
Clinical and Molecular Features of Epidermal Growth Factor Receptor (EGFR) Mutation Positive Non-Small-Cell Lung Cancer (NSCLC) Patients Treated with Tyrosine Kinase Inhibitors (TKIs): Predictive and Prognostic Role of Co-Mutations


 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Demographics and Outcome Measurements
- Patient characteristics: age, sex, smoking habit
- Disease characteristics: date of first diagnosis, method and site of diagnosis, histology, staging (TNM VIII edition), date of diagnosis of metastatic disease, number and sites of metastases;
- Molecular characteristics: EGFR mutation type (exon 19 deletion, exon 21 L858R mutation, non-T790M exon 20 mutations, exon 20 T790M mutation, others), diagnostic technique, PD-L1 expression level, presence/absence of co-mutations;
- Clinical course: starting date of first-line treatment, PS, best response, suspension of therapy and motivation, progression of the disease with relative sites, local treatments (radiotherapy, surgery or other), site and result of biopsy at the time of progression (liquid and /or tissue). Similar data were collected for second and third lines of therapy;
- Survival outcome: date of the last follow-up, status of patients (dead or alive).
2.2. NGS Sequencing
2.3. Immunohistochemical Scoring for PD-L1
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Patients’ and Tumour Characteristics
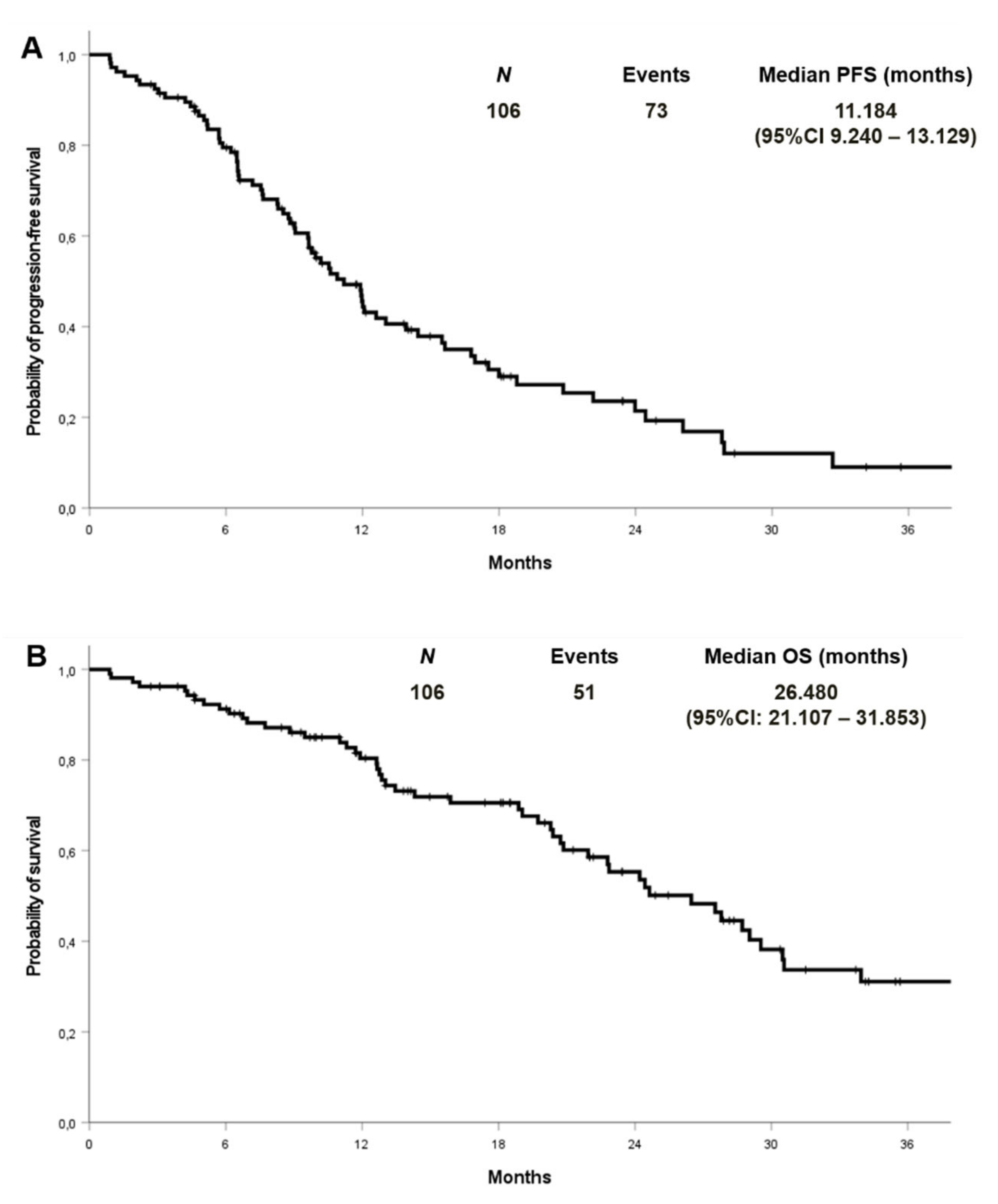
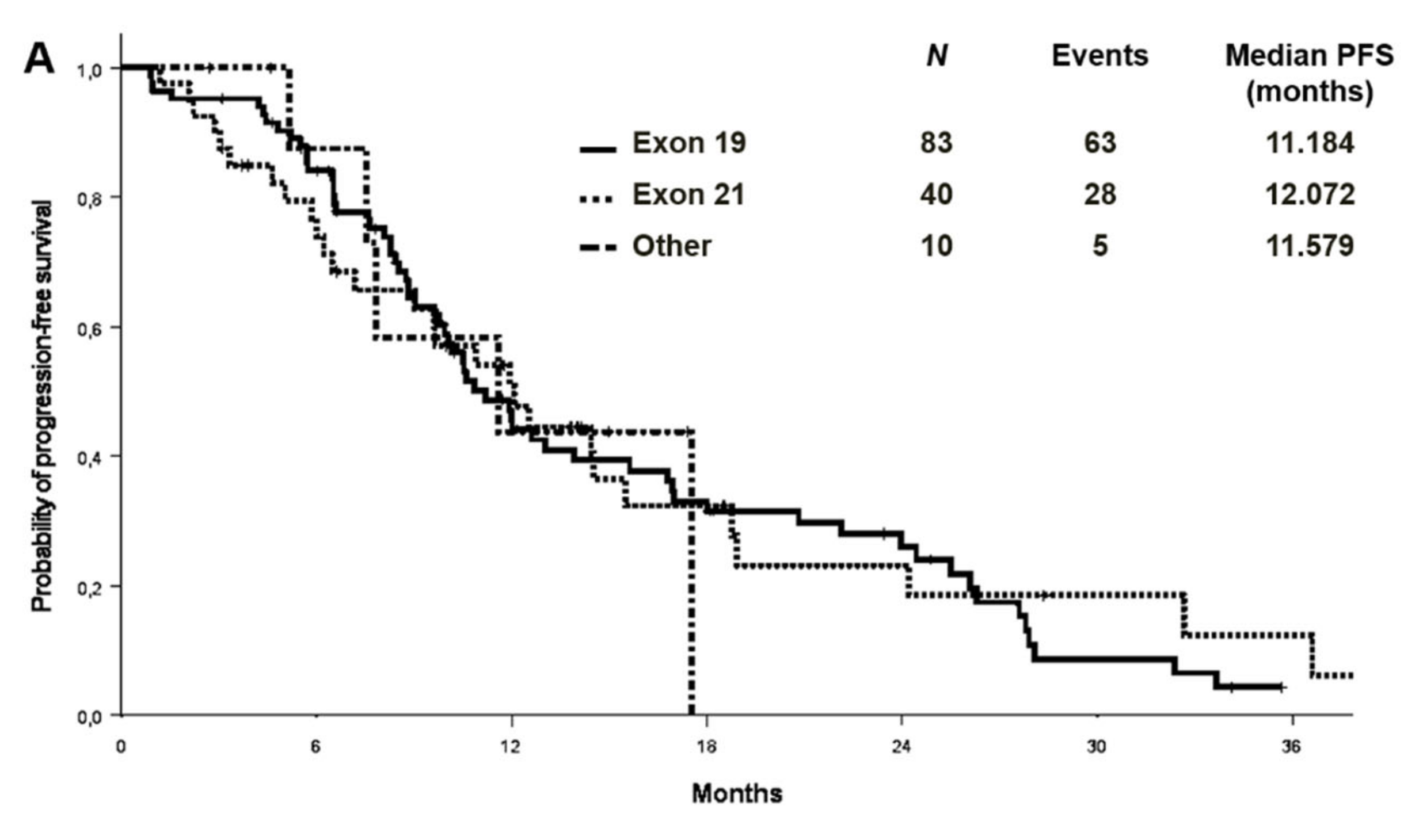
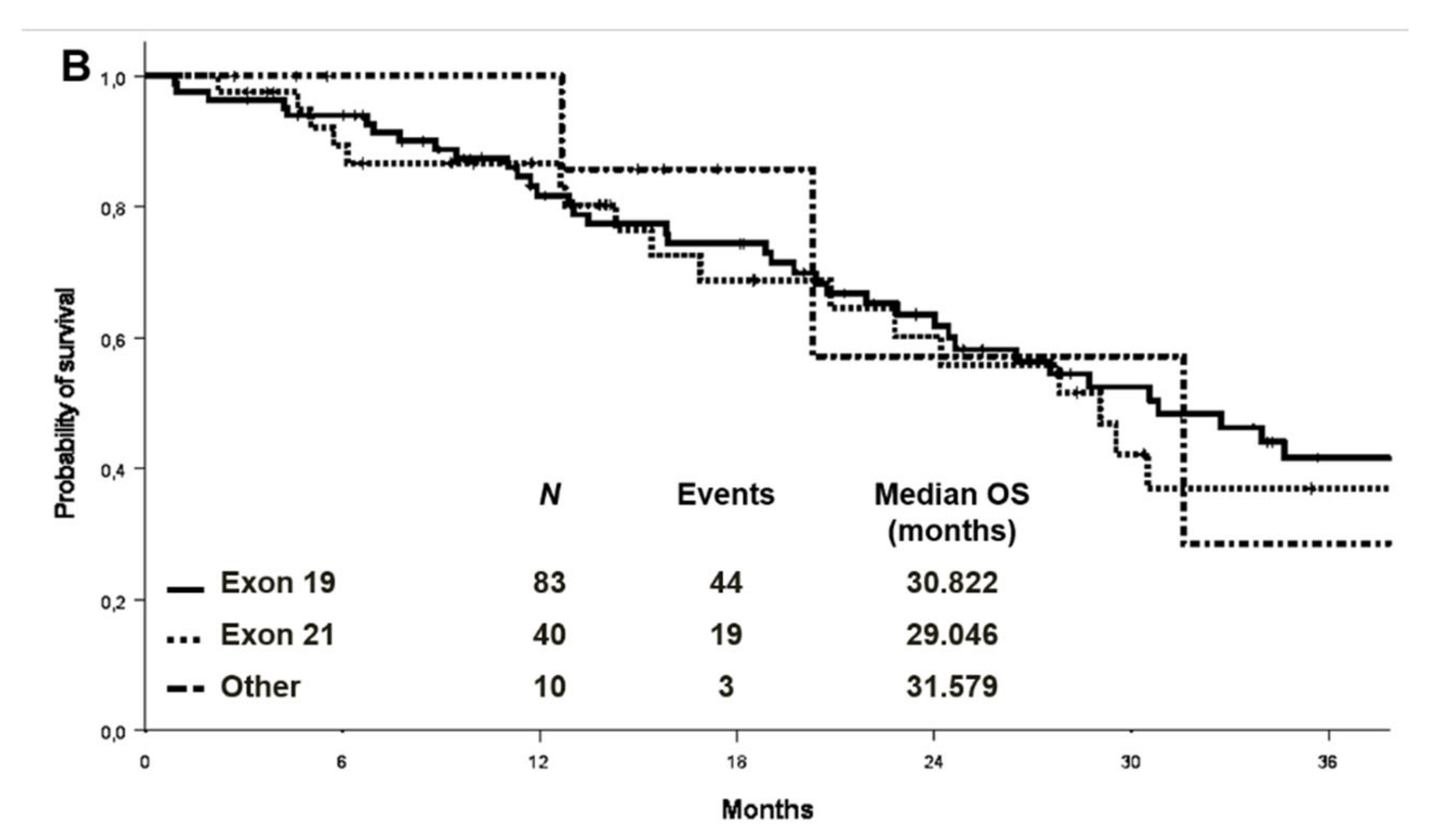
3.2. Treatment Outcomes in the Considered Cohort
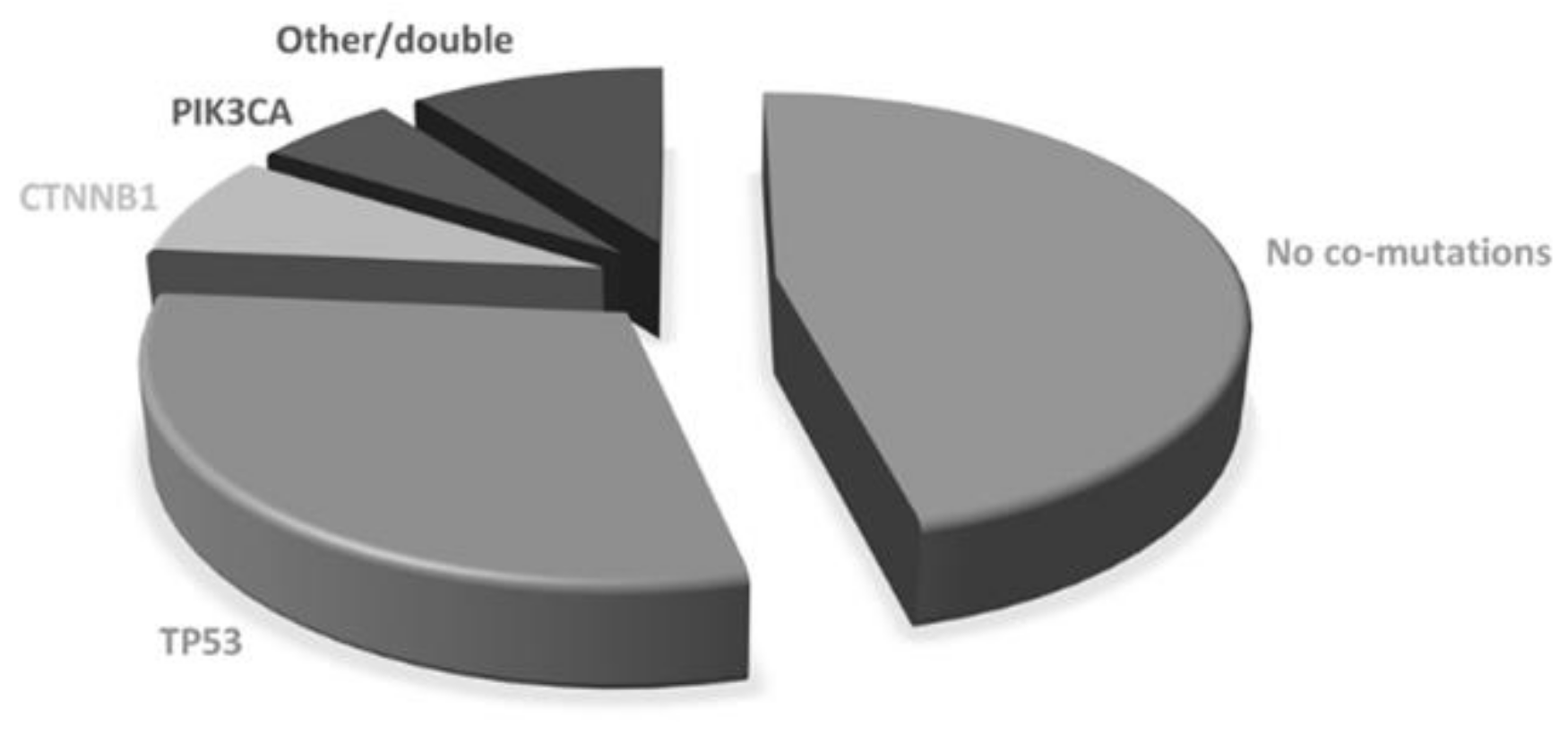
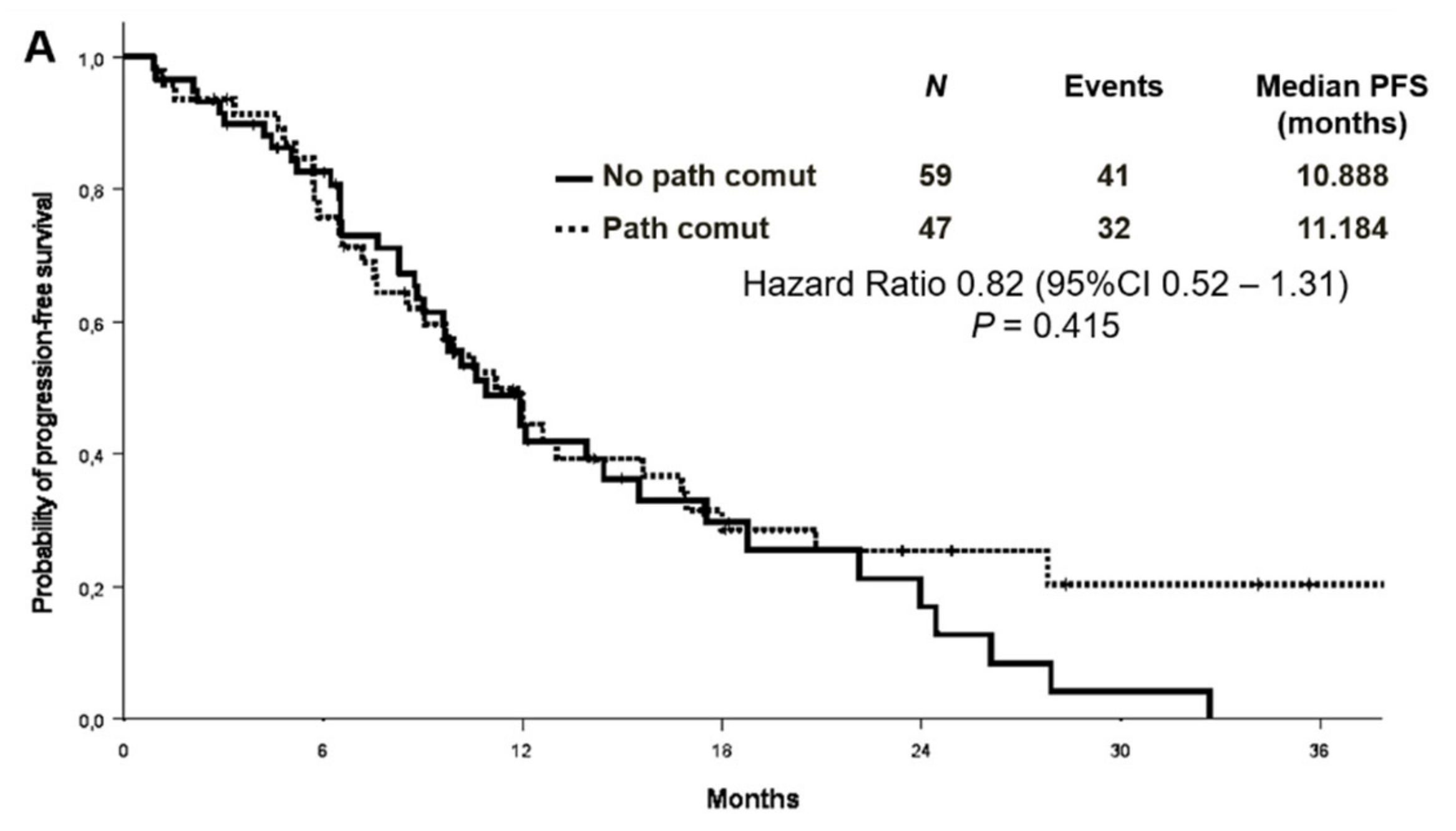
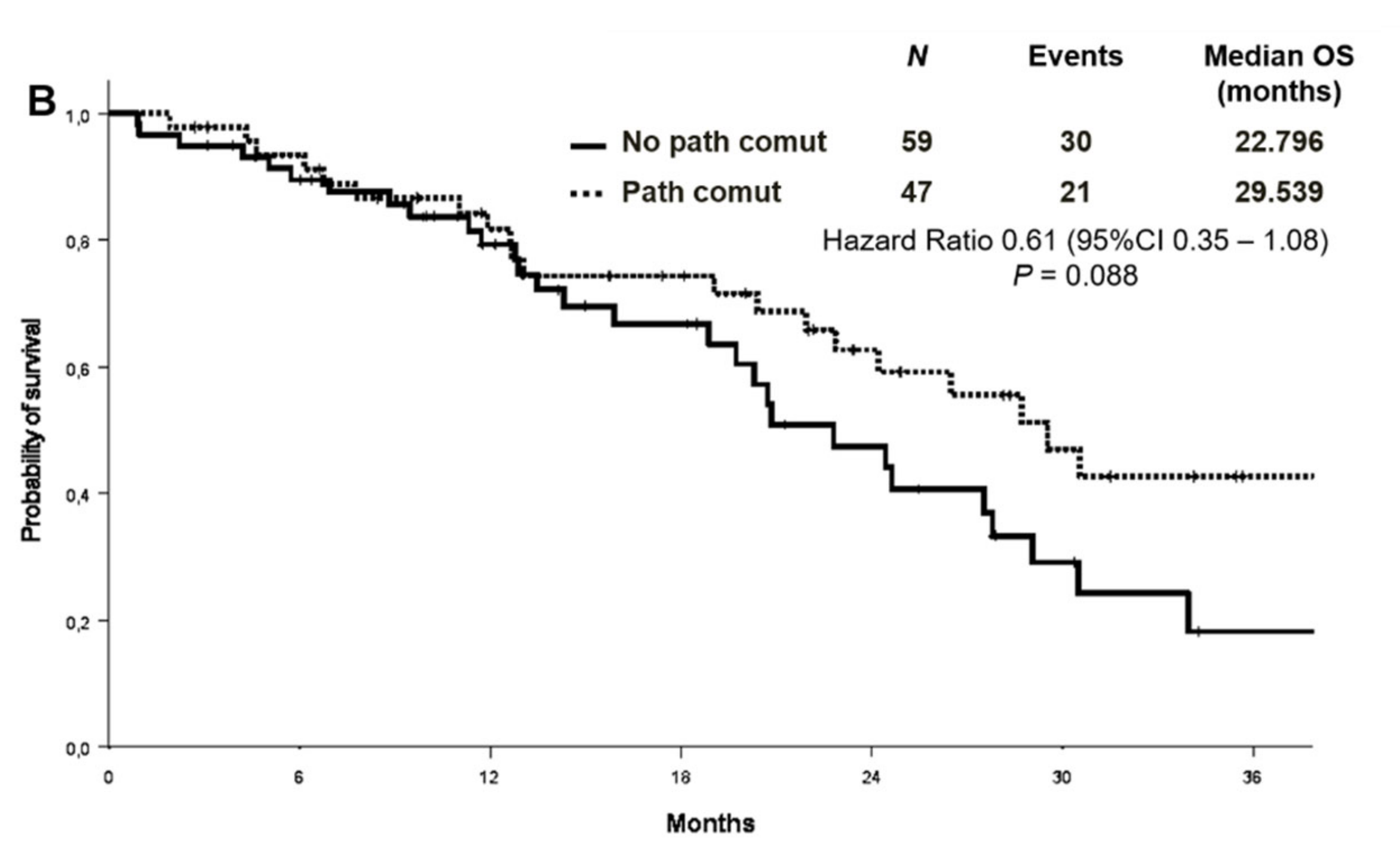
3.3. Association between Concomitant Alterations and Treatment Outcomes
