
Pretreatment Albumin-to-Alkaline Phosphatase Ratio Is a Prognostic Marker in Lung Cancer Patients: A Registry-Based Study of 7077 Lung Cancer Patients


Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patients
2.2. Patient Characteristics and AAPR Level in Patients with NSCLC
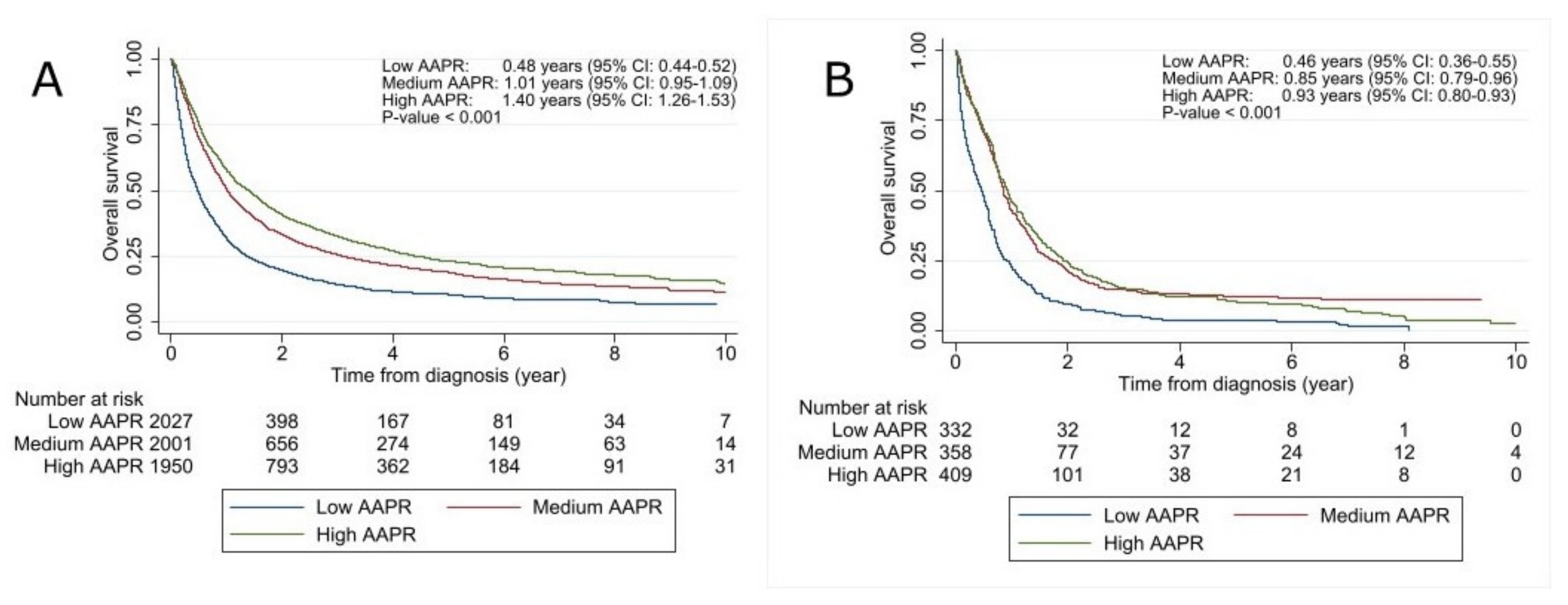
2.3. Survival According to AAPR Level in Patients with NSCLC
2.4. Patient Characteristics and AAPR Level in Patients with SCLC
2.5. Survival According to AAPR in Patients with SCLC
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. The Albumin-to-Alkaline Phosphatase Ratio
4.3. Ethics
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Fanali, G.; di Masi, A.; Trezza, V.; Marino, M.; Fasano, M.; Ascenzi, P. Human serum albumin: From bench to bedside. Mol. Asp. Med. 2012, 33, 209–290. [Google Scholar] [CrossRef] [PubMed]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef]
- Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Hypoalbuminemia: Pathogenesis and Clinical Significance. J. Parenter. Enter. Nutr. 2019, 43, 181–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Hung, H.A.-O.; Chen, J.S.; Chien, Y.; Tang, R.; Hsieh, P.S.; Wen, S.; You, Y.T.; You, J.F.; Chiang, J.M. Preoperative alkaline phosphatase elevation was associated with poor survival in colorectal cancer patients. Int. J. Colorectal Dis. 2017, 32, 1775–1778. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Lu, J.; Chang, W.; Chen, Y.; Li, X.; Li, D.; Xu, C.A.-O.; Yang, H.; Hung, H.A.-O.; Chen, J.S.; et al. Dynamic serum alkaline phosphatase is an indicator of overall survival in pancreatic cancer. BMC Cancer 2019, 19, 785. [Google Scholar] [CrossRef] [PubMed]
- Siller, A.F.; Whyte, M.P.; Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Alkaline Phosphatase: Discovery and Naming of Our Favorite Enzyme. J. Bone Miner. Res. 2018, 33, 362–364. [Google Scholar] [CrossRef] [Green Version]
- An, L.; Yin, W.T.; Sun, D.A.-O. Albumin-to-alkaline phosphatase ratio as a promising indicator of prognosis in human cancers: Is it possible? BMC Cancer 2021, 21, 247. [Google Scholar] [CrossRef] [PubMed]
- Tian, G.; Li, G.; Guan, L.; Yang, Y.; Li, N.; An, L.; Yin, W.T.; Sun, D.A.-O. Pretreatment albumin-to-alkaline phosphatase ratio as a prognostic indicator in solid cancers: A meta-analysis with trial sequential analysis. Int. J. Surg. 2020, 81, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, Y.; Zhao, Q.; Jiang, H.; Ni, J.; Cai, H. Albumin-to-alkaline phosphatase ratio: A novel prognostic index for patients with driver mutation-negative advanced non-small cell lung cancer. Clin. Respir. J. 2021, 15, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Chan, S.A.