
Malignant Transformation of Postmenopausal Endometriosis: A Systematic Review of the Literature

 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
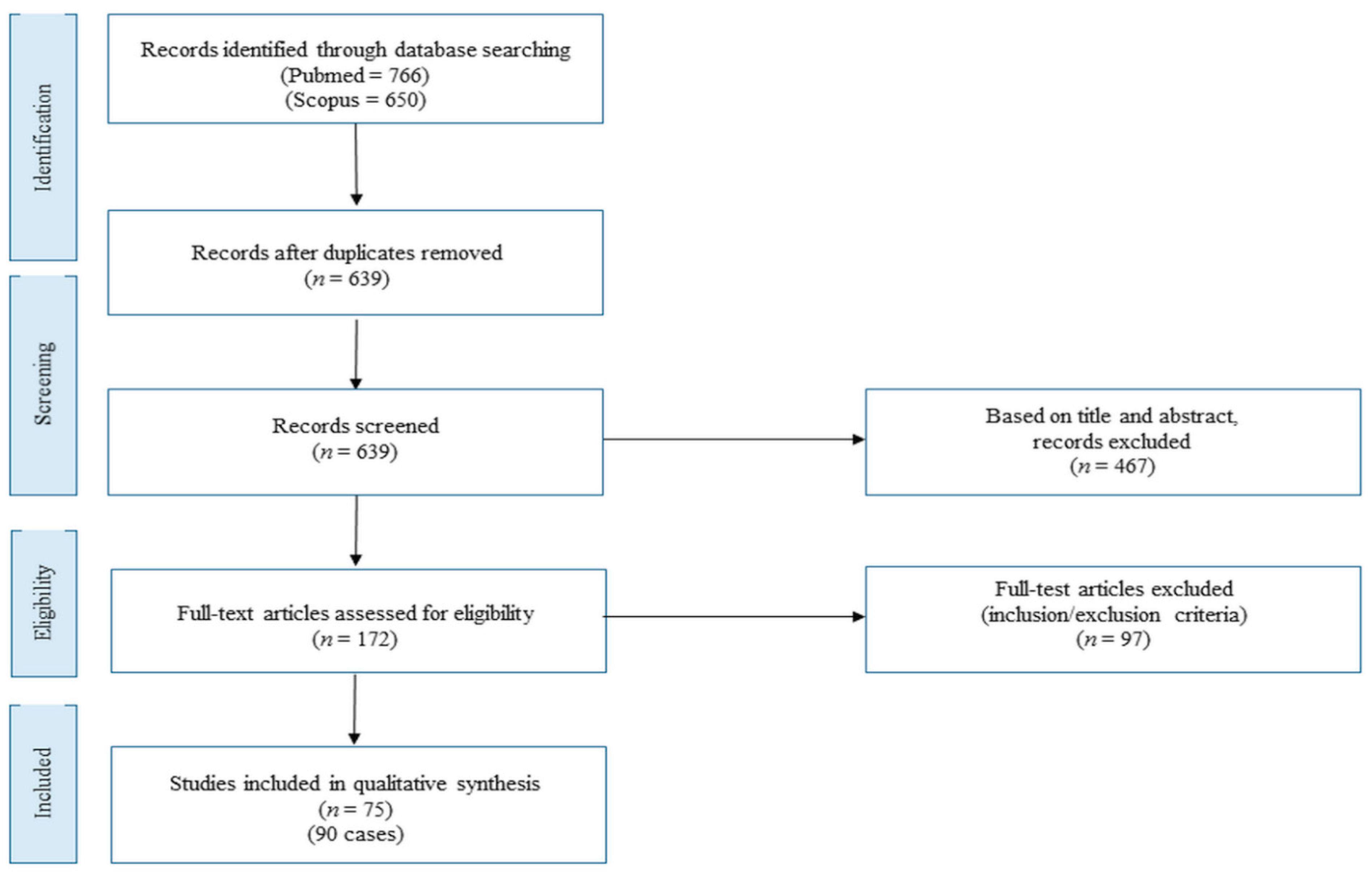
2. Materials and Methods
- Population: postmenopausal women with malignant endometriosis transformation;
- Intervention: personal history including data on previous endometriosis and surgery, hormone replacement therapy (HRT) use, and duration over the years of case publication;
- Comparison: no comparison expected;
- Outcomes: (1) presence of common patient characteristics based on descriptive analysis, (2) distribution of recurrent clinical conditions over time, (3) follow-up outcomes when available (alive, recurrence, death).
