar] [CrossRef]
- Krook, J.E.; Moertel, C.G.; Gunderson, L.L.; Wieand, H.S.; Collins, R.T.; Beart, R.W.; Kubista, T.P.; Poon, M.A.; Meyers, W.C.; Mailliard, J.A.; et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N. Engl. J. Med. 1991, 324, 709–715. [Google Scholar] [CrossRef]
- Seiwert, T.Y.; Salama, J.K.; Vokes, E.E. The concurrent chemoradiation paradigm—General principles. Nat. Clin. Pract. Oncol. 2007, 4, 86–100. [Google Scholar] [CrossRef]
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330–338. [Google Scholar] [CrossRef]
- Zhang, N.; Yin, Y.; Xu, S.J.; Chen, W.S. 5-Fluorouracil: Mechanisms of resistance and reversal strategies. Molecules 2008, 13, 1551–1569. [Google Scholar] [CrossRef] [Green Version]
- Mun, E.J.; Babiker, H.M.; Weinberg, U.; Kirson, E.D.; Von Hoff, D.D. Tumor-treating fields: A fourth modality in cancer treatment. Clin. Cancer Res. 2018, 24, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Wong, E.T.; Kanner, A.A.; Steinberg, D.; Engelhard, H.; Heidecke, V.; Kirson, E.D.; Taillibert, S.; Liebermann, F.; Dbalý, V.; et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. Eur. J. Cancer 2012, 48, 2192–2202. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Taillibert, S.; Kanner, A.A.; Kesari, S.; Steinberg, D.M.; Toms, S.A.; Taylor, L.P.; Lieberman, F.; Silvani, A.; Fink, K.L.; et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: A randomized clinical trial. JAMA. 2015, 314, 2535–2543. [Google Scholar] [CrossRef]
- Davies, A.M.; Weinberg, U.; Palti, Y. Tumor treating fields: A new frontier in cancer therapy. Ann. N. Y. Acad. Sci. 2013, 1291, 86–95. [Google Scholar] [CrossRef] [PubMed]
- NCCN. Clinical Practice Guidelines in Oncology (NCCN Guidelines) for Central Nervous System Cancers; NCCN: Plymouth Meeting, PA, USA, 2016. [Google Scholar]
- NOVOCURE. Available online: https://www.novocure.com/our-pipeline/ (accessed on 3 May 2018).
- Jo, Y.; Kim, E.H.; Sai, S.; Kim, J.S.; Cho, J.M.; Kim, H.; Baek, J.H.; Kim, J.Y.; Hwang, S.G.; Yoon, M. Functional biological activity of sorafenib as a tumor-treating field sensitizer for glioblastoma therapy. Int. J. Mol. Sci. 2018, 19, 3684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valeriote, F.; Lin, H. Synergistic interaction of anticancer agents: A cellular perspective. Cancer Chemother. Rep. 1975, 59, 895–900. [Google Scholar] [PubMed]
- Carpentier, Y.; Demange, L.; Loirette, M.; Hivet, J.; Desoize, B. Chronology of combined chemotherapy (5FU) and radiotherapy. I. In vitro study. Anticancer Res. 1993, 13, 2177–2180. [Google Scholar] [PubMed]
- Giladi, M.; Munster, M.; Schneiderman, R.S.; Voloshin, T.; Porat, Y.; Blat, R.; Zielinska-Chomej, K.; Haag, P.; Bomzon, Z.; Kirson, E.D.; et al. Tumor treating fields (TTFields) delay DNA damage repair following radiation treatment of glioma cells. Radiat. Oncol. 2017, 12, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Craene, B.; Berx, G. Regulatory networks defining EMT during cancer initiation and progression. Nat. Rev. Cancer 2013, 13, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Bracht, K.; Nicholls, A.M.; Liu, Y.; Bodmer, W.F. 5-Fluorouracil response in a large panel of colorectal cancer cell lines is associated with mismatch repair deficiency. Br. J. Cancer 2010, 103, 340–346. [Google Scholar] [CrossRef] [Green Version]
