
Transarterial Radioembolization for Unresectable Hepatocellular Carcinoma: Real-Life Efficacy and Safety Analysis of Korean Patients

 , ,
, ,  , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
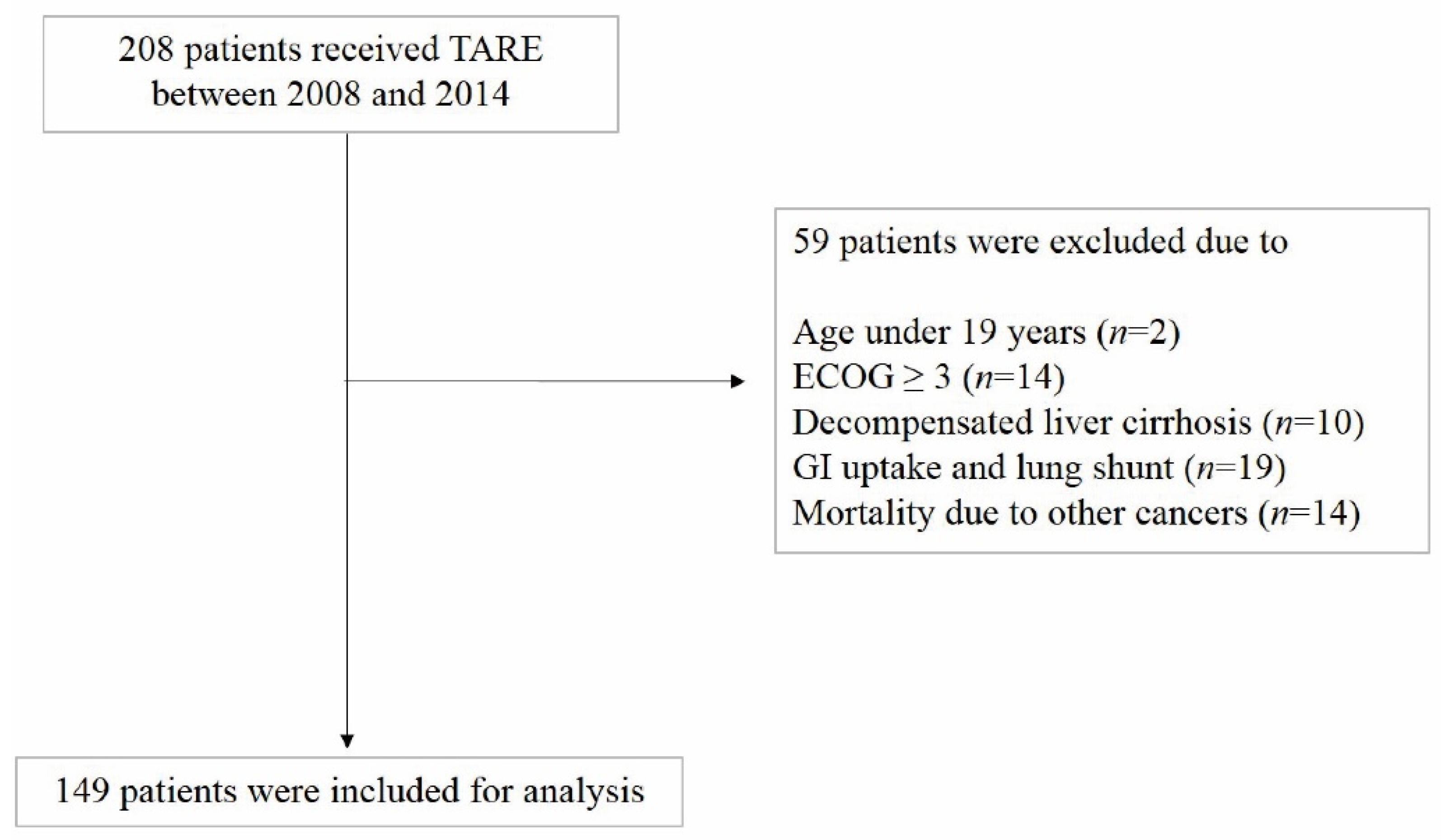
2.1. Patients
2.2. Pretreatment Assessment
2.3. Treatment Modality
2.4. Follow-Up and Assessment of Treatment Responses
2.5. Statistical Analyses
3. Results
3.1. Patient, Tumor, and Treatment Characteristics
3.2. Radiological Tumor Response
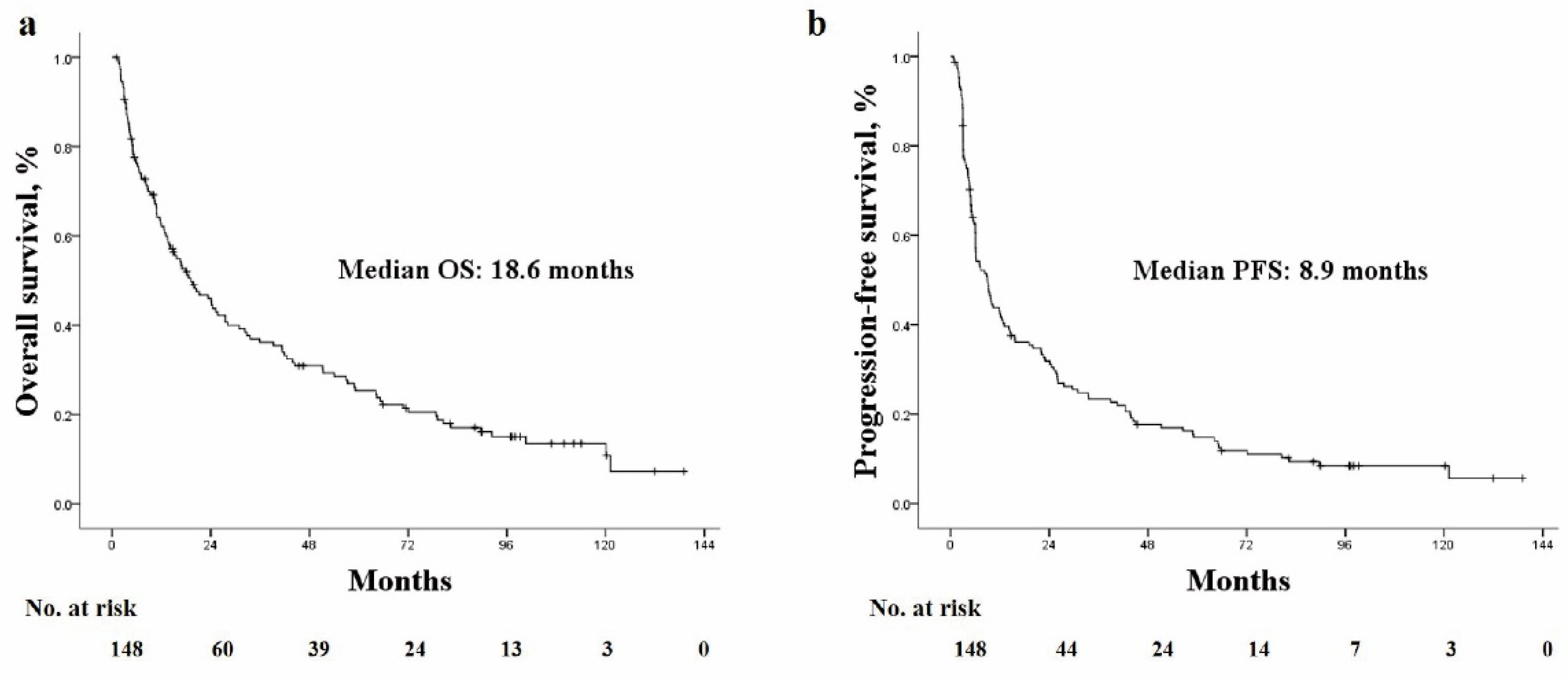
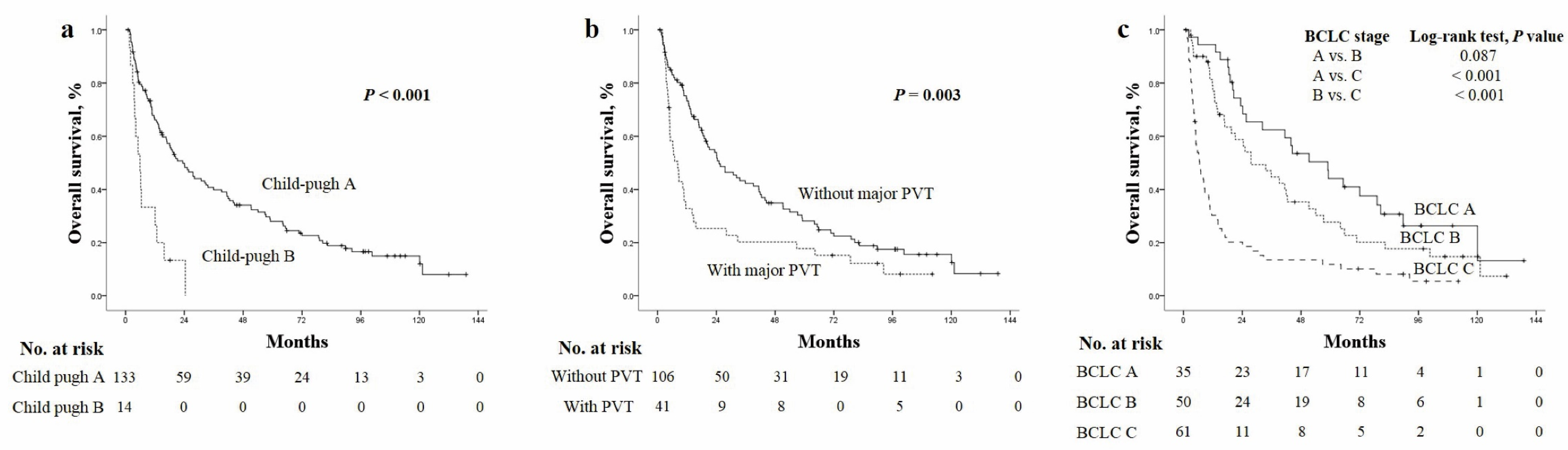
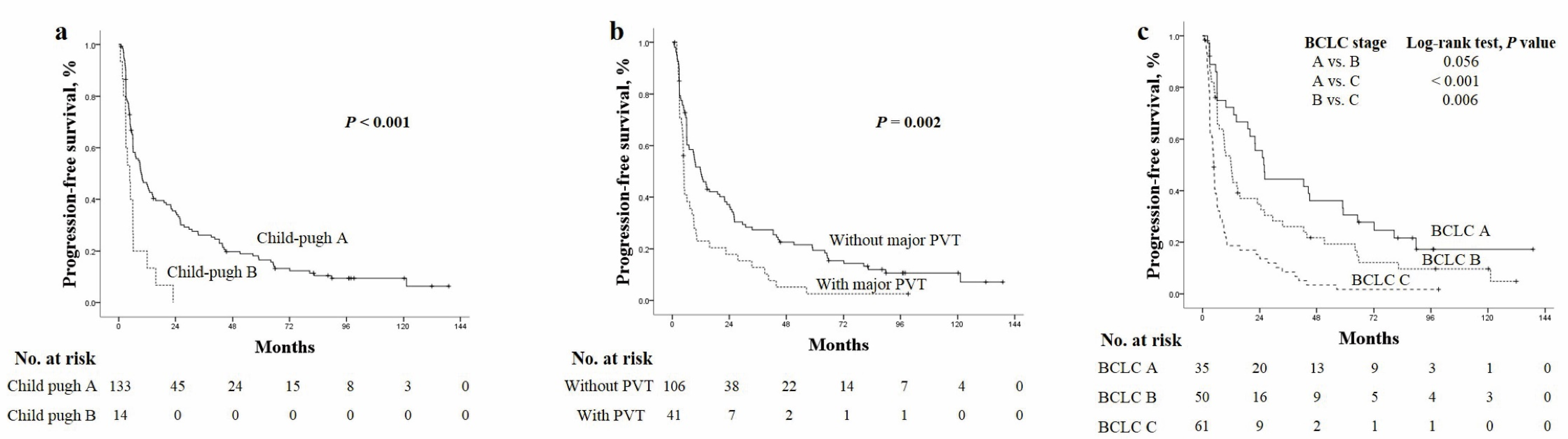
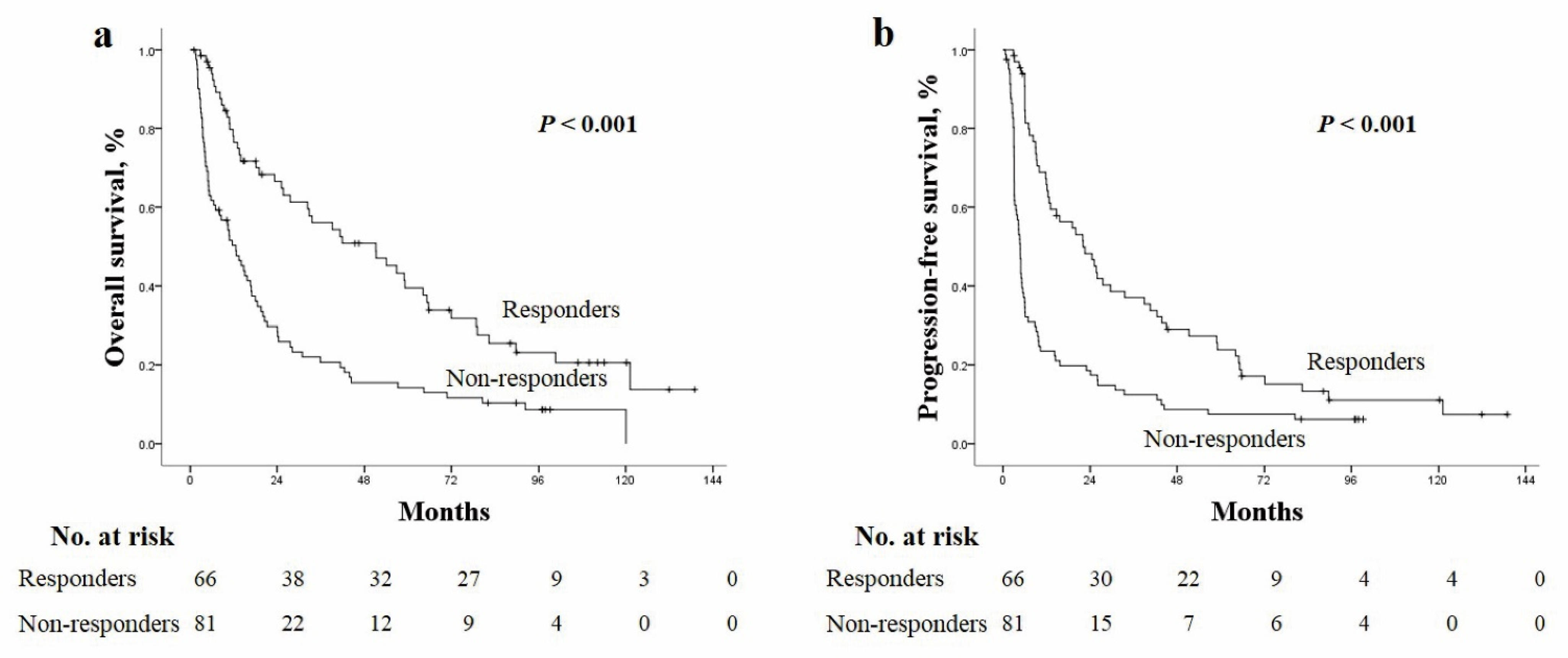
3.3. Overall Survival and Progression-Free Survival
3.4. Prognostic Factors
3.5. Predictive Factors for Achieving Tumor Response
3.6. Toxicity after TARE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balogh, J.; Victor, D.; Asham, E.H., 3rd; Burroughs, S.G.; Boktour, M.; Saharia, A.; Li, X.; Ghobrial, R.M.; Monsour, H.P., Jr. Hepatocellular carcinoma: A review. J. Hepatocell. Carcinoma 2016, 3, 41–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16, 1. [Google Scholar]
- Korean Liver Cancer Association; National Cancer Center. 2018 Korean Liver Cancer Association-National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Gut Liver 2019, 13, 227–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sotiropoulos, G.C.; Lang, H.; Frilling, A.; Molmenti, E.P.; Paul, A.; Nadalin, S.; Radtke, A.; Brokalaki, E.I.; Saner, F.; Hilgard, P.; et al. Resectability of hepatocellular carcinoma: Evaluation of 333 consecutive cases at a single hepatobiliary specialty center and systematic review of the literature. Hepatogastroenterology 2006, 53, 322–329. [Google Scholar]
- Kim, S.U.; Kim, B.K.; Han, K.H. Clinical application of liver stiffness measurement using transient elastography: A surgical perspective. Digestion 2013, 88, 258–265. [Google Scholar] [CrossRef]
