
The Mutational Landscape of Acute Myeloid Leukaemia Predicts Responses and Outcomes in Elderly Patients from the PETHEMA-FLUGAZA Phase 3 Clinical Trial

 , , , , ,
, , , , ,  , ,
, ,  , , ,
, , ,  ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Identification Cohort
2.2. Methods
2.2.1. High-Sensitivity Targeted Sequencing and Mutation Analysis
2.2.2. Availability of Data and Materials
2.2.3. Statistical Analysis
3. Results
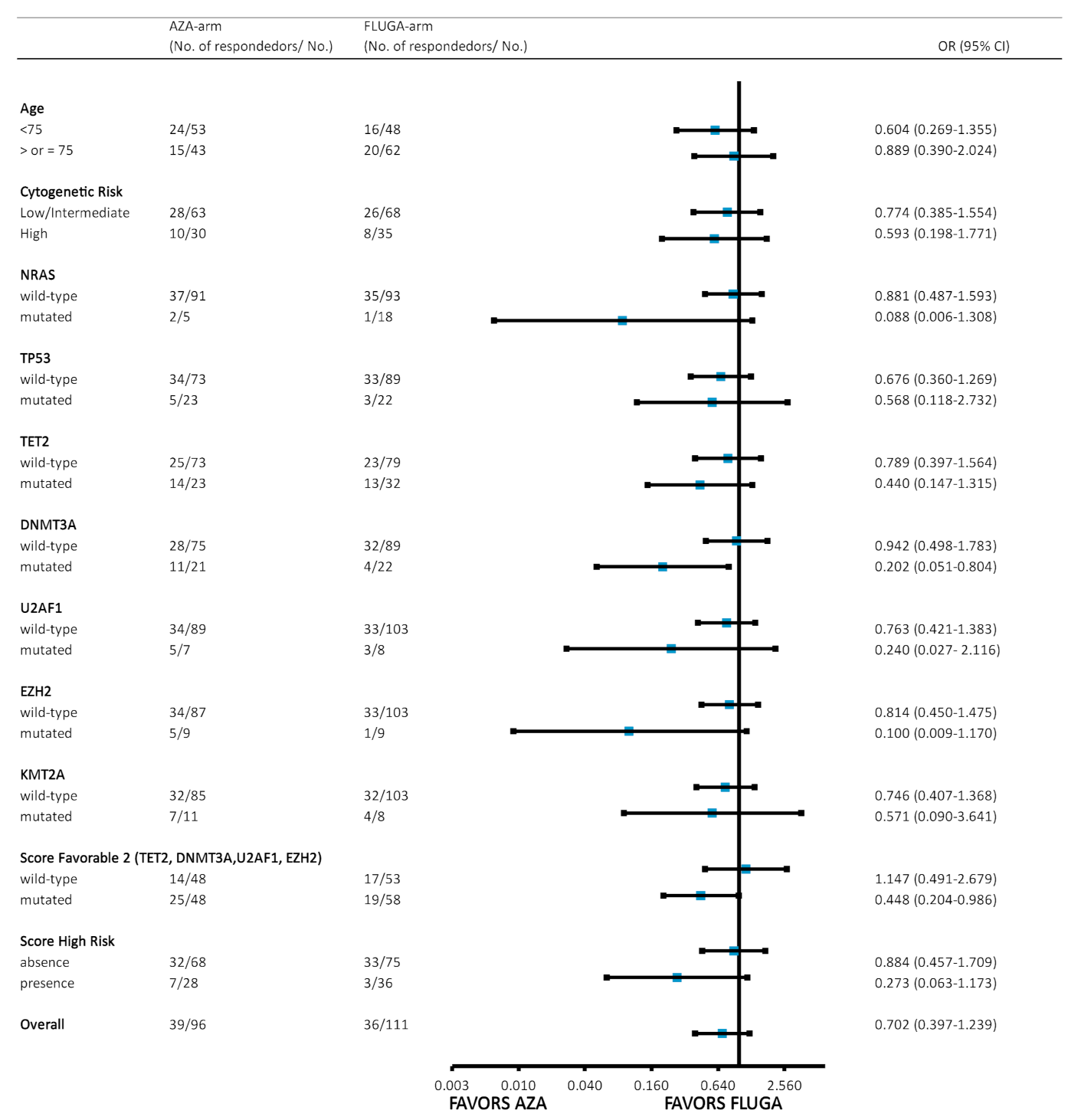
3.1. Mutational Landscape Predicts Response to Azacytidine and LDAC Plus Fludarabine Treatments
3.2. The Higher Variant Allele Frequency of Some Variants Influences Overall Response after the Third Cycle of Azacytidine and LDAC Plus Fludarabine
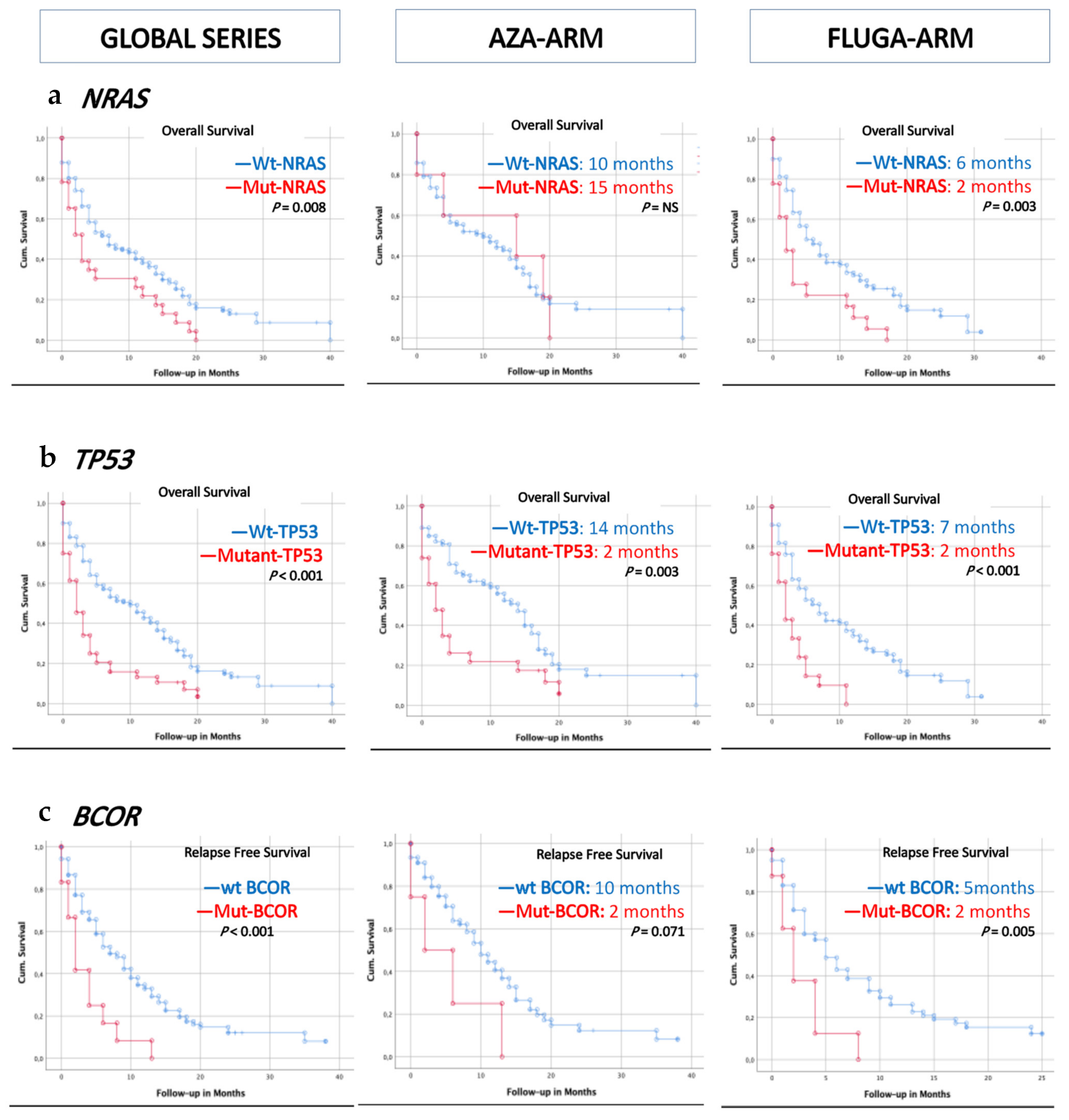
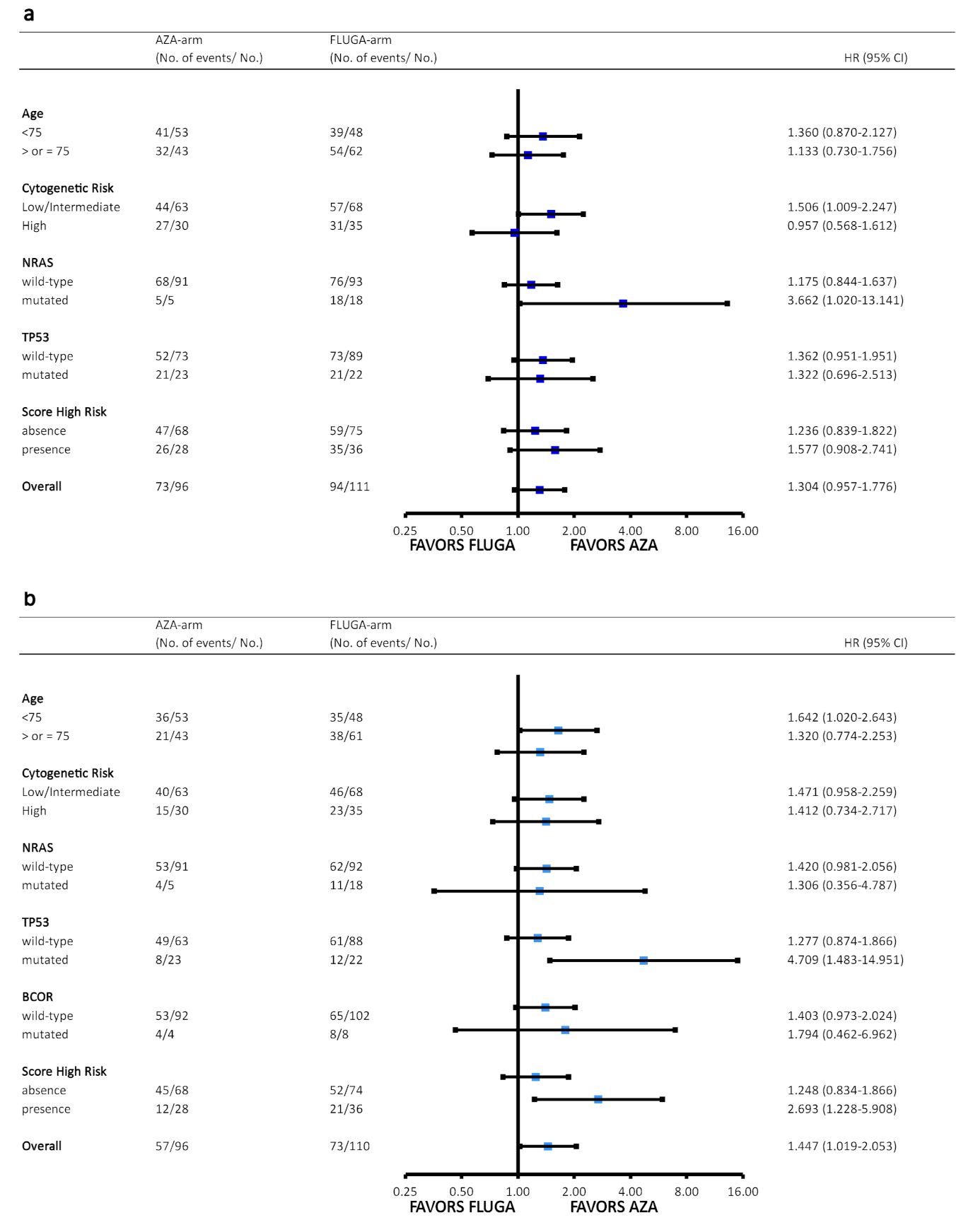
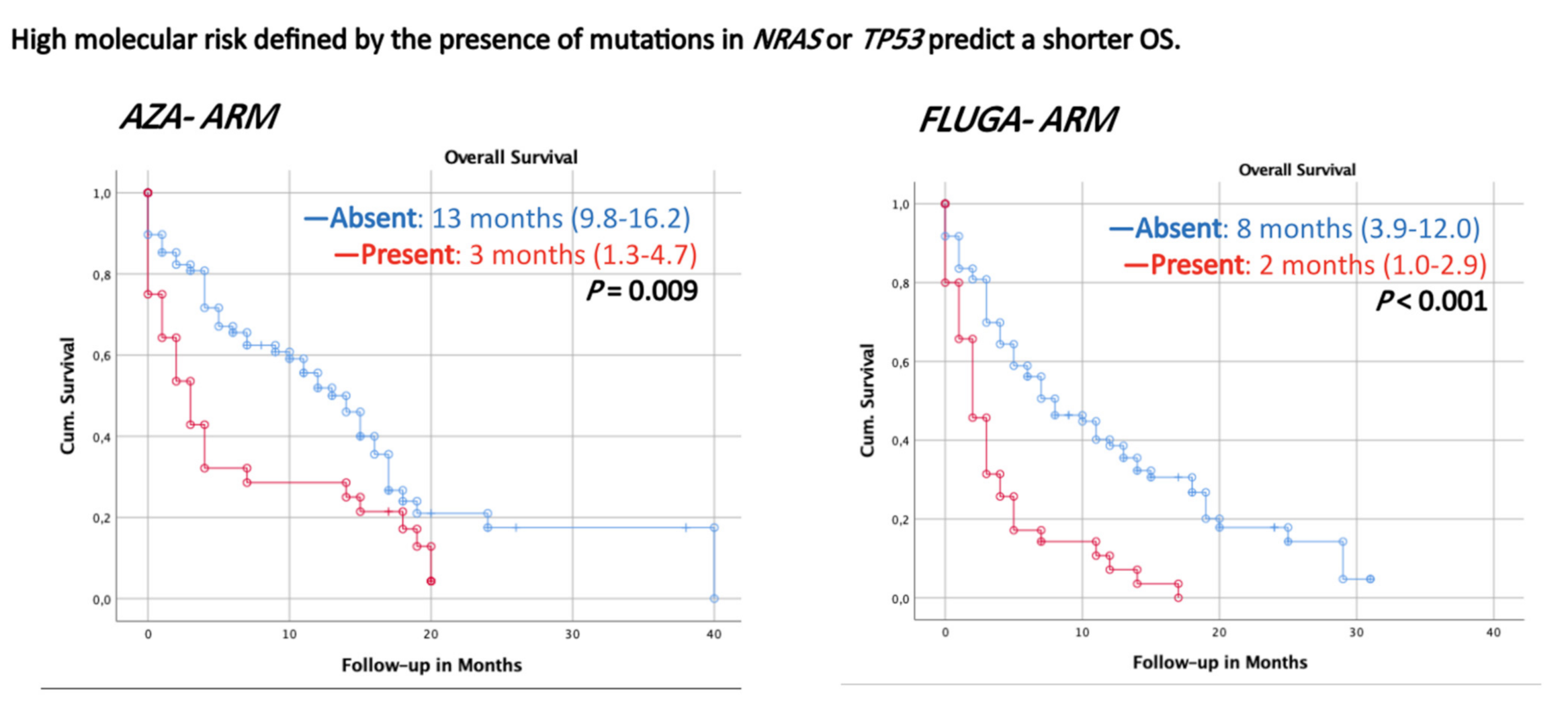
3.3. Somatic Mutations in NRAS, TP53, and BCOR Predict a Shorter Overall and/or Relapse-Free Survival According to Univariate Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Buccisano, F.; Dillon, R.; Freeman, S.D.; Venditti, A. Role of Minimal (Measurable) Residual Disease Assessment in Older Patients with Acute Myeloid Leukemia. Cancers 2018, 10, 215. [Google Scholar] [CrossRef] [Green Version]
- Juliusson, G.; Antunovic, P.; Derolf, Å.; Lehmann, S.; Möllgård, L.; Stockelberg, D.; Tidefelt, U.; Wahlin, A.; Höglund, M. Age and Acute Myeloid Leukemia: Real World Data on Decision to Treat and Outcomes from the Swedish Acute Leukemia Registry. Blood 2009, 113, 4179–4187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, A.K.; Milligan, D.; Prentice, A.G.; Goldstone, A.H.; McMullin MD, M.F.; Phil, R.K.H.; Phil, K.W. A