
Beneficial Prognostic Effects of Aspirin in Patients Receiving Sorafenib for Hepatocellular Carcinoma: A Tale of Multiple Confounders

 ,
,  ,
,  , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Baseline Evaluation
2.3. Definition of Aspirin-Treated Patients
2.4. Management of Sorafenib
2.5. Ethics
2.6. Statistical Analysis
3. Results
3.1. Study Population
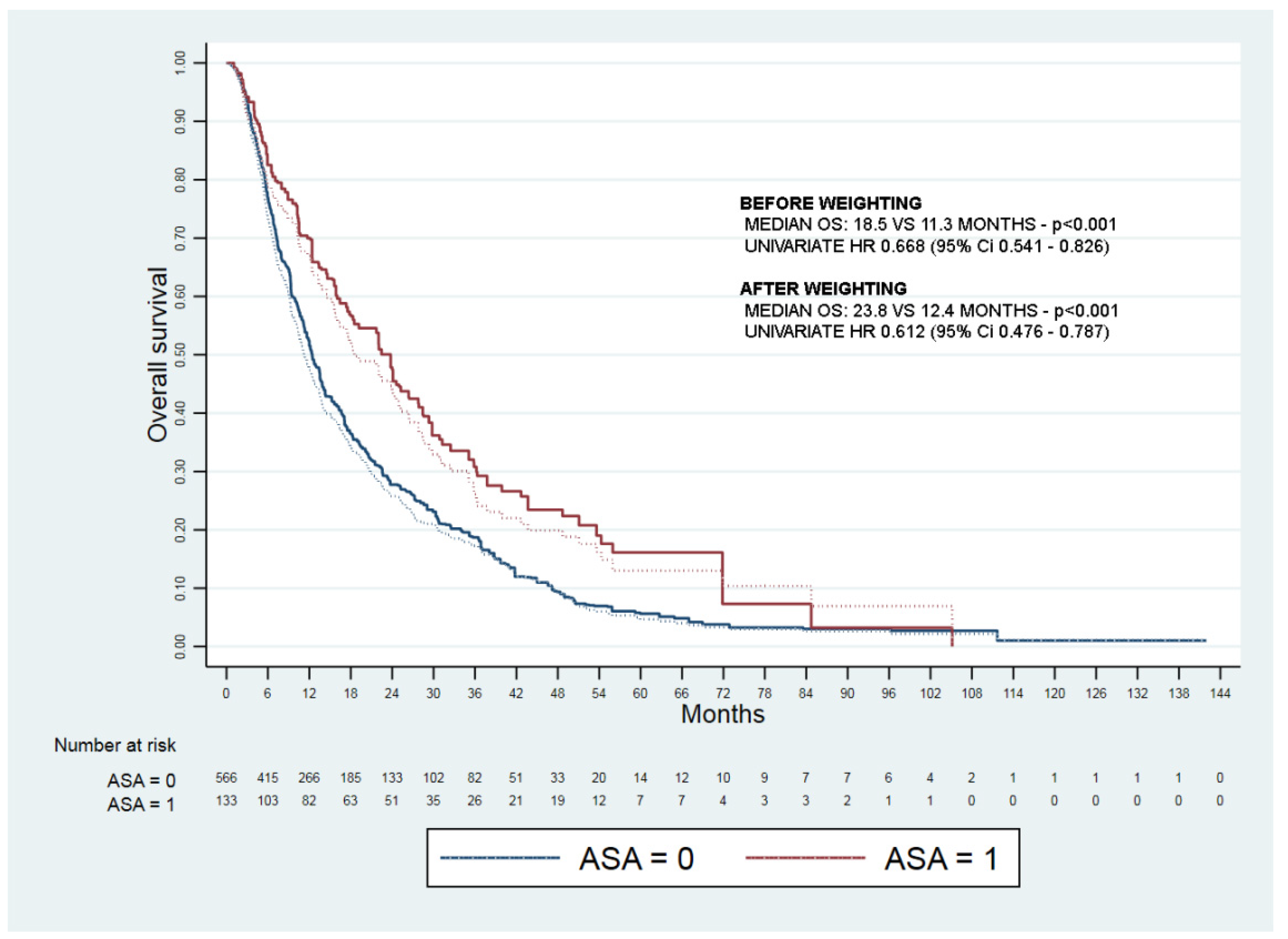
3.2. Unadjusted Analysis
3.3. Propensity Score Analysis
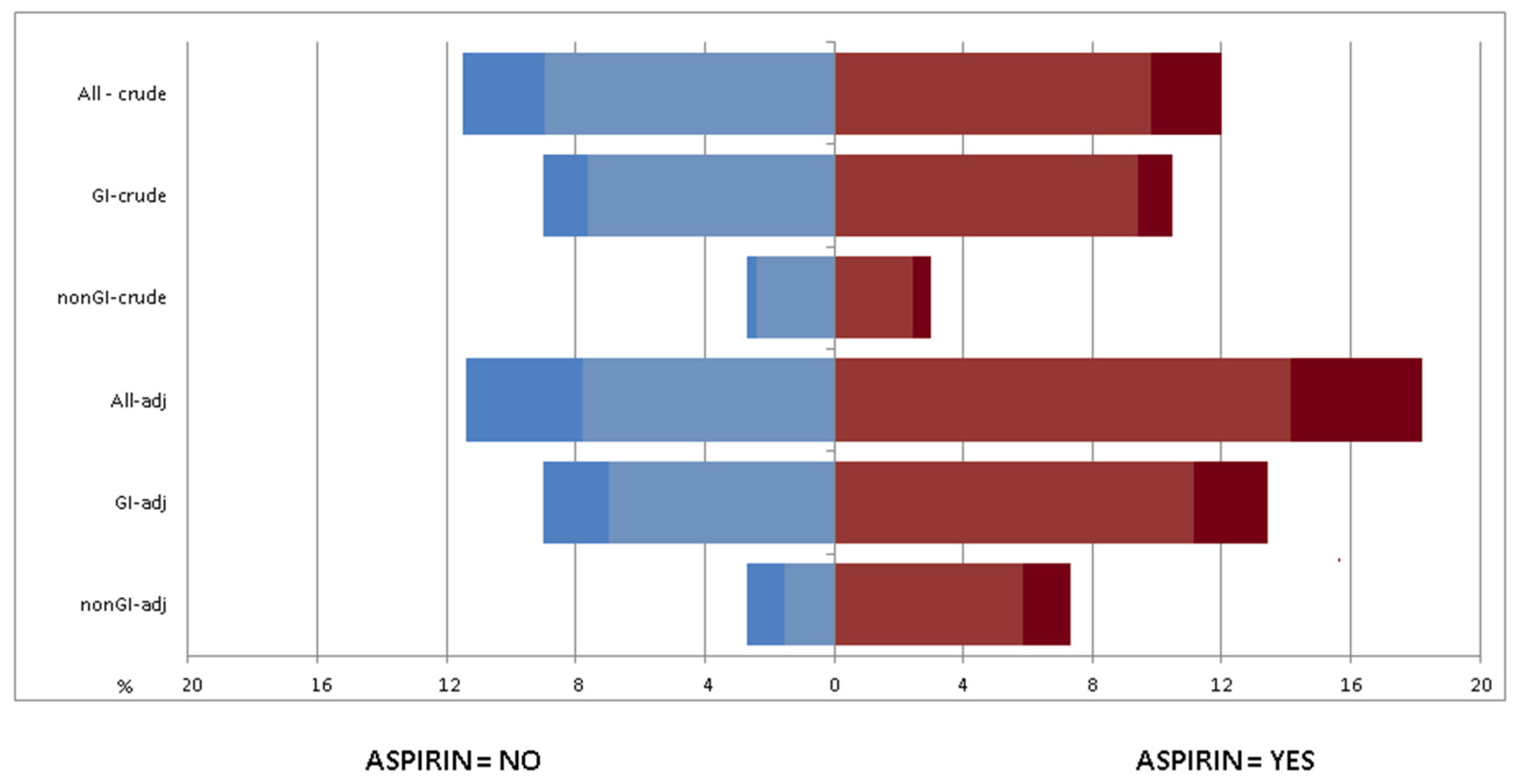
3.4. Adjusted Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Choi, J.; Ghoz, H.M.; Peeraphatdit, T.; Baichoo, E.; Addissie, B.D.; Harmsen, W.S.; Therneau, T.M.; Olson, J.E.; Chaiteerakij, R.; Roberts, L.R. Aspirin Use and the Risk of Cholangiocarcinoma. Hepatol. Baltim. Md. 2016, 64, 785–796. [Google Scholar] [CrossRef] [Green Version]
- Simon, T.G.; Duberg, A.-S.; Aleman, S.; Chung, R.T.; Chan, A.T.; Ludvigsson, J.F. Association of Aspirin with Hepatocellular Carcinoma and Liver-Related Mortality. N. Engl. J. Med. 2020, 382, 1018–1028. [Google Scholar] [CrossRef] [PubMed]
- Casadei-Gardini, A.; Rovesti, G.; Dadduzio, V.; Vivaldi, C.; Lai, E.; Lonardi, S.; Fornaro, L.; Pretta, A.; Zagonel, V.; Bernardini, L.; et al. Impact of Aspirin on Clinical Outcome in Advanced HCC Patients Receiving Sorafenib and Regorafenib. HPB 2021, 23, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, X. Impact of Statin Use on the Risk and Prognosis of Hepatocellular Carcinoma: A Meta-Analysis. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Casadei Gardini, A.; Faloppi, L.; De Matteis, S.; Foschi, F.G.; Silvestris, N.; Tovoli, F.; Palmieri, V.; Marisi, G.; Brunetti, O.; Vespasiani-Gentilucci, U.; et al. Metformin and Insulin Impact on Clinical Outcome in Patients with Advanced Hepatocellular Carcinoma Receiving Sorafenib: Validation Study and Biological Rationale. Eur. J. Cancer 2017, 86, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Tovoli, F.; Dadduzio, V.; De Lorenzo, S.; Rimassa, L.; Masi, G.; Iavarone, M.; Marra, F.; Garajova, I.; Brizzi, M.P.; Daniele, B.; et al. Real-Life Clinical Data of Cabozantinib for Unresectable Hepatocellular Carcinoma. Liver Cancer 2021, 10, 370–379. [Google Scholar] [CrossRef]