- Llovet, J.M.; Real, M.I.; Montana, X.; Planas, R.; Coll, S.; Aponte, J.; Ayuso, C.; Sala, M.; Muchart, J.; Solà, R.; et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: A randomised controlled trial. Lancet 2002, 359, 1734–1739. [Google Scholar] [CrossRef]
- Iwadou, S.; Nouso, K.; Kuwaki, K.; Kobayashi, Y.; Nakamura, S.; Tanaka, H.; Miyoshi, K.; Ohnishi, H.; Miyake, Y.; Shiraha, H.; et al. Time-dependent analysis of predisposing factors for the recurrence of hepatocellular carcinoma. Liver Int. 2010, 30, 1027–1032. [Google Scholar] [CrossRef] [Green Version]
- Park, M.S.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.H.; Chon, C.Y.; Seong, J. Combination treatment of localized concurrent chemoradiation therapy and transarterial chemoembolization in locally advanced hepatocellular carcinoma with intrahepatic metastasis. Cancer Chemother. Pharmacol. 2013, 71, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Mlynarsky, L.; Menachem, Y.; Shibolet, O. Treatment of hepatocellular carcinoma: Steps forward but still a long way to go. World J. Hepatol. 2015, 7, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Lewandowski, R.J.; Mulcahy, M.F.; Riaz, A.; Ryu, R.K.; Ibrahim, S.; Atassi, B.; Baker, T.; Gates, V.; Miller, F.H.; et al. Radioembolization for Hepatocellular Carcinoma Using Yttrium-90 Microspheres: A Comprehensive Report of Long-term Outcomes. Gastroenterology 2010, 138, 52–64. [Google Scholar] [CrossRef]
- Hilgard, P.; Hamami, M.; Fouly, A.E.; Scherag, A.; Muller, S.; Ertle, J.; Heusner, T.; Cicinnati, V.R.; Paul, A.; Bockisch, A.; et al. Radioembolization with yttrium-90 glass microspheres in hepatocellular carcinoma: European experience on safety and long-term survival. Hepatology 2010, 52, 1741–1749. [Google Scholar] [CrossRef]
- Kulik, L.M.; Carr, B.I.; Mulcahy, M.F.; Lewandowski, R.J.; Atassi, B.; Ryu, R.K.; Sato, K.T.; Benson, A., III; Nemcek, A.A., Jr.; Gates, V.L.; et al. Safety and efficacy of 90Y radiotherapy for hepatocellular carcinoma with and without portal vein thrombosis. Hepatology 2008, 47, 71–81. [Google Scholar] [CrossRef]