Comparison of Low-dose Cytarabine and Hydroxyurea with or without all-Trans Retinoic Acid for Acute Myeloid Leukemia and High-Risk Myelodysplastic Syndrome in Patients not Considered Fit for Intensive Treatment. Cancer 2007, 109, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Mufti, G.J.; Hellström-Lindberg, E.; Santini, V.; Gattermann, N.; Germing, U.; Sanz, G.; List, A.F.; Gore, S.; Seymour, J.F.; et al. Azacitidine Prolongs Overall Survival Compared With Conventional Care Regimens in Elderly Patients With Low Bone Marrow Blast Count Acute Myeloid Leukemia. J. Clin. Oncol. 2010, 28, 562–569. [Google Scholar] [CrossRef]
- Williams, S.; Nanah, R.; Zblewski, D.; Elliott, M.; Hogan, W.J.; Tibes, R.; Foran, J.M.; Litzow, M.R.; Al-Kali, A. Deficiency of Current Acute Myeloid Leukemia (AML) Response Criteria to Predict Response to Hypomethylating Agent Therapy: The Value of Long-Lasting Stable Disease. Blood 2016, 128, 2799. [Google Scholar] [CrossRef]
- Kantarjian, H.; Kadia, T.; DiNardo, C.; Daver, N.; Borthakur, G.; Jabbour, E.; Garcia-Manero, G.; Konopleva, M.; Ravandi, F. Acute myeloid Leukemia: Current Progress and Future Directions. Blood Cancer J. 2021, 11, 1–25. [Google Scholar] [CrossRef]
- Bejar, R.; Lord, A.; Stevenson, K.; Bar-Natan, M.; Pérez-Ladaga, A.; Zaneveld, J.; Wang, H.; Caughey, B.; Stojanov, P.; Getz, G.; et al. TET2 Mutations Predict Response to Hypomethylating Agents in Myelodysplastic Syndrome Patients. Blood 2014, 124, 2705–2712. [Google Scholar] [CrossRef]