- Tovoli, F.; Casadei-Gardini, A.; Benevento, F.; Piscaglia, F. Immunotherapy for Hepatocellular Carcinoma: A Review of Potential New Drugs Based on Ongoing Clinical Studies as of 2019. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2019, 51, 1067–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reig, M.; Torres, F.; Rodriguez-Lope, C.; Forner, A.; LLarch, N.; Rimola, J.; Darnell, A.; Ríos, J.; Ayuso, C.; Bruix, J. Early Dermatologic Adverse Events Predict Better Outcome in HCC Patients Treated with Sorafenib. J. Hepatol. 2014, 61, 318–324. [Google Scholar] [CrossRef]
- Liu, Y.; Ren, T.; Xu, X.; Jin, J. Association of Aspirin and Nonaspirin NSAIDs Therapy with the Incidence Risk of Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis on Cohort Studies. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. ECP 2021, 31, 35–43. [Google Scholar] [CrossRef]
- Tan, R.Z.H.; Lockart, I.; Abdel Shaheed, C.; Danta, M. Systematic Review with Meta-Analysis: The Effects of Non-Steroidal Anti-Inflammatory Drugs and Anti-Platelet Therapy on the Incidence and Recurrence of Hepatocellular Carcinoma. Aliment. Pharmacol. Ther. 2021, 54, 356–367. [Google Scholar] [CrossRef]
- Li, J.-H.; Wang, Y.; Xie, X.-Y.; Yin, X.; Zhang, L.; Chen, R.-X.; Ren, Z.-G. Aspirin in Combination with TACE in Treatment of Unresectable HCC: A Matched-Pairs Analysis. Am. J. Cancer Res. 2016, 6, 2109–2116. [Google Scholar]
- Hull, M.A.; Sprange, K.; Hepburn, T.; Tan, W.; Shafayat, A.; Rees, C.J.; Clifford, G.; Logan, R.F.; Loadman, P.M.; Williams, E.A.; et al. Eicosapentaenoic Acid and Aspirin, Alone and in Combination, for the Prevention of Colorectal Adenomas (SeAFOod Polyp Prevention Trial): A Multicentre, Randomised, Double-Blind, Placebo-Controlled, 2 ;× 2 Factorial Trial. Lancet Lond. Engl. 2018, 392, 2583–2594. [Google Scholar] [CrossRef] [Green Version]
- Elwood, P.C.; Morgan, G.; Galante, J.; Chia, J.W.K.; Dolwani, S.; Graziano, J.M.; Kelson, M.; Lanas, A.; Longley, M.; Phillips, C.J.; et al. Systematic Review and Meta-Analysis of Randomised Trials to Ascertain Fatal Gastrointestinal Bleeding Events Attributable to Preventive Low-Dose Aspirin: No Evidence of Increased Risk. PLoS. ONE 2016, 11, e0166166. [Google Scholar] [CrossRef] [Green Version]