- Kim, H.C. Radioembolization for the treatment of hepatocellular carcinoma. Clin. Mol. Hepatol. 2017, 23, 109–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangro, B.; Salem, R. Transarterial chemoembolization and radioembolization. Semin. Liver Dis. 2014, 34, 435–443. [Google Scholar]
- Kim, D.Y.; Han, K.H. Transarterial chemoembolization versus transarterial radioembolization in hepatocellular carcinoma: Optimization of selecting treatment modality. Hepatol. Int. 2016, 10, 883–892. [Google Scholar] [CrossRef]
- Clavien, P.A.; Petrowsky, H.; DeOliveira, M.L.; Graf, R. Strategies for safer liver surgery and partial liver transplantation. N. Engl. J. Med. 2007, 356, 1545–1559. [Google Scholar] [CrossRef]
- Luo, J.; Peng, Z.W.; Guo, R.P.; Zhang, Y.Q.; Li, J.Q.; Chen, M.S.; Shi, M. Hepatic resection versus transarterial lipiodol chemoembolization as the initial treatment for large, multiple, and resectable hepatocellular carcinomas: A prospective nonrandomized analysis. Radiology 2011, 259, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Hyun, M.H.; Lee, Y.S.; Kim, J.H.; Lee, C.U.; Jung, Y.K.; Seo, Y.S.; Yim, H.J.; Yeon, J.E.; Byun, K.S. Hepatic resection compared to chemoembolization in intermediate- to advanced-stage hepatocellular carcinoma: A meta-analysis of high-quality studies. Hepatology 2018, 68, 977–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciria, R.; Lopez-Cillero, P.; Gallardo, A.B.; Cabrera, J.; Pleguezuelo, M.; Ayllon, M.D.; Luque, A.; Zurera, L.; Espejo, J.J.; Rodríguez-Perálvarez, M.; et al. Optimizing the management of patients with BCLC stage-B hepatocellular carcinoma: Modern surgical resection as a feasible alternative to transarterial chemoemolization. Eur. J. Surg. Oncol. 2015, 41, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Bogdanovic, A.; Bulajic, P.; Masulovic, D.; Bidzic, N.; Zivanovic, M.; Galun, D. Liver resection versus transarterial chemoembolization for huge hepatocellular carcinoma: A propensity score matched analysis. Sci. Rep. 2021, 11, 4493. [Google Scholar] [CrossRef]