- Welch, J.S.; Petti, A.A.; Miller, C.A.; Fronick, C.C.; O’Laughlin, M.; Fulton, R.S.; Wilson, R.K.; Baty, J.D.; Duncavage, E.J.; Tandon, B.; et al. TP53 and Decitabine in Acute Myeloid Leukemia and Myelodysplastic Syndromes. N. Engl. J. Med. 2016, 375, 2023–2036. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and Management of AML in Adults: 2017 ELN Recommendations from an International Expert Panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Vives, S.; Martínez-Cuadrón, D.; Burgues, J.B.; Algarra, L.; Tormo, M.; Martínez-Sánchez, M.P.; Serrano, J.; Herrera, P.; Ramos, F.; Salamero, O.; et al. A Phase 3 Trial of Azacitidine Versus a Semi-Intensive Fludarabine and Cytarabine Schedule in Older Patients with Untreated Acute Myeloid Leukemia. Cancer 2021. [Google Scholar] [CrossRef]
- Simoes, C.; Paiva, B.; Martínez-Cuadrón, D.; Bergua, J.-M.; Vives, S.; Algarra, L.; Tormo, M.; Martinez, P.; Serrano, J.; Herrera, P.; et al. Measurable Residual Disease in Elderly Acute Myeloid Leukemia: Results from the PETHEMA-FLUGAZA Phase 3 Clinical Trial. Blood Adv. 2021, 5, 760–770. [Google Scholar] [CrossRef] [PubMed]
- Onecha, E.; Linares, M.; Rapado, I.; Ruiz-Heredia, Y.; Martinez-Sanchez, P.; Cedena, T.; Pratcorona, M.; Oteyza, J.P.; Herrera, P.; Barragan, E.; et al. A Novel Deep Targeted Sequencing Method for Minimal Residual Disease Monitoring in Acute Myeloid Leukemia. Haematologica 2018, 104, 288–296. [Google Scholar] [CrossRef]
- Onecha, E.; Ruiz-Heredia, Y.; Martínez-Cuadrón, D.; Barragán, E.; Martinez-Sanchez, P.; Linares, M.; Rapado, I.; Oteyza, J.P.; Magro, E.; Herrera, P.; et al. Improving the Prediction of Acute Myeloid Leukaemia Outcomes by Complementing Mutational Profiling with ex Vivo Chemosensitivity. Br. J. Haematol. 