-O.; Mo, F.K.; Wong, G.L.; Wong, V.W.; Cheung, Y.S.; Chan, H.L.; Yeo, W.; Lai, P.B.; To, K.F. Albumin-to-alkaline phosphatase ratio: A novel prognostic index for hepatocellular carcinoma. Dis. Markers 2015, 2015, 564057. [Google Scholar] [CrossRef]
- Li, B.; Jiang, C.; Wang, R.; Zou, B.; Xie, P.; Li, W.; Sun, X.; Yu, J.; Wang, L. Prognostic Value of a Nomogram Based on the Dynamic Albumin-to-Alkaline Phosphatase Ratio for Patients with Extensive-Stage Small-Cell Lung Cancer. Onco Targets Ther. 2020, 13, 9043–9057. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Yu, H.; Li, W. Albumin-to-alkaline phosphatase ratio at diagnosis predicts survival in patients with metastatic non-small-cell lung cancer. Onco Targets Ther. 2019, 12, 5241–5249. [Google Scholar] [CrossRef] [Green Version]
- Li, S.J.; Lv, W.Y.; Du, H.; Li, Y.J.; Zhang, W.B.; Che, G.W.; Liu, L.X. Albumin-to-alkaline phosphatase ratio as a novel prognostic indicator for patients undergoing minimally invasive lung cancer surgery: Propensity score matching analysis using a prospective database. Int. J. Surg. 2019, 69, 32–42. [Google Scholar] [CrossRef]
- Li, X.; Li, B.; Zeng, H.; Wang, S.; Sun, X.; Yu, Y.; Wang, L.; Yu, J. Prognostic value of dynamic albumin-to-alkaline phosphatase ratio in limited stage small-cell lung cancer. Future Oncol. 2019, 15, 995–1006. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, H.; Yue, D.; Wei, W.; Chen, Y.; Zhao, X.; Zhu, J.; Zhang, B.; Zhang, Z.; Wang, C. The prognostic value of the preoperative albumin to alkaline phosphatase ratio in patients with non-small cell lung cancer after surgery. Thorac. Cancer 2019, 10, 1581–1589. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Jiang, W.; Wang, H.; Wei, N.; Yu, Q. Predictive value of pretreatment albumin-to-alkaline phosphatase ratio for overall survival for patients with advanced non-small cell lung cancer. Cancer Med. 2020, 9, 6268–6280. [Google Scholar] [CrossRef]
- Zhou, S.A.-O.; Wang, H.; Jiang, W.; Yu, Q.; Zeng, A. Prognostic Value of Pretreatment Albumin-to-Alkaline Phosphatase Ratio in Extensive-Disease Small-Cell Lung Cancer: A Retrospective Cohort Study. Cancer Manag. Res. 2020, 12, 2015–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.S.; Keam, B.; Heo, D.S.; Han, D.H.; Rhee, C.S.; Kim, J.H.; Jung, K.C.; Wu, H.G. The Prognostic Value of Albumin-to-Alkaline Phosphatase Ratio before Radical Radiotherapy in Patients with Non-metastatic Nasopharyngeal Carcinoma: A Propensity Score Matching Analysis. Cancer Res. Treat. 