3. Results
3.1. Literature Review Details
3.2. Patient Characteristics
3.3. Signs/Symptoms at Clinical Presentation
3.4. Hormone Replacement Therapy Data
3.5. Cancer Lesion Characteristics
3.6. Treatment and Outcome
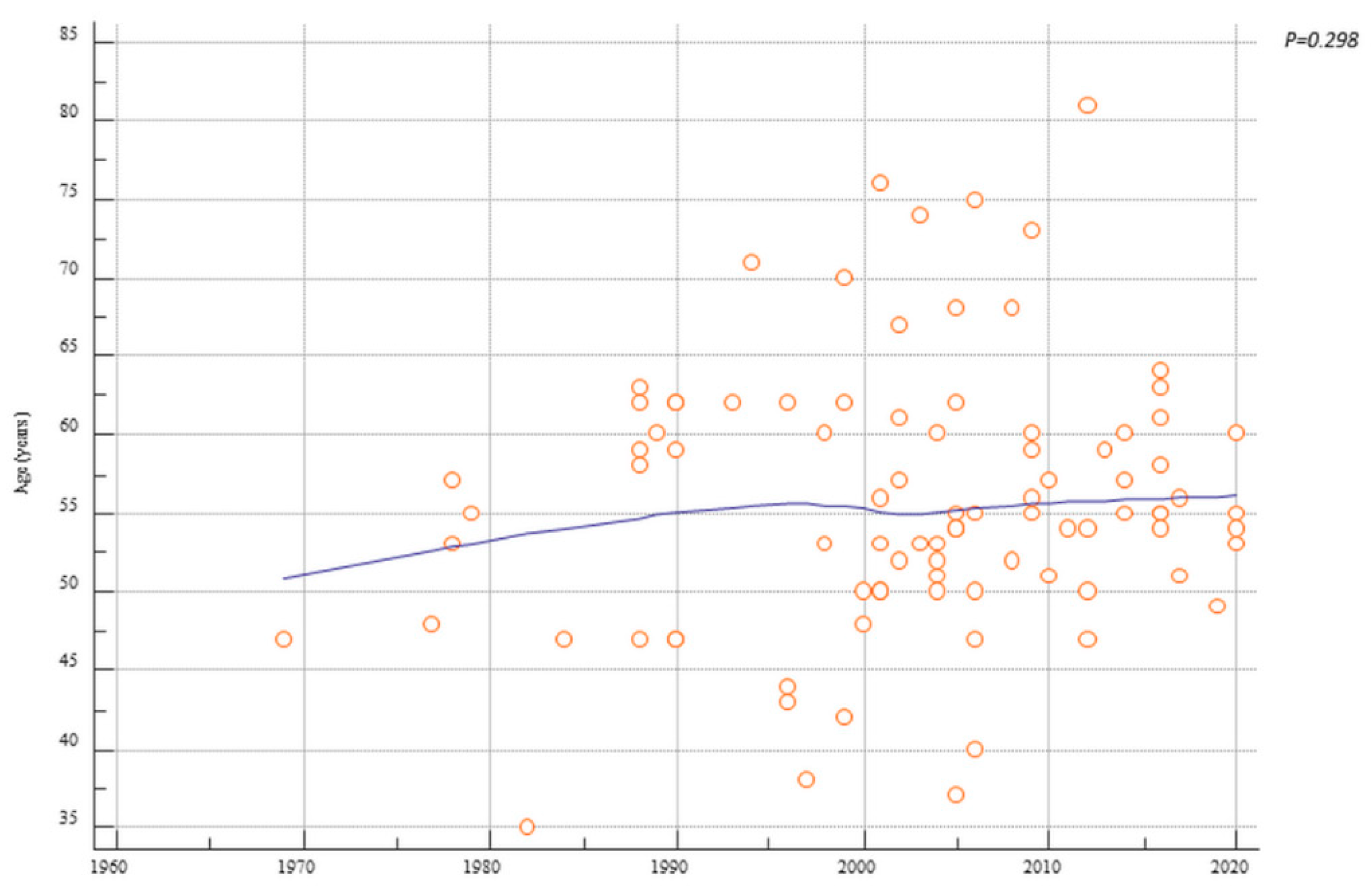
3.7. Distribution of Patient Characteristics over Time
3.8. Missing Data
4. Discussion
Conclusions
- Previous endometriosis
- Definitive gynecological surgery before menopause
- Estrogen-only HRT for a relatively long time.
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Johnson, N.P.; Hummelshoj, L. World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum. Reprod. 2013, 28, 1552–1568. [Google Scholar] [CrossRef] [PubMed]
- Dunselman, G.A.; Vermeulen, N.; Becker, C.; Calhaz-Jorge, C.; D’Hooghe, T.; De Bie, B.; Heikinheimo, O.; Horne, A.W.; Kiesel, L.; Nap, A.; et al. European Society of Human Reproduction and Embryology. ESHRE guideline: Management of women with endometriosis. Hum. Reprod. 2014, 29, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, R.; Tang, S.; Feng, F.; Liu, C.; Wang, L.; Zhao, W.; Zhang, T.; Yao, Y.; Wang, X.; et al. Impact of endometriosis on risk of ovarian, endometrial and cervical cancers: A meta-analysis. Arch. Gynecol. Obstet. 2019, 299, 35–46. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, T.H.; Chung, H.H.; Song, Y.S. Risk and prognosis of ovarian cancer in women with endometriosis: A meta-analysis. Br. J. Cancer 2014, 110, 1878–1890. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.A.; Almaria, M.J.G. Postmenopausal endometriosis: Drawing a clearer clinical picture. Climacteric 2018, 21, 249–255. [Google Scholar] [CrossRef]
- Gemmell, L.C.; Webster, K.E.; Kirtley, S.; Vincent, K.; Zondervan, K.T.; Becker, C.M. The management of menopause in women with a history of endometriosis: A systematic review. Hum. Reprod. Update 2017, 23, 481–500. [Google Scholar] [CrossRef] [Green Version]
- Prisma Transparent Reporting of Systematic Reviews and Meta-Analyses. Available online: http://www.prisma-statement.org/ (accessed on 5 December 2020).