- Mhaidat, N.M.; Bouklihacene, M.; Thorne, R.F. 5-Fluorouracil-induced apoptosis in colorectal cancer cells is caspase-9-dependent and mediated by activation of protein kinase C-delta. Oncol. Lett. 2014, 8, 699–704. [Google Scholar] [CrossRef]
- Yang, S.Y.; Bolvin, C.; Sales, K.M.; Fuller, B.; Seifalian, A.M.; Winslet, M.C. IGF-I activates caspases 3/7, 8 and 9 but does not induce cell death in colorectal cancer cells. BMC Cancer 2009, 9, 158. [Google Scholar] [CrossRef] [Green Version]
- Uchiyama, K.; Iwabuchi, H.; Nakayama, S. [Phase I/II clinical trial of induction chemotherapy with nedaplatin (CDGP), docetaxel (DOC) and 5-fluorouracil (5-FU) for squamous cell carcinoma of head and neck]. Gan Kagaku Ryoho 2007, 34, 43–48. [Google Scholar]
- Malet-Martino, M.; Martino, R. Clinical studies of three oral prodrugs of 5-fluorouracil (capecitabine, UFT, S-1): A review. Oncologist 2002, 7, 288–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneiderman, R.S.; Giladi, M.; Zeevi, E.; Voloshin, T.; Shteingauz, A.; Porat, Y.; Munster, M.; Kirson, E.; Weinberg, U.; Palti, Y. Angi-11. Tumor treating fields (ttfields) inhibit cancer cell migration and invasion by inducing reorganization of the actin cytoskeleton and formation of cell adhesions. Neuro Oncol. 2018, 20 (Suppl. 6), vi30. [Google Scholar] [CrossRef]
- Giladi, M.; Schneiderman, R.S.; Porat, Y.; Munster, M.; Itzhaki, A.; Mordechovich, D.; Cahal, S.; Kirson, E.D.; Weinberg, U.; Palti, Y. Mitotic disruption and reduced clonogenicity of pancreatic cancer cells in vitro and in vivo by tumor treating fields. Pancreatology 2014, 14, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Voloshin, T.; Munster, M.; Blatt, R.; Shteingauz, A.; Roberts, P.C.; Schmelz, E.M.; Giladi, M.; Schneiderman, R.S.; Zeevi, E.; Porat, Y.; et al. Alternating electric fields (TTFields) in combination with paclitaxel are therapeutically effective against ovarian cancer cells in vitro and in vivo. Int. J. Cancer 2016, 139, 2850–2858. [Google Scholar] [CrossRef]
- Pless, M.; Droege, C.; von Moos, R.; Salzberg, M.; Betticher, D. A phase I/II trial of Tumor Treating Fields (TTFields) therapy in combination with pemetrexed for advanced non-small cell lung cancer. Lung Cancer 2013, 81, 445–450. [Google Scholar] [CrossRef]
- Ceresoli, G.L.; Aerts, J.G.; Dziadziuszko, R.; Ramlau, R.; Cedres, S.; van Meerbeeck, J.P.; Mencoboni, M.; Planchard, D.; Chella, A.; Crino, L.; et al. Tumour Treating Fields in combination with pemetrexed and cisplatin or carboplatin as first-line treatment for unresectable malignant pleural mesothelioma (STELLAR): A multicentre, single-arm phase 2 trial. Lancet Oncol. 2019, 20, 1702–1709. [Google Scholar] [CrossRef]
- Kim, E.H.; Song, H.S.; Yoo, S.H.; Yoon, M. Tumor treating fields inhibit glioblastoma cell migration, invasion and angiogenesis. Oncotarget 2016, 7, 65125–65136. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.H.; Jo, Y.; Sai, S.; Park, M.J.; Kim, J.Y.; Kim, J.S.; Lee, Y.J.; Cho, J.M.; Kwak, S.Y.; Baek, J.H.; et al. Tumor-treating fields induce autophagy by blocking the Akt2/miR29b axis in glioblastoma cells. Oncogene 2019, 38, 6630–6646. [Google Scholar] [CrossRef]