2020, 189, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Onecha, E.; Rapado, I.; Morales, M.L.; Carreño-Tarragona, G.; Martinez-Sanchez, P.; Gutierrez, X.; Pina, J.M.S.; Linares, M.; Gallardo, M.; Martinez-López, J.; et al. Monitoring of Clonal Evolution of Acute Myeloid Leukemia Identifies the Leukemia Subtype, Clinical Outcome and Potential New Drug Targets for Post-Remission Strategies or Relapse. Haematologica 2020. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, A.; Maharry, K.; Mrózek, K.; Thiede, C.; Marcucci, G.; Paschka, P.; Mayer, R.J.; Larson, R.A.; Liu, E.T.; Bloomfield, C.D. Patients With Acute Myeloid Leukemia and RAS Mutations Benefit Most From Postremission High-Dose Cytarabine: A Cancer and Leukemia Group B Study. J. Clin. Oncol. 2008, 26, 4603–4609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amatangelo, M.D.; Quek, L.; Shih, A.; Stein, E.M.; Roshal, M.; David, M.D.; Marteyn, B.; Farnoud, N.R.; De Botton, S.; Bernard, O.A.; et al. Enasidenib Induces Acute Myeloid Leukemia Cell Differentiation to Promote Clinical Response. Blood 2017, 130, 732–741. [Google Scholar] [CrossRef]
- Zhang, H.; Savage, S.; Schultz, A.R.; Bottomly, D.; White, L.; Segerdell, E.; Wilmot, B.; McWeeney, S.K.; Eide, C.A.; Nechiporuk, T.; et al. Clinical Resistance to Crenolanib in Acute Myeloid Leukemia due to Diverse Molecular Mechanisms. Nat. Commun. 2019, 10, 1–13. [Google Scholar] [CrossRef]
- McMahon, C.M.; Ferng, T.; Canaani, J.; Wang, E.S.; Morrissette, J.J.; Eastburn, D.J.; Pellegrino, M.; Durruthy-Durruthy, R.; Watt, C.D.; Asthana, S.; et al. Clonal Selection with RAS Pathway Activation Mediates Secondary Clinical Resistance to Selective FLT3 Inhibition in Acute Myeloid Leukemia. Cancer Discov. 2019, 9, 1050–1063. [Google Scholar] [CrossRef]