3.4. Association between Concomitant Alterations and Second-Line Treatment Outcomes
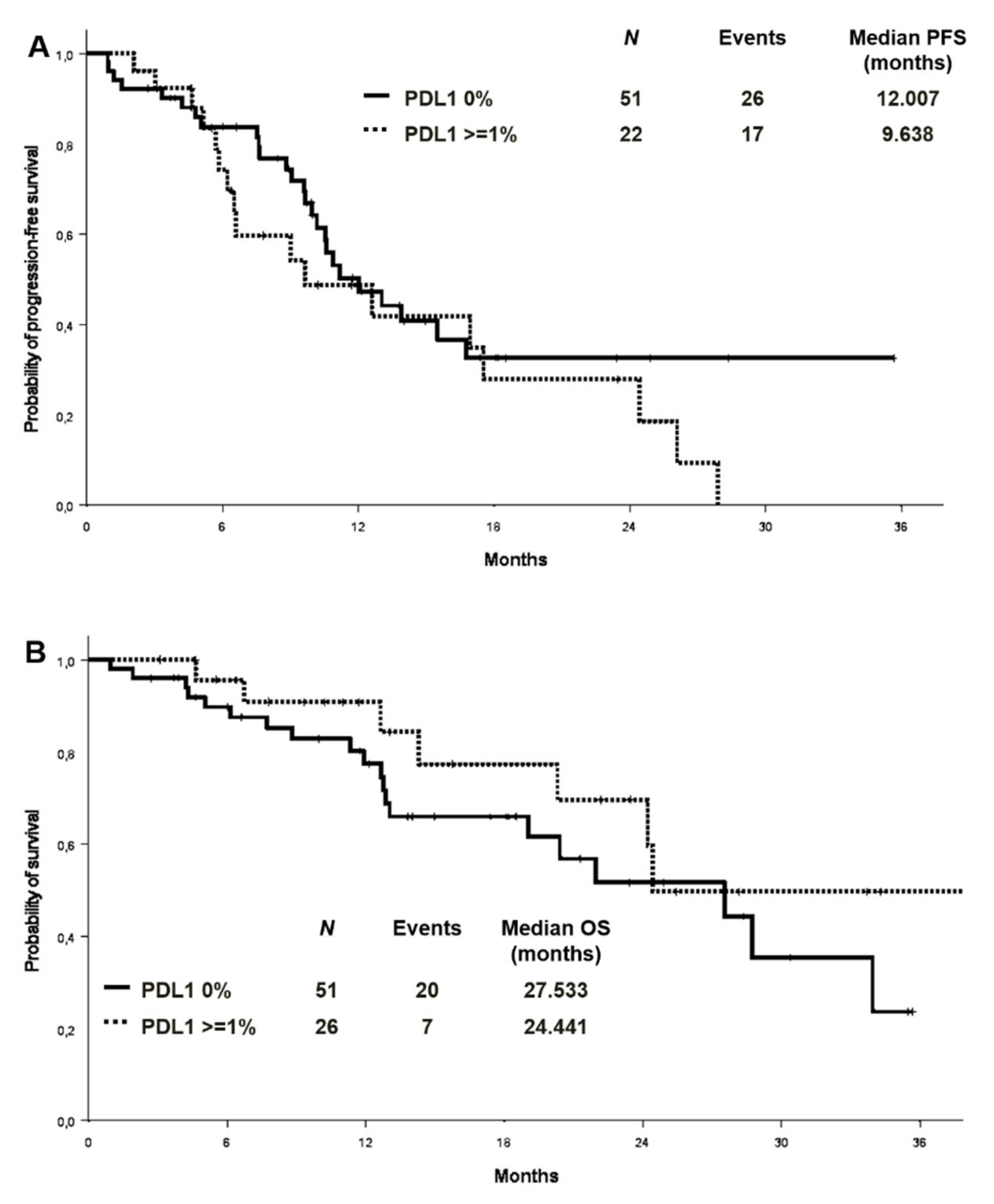
3.5. PD-L1 Expression and Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Word Health Organization. International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=900&key=asr&sex=0&cancer=39&type=1&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=1&include_nmsc=1&include_nmsc_other=1 (accessed on 24 January 2021).