- Qamar, A.A.; Grace, N.D.; Groszmann, R.J.; Garcia-Tsao, G.; Bosch, J.; Burroughs, A.K.; Ripoll, C.; Maurer, R.; Planas, R.; Escorsell, A.; et al. Incidence, Prevalence, and Clinical Significance of Abnormal Hematologic Indices in Compensated Cirrhosis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2009, 7, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Carr, B.I.; Pancoska, P.; Giannini, E.G.; Farinati, F.; Ciccarese, F.; Rapaccini, G.L.; Marco, M.D.; Benvegnù, L.; Zoli, M.; Borzio, F.; et al. Identification of Two Clinical Hepatocellular Carcinoma Patient Phenotypes from Results of Standard Screening Parameters. Semin. Oncol. 2014, 41, 406–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, B.I.; Guerra, V.; Giannini, E.G.; Farinati, F.; Ciccarese, F.; Rapaccini, G.L.; Di Marco, M.; Benvegnù, L.; Zoli, M.; Borzio, F.; et al. A Liver Index and Its Relationship to Indices of HCC Aggressiveness. J. Integr. Oncol. 2016, 5, 178. [Google Scholar] [CrossRef]
- Lai, Q.; Vitale, A.; Manzia, T.M.; Foschi, F.G.; Levi Sandri, G.B.; Gambato, M.; Melandro, F.; Russo, F.P.; Miele, L.; Viganò, L.; et al. Platelets and Hepatocellular Cancer: Bridging the Bench to the Clinics. Cancers 2019, 11, 1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.-F.; Zhong, M.-F.; Zhang, Y.-R.; Wang, H.; Zhao, H.-T.; Cheng, B.-B.; Ling, C.-Q. Prognostic Role of Platelet-to-Lymphocyte Ratio in Hepatocellular Carcinoma with Different BCLC Stages: A Systematic Review and Meta-Analysis. Gastroenterol. Res. Pract. 2018, 2018, 5670949. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic, N.; Rani, B.; Gerwins, P.; Heindryckx, F. Platelets as Key Factors in Hepatocellular Carcinoma. Cancers 2019, 11, 1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nischalke, H.D.; Klüners, A.; Nattermann, J.; Berg, T.; Strassburg, C.P.; Lutz, P. Hepatocellular Carcinoma Prevention by Aspirin: Are Platelets the Link? Hepatol. Commun. 2021, 5, 2151–2152. [Google Scholar] [CrossRef]
- Menter, D.G.; Tucker, S.C.; Kopetz, S.; Sood, A.K.; Crissman, J.D.; Honn, K.V. Platelets and Cancer: A Casual or Causal Relationship: Revisited. Cancer Metastasis Rev. 2014, 33, 231–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawasaki, T.; Murata, S.; Takahashi, K.; Nozaki, R.; Ohshiro, Y.; Ikeda, N.; Pak, S.; Myronovych, A.; Hisakura, K.; Fukunaga, K.; et al. Activation of Human Liver Sinusoidal Endothelial Cell by Human Platelets Induces Hepatocyte Proliferation. J. Hepatol. 