- Gabr, A.; Abouchaleh, N.; Ali, R.; Baker, T.; Caicedo, J.; Katariya, N.; Abecassis, M.; Riaz, A.; Lewandowski, R.J.; Salem, R. Outcomes of Surgical Resection after Radioembolization for Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2018, 29, 1502–1510.e1. [Google Scholar] [CrossRef] [PubMed]
- Song, J.E.; Jung, K.S.; Kim, D.Y.; Song, K.; Won, J.Y.; Lee, H.W.; Kim, B.K.; Kim, S.U.; Park, J.Y.; Ahn, S.H.; et al. Transarterial Radioembolization Versus Concurrent Chemoradiation Therapy for Locally Advanced Hepatocellular Carcinoma: A Propensity Score Matching Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Fuster, J.; Bruix, J. The Barcelona approach: Diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. 2004, 10 (Suppl. S2), S115–S120. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Lewandowski, R.J.; Sato, K.T.; Atassi, B.; Ryu, R.K.; Nemcek, A.A.; Kulik, L., Jr.; Geschwind, J.F.; Murthy, R.; Rilling, W.; Liu, D.; et al. Radioembolization with 90Y microspheres: Angiographic and technical considerations. Cardiovasc. Interv. Radiol. 2007, 30, 571–592. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Salem, R.; Lewandowski, R.J.; Kulik, L.; Wang, E.; Riaz, A.; Ryu, R.K.; Sato, K.T.; Gupta, R.; Nikolaidis, P.; Miller, F.H.; et al. Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology 2011, 140, 497–507.e2. [Google Scholar] [CrossRef] [Green Version]
- Mantry, P.S.; Mehta, A.; Madani, B.; Mejia, A.; Shahin, I. Selective internal radiation therapy using yttrium-90 resin microspheres in patients with unresectable hepatocellular carcinoma: A retrospective study. J. Gastrointest. Oncol. 2017, 8, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Van Thai, N.; Thinh, N.T.; Ky, T.D.; Bang, M.H.; Giang, D.T.; Ha, L.N.; Son, M.H.; Tien, D.D.; Lee, H.W. Efficacy and safety of selective internal radiation therapy with yttrium-90 for the treatment of unresectable hepatocellular carcinoma. BMC Gastroenterol. 2021, 21, 216. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Vilgrain, V.; Pereira, H.; Assenat, E.; Guiu, B.; Ilonca, A.D.; Pageaux, G.P.; Sibert, A.; Bouattour, M.; Lebtahi, R.; Allaham, W.; et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): An open-label randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1624–1636. [Google Scholar] [CrossRef]