- Kuendgen, A.; Müller-Thomas, C.; Lauseker, M.; Haferlach, T.; Urbaniak, P.; Schroeder, T.; Brings, C.; Wulfert, M.; Meggendorfer, M.; Hildebrandt, B.; et al. Efficacy of Azacitidine is Independent of Molecular and Clinical Characteristics-an Analysis of 128 Patients with Myelodysplastic Syndromes or Acute Myeloid Leukemia and a Review of the Literature. Oncotarget 2018, 9, 27882–27894. [Google Scholar] [CrossRef] [Green Version]
- Döhner, H.; Dolnik, A.; Tang, L.; Seymour, J.F.; Minden, M.D.; Stone, R.M.; Del Castillo, T.B.; Al-Ali, H.K.; Santini, V.; Vyas, P.; et al. Cytogenetics and Gene Mutations Influence Survival in Older Patients with Acute Myeloid Leukemia Treated with Azacitidine or Conventional Care. Leukemia 2018, 32, 2546–2557. [Google Scholar] [CrossRef]
- Itzykson, R.; on behalf of the Groupe Francophone des Myelodysplasies (GFM); Kosmider, O.; Cluzeau, T.; Mas, V.M.-D.; Dreyfus, F.; Beyne-Rauzy, O.; Quesnel, B.; Vey, N.; Gelsi-Boyer, V.; et al. Impact of TET2 Mutations on Response Rate to Azacitidine in Myelodysplastic Syndromes and Low Blast Count Acute Myeloid Leukemias. Leukemia 2011, 25, 1147–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drusbosky, L.M.; Singh, N.K.; Hawkins, K.E.; Salan, C.; Turcotte, M.; Wise, E.A.; Meacham, A.; Vijay, V.; Anderson, G.G.; Kim, C.C.; et al. A Genomics-Informed Computational Biology Platform Prospectively Predicts Treatment Responses in AML and MDS Patients. Blood Adv. 2019, 3, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.-H.; Kim, Y.-J.; Yim, S.-H.; Kim, H.-J.; Kwon, Y.-R.; Hur, E.-H.; Goo, B.-K.; Choi, Y.