- Greenhalgh, J.; Boland, A.; Bates, V.; Vecchio, F.; Dundar, Y.; Chaplin, M.; Green, J.A. First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-small cell lung cancer. Cochrane Database Syst Rev. 2021, 3, CD010383. [Google Scholar] [CrossRef]
- Barnet, M.B.; O’Toole, S.; Horvath, L.G.; Selinger, C.; Yu, B.; Ng, C.C.; Boyer, M.; Cooper, W.A.; Kao, S. EGFR-co-mutated advanced NSCLC and response to EGFR tyrosine kinase inhibi-tors. J. Thorac. Oncol. 2017, 12, 585–590. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.; Liu, Y.; Chen, J. Concurrent gene alterations with EGFR mutation and treatment efficacy of EGFR-TKIs in Chinese pa-tients with non-small cell lung cancer. Oncotarget 2017, 8, 25046–25054. [Google Scholar] [CrossRef] [Green Version]
- Labbé, C.; Cabanero, M.; Korpanty, G.J.; Tomasini, P.; Doherty, M.K.; Mascaux, C.; Jao, K.; Pitcher, B.; Wang, R.; Pintilie, M.; et al. Prognostic and predictive effects of TP53 co-mutation in patients with EGFR -mutated non-small cell lung cancer (NSCLC). Lung Cancer 2017, 111, 23–29. [Google Scholar] [CrossRef] [PubMed]
- VanderLaan, P.A.; Rangachari, D.; Mockus, S.M.; Spotlow, V.; Reddi, H.V.; Malcolm, J.; Huberman, M.S.; Joseph, L.J.; Kobayashi, S.S.; Costa, D.B. Mutations in TP53, PIK3CA, PTEN and other genes in EGFR mutated lung cancers: Correlation with clinical outcomes. Lung Cancer 2017, 106, 17–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.; Gao, F.; Fu, S.; Wang, Y.; Fang, W.; Huang, Y.; Zhang, L. Concomitant genetic alterations with response to treatment and epidermal growth factor recep-tor tyrosine kinase inhibitors in patients with EGFR-mutant advanced non-small cell lung cancer. JAMA Oncol. 2018, 4, 739–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakobsen, J.N.; Santoni-Rugiu, E.; Grauslund, M.; Melchior, L.; Sørensen, J.B. Concomitant driver mutations in advanced EGFR-mutated non-small-cell lung cancer and their impact on erlotinib treatment. Oncotarget 2018, 9, 26195–26208. [Google Scholar] [CrossRef] [Green Version]
- Helena, A.Y.; Suzawa, K.; Jordan, E.J.; Zehir, A.; Ni, A.; Kim, H.R.; Kris, M.G.; Hellmann, M.D.; Li, B.T.; Somwar, R.; et al. Concurrent Alterations in EGFR-Mutant Lung Cancers Associated with Resistance to EGFR Kinase Inhibitors and Characterization of MTOR as a Mediator of Resistance. Clin. Cancer Res. 2018, 24, 3108–3118. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Lee, B.; Shim, J.H.; Lee, S.H.; Park, W.Y.; Choi, Y.L.; Sun, J.M.; Ahn, J.S.; Ahn, M.J.; Park, K. Concurrent genetic alterations predict the progression to target therapy in EGFR-mutated ad-vanced NSCLC. J Thorac. Oncol. 2019, 14, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.-C.; Lai, Y.-C.; Chang, C.-Y.; Huang, L.-K.; Chen, S.-J.; Tan, K.T.; Yu, P.-N.; Lai, J.-I. Concomitant Genetic Alterations are Associated with Worse Clinical Outcome in EGFR Mutant NSCLC Patients Treated with Tyrosine Kinase Inhibitors. Transl. Oncol. 2019, 12, 1425–1431. [Google Scholar] [CrossRef]
- Chen, M.; Xu, Y.; Zhao, J.; Zhong, W.; Zhang, L.; Bi, Y.; Wang, M. Concurrent Driver Gene Mutations as Negative Predictive Factors in Epidermal Growth Factor Receptor-Positive Non-Small Cell Lung Cancer. EBioMedicine 2019, 42, 304–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rachiglio, A.M.; Fenizia, F.; Piccirillo, M.C.; Galetta, D.; Crinò, L.; Vincenzi, B.; Barletta, E.; Pinto, C.; Ferraù, F.; Lambiase, M.; et al. The Presence of Concomitant Mutations Affects the Activity of EGFR Tyrosine Kinase Inhibitors in EGFR-Mutant Non-Small Cell Lung Cancer (NSCLC) Patients. Cancers 2019, 11, 341. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Ma, L.; Liu, Y.; Zhu, J.; Xin, Y.; Liu, X.; Wang, Y.; Zhang, T.; Yang, C.; Wang, S.; et al. Comprehensive characterization and clinical impact of concomitant genomic alterations in EGFR-mutant NSCLCs treated with EGFR kinase inhibitors. Lung Cancer 2020, 145, 63–70. [Google Scholar] [CrossRef]
