
Long-Term Effects of Childhood Cancer Treatment on Dentition and Oral Health: A Dentist Survey Study from the DCCSS LATER 2 Study

 , ,
, , 


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Inclusion
3.2. Patient Demographics and Treatment Characteristics
3.3. Oral Health Data
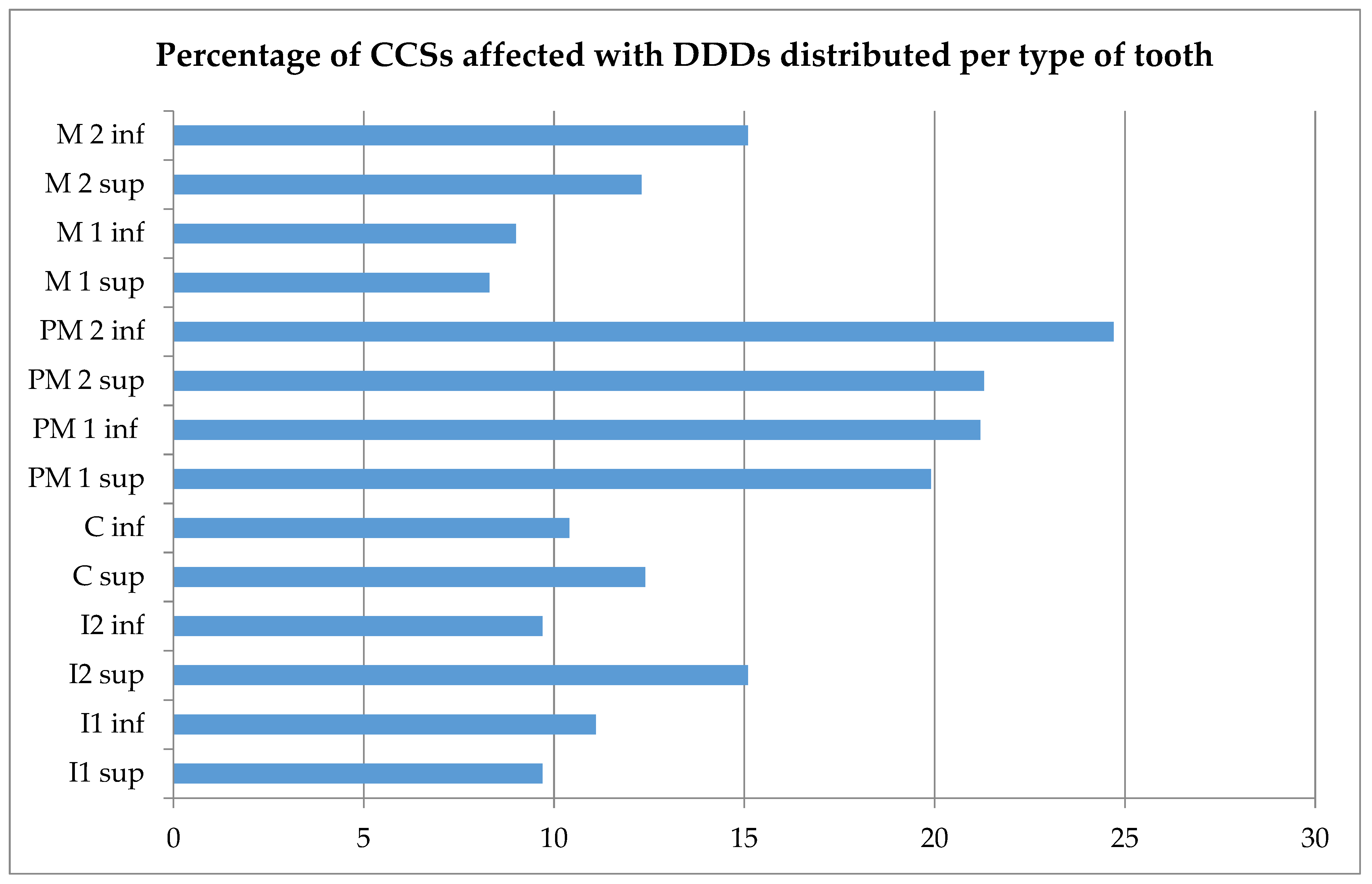
3.4. Dental Developmental Disorders
3.5. Risk Factor Analysis
4. Discussion
4.1. Oral Health
4.2. Age at Diagnosis
4.3. Head and Neck Irradiation
4.4. Chemotherapy
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Leary, M.; Krailo, M.; Anderson, J.R.; Reaman, G.H. Progress in Childhood Cancer: 50 Years of Research. Semin. Oncol. 2008, 35, 484–493. [Google Scholar] [CrossRef] [Green Version]
- Geenen, M.M.; Cardous-Ubbink, M.C.; Kremer, L.C.M.; Bos, C.V.D.; van der Pal, H.J.H.; Heinen, R.C.; Jaspers, M.W.M.; Koning, C.C.E.; Oldenburger, F.; Langeveld, N.E.; et al. Medical assessment of adverse health outcomes in long-term survivors of childhood cancer. J. Am. Med. Assoc. 2007, 297, 2705–2715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.; et al. Chronic health conditions in adult survivors of childhood cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef]
- Raber-Durlacher, J.; Epstein, J.; Bresters, D.; Stern-Zivan, L. Oral complications in children with cancer. Eur. J. Paediatr. Dent. Clin. Suppl. 2005, 6, 3–12. [Google Scholar]
- Gawade, P.; Hudson, M.M.; Kaste, S.C.; Neglia, J.P.; Constine, L.S.; Robison, L.L.; Ness, K.K. A systematic review of dental late effects in survivors of childhood cancer. Pediatr. Blood Cancer 2014, 61, 407–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busenhart, D.M.; Erb, J.; Rigakos, G.; Eliades, T.; Papageorgiou, S.N. Adverse effects of chemotherapy on the teeth and surrounding tissues of children with cancer: A systematic review with meta-analysis. Oral Oncol. 2018, 83, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Seremidi, K.; Kloukos, D.; Polychronopoulou, A.; Kattamis, A.; Kavvadia, K. Late effects of chemo and radiation treatment on dental structures of childhood cancer survivors. A systematic review and meta-analysis. Head Neck 2019, 41, 3422–3433. [Google Scholar] [CrossRef]
- Kaste, S.C.; Goodman, P.; Leisenring, W.; Stovall, M.; Hayashi, R.J.; Yeazel, M.; Beiraghi, S.; Hudson, M.M.; Sklar, C.A.; Robison, L.L.; et al. Impact of Radiation and Chemotherapy on Risk of Dental Abnormalities: A Report from the Childhood Cancer Survivor Study. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2009, 115, 5817–5827. [Google Scholar] [CrossRef]