-S.; Lee, S.H.; Chung, Y.-J.; et al. Somatic Mutations Predict Outcomes of Hypomethylating Therapy in Patients with Myelodysplastic Syndrome. Oncotarget 2016, 7, 55264–55275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terada, K.; Yamaguchi, H.; Ueki, T.; Usuki, K.; Kobayashi, Y.; Tajika, K.; Gomi, S.; Kurosawa, S.; Saito, R.; Furuta, Y.; et al. Usefulness of BCOR Gene Mutation as a Prognostic Factor in Acute Myeloid Leukemia with Intermediate Cytogenetic Prognosis. Genes Chromosom. Cancer 2018, 57, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Dinardo, C.D.; Pratz, K.; Pullarkat, V.; Jonas, B.A.; Arellano, M.; Becker, P.S.; Frankfurt, O.; Konopleva, M.; Wei, A.H.; Kantarjian, H.M.; et al. Venetoclax Combined with Decitabine or Azacitidine in Treatment-Naive, Elderly Patients with Acute Myeloid Leukemia. Blood 2019, 133, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.-W.; Tsai, C.-H.; Lin, C.-C.; Tien, F.-M.; Chen, Y.-W.; Lin, H.-Y.; Yao, M.; Lin, Y.-C.; Cheng, C.-L.; Tang, J.-L.; et al. Cytogenetics and Mutations could Predict Outcome in Relapsed and Refractory Acute Myeloid Leukemia Patients Receiving BCL-2 Inhibitor Venetoclax. Ann. Hematol. 2020, 99, 501–511. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | AZA Arm (N = 96) | FLUGA Arm (N = 111) | |
|---|---|---|---|
| Age at diagnosis | Years, median (range) | 75 (65–90) | 76 (65–88) |
| Blasts at diagnosis | %, median | 55 | 53 |
| WBC at diagnosis | ×10−9/L, median | 22 | 21 |
| Dyserythropoiesis | n cases, % | 45 | 47 |
| Dysmyelopoiesis | n cases, % | 38 | 42 |
| Dysthrombopoiesis | n cases, % | 23 | 31 |
| AML origin | de novo | 44 | 40 |