- Sampson, J.A. Endometrial carcinoma of the ovary, arising in endometrial tissue in that organ. Arch. Surg. 1925, 10, 1–72. [Google Scholar] [CrossRef]
- Scott, R.B. Malignant changes in endometriosis. Obs. Gynecol. 1953, 2, 283–289. [Google Scholar]
- Carbone, F.; Kaur, M.M.; Chok, A.Y.; Kontovounisios, C.; Ind, T.; Rasheed, S. Endometrial stromal sarcoma arising from polypoid endometriosis: Case report and literature review. Int. J. Surg. Case Rep. 2020, 72, 537–540. [Google Scholar] [CrossRef]
- Sao, C.H.; Lai, W.A.; Lin, S.C.; Chang, C.M.; Chen, Y.J.; Wang, P.H. Endometriosis-associated epithelial ovarian cancer: Primary synchronous different cellular type on each ovary. Taiwan J. Obstet. Gynecol. 2020, 59, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Uehara, T.; Yoshida, H.; Kondo, A.; Kato, T. A case of cervical adenocarcinoma arising from endometriosis in the absence of human papilloma virus infection. J. Obstet. Gynaecol. Res. 2020, 46, 536–541. [Google Scholar] [CrossRef]
- Cope, A.G.; VanBuren, W.M.; Sheedy, S.P. Endometriosis in the postmenopausal female: Clinical presentation, imaging features, and management. Abdom. Radiol. 2020, 45, 1790–1799. [Google Scholar] [CrossRef] [PubMed]
- Catherine, C.; Koji, M.; Paulette, M.F. Endometrioid Adenocarcinoma Arising in a Paratubal Cyst: A Case Report and Review of the Literature. Appl. Immunohistochem. Mol. Morphol. 2017, 25, e21–e24. [Google Scholar]
- Tashima, L.; Hori, K.; Ono, H.; Nagano, T.; Nakatsuka, S.I.; Ito, K. Endometrioid adenocarcinoma originating simultaneously from endometrium, sites of adenomyosis and ovarian endometriosis: A case report and review of our cancer database. Int. J. Surg. Case Rep. 2017, 41, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Luca, R.; Antonio, M.; Teresa, P.; Francesco, P.; Giuseppe, B. Testosterone Aromatization to Estradiol in Course of Ovarian Functioning Brenner Tumor Associated with Endometrial Carcinoma and Endometriosis (Roncati-Manenti Triad). Int. J. Gynecol. Cancer 2016, 26, 1461Y1464. [Google Scholar]
- Giovanni, P.; Mauro, C.; Anna, S.; Bruni, F.; Anna, P.; Marcello, C. Primary vaginal adenosarcoma with sarcomatous overgrowth arising in recurrent endometriosis: Feasibility of laparoscopic treatment and review of the literature. J. Minim. Invasive Gynecol. 2016, 23, 833–838. [Google Scholar]
- Andriola, V.; Battaglia, M.; Ditonno, P.; Fiore, M.G.; De Fazio, M.; Memeo, R.; Altomare, D.F. The unexpected conundrum of endometrioid carcinoma in deep rectal endometriosis arising 11 years after total hysterectomy bilateral salpingo-oophorectomy. Int. J. Colorectal Dis. 2016, 31, 475–477. [Google Scholar] [CrossRef]
- Lu, B.; Chen, Q.; Zhang, X. Serous carcinoma arising from uterine adenomyosis/adenomyotic cyst of the cervical stump: A report of 3 cases. Diagn Pathol. 2016, 11, 46. [Google Scholar] [CrossRef] [Green Version]
- Mohling, S.I. Malignant transformation of endometriosis: An unusual diverticular mass. J. Endometr. Pelvic Pain Disord. 2016, 8, 67–70. [Google Scholar] [CrossRef]
- Ijichi, S.; Mori, T.; Suganuma, I.; Yamamoto, T.; Matsushima, H.; Ito, F.; Akiyama, M.; Kusuki, I.; Kitawaki, J. Clear cell carcinoma arising from cesarean section scar endometriosis: Case report and review of the literature. Case Rep. Obstet. Gynecol. 2014, 2014, 642483. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.J.; Zhang, L.; Liu, Z.P.; Shi, Y.Q.; Liu, Y.X. Ovarian malignant mixed germ cell tumor with clear cell carcinoma in a postmenopausal woman. Int. J. Clin. Exp. Pathol. 2014, 7, 8996–9001. [Google Scholar] [PubMed]
- Taga, S.; Sawada, M.; Nagai, A.; Yamamoto, D.; Hayase, R. A case of endometrioid adenocarcinoma arising from adenomyosis. Case Rep. Obs. Gynecol. 2014, 2014, 569295. [Google Scholar] [CrossRef] [Green Version]
- Lah, K.; Desai, D.; Hadway, P.; Perry-Keene, J.; Coughlin, G. Primary vesical clear cell adenocarcinoma arising in endometriosis: A rare case of mullerian origin. Anticancer Res. 2013, 33, 615–617. [Google Scholar]