2019, 51, 1313–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, P.; Xie, N.; Ai, J.; Xu, H.; Xu, H.; Liu, L.; Yang, L.; Wei, Q. The prognostic significance of Albumin-to-Alkaline Phosphatase Ratio in upper tract urothelial carcinoma. Sci. Rep. 2018, 8, 12311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, A.; Chen, Y.; Chen, J.; Pan, Y.; Bao, L.; Gao, X. Prognostic value of the albumin-to-alkaline phosphatase ratio on urologic outcomes in patients with non-metastatic renal cell carcinoma following curative nephrectomy. J. Cancer 2019, 10, 5494–5503. [Google Scholar] [CrossRef]
- Kim, S.; McClave, S.A.; Martindale, R.G.; Miller, K.R.; Hurt, R.T. Hypoalbuminemia and Clinical Outcomes: What is the Mechanism behind the Relationship? Am. Surg. 2017, 83, 1220–1227. [Google Scholar] [CrossRef]
- Miura, K.; Hamanaka, K.; Koizumi, T.; Kitaguchi, Y.; Terada, Y.; Nakamura, D.; Kumeda, H.; Agatsuma, H.; Hyogotani, A.; Kawakami, S.; et al. Clinical significance of preoperative serum albumin level for prognosis in surgically resected patients with non-small cell lung cancer: Comparative study of normal lung, emphysema, and pulmonary fibrosis. Lung Cancer 2017, 111, 88–95. [Google Scholar] [CrossRef]
- Zhang, L.; Gong, Z. Clinical Characteristics and Prognostic Factors in Bone Metastases from Lung Cancer. Med. Sci. Monit. 2017, 23, 4087–4094. [Google Scholar] [CrossRef] [Green Version]
- Tanriverdi, O.; Avci, N.; Oktay, E.; Kalemci, S.; Pilanci, K.N.; Cokmert, S.; Menekse, S.; Kocar, M.; Sen, C.A.; Akman, T.; et al. Pretreatment Serum Albumin Level is an Independent Prognostic Factor in Patients with Stage IIIB Non-Small Cell Lung Cancer: A Study of the Turkish Descriptive Oncological Researches Group. Asian Pac. J. Cancer Prev. 2015, 16, 5971–5976. [Google Scholar] [CrossRef] [Green Version]
- Sandfeld-Paulsen, B.; Aggerholm-Pedersen, N.; Winther-Larsen, A. Hyponatremia in lung cancer: Incidence and prognostic value in a Danish population-based cohort study. Lung Cancer 2021, 153, 42–48. [Google Scholar] [CrossRef]
- Jakobsen, E.; Rasmussen, T.R. The Danish Lung Cancer Registry. Clin. Epidemiol. 2016, 8, 537–541. [Google Scholar] [CrossRef] [Green Version]
- Statistics Denmark. Available online: www.dst.dk/en (accessed on 11 August 2020).
- Patobank. 2021. Available online: www.patobank.dk (accessed on 29 May 2018).