2010, 53, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Soll, C.; Jang, J.H.; Riener, M.-O.; Moritz, W.; Wild, P.J.; Graf, R.; Clavien, P.-A. Serotonin Promotes Tumor Growth in Human Hepatocellular Cancer. Hepatol. Baltim. Md. 2010, 51, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Gay, L.J.; Felding-Habermann, B. Contribution of Platelets to Tumour Metastasis. Nat. Rev. Cancer 2011, 11, 123–134. [Google Scholar] [CrossRef]
- Carr, B.I.; Cavallini, A.; D’Alessandro, R.; Refolo, M.G.; Lippolis, C.; Mazzocca, A.; Messa, C. Platelet Extracts Induce Growth, Migration and Invasion in Human Hepatocellular Carcinoma in Vitro. BMC Cancer 2014, 14, 43. [Google Scholar] [CrossRef]
- D’Alessandro, R.; Refolo, M.G.; Lippolis, C.; Giannuzzi, G.; Carella, N.; Messa, C.; Cavallini, A.; Carr, B.I. Antagonism of Sorafenib and Regorafenib Actions by Platelet Factors in Hepatocellular Carcinoma Cell Lines. BMC Cancer 2014, 14, 351. [Google Scholar] [CrossRef] [Green Version]
- Prizment, A.E.; Staley, C.; Onyeaghala, G.C.; Vivek, S.; Thyagarajan, B.; Straka, R.J.; Demmer, R.T.; Knights, D.; Meyer, K.A.; Shaukat, A.; et al. Randomised Clinical Study: Oral Aspirin 325 Mg Daily vs Placebo Alters Gut Microbial Composition and Bacterial Taxa Associated with Colorectal Cancer Risk. Aliment. Pharmacol. Ther. 2020, 52, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C.; Rosner, B.; Speizer, F.E.; Hennekens, C.H. A Prospective Study of Aspirin Use and Primary Prevention of Cardiovascular Disease in Women. JAMA 1991, 266, 521–527. [Google Scholar] [CrossRef]
- Danta, M.; Tan, R.Z.H.; Lockart, I.; Abdel Shaheed, C. Editorial: Aspirin and NSAID for Chemoprevention of Hepatocellular Carcinoma—Ready for Their Use? Authors’ Reply. Aliment. Pharmacol. Ther. 2021, 54, 852–853. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients n = 699 | ASA Users n = 133 | Non-Users n = 566 | p |
|---|---|---|---|---|
| Age (yrs) | 68 (60–74) | 72 (67–79) | 68 (64–76) | 0.444 |
| Sex (male) | 596 (85.3) | 126 (93.3) | 470 (83.3) | 0.003 |
| Viral etiology | 503 (72.0) | 81 (60.0) | 422 (74.8) | 0.001 |
| Disease duration (months) | 14.3 | 12.7 | 14.7 | 0.215 |