- Chow, P.K.H.; Gandhi, M.; Tan, S.B.; Khin, M.W.; Khasbazar, A.; Ong, J.; Choo, S.P.; Cheow, P.C.; Chotipanich, C.; Lim, K.; et al. SIRveNIB: Selective Internal Radiation Therapy Versus Sorafenib in Asia-Pacific Patients With Hepatocellular Carcinoma. J. Clin. Oncol. 2018, 36, 1913–1921. [Google Scholar] [CrossRef]
- Golfieri, R.; Giampalma, E.; Renzulli, M.; Cioni, R.; Bargellini, I.; Bartolozzi, C.; Breatta, A.D.; Gandini, G.; Nani, R.; Gasparini, D.; et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br. J. Cancer 2014, 111, 255–264. [Google Scholar] [CrossRef] [Green Version]
- Song, M.J.; Chun, H.J.; Song, D.S.; Kim, H.Y.; Yoo, S.H.; Park, C.-H.; Bae, S.H.; Choi, J.Y.; Im Chang, U.; Yang, J.M.; et al. Comparative study between doxorubicin-eluting beads and conventional transarterial chemoembolization for treatment of hepatocellular carcinoma. J. Hepatol. 2012, 57, 1244–1250. [Google Scholar] [CrossRef]
- Vouche, M.; Habib, A.; Ward, T.J.; Kim, E.; Kulik, L.; Ganger, D.; Mulcahy, M.; Baker, T.; Abecassis, M.; Sato, K.T.; et al. Unresectable solitary hepatocellular carcinoma not amenable to radiofrequency ablation: Multicenter radiology-pathology correlation and survival of radiation segmentectomy. Hepatology 2014, 60, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, R.J.; Gabr, A.; Abouchaleh, N.; Ali, R.; Al Asadi, A.; Mora, R.A.; Kulik, L.; Ganger, D.; Desai, K.; Thornburg, B.; et al. Radiation Segmentectomy: Potential Curative Therapy for Early Hepatocellular Carcinoma. Radiology 2018, 287, 1050–1058. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Li, Y.; Gao, Z.H.; Qu, X.J. The adverse effects of sorafenib in patients with advanced cancers. Basic Clin. Pharmacol. Toxicol. 2015, 116, 216–221. [Google Scholar] [CrossRef]