- Christopoulos, P.; Kirchner, M.; Roeper, J.; Saalfeld, F.; Janning, M.; Bozorgmehr, F.; Magios, N.; Kazdal, D.; Volckmar, A.L.; Brückner, L.M.; et al. Risk stratification of EGFR+ lung cancer diagnosed with pane-based next-generation sequencing. Lung Cancer 2020, 148, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Heymach, J.V. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat. Rev. Cancer 2019, 19, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Garon, E.; Reck, M.; Nishio, K.; Heymach, J.V.; Nishio, M.; Novello, S.; Paz-Ares, L.; Popat, S.; Aix, S.P.; Wijayawardana, S.; et al. Abstract CT215: RELAY, ramucirumab plus erlotinib (RAM+ERL) versus placebo plus erlotinib (PBO+ERL) in previously untreatedEGFRmutation-positive metastatic NSCLC: Next generation sequencing (NGS) results. In Tumor Biology; American Association for Cancer Research (AACR): Philadelphia, PA, USA, 2020; Volume 80, p. CT215. [Google Scholar]
- Jiang, W.; Zeng, A.; Ning, R.; Zhao, W.; Su, C.; Wang, H.; Zhou, S.; Yu, Q. Predictive value of tumor genetic alteration profiling for chemotherapy and EGFR-TKI treatment in advanced NSCLC. Oncol. Lett. 2020, 19, 3859–3870. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhang, Y.; Tang, H.; He, J. EGFR gene copy number as a predictive/biomarker for patients with non-small-cell lung cancer receiving tyrosine kinase inhibitor treatment: A systematic review and meta-analysis. J. Investig. Med. 2016, 65, 72–81. [Google Scholar] [CrossRef]
- Dahabreh, I.J.; Linardou, H.; Kosmidis, P.; Bafaloukos, D.; Murray, S. EGFR gene copy number as a predictive biomarker for pa-tients receiving tyrosine kinase inhibitor treatment: A systematic review and meta-analysis in non-small-cell lung cancer. Ann. Oncol. 2011, 22, 545–552. [Google Scholar] [CrossRef]
- Takada, K.; Toyokawa, G.; Tagawa, T.; Kohashi, K.; Shimokawa, M.; Akamine, T.; Takamori, S.; Hirai, F.; Shoji, F.; Okamoto, T.; et al. PD-L1 expression according to the EGFR status in primary lung adenocarcinoma. Lung Cancer 2018, 116, 1–6. [Google Scholar] [CrossRef]
- Hsu, K.-H.; Huang, Y.-H.; Tseng, J.-S.; Chen, K.-C.; Ku, W.-H.; Su, K.-Y.; Chen, J.J.; Chen, H.-W.; Yu, S.-L.; Yang, T.-Y.; et al. High PD-L1 expression correlates with primary resistance to EGFR-TKIs in treatment naïve advanced EGFR-mutant lung adenocarcinoma patients. Lung Cancer 2019, 127, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Liao, W.Y.; Ho, C.C.; Chen, K.Y.; Tsai, T.H.; Hsu, C.L.; Su, K.Y.; Chang, Y.L.; Wu, C.-T.; Hsu, C.-C.; et al. Association between programmed death-ligand 1 expression, immune microenviron-ments, and clinical outcomes in epidermal growth factor receptor mutant lung adenocarcinoma patients treated with tyro-sine kinase inhibitors. Eur. J. Cancer 2020, 124, 110–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Itchins, M.; Nagrial, A.; Cooper, W.A.; De Silva, M.; Barnet, M.; Varikatt, W.; Sivasubramaniam, V.; Davis, A.; Gill, A.J.; et al. Relationship between PD-L1 expression and outcome in EGFR-mutant lung cancer patients treated with EGFR tyrosine kinase inhibitors. Lung Cancer 2021, 155, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Almendro, V.; Marusyk, A.; Polyak, K. Cellular Heterogeneity and Molecular Evolution in Cancer. Annu. Rev. Pathol. Mech. Dis. 2013, 8, 277–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (%) (n = 106) | Patients without Concomitant Pathogenic Mutations(%) (n = 59) | Patients with Concomitant Pathogenic Mutations(%) (n = 47) | Chi Square |
|---|---|---|---|---|
| Gender Male Female | 37 (34.9%) 69 (65.1%) | 19 (32.2%) 40 (67.8%) | 18 (38.3%) 29 (61.7%) | p = 0.513 |
| Age (median, range) | 69.8 (32.0–90.7) | 72.5 (34.6–90.7) | 66.6 (32.0–85.5) | |
| Age Younger than 70 years 70 years or older | 54 (50.9%) 52 (49.1%) | 24 (40.7%) 35 (59.3%) | 30 (63.8%) 17 (36.2%) | p = 0.018 |
| ECOG Performance Status PS 0 PS 1 PS 2 PS 3 | 48 (45.3%) 50 (47.2%) 7 (6.6%) 1 (0.9%) | 25 (42.4%) 27 (45.8%) 6 (10.2%) 1 (1.7%) | 23 (48.9%) 23 (48.9%) 1 (2.1%) 0 | p = 0.300 |
| Smoking status Never Former/current | 61 (57.5%) 45 (42.5%) | 35 (59.3%) 24 (40.7%) | 26 (55.3%) 21 (44.7%) | p = 0.679 |
| Stage at diagnosis Stage I Stage II Stage III Stage IV | 1 (0.9%) 6 (5.7%) 5 (4.9%) 94 (88.7%) | 0 3 (5.1%) 2 (3.4%) 54 (91.5%) | 1 (2.1%) 3 (6.4%) 3 (6.4%) 40 (85.1%) | p = 0.583 |
| Histology Adenocarcinoma Non-adenocarcinoma | 105 (99.1%) 1 (0.9%) | 58 (98.3%) 1 (1.7%) | 47 (100.0%) 0 | p = 0.370 |
| EGFR mutation Ex19 del Ex21 L858R Rare or double | 66 (62.3%) 33 (31.1%) 7 (6.6%) | 33 (55.9%) 23 (39.0%) 3 (5.1%) | 33 (70.2%) 10 (21.3%) 4 (8.5%) | p = 0.138 |