- Hansen, K.; Simon, R.A.; Lawrence, W.D.; Quddus, M.R. Unilateral pelvic mass presenting in postmenopausal patients: Report of two unusual cases. Ann. Diagn. Pathol. 2012, 16, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Shalin, S.; Haws, A.; Carter, D.; Zarrin-Khame, N. Clear cell adenocarcinoma arising from endometriosis in abdominal wall cesarean section scar: A case report and review of the literature. J. Coutaneous Pathol. 2012, 39, 1035–1041. [Google Scholar] [CrossRef]
- Mann, S.; Patel, P.; Matthews, C.M.; Pinto, K.; O’Connor, J. Malignant transformation of endometriosis within the urinary bladder. Proc. Bayl. Univ. Med. Cent. 2012, 25, 293–295. [Google Scholar] [CrossRef]
- Coyne, J.D. Aggressive angiomyxoma admixed with endometriosis: A case report. Int. J. Surg. Pathol. 2012, 20, 205–207. [Google Scholar] [CrossRef]
- Takahashi, Y.; Mogami, H.; Hamada, S. Alpha-fetoprotein producing ovarian clear cell carcinoma with a neometaplasia to hepatoid carcinoma arising from endometriosis: A case report. J. Dec. Obstet. Gynaecol. Res. 2011, 37, 1842–1846. [Google Scholar] [CrossRef]
- Healy, K.A.; Carney, K.J.; Osunkoya, A.O. Endometrioid adenocarcinoma in the native ureter of a renal transplant patient: Case report and review of the literature. Sci. World J. 2010, 10, 1714–1722. [Google Scholar] [CrossRef]
- Nomoto, K.; Hori, T.; Kiva, C.; Fukuoka, J. Endometrioid adenocarcinoma of the vagina with a microglandular pattern arising from endometriosis after hysterectomy. Pathol. Int. 2010, 60, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, K.; Yasuda, M.; Kajiwara, H.; Nakamura, N.; Sato, S.; Nishijima, Y.; Mikami, M.; Osamura, R.Y. Clear cell adenocarcinoma arising from adenomyosis. Int. J. Gynecol. Pathol. 2009, 28, 262–266. [Google Scholar] [CrossRef]
- Efthymiou, C.A. Endometriosis associated intestinal tumors: A consequence of long term unopposed oestrogen? Ann. R. Coll. Surg. Eng. 2009, 91, 259–260. [Google Scholar] [CrossRef]
- Karanjgaokar, V.C.; Murphy, D.J.; Samra, J.S.; Mann, C.H. Malignant transformation of residual endometriosis after hysterectomy: A case series. Fertil. Steril. 2009, 92, 2037.e19–2037.e21. [Google Scholar] [CrossRef] [PubMed]
- Motohara, K. Endometrioid adenocarcinoma arising in adenomyosis: Elucidation by periodic magnetic resonance imaging evaluations. Int. J. Clin. Oncol. 2008, 13, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Al-Talib, A. Andometrioid adenocaricnoma 13 yearsafter total abdominal hysterectomy and bilateral salpingo oophorectomy. Saudi. Med. J. 2008, 29, 1044–1047. [Google Scholar] [PubMed]
- Noel, J.C. Uretral mullerian carcinosarcoma (mixed mullerian tumor) associated with endometriosis occurring in a patient with a concentrated soy isoflavones supplementation. Arch. Gynecol. Obs. 2006, 274, 389–392. [Google Scholar] [CrossRef]
- Nomura, S. Endometrioid adenocarcinoma arising form endometriosis during 2 years of estrogen replacement therapy after total hysterectomy and bilateral salpingo oophorectomy. Acta Obs. Gynecol. Scand. 2006, 85, 1019–1021. [Google Scholar] [CrossRef]
- Shah, C. Clear cell adenocarcinoma of the vagina in a patient with vaginal endometriosis. Gynecol. Oncol. 2006, 103, 1130–1132. [Google Scholar] [CrossRef]
- Hirabayashi, K. Ovarian nongestational choriocarcinoma mixed with various epithelial malignancies in association with endometriosis. Gynecol. Oncol. 2006, 102, 111–117. [Google Scholar] [CrossRef]
- Milam, M.R.; Atkinson, J.B.; Currie, J.L. Adenosarcoma arising in inguinal endometriosis. Obs. Gynecol. 2006, 108, 753–755. [Google Scholar] [CrossRef]
- Alexander Taylor, A. Postmenopausal endometriois and malignant transformation of endometriosis: A case series. Gynecol. Surg. 2005, 2, 135–137. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.Y.; Changchien, C.C.; Chen, H.H. Extrauterine mullerian adenocarcinoma associated with endometriosis and rectal villotubular adenoma: Report and a case and review of the literature. Int. J. Gynecol. Cancer 2005, 15, 361–365. [Google Scholar] [PubMed]
- Somoye, G.O.; Gull, S. Adenocarcinoma of the vaginal vault following prolonged unopposed oestrogen replacement therapy. J. Obs. Gynaecol. 2005, 25, 220–221. [Google Scholar] [CrossRef]