- Arendt, J.F.H.; Hansen, A.T.; Ladefoged, S.A.; Sørensen, H.T.; Pedersen, L.; Adelborg, K. Existing Data Sources in Clinical Epidemiology: Laboratory Information System Databases in Denmark. Clin. Epidemiol. 2020, 12, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Pedersen, L.; Sørensen, H.T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All Patients | Low AAPR a | Medium AAPR a | High AAPR a | p-Value b |
|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | ||
| Total number of patients | 5978 | 2027 | 2001 | 1950 | |
| Age, years | 0.263 | ||||
| Median age (5–95% percentiles) | 70 (52–84) | 70 (52–84) | 70 (52–84) | 70 (52–84) | |
| Sex | <0.001 | ||||
| Female | 2874 (48) | 931 (46) | 924 (46) | 1019 (52) | |
| Male | 3104 (52) | 1096 (54) | 1077 (54) | 931 (48) | |
| Histology | 0.005 | ||||
| Adenocarcinoma | 3197 (53) | 1064 (52) | 1055 (53) | 1078 (55) | |
| Squamous cell | 1424 (24) | 472 (23) | 528 (26) | 424 (22) | |
| Other | 1067 (18) | 395 (19) | 318 (16) | 354 (18) | |
| Unknown | 290 (5) | 96 (5) | 100 (5) | 94 (5) | |
| Stage | <0.001 | ||||
| I | 1067 (18) | 226 (11) | 351 (18) | 490 (25) | |
| II | 512 (9) | 160 (8) | 171 (9) | 181 (9) | |
| III | 1165 (19) | 341 (17) | 443 (22) | 381 (20) | |
| IV | 2775 (46) | 1136 (56) | 901 (45) | 738 (38) | |
| Unknown | 459 (8) | 164 (8) | 135 (7) | 160 (8) | |
| Performance status, ECOG | <0.001 | ||||
| 0 | 2013 (34) | 522 (26) | 755 (38) | 736 (38) | |
| 1 | 1906 (32) | 632 (31) | 639 (32) | 635 (33) | |
| 2 | 732 (12) | 297 (15) | 232 (12) | 203 (10) | |
| 3 + 4 | 704 (12) | 351 (17) | 182 (9) | 171 (9) | |
| Unknown | 623 (10) | 225 (11) | 193 (9) | 205 (11) | |
| Smoking status | 0.775 | ||||
| Never | 281 (5) | 91 (4) | 92 (5) | 98 (5) | |
| Current or former | 4437 (74) | 1456 (72) | 1521 (76) | 1460 (75) | |
| Unknown | 1260 (21) | 480 (24) | 388 (19) | 392 (20) |
| Characteristics | HR | Adjusted HR |
|---|---|---|
| (95% CI) | (95% CI) | |
| AAPR | ||
| Low | 1 | 1 |
| Medium | 0.63 (0.59–0.68) | 0.73 (0.68–0.79) |
| High | 0.53 (0.50–0.57) | 0.68 (0.62–0.73) |
| Sex | ||
| Female | 1 | 1 |
| Male | 1.18 (1.13–1.26) | 1.20 (1.12–1.28) |
| Histology | ||
| Adenocarcinoma | 1 | 1 |
| Squamous cell | 1.49 (1.37–1.63) | 1.20 (1.09–1.34) |
| Other | 1.04 (0.97–1.11) | 0.93 (0.86–1.01) |
| Stage | ||
| I | 1 | 1 |
| II | 1.39 (1.21–1.659) | 1.31 (1.13–1.53) |
| III | 2.86 (2.57–3.18) | 2.96 (2.63–3.32) |
| IV | 5.86 (5.32–6.44) | 5.95 (5.34–6.62) |
| Age | 1.02 (1.02–1.02) | 1.02 (1.01–1.02) |
| Smoking | ||
| Never | 1 | 1 |
| Current or former | 1.31 (1.14–1.51) | 1.52 (1.32–1.75) |
| Performance status, ECOG | ||
| 0 | 1 | 1 |
| 1 | 1.71 (1.60–1.84) | 1.42 (1.32–1.53) |
| 2 | 2.67 (2.44–2.93) | 2.14 (1.94–2.36) |
| 3 | 4.44 (4.04–4.87) | 3.79 (3.39–4.23) |
| Model NSCLC | AIC a | C-Index b |
|---|---|---|
| AAPR + stage + histology + age + sex + PS + smoking | 57746 | 0.7545 |
| Stage + histology +age + sex + PS + smoking | 57877 | 0.7480 |
| Model SCLC | ||
| AAPR + stage + age + sex + PS + smoking | 9063 | 0.7301 |
| Stage + age + sex + PS + smoking | 9097 | 0.7227 |
| Characteristics | All Patients | Low AAPR a | Medium AAPR a | High AAPR a | p-Value b |