- Avşar, A.; Elli, M.; Darka, Ö.; Pinarli, G. Long-term effects of chemotherapy on caries formation, dental development, and salivary factors in childhood cancer survivors. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, 781–789. [Google Scholar] [CrossRef]
- Nemeth, O.; Hermann, P.; Kivovics, P.; Garami, M. Long-term effects of chemotherapy on dental status of children cancer survivors. Pediatr. Hematol. Oncol. 2013, 30, 208–215. [Google Scholar] [CrossRef]
- Lauritano, D.; Petruzzi, M. Decayed, missing and filled teeth index and dental anomalies in long-term survivors leukaemic children: A prospective controlled study. Med. Oral Patol. Oral y Cir. Bucal 2012, 17, e977–e980. [Google Scholar] [CrossRef]
- EEffinger, K.E.; Migliorati, C.A.; Hudson, M.M.; McMullen, K.P.; Kaste, S.C.; Ruble, K.; Guilcher, G.M.T.; Shah, A.J.; Castellino, S.M. Oral and dental late effects in survivors of childhood cancer: A Children’s Oncology Group report. Support. Care Cancer 2014, 22, 2009–2019. [Google Scholar] [CrossRef] [Green Version]
- Van Der Pas-Van Voskuilen, I.G.M.; Veerkamp, J.S.J.; Raber-Durlacher, J.E.; Bresters, D.; Van Wijk, A.J.; Barasch, A.; McNeal, S.; Gortzak, A.T. Long-term adverse effects of hematopoietic stem cell transplantation on dental development in children. Support Care Cancer 2009, 17, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- Çetiner, D.; Çetiner, S.; Uraz, A.; Alpaslan, G.H.; Alpaslan, C.; Memikoğlu, T.U.T.; Karadeniz, C. Oral and dental alterations and growth disruption following chemotherapy in long-term survivors of childhood malignancies. Care Cancer 2018, 27, 1891–1899. [Google Scholar] [CrossRef] [PubMed]
- Quispe, R.A.; Rodrigues, A.C.C.; Buaes, A.M.G.; Capelozza, A.L.A.; Rubira, C.M.F.; Santos, P.S.D.S. A case-control study of dental abnormalities and dental maturity in childhood cancer survivors. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 498–507.e3. [Google Scholar] [CrossRef] [PubMed]
- Wilberg, P.; Kanellopoulos, A.; Ruud, E.; Hjermstad, M.J.; Fosså, S.D.; Herlofson, B.B. Dental abnormalities after chemotherapy in long-term survivors of childhood acute lymphoblastic leukemia 7–40 years after diagnosis. Support. Care Cancer 2016, 24, 1497–1506. [Google Scholar] [CrossRef]
- Goho, C. Chemoradiation therapy: Effect on dental development. Pediatr. Dent. 1993, 15, 6–12. [Google Scholar]
- Sonis, A.; Tarbell, N.; Valachovic, R.W.; Gelber, R.; Schwenn, M.; Sallan, S. Dentofacial development in long-term survivors of acute lymphoblastic leukemia: A comparison of three treatment modalities. Cancer 1990, 66, 2645–2652. [Google Scholar] [CrossRef]