- Kawate, S.; Takeyoshi, I.; Ikota, H.; Numaga, Y.; Sunose, Y.; Morishita, Y. Endometrioid adenocarcinoma arising from endometriosis of the mesentrium of the sigmoid colon. Jpn. J. Clin. Oncol. 2005, 35, 154–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salerno, M.G.; Masciullo, V.; Naldini, A. Endometrioid adenocarcinoma with squamous differentiation arising from uretral endometriosis in a patient with no history of gonadal endometriosis. Gynecol. Oncol. 2005, 99, 749–752. [Google Scholar] [CrossRef]
- Jelovsek, J.E. Endometriosis of the liver containing mullerian adenosarcoma: Case report. AMJ Obs. Gynecol. 2004, 191, 1725–1727. [Google Scholar] [CrossRef] [Green Version]
- Lacroix-Triki, M.; Beyris, L.; Martel, P.; Marques, B. Low-grade endometrial stromal sarcoma arising from sciatic nerve endometriosis. Obs. Gynecol. 2004, 104, 1147–1149. [Google Scholar] [CrossRef] [PubMed]
- Soliman, N.F.; Evans, A.J. Malignancy arising in residual endometriosis following hysterectomy and hormone replacement therapy. J. Br. Menop. Soc. 2004, 10, 123–124. [Google Scholar] [CrossRef]
- Garavan, F.; Grainger, R.; Jeffers, M. Endometrioid carcinoma of the urinary bladder complicating vesical mullerianosis: A case report and review of the literature. Virchows Arch. 2004, 444, 587–589. [Google Scholar] [CrossRef]
- Areia, A. Endometrioid adenocaricnoma arising in endometriosis foci six years after estrogen replacement therapy: A case report. Eur. J. Gynecol. Oncol. 2004, 25, 255–256. [Google Scholar]
- Bese, T. Extensive pelvic endometriosis with malignant change in tamoxifen trated postmenopausal women. Int. J. Gynecol. Cancer 2003, 13, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Okugawa, K.; Hirakawa, T.; Ogawa, S.; Kaku, T.; Nakano, H. Ovarian endometrioid adenocarcinoma arising from an endometriotic cyst in a postmenopausal woman under tamoxifen therapy for breast cancer: A case report. Gynecol. Oncol. 2002, 87, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Petersen, V.C.; Underwood, J.C.; Wells, M.; Shepherd, N.A. Primary endometrioid adenocarcinoma of the large intestine arising in colorectal endometriosis. Histopathology 2002, 40, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.D.; Owen, E.; Berresford, A.; Sutton, C. Endometrial adenocarcinoma arising from endometriosis of the rectosigmoid colon. Gynecol. Oncol. 2002, 86, 220–222. [Google Scholar] [CrossRef]
- Powell, J.L.; Conor, P.; Henderson, G.S. Androgenproducing, atypically proliferating endometrioid tumour arising in endometriosis. South. Med. J. 2001, 94, 450–453. [Google Scholar] [CrossRef]
- Larvey, S.; Gillmer, M. Malignant transformation of residual endometriosis in women on unopposed oestrogen hormone replacement therapy. Br. J. Obs. Gynaecol. 2001, 108, 1106–1107. [Google Scholar]
- Debus, G.; Schuhmacher, I. Endometrial adenocarcinoma arising during estrogenic treatment 17 years after total abdominal hysterectomy and bilateral salpingo-oophorectomy: A case report. Acta Obstet. Gynecol. Scand. 2001, 80, 589–590. [Google Scholar] [CrossRef]
- Magtibay, P.M.; Heppell, J.; Leslie, K.O. Endometriosis-associated invasive adenocarcinoma involving the rectum in a postmenopausal female: Report of a case. Dis. Colon Rectum 2001, 44, 1530–1533. [Google Scholar] [CrossRef]
- Jimenez, R.E.; Tiguert, R.; Hurley, P. Unilateral hydronephrosis resulting from intramural obstruction of the ureter by adenosquamous endometrioid carcinoma arising from disseminated endometriosis. Urology 2000, 56, 331. [Google Scholar] [CrossRef]
- McCluggage, W.G.; Bryson, C.; Lamki, H.; Boyle, D.D. Benign, borderline, and malignant endometrioid neoplasia arising in endometriosis in association with tamoxifen therapy. Int. J. Gynecol. Pathol. 2000, 19, 276–279. [Google Scholar] [CrossRef]
- Jennings, T.S. Clear Cell Ovarian Carcinoma Following Long-Term Tamoxifen Use. Breast J. 1999, 5, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, C.; Silverberg, S.G. Tamoxifen-associated polyps (basalomas) arising in multiple endometriotic foci: A case report and review of the literature. Gynecol. Oncol. 1999, 73, 305–311. [Google Scholar] [CrossRef]