| Treatment Gefitinib/Erlotinib/Afatinib Osimertinib | 65 (61.3%) 41 (38.7%) | 34 (57.6%) 25 (42.4%) | 31 (66.0%) 16 (34.0%) | p = 0.382 |
| Number of metastatic sites 0 sites 1 site 2 sites 3 sites More than 3 sites | 1 (0.9%) 35 (33.0%) 29 (27.4%) 22 (20.7%) 19 (18.0%) | 0 20 (33.9%) 13 (22.0%) 14 (23.7%) 12 (20.3%) | 1 (2.1%) 15 (31.9%) 16 (34.0%) 8 (17.0%) 7 (14.9%) | p = 0.637 |
| Metastatic sites at diagnosis Lung Pleural CNS Liver Bone Adrenal Nodes | 32 (30.2%) 47 (44.3%) 35 (33.0%) 18 (17.0%) 51 (48.1%) 14 (13.2%) 53 (50%) | 19 (32.2%) 33 (55.9%) 20 (33.9%) 12 (20.3%) 29 (49.2%) 7 (11.9%) 24 (40.7%) | 13 (27.7%) 14 (29.8%) 15 (31.9%) 6 (12.8%) 22 (46.8%) 7 (14.9%) 29 (61.7%) | p = 0.613 p = 0.007 p = 0.829 p = 0.302 p = 0.810 p = 0.647 p = 0.032 |
| Progression-Free Survival | ||
|---|---|---|
| Variable | Univariate Analysis Hazard Ratio (95%CI), p-Value | Multivariate Analysis Hazard Ratio (95%CI), p-Value |
| Pathogenic comutations (yes vs. no) | 0.82 (0.52–1.31), p = 0.415 | |
| Age (older than 70 vs. younger) | 0.84 (0.53–1.33), p = 0.451 | |
| ECOG performance status (>=1 vs. 0) | 1.36 (0.85–2.18), p = 0.196 | |
| TKI generation (osimertinib vs. other) | 0.56 (0.32–0.98),p=0.04 | 0.55 (0.31–0.98), p = 0.043 |
| Number of metastatic sites (>1 vs. 1) | 1.50 (0.92–2.46), p = 0.106 | |
| Lung (yes vs. no) | 0.91 (0.53–1.57), p = 0.735 | |
| Pleura (yes vs. no) | 0.69 (0.43–1.10), p = 0.116 | |
| CNS (yes vs. no) | 2.43 (1.49–3.96), p < 0.001 | 2.14 (1.17–3.89), p = 0.013 |
| Liver (yes vs. no) | 1.92 (1.02–3.61),p=0.044 | |
| Bone (yes vs. no) | 1.62 (1.02–2.57),p=0.042 | |
| Overall Survival | ||
|---|---|---|
| Variables | Univariate Analysis Hazard Ratio (95%CI), p-Value | Multivariate Analysis Hazard Ratio (95%CI), p-Value |
| Pathogenic comutations (yes vs. no) | 0.61 (0.35–1.08), p = 0.088 | |
| Age (older than 70 vs. younger) | 1.25 (0.71–2.18), p = 0.439 | |
| ECOG performance status (>=1 vs. 0) | 1.72 (0.97–3.04), p = 0.062 | |
| TKI generation (osimertinib vs. other) | 0.86 (0.40–1.86), p = 0.698 | |
| Number of metastatic sites (>1 vs. 1) | 1.58 (0.85–2.95), p = 0.150 | |
| Lung (yes vs. no) | 1.01 (0.52–1.93), p = 0.989 | |
| Pleura (yes vs. no) | 0.79 (0.45–1.40), p = 0.421 | |
| CNS (yes vs. no) | 2.08 (1.20–3.62),p=0.009 | 2.62 (1.25–5.46),p=0.011 |
| Liver (yes vs. no) | 2.17 (1.10–4.29),p=0.025 | |
| Bone (yes vs. no) | 1.98 (1.12–3.48),p=0.018 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bironzo, P.; Reale, M.L.; Sperone, T.; Tabbò, F.; Caglio, A.; Listì, A.; Passiglia, F.; Di Maio, M.; Righi, L.; Bussolino, F.; et al. Clinical and Molecular Features of Epidermal Growth Factor Receptor (EGFR) Mutation Positive Non-Small-Cell Lung Cancer (NSCLC) Patients Treated with Tyrosine Kinase Inhibitors (TKIs): Predictive and Prognostic Role of Co-Mutations. Cancers 2021, 13, 2425. https://doi.org/10.3390/cancers13102425
Bironzo P, Reale ML, Sperone T, Tabbò F, Caglio A, Listì A, Passiglia F, Di Maio M, Righi L, Bussolino F, et al. Clinical and Molecular Features of Epidermal Growth Factor Receptor (EGFR) Mutation Positive Non-Small-Cell Lung Cancer (NSCLC) Patients Treated with Tyrosine Kinase Inhibitors (TKIs): Predictive and Prognostic Role of Co-Mutations. Cancers. 2021; 13(10):2425. https://doi.org/10.3390/cancers13102425
Chicago/Turabian StyleBironzo, Paolo, Maria Lucia Reale, Tessa Sperone, Fabrizio Tabbò, Andrea Caglio, Angela Listì, Francesco Passiglia, Massimo Di Maio, Luisella Righi, Federico Bussolino, and et al. 2021. "Clinical and Molecular Features of Epidermal Growth Factor Receptor (EGFR) Mutation Positive Non-Small-Cell Lung Cancer (NSCLC) Patients Treated with Tyrosine Kinase Inhibitors (TKIs): Predictive and Prognostic Role of Co-Mutations" Cancers 13, no. 10: 2425. https://doi.org/10.3390/cancers13102425
APA StyleBironzo, P., Reale, M. L., Sperone, T., Tabbò, F., Caglio, A., Listì, A., Passiglia, F., Di Maio, M., Righi, L., Bussolino, F., Scagliotti, G. V., & Novello, S. (2021). Clinical and Molecular Features of Epidermal Growth Factor Receptor (EGFR) Mutation Positive Non-Small-Cell Lung Cancer (NSCLC) Patients Treated with Tyrosine Kinase Inhibitors (TKIs): Predictive and Prognostic Role of Co-Mutations. Cancers, 13(10), 2425. https://doi.org/10.3390/cancers13102425