- Kang, C.-M.; Hahn, S.M.; Kim, H.S.; Lyu, C.J.; Lee, J.-H.; Lee, J.; Han, J.W. Clinical risk factors influencing dental developmental disturbances in childhood cancer survivors. Cancer Res. Treat. 2018, 50, 926–935. [Google Scholar] [CrossRef] [Green Version]
- Milgrom, S.A.; van Luijk, P.; Pino, R.; Ronckers, C.M.; Kremer, L.C.; Gidley, P.W.; Grosshans, D.R.; Laskar, S.; Okcu, M.F.; Constine, L.S.; et al. Salivary and Dental Complications in Childhood Cancer Survivors Treated with Radiation Therapy to the Head and Neck: A Pediatric Normal Tissue Effects in the Clinic (PENTEC) Comprehensive Review. Int. J. Radiat. Oncol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Seremidi, K.; Kavvadia, K.; Kattamis, A.; Polychronopoulou, A. Dental late effects of antineoplastic treatment on childhood cancer survivors: Radiographic findings. Int. J. Paediatr. Dent. 2021, in press. [Google Scholar] [CrossRef]
- Maguire, A.; Craft, A.W.; Evans, R.G.B.; Amineddine, H.; Kernahan, J.; MacLeod, R.I.; Murray, J.J.; Welbury, R. The long-term effects of treatment on the dental condition of children surviving malignant disease. Cancer 1987, 60, 2570–2575. [Google Scholar] [CrossRef]
- Macleod, R.I.; Welbury, R.R.; Soames, J.V. Effects of cytotoxic chemotherapy on dental development. J. R. Soc. Med. 1987, 80, 207–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, M.; Kamata, T.; Yanagisawa, R.; Morita, D.; Saito, S.; Sakashita, K.; Shiohara, M.; Kurita, H.; Koike, K.; Nakazawa, Y. Increasing Risk of Disturbed Root Development in Permanent Teeth in Childhood Cancer Survivors Undergoing Cancer Treatment at Older Age. J. Pediatr. Hematol. 2017, 39, e150–e154. [Google Scholar] [CrossRef] [PubMed]
- Ritwik, P. Dental care for patients with childhood cancers. Ochsner J. 2018, 18, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Hölttä, P.; Hovi, L.; Saarinen-Pihkala, U.M.; Peltola, J.; Alaluusua, S. Disturbed root development of permanent teeth after pediatric stem cell transplantation. Dental root development after SCT. Cancer 2005, 103, 1484–1493. [Google Scholar] [CrossRef]
- Knol, M.J.; Le Cessie, S.; Algra, A.; Vandenbroucke, J.P.; Groenwold, R.H. Overestimation of risk ratios by odds ratios in trials and cohort studies: Alternatives to logistic regression. Can. Med. Assoc. J. 2012, 184, 895–899. [Google Scholar] [CrossRef] [Green Version]