- Taylor, M.; Bowen-Simpkins, P.; Barrington, J. Complications of unopposed oestrogen following radical surgery. Gynaecology 1999, 19, 647–648. [Google Scholar]
- Sidhu, S.; Rainer, E.S.; O’Connor, T.O. Extraovarian endometrioid carcinoma associated with unopposed oestrogen replacement therapy. Aust. N. Z. J. Obs. Gynaecol. 1998, 38, 125–127. [Google Scholar] [CrossRef]
- Horiuchi, A.; Osada, R.; Nakayama, K.; Toki, T.; Nikaido, T.; Fujii, S. Ovarian yolk sac tumor with endometrioid carcinoma arising from endometriosis in a postmenopausal woman, with special reference to expression of alpha-fetoprotein, sex steroid receptors, and p53. Gynecol. Oncol. 1998, 70, 295–299. [Google Scholar] [CrossRef]
- Abu, M.A.E.; Sinha, P.; Totoe, L. Endometrial cancer thirteen years after total abdominal hysterectomy and bilateral salpingo-oophorectomy and hormone replacement therapy: A case report. Eur. J. Gynecol. Oncol. 1997, 18, 482–483. [Google Scholar]
- Eichhorn, J.H.; Scully, R.E. Endometrioid ciliated-cell tumors of the ovary: A report of five cases. Int. J. Gynecol. Pathol. 1996, 15, 248–256, Erratum in 1996, 15, 369. [Google Scholar] [CrossRef]
- McCluggage, W.G.; Bailie, C.; Weir, P. Endometrial stromal sarcoma arising in pelvic endometriosis in a patient receiving unopposed oestrogen therapy. Br. J. Obs. Gynaecol. 1996, 103, 1252–1254. [Google Scholar] [CrossRef]
- Cohen, I.; Altaras, M.M.; Lew, S.; Tepper, R.; Beyth, Y.; Ben-Baruch, G. Ovarian endometrioid carcinoma and endometriosis developing in a postmenopausal breast cancer patient during tamoxifen therapy: A case report and review of the literature. Gynecol. Oncol. 1994, 55, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Dunn, S.; Boed-Petersen, K.; Michelsen, J.W. Endometrioid carcinoma arising from endometriosis of the sigmoid colon during estrogenic treatment. Acta Obs. Gynecol. Scand. 1993, 72, 676–678. [Google Scholar] [CrossRef]
- Vara, A.R.; Ruzics, E.P.; Moussabeck, O.; Martin, D.C. Endometrioid adenosarcoma of the bladder arising from endometriosis. J. Urol. 1990, 143, 813–815. [Google Scholar] [CrossRef]
- Heaps, J.M.; Neiberg, R.K.; Berek, J.S. Malignant neoplasms arising in endometriosis. Obs. Gynecol. 1990, 75, 1023–1032. [Google Scholar] [CrossRef]
- Orr, J.W.; Holimon, J.L.; Sission, P.F. Vaginal adenocarcinoma developing in residual pelvic endometriosis: A clinical dilemma. Gynecol. Oncol. 1989, 33, 96–98. [Google Scholar] [CrossRef]
- Al-Izzi, M.S.; Horton, L.W.; Kelleher, J.; Fawcett, D. Malignant transformation in endometriosis of the urinary bladder. Histopathology 1989, 14, 191–198. [Google Scholar] [CrossRef]
- Remnitz, C.; Brand, E.; Neiberg, R.K. Malignancy arising in endometriosis associated with unopposed estrogen replacement. Obs. Gynecol. 1988, 1, 444–447. [Google Scholar]
- Brunson, G.L.; Barclay, D.I.; Sanders, M. Malignant extraovarian endometriosis: Two case reports and review of the literature. Gynecol. Oncol. 1988, 30, 123–130. [Google Scholar] [CrossRef]
- Granai, C.O.; Walters, M.D.; Safaii, H. Malignant transformation of vaginal endometriosis. Obs. Gynecol. 1984, 64, 592–595. [Google Scholar]
- Kapp, D.S.; Merino, M.; LiVolsi, V. Case reports: Adenocarcinoma of the vagina developing in endometriosis; long term survival following radiation therapy. Gynecol. Oncol. 1982, 14, 271–278. [Google Scholar] [CrossRef]
- Shamsuddin, A.K.M.; Villa Santa, U.; Tang, C.K. Adenocarcinoma arising from extragonadal endometriosis 14 years after total hysterectomy and bilateral salpingo-oophorectomy for endometriosis: Report of a case with ultrastructural studies. Am. J. Obs. Gynecol. 1979, 133, 585–586. [Google Scholar] [CrossRef]
- Lott, J.V.; Rubin, R.J.; Salvati, E.P.; Salazar, G.H. Endometrioid carcinoma of the rectum arising in endometriosis: Report of a case. Dis. Colon Rectum 1978, 21, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, R.S.; Ehmann, R.L.; Knapp, R.C. Endometrial stromal sarcoma arising from vaginal endometriosis. Obstet. Gynecol. 1978, 51, 34–37S. [Google Scholar]
- Brooks, J.J.; Wheeler, J.E. Malignancy arising in extragonadal endometriosis. A case report and summary of the literature. Cancer 1977, 40, 3065–3073. [Google Scholar] [CrossRef]