| AML secondary MDS | 47 | 45 | |
| AML secondary Treatment | 5 | 11 | |
| FAB classification | M0/M1/M2/M4/M5/M6/M7/NOS | 16/15/13/1/21/12/5/9 | 16/21/22/0/22/12/5/10 |
| Cytogenetics | Abnormal Karyotype/Normal Karyotype | 46/38 | 51/26 |
| Cytogenetics Risk Group | Low–Intermediate Risk | 63 | 68 |
| High Risk | 30 | 35 | |
| WHO classification | AML with certain genetic abnormalities | 5 | 13 |
| AML with myelodysplastic-related changes | 47 | 45 | |
| AML related to chemotherapy or radiation previous | 5 | 11 | |
| AML NOS | 38 | 42 | |
| Follow-up time | Months, median (SD) | 15 (9) | 16 (7) |
| Variable | HR | Risk of Death 95% CI for HR | p-Value (Bonferroni) | |
|---|---|---|---|---|
| Lower | Upper | |||
| NRAS (wt vs. mut) | 1.94 | 1.21 | 3.08 | 0.005 (0.067) |
| TP53 (wt vs. mut) | 2.57 | 1.76 | 3.76 | 9.8 × 10−7 (0.128 × 10−5) |
| Variable | HR | Risk of Relapse 95% CI for HR | p-Value (Bonferroni) | |
| Lower | Upper | |||
| BCOR (wt vs. mut) | 3.60 | 1.81 | 7.16 | 0.000271 (0.004) |
| Parameter | Global Series | Favors AZA-Arm * |
|---|---|---|
| Predictive markers for response to treatment | Lower patient age Wildtype TP53 Mutated KMT2A, NF1 or TET2 | Mutated DNMT3A Presence Score predicting an AZA response |
| Prognostic markers for OS | Mutated NRAS or TP53 confer adverse prognostic for OS | Mutated NRAS Low-Intermediate Cytogenetic Risk. |
| Prognostic markers for RFS | Mutated BCORconfers adverse prognostic for RFS | Mutated TP53 Presence high molecular risk (HMR) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayala, R.; Rapado, I.; Onecha, E.; Martínez-Cuadrón, D.; Carreño-Tarragona, G.; Bergua, J.M.; Vives, S.; Algarra, J.L.; Tormo, M.; Martinez, P.; et al. The Mutational Landscape of Acute Myeloid Leukaemia Predicts Responses and Outcomes in Elderly Patients from the PETHEMA-FLUGAZA Phase 3 Clinical Trial. Cancers 2021, 13, 2458. https://doi.org/10.3390/cancers13102458