| Previous HCC treatments | 518 (74.1) | 96 (72.1) | 422 (74.3) | 0.721 |
| Bilirubin (mg/dL) | 0.93 (0.68–1.40) | 0.92 (0.60–1.31) | 0.95 (0.62–1.30) | 0.884 |
| Albumin (g/dL) | 36 (33–39) | 37 (34–40) | 36 (32–39) | 0.482 |
| Platelets (103/mL) | 135 (95–186) | 156 (115–200) | 125 (92–182) | 0.001 |
| ALBI grade 1 | 131 (18.7) | 39 (28.9) | 92 (16.3) | 0.001 |
| Child-Pugh B | 41 (5.9) | 2 (1.5) | 39 (6.9) | 0.013 |
| Esophageal varices | 300 (42.9) | 28 (20.7) | 272 (48.2) | <0.001 |
| Metformin | 89 (12.7) | 19 (14.1) | 70 (12.4) | 0.569 |
| Insulin | 80 (11.4) | 16 (11.9) | 64 (11.3) | 0.881 |
| Statin | 45 (6.4) | 25 (18.5) | 20 (3.5) | <0.001 |
| AFP > 400 ng/mL | 217 (31.0) | 34 (25.2) | 183 (32.4) | 0.120 |
| ECOG-PS > 0 | 150 (21.5) | 28 (20.7) | 122 (21.6) | 0.907 |
| Tumor > 50% of liver volume or main trunk PVT | 29 (4.1) | 5 (3.7) | 24 (4.3) | 1.000 |
| Macrovascular invasion | 275 (39.3) | 43 (31.9) | 232 (41.1) | 0.050 |
| Extrahepatic spread | 220 (31.5) | 51 (37.8) | 169 (30.0) | 0.081 |
| BCLC-intermediate stage | 191 (27.3) | 39 (28.9) | 152 (27.0) | 0.668 |
| Variable | Aspirin Users | Non-Users | Standardized Difference |
|---|---|---|---|
| Age (yrs) | 67.0 | 67.0 | +0.3 |
| Sex (male) | 83 | 85 | −5.6 |
| Viral etiology | 73 | 71 | +4.4 |
| Esophageal varices | 47 | 43 | +8.0 |
| Platelets (×103/mmc) | 148.1 | 149.9 | −2.2 |
| ALBI grade 1 | 19 | 19 | +0.9 |
| Child-Pugh B | 7 | 6 | +4.3 |
| ECOG-PS > 0 | 21 | 21 | −0.8 |
| Tumor > 50% of liver volume or main trunk PVT | 3 | 4 | −6.4 |
| Macrovascular invasion | 38 | 39 | −2.0 |
| Extrahepatic spread | 37 | 33 | +8.8 |
| AFP > 400 ng/mL | 32 | 31 | +2.2 |
| Metformin | 12 | 14 | −5.7 |
| Insulin | 13 | 11 | +2.9 |
| Statin | 6 | 7 | −3.9 |
| Variable | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (yrs) | 1.006 | 0.997–1.070 | 0.197 | - | - | - |
| Sex (male) | 0.876 | 0.593–1.294 | 0.506 | - | - | - |
| Viral etiology | 1.195 | 0.959–1.490 | 0.112 | - | - | - |
| Platelets (103/mmc) | 1.001 | 1.000–1.002 | 0.062 | 1.002 | 1.001–1.003 | 0.001 |
| Aspirin | 0.612 | 0.476–0.787 | <0.001 | 0.685 | 0.529–0.888 | 0.004 |
| Metformin | 0.912 | 0.663–1.257 | 0.575 | - | - | - |
| Insulin | 1.438 | 1.137–1.820 | 0.002 | 1.277 | 0.964–1.691 | 0.088 |