- Young, E.; Gamble, C. Primary adenocarcinoma of the rectovaginal septum arising from endometriosis. Report of a case. Cancer 1969, 24, 597–601. [Google Scholar] [CrossRef]
- Kempers, R.D.; Dockerty, M.B.; Hunt, A.B.; Symmonds, R.E. Significant postmenopausal endometriosis. Surg. Gynecol. Obs. 1960, 111, 348–356. [Google Scholar]
- Williams, T.J.; Pratt, J.H. Endometriosis in 1000 consecutive celiotomies: Incidence and management. Am. J. Obs. Gynecol. 1977, 129, 245–250. [Google Scholar] [CrossRef]
- Bulun, S.E. Endometriosis. N. Engl. J. Med. 2009, 360, 268–279. [Google Scholar] [CrossRef]
- Bulun, S.E.; Yang, S.; Fang, Z.; Gurates, B.; Tamura, M.; Sebastian, S. Estrogen production and metabolism in endometriosis. Ann. N. Y. Acad. Sci. 2002, 955, 396–406. [Google Scholar] [CrossRef]
- Stern, R.C.; Dash, R.; Bentley, R.C.; Snyder, M.J.; Haney, A.F.; Robboy, S.J. Malignancy in endometriosis: Frequency and comparison of ovarian and extraovarian types. Int. J. Gynecol. Pathol. 2001, 20, 133–139. [Google Scholar] [CrossRef]
- Melin, A.; Sparen, P.; Perrson, I.; Bergqvist, A. Endometriosis and the risk of cancer with special emphasis on ovarian cancer. Hum. Reprod. 2006, 21, 1237–1242. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, H. Ovarian cancer in endometriosis: Epidemiology, natural history, and clinical diagnosis. Int. J. Clin. Oncol. 2009, 14, 378–382. [Google Scholar] [CrossRef]
- Modesitt, S.C.; Tortolero-Luna, G.; Robinson, J.B.; Gershenson, D.M.; Wolf, J.K. Ovarian and extraovarian endometriosis-associated cancer. Obs. Gynecol. 2002, 100, 788–795. [Google Scholar]
- Kobayashi, H.; Sumimoto, K.; Kitanaka, T. Ovarian endometrioma–risks factors of ovarian cancer development. Eur. J. Obs. Gynecol. Reprod. Biol. 2008, 138, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, A.N.; Koutsouridou, R.N.; Penketh, R.J. Rectovaginal endometriosis—A frequently missed diagnosis. J. Obs. Gynaecol. 2007, 27, 605–607. [Google Scholar] [CrossRef]
- Vikstedt, T.; Arffman, M.; Heliövaara-Peippo, S.; Manderbacka, K.; Reissell, E.; Keskimäki, I. Change in medical practice over time? A register based study of regional trends in hysterectomy in Finland in 2001–2018. BMC Womens Health 2021, 21, 242. [Google Scholar] [CrossRef] [PubMed]
- Lycke, K.D.; Kahlert, J.; Damgaard, R.; Mogensen, O.; Hammer, A. Trends in Hysterectomy Incidence Rates During 2000–2015 in Denmark: Shifting from Abdominal to Minimally Invasive Surgical Procedures. Clin. Epidemiol. 2021, 13, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Ghiasi, M.; Kulkarni, M.T.; Missmer, S.A. Is Endometriosis More Common and More Severe than It Was 30 Years Ago? J. Minim. Invasive Gynecol. 2020, 27, 452–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christ, J.P.; Yu, O.; Schulze-Rath, R.; Grafton, J.; Hansen, K.; Reed, S.D. Incidence, prevalence, and trends in endometriosis diagnosis: A United States population-based study from 2006 to 2015. Am. J. Obs. Gynecol. 2021, 6, 67. [Google Scholar] [CrossRef]
- Vercellini, P.; Viganò, P.; Buggio, L.; Makieva, S.; Scarfone, G.; Cribiù, F.M.; Parazzini, F.; Somigliana, E. Perimenopausal management of ovarian endometriosis and associated cancer risk: When is medical or surgical treatment indicated? Best Pract. Res. Clin. Obs. Gynaecol. 2018, 51, 151–168. [Google Scholar] [CrossRef]
- Marie-Scemama, L.; Even, M.; De La Joliniere, J.B.; Ayoubi, J.M. Endometriosis and the menopause: Why the question merits our full attention. Horm. Mol. Biol. Clin. Investig. 2019, 26, 37. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Sample Size (90) Available Data (%) |
|---|---|
| Age at diagnosis (mean ± standard deviation) | 55.8 ± 8.5 |
| Nulligravid | 18/90 (20) |
| Hypertension | 4/89 (4.5) |
| Diabetes | 3/89 (3.4) |
| Breast cancer | 7/90 (7.8) |
| Leiomyomatosis | 17/89 (19.1) |
| BMI ≥ 30 | 3/89 (3.4) |
| Tamoxifen use | |
| Current use | 2 (2.2) |
| Past use | 4 (4.4) |
| No | 84 (93.3) |
| Previous endometriosis/adenomiosis | |
| Adenomiosis | 4 (4.4) |
| Endometriosis | 44 (48.9) |
| Adenomiosis + Endometriosis | 10 (11.1) |
| No | 32 (35.6) |
| Previous surgery | |