- Giladi, M.; Voloshin, T.; Shteingauz, A.; Munster, M.; Blat, R.; Porat, Y.; Schneiderman, R.S.; Cahal, S.; Itzhaki, A.; Kirson, E. Alternating electric fields (TTFields) induce immunogenic cell death resulting in enhanced antitumor efficacy when combined with anti-PD-1 therapy. Am. Assoc. Immnol. 2016, 196, 75.26. [Google Scholar]
- Park, J.I.; Song, K.H.; Jung, S.Y.; Ahn, J.; Hwang, S.G.; Kim, J.; Kim, E.H.; Song, J.Y. Tumor-treating fields induce RAW264.7 macrophage activation via NK-kappaB/MAPK signaling pathways. Technol. Cancer Res. Treat. 2019, 18. [Google Scholar] [CrossRef] [Green Version]
- Kirson, E.D.; Dbalý, V.; Tovaryš, F.; Vymazal, J.; Soustiel, J.F.; Itzhaki, A.; Mordechovich, D.; Steinberg-Shapira, S.; Gurvich, Z.; Schneiderman, R.; et al. Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors. Proc. Natl. Acad. Sci. USA 2007, 104, 10152–10157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirson, E.D.; Schneiderman, R.S.; Dbalý, V.; Tovaryš, F.; Vymazal, J.; Itzhaki, A.; Mordechovich, D.; Gurvich, Z.; Shmueli, E.; Goldsher, D.; et al. Chemotherapeutic treatment efficacy and sensitivity are increased by adjuvant alternating electric fields (TTFields). BMC Med Phys. 2009, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodwin, R.A.; Asmis, T.R. Overview of systemic therapy for colorectal cancer. Clin. Colon Rectal Surg. 2009, 22, 251–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, H.; Sung, J.; Oh, S.-i.; Jeong, S.; Koh, E.K.; Hong, S.; Yoon, M. Inhibition of brain tumor cell proliferation by alternating electric fields. Appl. Phys. Lett. 2014, 105, 203703. [Google Scholar] [CrossRef]
- Guo, S.; Liang, Y.; Murphy, S.F.; Huang, A.; Shen, H.; Kelly, D.F.; Sobrado, P.; Sheng, Z. A rapid and high content assay that measures cyto-ID-stained autophagic compartments and estimates autophagy flux with potential clinical applications. Autophagy 2015, 11, 560–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Type | TTFields (V/cm) | SFTTF + 5-FU | SFTTF × SF5-FU | TTF Effect |
|---|---|---|---|---|
| HCT116 | 0.9 | 0.950 | 0.953 | Synergism |
| 1.2 | 0.811 | 0.926 | Synergism | |
| 1.5 | 0.653 | 0.824 | Synergism | |
| SW480 | 0.9 | 0.201 | 0.421 | Synergism |
| 1.2 | 0.089 | 0.141 | Synergism | |
| 1.5 | 0.084 | 0.113 | Synergism |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-J.; Cho, J.-M.; Sai, S.; Oh, J.Y.; Park, J.-A.; Oh, S.J.; Park, M.; Kwon, J.; Shin, U.S.; Baek, J.-H.; et al. 5-Fluorouracil as a Tumor-Treating Field-Sensitizer in Colon Cancer Therapy. Cancers 2019, 11, 1999. https://doi.org/10.3390/cancers11121999
Lee Y-J, Cho J-M, Sai S, Oh JY, Park J-A, Oh SJ, Park M, Kwon J, Shin US, Baek J-H, et al. 5-Fluorouracil as a Tumor-Treating Field-Sensitizer in Colon Cancer Therapy. Cancers. 2019; 11(12):1999. https://doi.org/10.3390/cancers11121999
Chicago/Turabian StyleLee, Yeon-Joo, Jae-Min Cho, Sei Sai, Ju Yeon Oh, Ji-Ae Park, Se Jong Oh, Misun Park, Junhye Kwon, Ui Sup Shin, Jeong-Hwa Baek, and et al. 2019. "5-Fluorouracil as a Tumor-Treating Field-Sensitizer in Colon Cancer Therapy" Cancers 11, no. 12: 1999. https://doi.org/10.3390/cancers11121999
APA StyleLee, Y. -J., Cho, J. -M., Sai, S., Oh, J. Y., Park, J. -A., Oh, S. J., Park, M., Kwon, J., Shin, U. S., Baek, J. -H., Lim, S. H., Song, J. -Y., Hwang, S. -G., & Kim, E. H. (2019). 5-Fluorouracil as a Tumor-Treating Field-Sensitizer in Colon Cancer Therapy. Cancers, 11(12), 1999. https://doi.org/10.3390/cancers11121999