- Green, D.M.; Nolan, V.G.; Ms, P.J.G.; Ms, J.A.W.; Srivastava, D.; ScD, W.M.L.; Neglia, J.; Sklar, C.A.; Kaste, S.C.; Hudson, M.M.; et al. The cyclophosphamide equivalent dose as an approach for quantifying alkylating agent exposure: A report from the Childhood Cancer Survivor Study. Pediatr. Blood Cancer 2014, 61, 53–67. [Google Scholar] [CrossRef] [Green Version]
- Cubukcu, C.E.; Sevinir, B.; Ercan, I. Disturbed dental development of permanent teeth in children with solid tumors and lymphomas. Pediatr. Blood Cancer 2012, 58, 80–84. [Google Scholar] [CrossRef]
- Apajalahti, S.; Hölttä, P.; Turtola, L.; Pirinen, S. Prevalence of short-root anomaly in healthy young adults. Acta Odontol. Scand. 2002, 60, 56–59. [Google Scholar] [CrossRef]
- Polder, B.J.; Hof, M.A.V.; Van Der Linden, F.P.G.M.; Kuijpers-Jagtman, A.M. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent. Oral Epidemiol. 2004, 32, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Ooshima, T.; Ishida, R.; Mishima, K.; Sobue, S. The prevalence of developmental anomalies of teeth and their association with tooth size in the primary and permanent dentitions of 1650 Japanese children. Int. J. Paediatr. Dent. 2009, 6, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, C.M.; Corrêa, F.N.P.; Lopes, N.N.F.; Fava, M.; Filho, V.O. Dental anomalies in children submitted to antineoplastic therapy. Clinics 2014, 69, 433–437. [Google Scholar] [CrossRef]
- Minicucci, E.M.; Lopes, L.F.; Crocci, A.J. Dental abnormalities in children after chemotherapy treatment for acute lymphoid leukemia. Leuk. Res. 2003, 27, 45–50. [Google Scholar] [CrossRef]
- Dahllöf, G.; Jönsson, A.; Ulmner, M.; Huggare, J. Orthodontic treatment in long-term survivors after pediatric bone marrow transplantation. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 459–465. [Google Scholar] [CrossRef]
- Roscoe, M.G.; Meira, J.; Cattaneo, P.M. Association of orthodontic force system and root resorption: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 610–626. [Google Scholar] [CrossRef]
- Pajari, U.; Lanning, M. Developmental defects of teeth in survivors of childhood ALL are related to the therapy and age at diagnosis. Med Pediatr. Oncol. 1995, 24, 310–314. [Google Scholar] [CrossRef]
- Koch, G.; Thesleff, I.; Kreiborg, S. Tooth Development and Disturbances in Number and Shape of Teeth. In Pediatric Dentistry—A Clinical Approach; Koch, G., Poulsen, S., Eds.; Wiley: Oxford, UK, 2009; pp. 183–196. [Google Scholar]
- Koch, G.; Kreiborg, S.; Andreasen, J.O. Eruption and Shedding of Teeth. In Pediatric Dentistry—A Clinical Approach, 3rd ed.; Wiley: Oxford, UK, 2016; pp. 40–54. [Google Scholar]