| Hysterectomy | 6/89 (6.7) |
| Hysterectomy + BSO | 51/89 (57.3) |
| Other surgery | 10/89 (11.2) |
| No surgery | 22/89 (24.7) |
| Previous BSO | 52/89 (58.4) |
| Endometriosis as indication for previous surgery | |
| Yes | 37/67 (55.2) |
| No | 30/67 (34.8) |
| Signs | Sample Size (90) Available Data (%) |
|---|---|
| Constipation | 2 (2.2) |
| Dyschezia | 5 (5.6) |
| Hematuria | 8 (8.9) |
| Pelvic mass | 31 (34.4) |
| Weight loss | 3 (3.3) |
| None | 41 (45.6) |
| Abnormal uterine bleeding | 39/90 (43.3) |
| Symptoms | Sample size (90) Available data (%) |
| Dyspareunia | 1 (1.1) |
| Urinary symptoms | 2 (2.2) |
| Pelvic/abdominal pain | 50 (55.6) |
| Asymptomatic | 37 (41.1) |
| No sign and symptom | 21/90 (23.3) |
| Hormone Replacement Therapy | Sample Size (90) Available Data (%) |
|---|---|
| HRT use | |
| Yes | 49/74 (66.2) |
| No | 25/74 (33.8) |
| HRT type | |
| CEE | 8/49 (16.3) |
| E only | 28/49 (57.1) |
| E + T | 5/49 (10.2) |
| CT | 7/49 (14.3) |
| Soy Isoflavones | 1/49 (2.1) |
| Duration of treatment (years) | |
| Median (interquartile range) | 11 (5–14) |
| ≤5 years | 16/44 (36.3) |
| >5 years | 28/44 (63.7) |
| Histology | Sample Size (90) Available Data (%) |
|---|---|
| EAC | 45 (50.0) |
| CCC | 9 (10.0) |
| EAC + CCC | 6 (6.7) |
| Adenocarcinoma | 16 (17.8) |
| Sarcoma | 11 (12.2) |
| Other histology | 3 (3.3) |
| Cancer location | Sample size (90) Available data (%) |
| Abdomen | 4/88 (4.5) |
| Bladder | 5/88 (5.7) |
| Cervix | 3/88 (3.4) |
| Ovary | 16/88 (18.2) |
| Parametrium | 1/88 (1.1) |
| Pelvis | 21/88 (23.9) |
| Rectum | 8/88 (9.1) |
| Ureter | 8/88 (9.1) |
| Uterus | 7/88 (8.0) |
| Vaginal vault | 15/88 (17.0) |
| Involved site | Sample size (90) Available data (%) |
| Multiple | 32 (35.6) |
| Single | 58 (64.4) |
| Surgical Treatment | Sample Size (90) Available Data (%) |
|---|---|
| Debulking surgery | 13/83 (15.7) |
| Mass excision | 21/83 (25.3) |
| RAH + BSO | 2/83 (2.4) |
| TH + BSO | 20/83 (24.1) |
| Other surgery | 21/83 (25.3) |
| No surgery | 6/83 (7.2) |
| Medical treatment | Sample size (90) Available data (%) |
| Adjuvant CHT | 30/79 (38.0) |
| Adjuvant CHT + RT | 4/79 (5.1) |
| Adjuvant RT | 11/79 (13.9) |
| Neoadjuvant CHT | 1/79 (1.3) |
| No medical treatment | 33/79 (41.8) |
| Outcome | Sample size (90) Available data (%) |
| Alive | 48/61 (78.7) |
| Recurrence | 6/61 (9.8) |
| Deceased | 7/61 (11.5) |
| Follow-up duration (months) | 45/90 |
| Median (interquartile range) | 12 (6.75–25) |
| Outcome | Years of Case Publication | p Value | ||
|---|---|---|---|---|
| <2000 | 2000–2009 | ≥2010 | ||
| (19) | (24) | (18) | ||
| n (%) | n (%) | n (%) | 0.102 | |
| Alive | 14 (73.7) | 20 (83.3) | 14 (77.8) | |
| Deceased | 4 (21.1) | 3 (12.5) | 0 (0.0) | |
| Recurrence | 1 (5.3) | 1 (4.2) | 4 (22.2) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giannella, L.; Marconi, C.; Di Giuseppe, J.; Delli Carpini, G.; Fichera, M.; Grelloni, C.; Giuliani, L.; Montanari, M.; Insinga, S.; Ciavattini, A. Malignant Transformation of Postmenopausal Endometriosis: A Systematic Review of the Literature. Cancers 2021, 13, 4026. https://doi.org/10.3390/cancers13164026
Giannella L, Marconi C, Di Giuseppe J, Delli Carpini G, Fichera M, Grelloni C, Giuliani L, Montanari M, Insinga S, Ciavattini A. Malignant Transformation of Postmenopausal Endometriosis: A Systematic Review of the Literature. Cancers. 2021; 13(16):4026. https://doi.org/10.3390/cancers13164026
Chicago/Turabian StyleGiannella, Luca, Chiara Marconi, Jacopo Di Giuseppe, Giovanni Delli Carpini, Mariasole Fichera, Camilla Grelloni, Lucia Giuliani, Michele Montanari, Salvatore Insinga, and Andrea Ciavattini. 2021. "Malignant Transformation of Postmenopausal Endometriosis: A Systematic Review of the Literature" Cancers 13, no. 16: 4026. https://doi.org/10.3390/cancers13164026
APA StyleGiannella, L., Marconi, C., Di Giuseppe, J., Delli Carpini, G., Fichera, M., Grelloni, C., Giuliani, L., Montanari, M., Insinga, S., & Ciavattini, A. (2021). Malignant Transformation of Postmenopausal Endometriosis: A Systematic Review of the Literature. Cancers, 13(16), 4026. https://doi.org/10.3390/cancers13164026