Ayala R, Rapado I, Onecha E, Martínez-Cuadrón D, Carreño-Tarragona G, Bergua JM, Vives S, Algarra JL, Tormo M, Martinez P, et al. The Mutational Landscape of Acute Myeloid Leukaemia Predicts Responses and Outcomes in Elderly Patients from the PETHEMA-FLUGAZA Phase 3 Clinical Trial. Cancers. 2021; 13(10):2458. https://doi.org/10.3390/cancers13102458
Chicago/Turabian StyleAyala, Rosa, Inmaculada Rapado, Esther Onecha, David Martínez-Cuadrón, Gonzalo Carreño-Tarragona, Juan Miguel Bergua, Susana Vives, Jesus Lorenzo Algarra, Mar Tormo, Pilar Martinez, and et al. 2021. "The Mutational Landscape of Acute Myeloid Leukaemia Predicts Responses and Outcomes in Elderly Patients from the PETHEMA-FLUGAZA Phase 3 Clinical Trial" Cancers 13, no. 10: 2458. https://doi.org/10.3390/cancers13102458
APA StyleAyala, R., Rapado, I., Onecha, E., Martínez-Cuadrón, D., Carreño-Tarragona, G., Bergua, J. M., Vives, S., Algarra, J. L., Tormo, M., Martinez, P., Serrano, J., Herrera, P., Ramos, F., Salamero, O., Lavilla, E., Gil, C., López Lorenzo, J. L., Vidriales, M. B., Labrador, J., ... on behalf of the Programa para el Estudio de la Terapeutica en Hemopatias Malignas (PETHEMA) Cooperative Study Group. (2021). The Mutational Landscape of Acute Myeloid Leukaemia Predicts Responses and Outcomes in Elderly Patients from the PETHEMA-FLUGAZA Phase 3 Clinical Trial. Cancers, 13(10), 2458. https://doi.org/10.3390/cancers13102458