- Németh, O. Dental and Craniofacial Effects on Childhood Cancer Survivors. In Pediatric Cancer Survivors; Wonders, K., Stout, B., Eds.; IntechOpen: Rijeka, Croatia, 2017. [Google Scholar]
- Hölttä, P.; Alaluusua, S.; Saarinen-Pihkala, U.M.; Wolf, J.; Nyström, M.; Hovi, L. Long-term adverse effects on dentition in children with poor-risk neuroblastoma treated with high-dose chemotherapy and autologous stem cell transplantation with or without total body irradiation. Bone Marrow Transplant. 2002, 29, 121–127. [Google Scholar] [CrossRef]
- Hölttä, P.; Alaluusua, S.; Saarinen-Pihkala, U.M.; Peltola, J.; Hovi, L. Agenesis and microdontia of permanent teeth as late adverse effects after stem cell transplantation in young children. Cancer 2004, 103, 181–190. [Google Scholar] [CrossRef]
- Maciel, J.C.C.; de Castro, C.G.; Brunetto, A.L.; Di Leone, L.P.; da Silveira, H.E.D. Oral health and dental anomalies in patients treated for leukemia in childhood and adolescence. Pediatr. Blood Cancer 2009, 53, 361–365. [Google Scholar] [CrossRef]
- Duggal, M. Root surface areas in long-term survivors of childhood cancer. Oral Oncol. 2003, 39, 178–183. [Google Scholar] [CrossRef]
- Hsieh, S.G.-S.; Hibbert, S.; Shaw, P.; Ahern, V.; Arora, M. Association of cyclophosphamide use with dental developmental defects and salivary gland dysfunction in recipients of childhood antineoplastic therapy. Cancer 2011, 117, 2219–2227. [Google Scholar] [CrossRef]
- Teepen, J.C.; Van Leeuwen, F.E.; Tissing, W.J.; Broeder, E.V.D.-D.; Heuvel-Eibrink, M.M.V.D.; Van Der Pal, H.J.; Loonen, J.; Bresters, D.; Versluys, B.; Neggers, S.J.C.M.M.; et al. Long-Term Risk of Subsequent Malignant Neoplasms after Treatment of Childhood Cancer in the DCOG LATER Study Cohort: Role of Chemotherapy. J. Clin. Oncol. 2017, 35, 2288–2298. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Total n = 154 (100%) | H&N RT a n = 47 (30.5%) | No H&N RT n = 107 (69.5%) | p | |
|---|---|---|---|---|
| Gender | ||||
| Male | 75 (48.7) | 27 (57.4) | 48 (44.9) | 0.165 * |
| Female | 79 (51.3) | 20 (42.6) | 59 (55.1) | |
| Age at enrollment (years) | 32.4 (16.8–56.6) | 38.4 (21.1–56.6) | 30.3 (16.8–51.6) | 0.000 ** |
| Age at cancer diagnosis (years) | 5.2 (0.3–16.1) | 7.5 (1.3–14.1) | 4.0 (0.3–16.1) | 0.002 ** |
| 0–2.99 (youngest) | 46 (29.9) | 6 (12.8) | 40 (37.4) | |
| 3–4.99 (middlest) | 29 (18.8) | 7 (14.9) | 22 (20.6) | |
| >5 (oldest) | 79 (51.3) | 34 (72.3) | 45 (42.1) | |