- Lemieux, S.; Buies, A.; Hallet, J.; Daigle, G.; Cote, F.; Provencher, S. Effect of Yttrium-90 transarterial radioembolization in patients with non-surgical hepatocellular carcinoma: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0247958. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patients, N = 149 |
|---|---|
| Demographic variables | |
| Age (y) | 60.6 ± 12.6 |
| Male sex | 117 (78.5) |
| Etiology | |
| Hepatitis B virus | 87 (58.4) |
| Hepatitis C virus | 42 (28.2) |
| Alcohol | 10 (6.7) |
| Cryptogenic | 7 (4.7) |
| Hepatitis B virus and hepatitis C virus | 2 (1.3) |
| Hepatitis C virus and alcohol | 1 (0.7) |
| Previous HCC therapy | |
| None | 135 (90.6) |
| Resection | 2 (1.3) |
| TACE | 12 (8.1) |
| Liver cirrhosis | 94 (63.1) |
| Ascites | 15 (10.1) |
| Child–Turcotte–Pugh class | |
| A | 134 (89.9) |
| B | 15 (10.1) |
| ECOG score | |
| 0 | 63 (42.3) |
| 1 | 75 (50.3) |
| 2 | 11 (7.4) |
| Laboratory variables | |
| Total bilirubin (mg/dL) | 0.8 ± 0.5 |
| Serum albumin (g/dL) | 3.7 ± 0.5 |
| Prothrombin time (INR) | 1.06 ±0.12 |
| AFP (ng/mL) | 19,884 ± 93,841 |
| >200 | 72 (48.3) |
| DCP (mAU/mL) | 12,428 ± 23,879 |
| >15,000 | 27 (18.1) |
| Tumor characteristics | |
| Tumor number | |
| 1 | 52 (34.9) |
| 2–3 | 42 (28.2) |
| >3 | 55 (36.9) |
| Largest tumor diameter, cm | 7.7 ± 3.5 |
| BCLC stage | |
| A | 36 (24.2) |
| B | 51 (34.2) |
| C | 62 (41.6) |
| Metastasis | |
| None | 122 (81.9) |
| Lymph node | 7 (4.7) |
| Solid organ | 14 (9.4) |
| Bone | 6 (4) |
| Tumor location | |
| Bilobar | 66 (44.3) |
| Unilobar | 83 (55.7) |
| Tumor burden > 25% | 41 (27.5%) |
| Tumor-related PVT | |
| None | 91 (61.1) |
| Segmental branch | 16 (10.7) |
| Rt. or Lt. portal vein | 37 (24.8) |
| Main portal vein | 5 (3.4) |
| Hepatic vein invasion | 13 (8.7) |
| Bile duct invasion | 10 (6.7) |
| Treatment modalities after TARE | |
| Resection | 8 (5.4) |
| Liver transplantation | 9 (6) |
| TACE | 62 (41.6) |
| Radiotherapy and systemic treatment | 28 (18.8) |
| None | 42 (28.2) |
| Best supportive care | 33 |
| Not evaluable | 9 |