|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | ||
| Total number of patients | 1099 | 332 | 358 | 409 | |
| Age, years | 0.568 | ||||
| Median age (5–95% percentiles) | 69 (52–82) | 69 (51–83) | 69 (52–82) | 70 (53–83) | |
| Sex | <0.001 | ||||
| Female | 551 (50) | 137 (41) | 189(53) | 225 (55) | |
| Male | 548 (50) | 195 (59) | 169 (47) | 184 (45) | |
| Stage | <0.001 | ||||
| I | 51 (5) | 10 (3) | 22 (6) | 19 (5) | |
| II | 28 (2) | 2 (1) | 10 (3) | 16 (4) | |
| III | 294 (27) | 53 (16) | 113 (31) | 128 (31) | |
| IV | 644 (58) | 231 (70) | 190 (53) | 223 (54) | |
| Unknown | 82 (8) | 36 (11) | 23 (6) | 23 (6) | |
| Performance status, ECOG | <0.001 | ||||
| 0 | 296 (27) | 67 (20) | 108 (30) | 121 (29) | |
| 1 | 381 (35) | 96 (29) | 134 (38) | 151 (37) | |
| 2 | 176 (16) | 64 (19) | 52 (15) | 60 (15) | |
| 3 + 4 | 148 (13) | 63 (19) | 39 (11) | 46 (11) | |
| Unknown | 98 (9) | 42 (13) | 25 (6) | 31 (8) | |
| Smoking status | 0.106 | ||||
| Never | 9 (1) | 0 (0) | 3 (1) | 6 (1) | |
| Current or former | 861 (79) | 247 (74) | 287 (81) | 327 (80) | |
| Unknown | 229 (20) | 85 (26) | 66 (18) | 78 (19) |
| Characteristics | HR | Adjusted HR |
|---|---|---|
| (95% CI) | (95% CI) | |
| AAPR | ||
| Low | 1 | 1 |
| Medium | 0.54 (0.46–0.63) | 0.62 (0.52–0.74) |
| High | 0.54 (0.47–0.63) | 0.59 (0.50–0.70) |
| Sex | ||
| Female | 1 | 1 |
| Male | 1.12 (1.00–1.27) | 1.13 (0.98–1.30) |
| Stage | ||
| I | 1 | 1 |
| II | 1.05 (0.55–2.00) | 1.11 (0.55–2.24) |
| III | 3.09 (2.07–4.60) | 3.33 (2.15–5.16) |
| IV | 6.47 (4.37–9.59) | 6.65 (4.31–10.27) |
| Age | 1.04 (1.03–1.04) | 1.02 (1.01–1.03) |
| Smoking | ||
| Never | 1 | 1 |
| Current or former | 0.90 (0.47–1.74) | 0.68 (0.35–1.32) |
| Performance status, ECOG | ||
| 0 | 1 | 1 |
| 1 | 1.51 (1.29–1.78) | 1.28 (1.07–1.53) |
| 2 | 2.88 (2.37–3.51) | 2.29 (1.83–2.85) |
| 3 | 4.15 (3.37–5.11) | 4.33 (3.39–5.54) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandfeld-Paulsen, B.; Aggerholm-Pedersen, N.; Winther-Larsen, A. Pretreatment Albumin-to-Alkaline Phosphatase Ratio Is a Prognostic Marker in Lung Cancer Patients: A Registry-Based Study of 7077 Lung Cancer Patients. Cancers 2021, 13, 6133. https://doi.org/10.3390/cancers13236133
Sandfeld-Paulsen B, Aggerholm-Pedersen N, Winther-Larsen A. Pretreatment Albumin-to-Alkaline Phosphatase Ratio Is a Prognostic Marker in Lung Cancer Patients: A Registry-Based Study of 7077 Lung Cancer Patients. Cancers. 2021; 13(23):6133. https://doi.org/10.3390/cancers13236133
Chicago/Turabian StyleSandfeld-Paulsen, Birgitte, Ninna Aggerholm-Pedersen, and Anne Winther-Larsen. 2021. "Pretreatment Albumin-to-Alkaline Phosphatase Ratio Is a Prognostic Marker in Lung Cancer Patients: A Registry-Based Study of 7077 Lung Cancer Patients" Cancers 13, no. 23: 6133. https://doi.org/10.3390/cancers13236133
APA StyleSandfeld-Paulsen, B., Aggerholm-Pedersen, N., & Winther-Larsen, A. (2021). Pretreatment Albumin-to-Alkaline Phosphatase Ratio Is a Prognostic Marker in Lung Cancer Patients: A Registry-Based Study of 7077 Lung Cancer Patients. Cancers, 13(23), 6133. https://doi.org/10.3390/cancers13236133