| Time since diagnosis (years) b | 25.2 (15.9–48.8) | 31.0 (16.5–43.8) | 24.4 (15.9–48.8) | 0.000 ** |
| 0 < 20 | 30 (19.5) | 5 (10.6) | 25 (23.4) | |
| 20 < 30 | 78 (50.6) | 16 (34.0) | 62 (57.9) | |
| ≥30 | 46 (29.9) | 26 (55.3) | 20 (18.7) | |
| Diagnosis | ||||
| Hematological malignancy | 111 (72.1) | 36 (76.6) | 75 (70.1) | 0.442 * |
| Brain tumor | 7 (4.5) | 7 (14.9) | 0 (0.0) | 0.000 * |
| Solid tumor | 36 (23.4) | 4 (8.5) | 32 (29.9) | 0.004 * |
| Type of treatment | ||||
| H&N RT | 47 (100) | |||
| Head/cranium | 26 (55.3) | |||
| Brain | 21 (44.7) | |||
| Face | 5 (10.6) | |||
| Neck c | 5 (10.6) | |||
| TBI (HSCT) d | 16 (34.0) | |||
| Chemotherapy | 149 (96.8) | 42 (89.4) | 107 (100.0) | |
| Alkylating agents e | 101 (65.6) | 33 (70.2) | 68 (63.6) | 0.466 * |
| Vinca alkaloids f | 129 (83.8) | 34 (72.3) | 95 (88.8) | 0.017 * |
| Chemotherapy only | 58 (54.2) | |||
| Chemotherapy and RT but no H&N | 12 (11.2) | |||
| Chemotherapy and HSCT without RT g | 8 (7.5) | |||
| Chemotherapy and surgery without RT | 29 (27.1) |
| Response (%) a | Total n(%) b | H&N RT | No H&N RT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–3 years, n | 3–5 years, n | > 5 years, n | Total, n(%) b | 0–3 years, n | 3–5 years, n | > 5 years, n | Total, n(%) b | pe | ||||
| Oral health | ||||||||||||
| Poor oral hygiene | 96.1 | 7 (4.7) | 0 | 1 | 1 | 2 (4.4) | 4 | 1 | 0 | 5 (4.9) | 1.000 | |
| Moderate oral hygiene | 96.1 | 48 (32.4) | 1 | 1 | 14 | 16 (35.6) | 11 | 6 | 15 | 32 (31.1) | 0.706 | |
| Good oral hygiene | 96.1 | 93 (62.8) | 5 | 4 | 18 | 27 (60.0) | 25 | 13 | 28 | 66 (64.1) | 0.721 | |
| Increased caries susceptibility | 92.2 | 29 (20.4) | 0 | 0 | 11 | 11 (26.2) | 7 | 1 | 10 | 18 (18.0) | 0.361 | |
| High susceptibility to developing periodontal problems | 90.9 | 15 (10.7) | 0 | 0 | 6 | 6 (14.6) | 4 | 2 | 3 | 9 (9.1) | 0.373 | |
| Oral health problems | ||||||||||||
| Trismus | 88.3 | 2 (1.5) | 0 | 0 | 0 | 0 (0) | 2 | 0 | 0 | 2 (2.1) | 1.000 | |
| TMD | 85.7 | 6 (4.5) | 0 | 0 | 1 | 1 (2.5) | 1 | 1 | 3 | 5 (5.4) | 0.667 | |
| Xerostomia | 80.5 | 5 (4.0) | 0 | 0 | 2 | 2 (5.4) | 0 | 0 | 3 | 3 (3.4) | 0.634 | |
| Hyposalivation | 83.1 | 6 (4.7) | 0 | 0 | 2 | 2 (5.1) | 1 | 0 | 3 | 4 (4.5) | 1.000 | |
| Complaints of altered taste | 72.7 | 2 (1.8) | 0 | 0 | 0 | 0 (0) | 0 | 1 | 1 | 2 (2.5) | 1.000 | |
| Fungal infection | 82.5 | 1 (0.8) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 1 | 1 (1.1) | 1.000 | |
| Generalized severe tooth wear | 92.2 | 2 (1.4) | 0 | 0 | 1 | 1 (2.2) | 0 | 1 | 0 | 1 (1.0) | 0.535 | |