| Statin | 0.747 | 0.524–1.044 | 0.087 | 0.815 | 0.590–1.126 | 0.216 |
| Varices | 1.363 | 1.113–1.668 | 0.003 | 1.223 | 1.002–1.518 | 0.048 |
| ALBI grade 1 | 0.806 | 0.626–1.038 | 0.095 | 0.951 | 0.738–1.228 | 0.703 |
| Child-Pugh B | 4.069 | 2.907–5.700 | <0.001 | 3.103 | 1.873–5.140 | <0.001 |
| AFP > 400 ng/mL | 1.511 | 1.162–1.966 | 0.002 | 1.520 | 1.204–1.918 | <0.001 |
| ECOG-PS > 0 | 1.706 | 1.300–2.241 | <0.001 | 1.510 | 1.164–1.961 | 0.002 |
| Tumor > 50% of liver volume or main trunk PVT | 2.798 | 1.935–4.047 | <0.001 | 1.634 | 1.012–2.639 | 0.044 |
| Macrovascular invasion | 1.587 | 1.286–1.960 | <0.001 | 1.558 | 1.245–1.949 | <0.001 |
| Extrahepatic spread | 1.209 | 0.997–1.578 | 0.097 | 1.360 | 1.069–1.731 | 0.012 |
| Dermatological AEs * | 0.680 | 0.551–0.838 | <0.001 | 0.679 | 0.558–0.826 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ielasi, L.; Tovoli, F.; Tonnini, M.; Tortora, R.; Magini, G.; Sacco, R.; Pressiani, T.; Trevisani, F.; Sansone, V.; Marasco, G.; et al. Beneficial Prognostic Effects of Aspirin in Patients Receiving Sorafenib for Hepatocellular Carcinoma: A Tale of Multiple Confounders. Cancers 2021, 13, 6376. https://doi.org/10.3390/cancers13246376
Ielasi L, Tovoli F, Tonnini M, Tortora R, Magini G, Sacco R, Pressiani T, Trevisani F, Sansone V, Marasco G, et al. Beneficial Prognostic Effects of Aspirin in Patients Receiving Sorafenib for Hepatocellular Carcinoma: A Tale of Multiple Confounders. Cancers. 2021; 13(24):6376. https://doi.org/10.3390/cancers13246376
Chicago/Turabian StyleIelasi, Luca, Francesco Tovoli, Matteo Tonnini, Raffaella Tortora, Giulia Magini, Rodolfo Sacco, Tiziana Pressiani, Franco Trevisani, Vito Sansone, Giovanni Marasco, and et al. 2021. "Beneficial Prognostic Effects of Aspirin in Patients Receiving Sorafenib for Hepatocellular Carcinoma: A Tale of Multiple Confounders" Cancers 13, no. 24: 6376. https://doi.org/10.3390/cancers13246376
APA StyleIelasi, L., Tovoli, F., Tonnini, M., Tortora, R., Magini, G., Sacco, R., Pressiani, T., Trevisani, F., Sansone, V., Marasco, G., Piscaglia, F., & Granito, A. (2021). Beneficial Prognostic Effects of Aspirin in Patients Receiving Sorafenib for Hepatocellular Carcinoma: A Tale of Multiple Confounders. Cancers, 13(24), 6376. https://doi.org/10.3390/cancers13246376