| Overall Radiological Response (From Any Time on Study) | Total Patients (n, %) | BCLC A (n, %) | BCLC B (n, %) | BCLC C (n, %) |
|---|---|---|---|---|
| Number of patients | 149 | 36 | 51 | 62 |
| Complete response | 23 (15.4) | 10 (27.8) | 11 (21.6) | 2 (3.2) |
| Partial response | 44 (29.5) | 12 (33.3) | 19 (37.3) | 13 (21) |
| Stable disease | 44 (29.5) | 10 (27.8) | 16 (31.4) | 18 (29) |
| Progressive disease | 38 (25.5) | 4 (11.1) | 5 (9.8) | 29 (46.8) |
| Objective response (CR + PR) | 67 (45) | 22 (61.1) | 30 (58.8) | 15 (24.2) |
| Disease control (CR + PR + SD) | 111 (74.5) | 32 (88.9) | 46 (90.2) | 33 (53.2) |
| Variable | Overall Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Multivariate Analysis Using BCLC Stage | |||||||
| HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Demographic variables | |||||||||
| Age (≥60 y) | 1.001 | 0.986–1.001 | 0.725 | - | - | - | - | - | - |
| Male sex | 1.027 | 0.655–1.611 | 0.906 | - | - | - | - | - | - |
| Etiology (CHB) | 1.414 | 0.985–2.030 | 0.06 | - | - | - | - | - | - |
| Previous HCC therapy | 2.147 | 1.165–3.959 | 0.014 | 1.487 | 0.633–3.494 | 0.362 | 0.896 | 0.418–1.924 | 0.779 |
| Liver cirrhosis | 1.55 | 1.054–2.279 | 0.026 | 1.996 | 1.28–3.112 | 0.009 | 1.393 | 0.882–2.199 | 0.155 |
| Ascites | 1.686 | 0.925–3.073 | 0.088 | - | - | - | - | - | - |
| CTP score | |||||||||
| A | 1 | - | - | - | - | - | - | - | - |
| B | 3.507 | 1.949–6.311 | <0.001 | 1.81 | 0.845–3.876 | 0.143 | - | - | - |
| ECOG | |||||||||
| 0 | 1 | - | <0.001 | 1 | - | 0.428 | 1 | - | 0.019 |
| 1 | 1.727 | 1.777–2.534 | 0.005 | 1.326 | 0.863–2.037 | 0.197 | 1.813 | 1.199–2.74 | 0.005 |
| 2 | 3.746 | 1.868–7.511 | <0.001 | 1.261 | 0.505–3.147 | 0.62 | 1.323 | 0.568–3.082 | 0.517 |
| Laboratory variables | |||||||||
| Bilirubin (mg/dL) | 1.989 | 1.429–2.769 | <0.001 | - | - | - | - | - | - |
| Albumin (g/dL) | 0.45 | 0.324–0.625 | <0.001 | - | - | - | - | - | - |
| PT (INR) | 4.905 | 0.867–27.732 | 0.072 | - | - | - | - | - | - |
| AFP > 200 ng/mL | 1.496 | 1.037 | 0.031 | 0.942 | 0.607–1.464 | 0.791 | 0.944 | 0.615–1.45 | 0.794 |