| Leukoplakia | 91.6 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | - | |
| Squamous-cell carcinoma | 90.3 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | - | |
| Other abnormalities | 87.7 | 17 (12.6) | 1 | 3 | 4 | 8 (18.6) | 3 | 1 | 5 | 9 (9.8) | 0.170 | |
| Orthodontic | ||||||||||||
| Craniofacial growth disorders | 84.4 | 5 (3.8) | 0 | 0 | 2 | 2 (4.8) | 1 | 0 | 2 | 3 (3.4) | 0.658 | |
| Malocclusion | 86.4 | 17 (12.8) | 0 | 1 | 4 | 5 (11.6) | 5 | 0 | 7 | 12 (13.3) | 1.000 | |
| History of OT | 66.9 | 59 (57.3) | 2 | 3 | 5 | 10 (37.0) | 23 | 13 | 13 | 49 (64.5) | 0.023 | |
| Precautions in OT | 66.1 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | - | |
| Problems in OT | 62.7 | 6 (16.2) | 0 | 0 | 2 | 2 (28.6) | 1 | 0 | 3 | 4 (13.3) | 0.315 | |
| Dental developmental disorder | ||||||||||||
| Agenesis c | 95.5 | 21 (14.3) | 1 | 0 | 3 | 4 (8.9) | 11 | 3 | 3 | 17 (16.7) | 0.307 | |
| Microdontia | 95.5 | 20 (13.6) | 1 | 1 | 3 | 5 (11.1) | 12 | 2 | 1 | 15 (14.7) | 0.794 | |
| Peg-shaped teeth | 95.5 | 5 (3.4) | 0 | 0 | 0 | 0 (0) | 5 | 0 | 0 | 5 (4.9) | 0.324 | |
| Hypomineralization | 94.8 | 9 (6.2) | 0 | 0 | 3 | 3 (6.7) | 4 | 0 | 2 | 6 (5.9) | 1.000 | |
| Taurodontism | 95.5 | 3 (2.0) | 0 | 0 | 1 | 1 (2.2) | 0 | 1 | 1 | 2 (2.0) | 1.000 | |
| Short-root anomaly | 93.5 | 21 (14.6) | 1 | 3 | 6 | 10 (23.3) | 4 | 2 | 5 | 11 (10.9) | 0.071 | |
| Persisting deciduous teeth | 94.8 | 7 (4.8) | 1 | 0 | 0 | 1 (2.2) | 4 | 2 | 0 | 6 (5.9) | 0.438 | |
| Number of dental developmental disorders d | 95.5 | |||||||||||
| 0 | 94 (63.9) | 3 | 3 | 23 | 29 (64.4) | 17 | 14 | 34 | 65 (63.7) | |||
| ≥ 1 | 53 (36.1) | 2 | 3 | 11 | 16 (35.6) | 21 | 8 | 8 | 37 (36.3) | 1.000 | ||
| Age at diagnosis a | |||||
|---|---|---|---|---|---|
| 0–3 years b | 3–5 years b | > 5 years b | Total b | p c | |
| Agenesis | 12 (27.9) | 3 (10.7) | 6 (7.9) | 21 (14.3) | 0.013 |
| Microdontia | 13 (30.2) | 3 (10.7) | 4 (5.3) | 20 (13.6) | 0.001 |
| Peg-shaped teeth | 5 (11.6) | 0 (0.0) | 0 (0.0) | 5 (3.4) | 0.004 |
| Hypomineralization | 4 (9.3) | 0 (0.0) | 5 (6.6) | 9 (6.2) | 0.272 |
| Taurodontism | 0 (0.0) | 1 (3.6) | 2 (2.6) | 3 (2.0) | 0.587 |
| Short-root anomaly | 5 (11.6) | 5 (18.5) | 11 (14.9) | 21 (14.6) | 0.736 |
| Persisting deciduous teeth | 5 (11.9) | 2 (7.1) | 0 (0.0) | 7 (4.8) | 0.006 |
| ≥1 DDD | 23 (53.5) | 11 (39.3) | 19 (25.0) | 53 (36.1) | 0.008 |
| Variable | Number of Survivors § | ≥1 DDD, n | Relative Risk | 95% CI | p |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 72 | 26 | 1.0 (ref) | ||
| Female | 73 | 27 | 1.03 | 0.67 to 1.58 | 0.896 |
| Age at diagnosis | |||||
| 0 < 3 years | 42 | 23 | 1.0 (ref) | ||
| 3 < 5 years | 28 | 11 | 0.79 | 0.45 to 1.38 | 0.398 |
| >5 years | 75 | 19 | 0.46 | 0.27 to 0.78 | 0.004 |
| Type of treatment | |||||
| No H&N RT | 101 | 37 | 1.0 (ref) | ||
| H&N RT | 44 | 16 | 1.15 | 0.72 to 1.83 | 0.561 |
| Chemotherapy | |||||
| No vinca alkaloids | 25 | 12 | 1.0 (ref) | ||
| Vinca alkaloids | 120 | 41 | 0.67 | 0.41 to 1.09 | 0.107 |
| No Epipodophyllotoxins | 108 | 31 | 1.0 (ref) | ||
| Epipodophyllotoxins | 37 | 22 | 1.42 | 0.91 to 2.22 | 0.122 |
| CED, mg/m2 * | |||||
| No alkylating agents | 52 | 12 | 1.0 (ref) | ||
| <4000 | 42 | 13 | 1.46 | 0.78 to 2.73 | 0.237 |
| 4000–9999 | 31 | 15 | 1.89 | 1.03 to 3.47 | 0.040 |
| ≥10,000 | 20 | 13 | 2.61 | 1.39 to 4.91 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stolze, J.; Vlaanderen, K.C.E.; Holtbach, F.C.E.D.; Teepen, J.C.; Kremer, L.C.M.; Loonen, J.J.; van Dulmen-den Broeder, E.; Heuvel-Eibrink, M.M.v.d.; Pal, H.J.H.v.d.; Versluys, B.; et al. Long-Term Effects of Childhood Cancer Treatment on Dentition and Oral Health: A Dentist Survey Study from the DCCSS LATER 2 Study. Cancers 2021, 13, 5264. https://doi.org/10.3390/cancers13215264
Stolze J, Vlaanderen KCE, Holtbach FCED, Teepen JC, Kremer LCM, Loonen JJ, van Dulmen-den Broeder E, Heuvel-Eibrink MMvd, Pal HJHvd, Versluys B, et al. Long-Term Effects of Childhood Cancer Treatment on Dentition and Oral Health: A Dentist Survey Study from the DCCSS LATER 2 Study. Cancers. 2021; 13(21):5264. https://doi.org/10.3390/cancers13215264
Chicago/Turabian StyleStolze, Juliette, Kim C. E. Vlaanderen, Frederique C. E. D. Holtbach, Jop C. Teepen, Leontien C. M. Kremer, Jacqueline J. Loonen, Eline van Dulmen-den Broeder, Marry M. van den Heuvel-Eibrink, Helena J. H. van der Pal, Birgitta Versluys, and et al. 2021. "Long-Term Effects of Childhood Cancer Treatment on Dentition and Oral Health: A Dentist Survey Study from the DCCSS LATER 2 Study" Cancers 13, no. 21: 5264. https://doi.org/10.3390/cancers13215264
APA StyleStolze, J., Vlaanderen, K. C. E., Holtbach, F. C. E. D., Teepen, J. C., Kremer, L. C. M., Loonen, J. J., van Dulmen-den Broeder, E., Heuvel-Eibrink, M. M. v. d., Pal, H. J. H. v. d., Versluys, B., van der Heiden-van der Loo, M., Louwerens, M., Raber-Durlacher, J. E., Bresters, D., & Brand, H. S. (2021). Long-Term Effects of Childhood Cancer Treatment on Dentition and Oral Health: A Dentist Survey Study from the DCCSS LATER 2 Study. Cancers, 13(21), 5264. https://doi.org/10.3390/cancers13215264