| DCP > 15,000 mAU/mL | 1.538 | 1.05–2.251 | 0.027 | 1.307 | 0.716–2.385 | 0.383 | 1.357 | 0.804–2.29 | 0.253 |
| Tumor characteristics | |||||||||
| Size ≥ 10 cm | 1.821 | 1.19–2.787 | 0.006 | 0.663 | 0.326–1.349 | 0.257 | |||
| Tumor number >3 | 2.438 | 1.674–3.552 | <0.001 | 2.457 | 1.552–3.888 | <0.001 | |||
| BCLC stage | |||||||||
| A | 1 | - | <0.001 | - | - | - | 1 | - | <0.001 |
| B | 1.444 | 0.87–2.397 | 0.155 | - | - | - | 2.278 | 1.279–4.059 | 0.005 |
| C | 3.498 | 2.164–5.654 | <0.001 | - | - | - | 3.925 | 2.238–6.886 | <0.001 |
| Presence of metastasis | 5.683 | 3.482–9.275 | <0.001 | 2.773 | 1.571–4.895 | 0.004 | |||
| Bilobar location | 1.424 | 0.992–2.044 | 0.055 | - | - | - | - | - | - |
| Tumor burden >25% | 1.579 | 1.068–2.336 | 0.022 | 1.426 | 0.803–2.532 | 0.226 | 0.897 | 0.55–1.463 | 0.664 |
| Portal vein thrombosis | 1.796 | 1.2096–2.668 | 0.004 | 1.831 | 1.172–2.858 | 0.008 | - | - | - |
| Hepatic vein invasion | 5.102 | 2.786–9.344 | <0.001 | 1.855 | 0.943–3.65 | 0.074 | - | - | - |
| Bile duct invasion | 1.451 | 0.734–2.869 | 0.284 | - | - | - | - | - | - |
| Objective response | 0.437 | 0.3–0.636 | <0.001 | 0.424 | 0.271–0.663 | <0.001 | 0.486 | 0.316–0.747 | <0.001 |
| Post TARE treatment | |||||||||
| Curative | <0.001 | 1 | - | <0.001 | - | - | <0.001 | ||
| TACE | 15.801 | 2.183–114.381 | 0.006 | 13.55 | 1.834–100.133 | 0.01 | 20.51 | 2.81–149.65 | 0.003 |
| RTx/Systemic CTx/BSC | 53.702 | 7.232–398.797 | <0.001 | 32.35 | 4.347–240.833 | 0.001 | 41.72 | 5.55–313.55 | <0.001 |
| Variable | Progression-Free Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Multivariate Analysis Using BCLC Stage | |||||||
| HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Demographic variables | |||||||||
| Age (≥60y) | 0.991 | 0.702–1.397 | 0.957 | - | - | - | - | - | - |
| Male sex | 0.926 | 0.602–1.425 | 0.728 | - | - | - | - | - | - |
| Etiology (CHB) | 0.782 | 0.553–1.105 | 0.163 | - | - | - | - | - | - |
| Previous HCC therapy | 2.552 | 1.375–4.738 | 0.003 | 1.889 | 0.851–4.192 | 0.114 | 1.778 | 0.839–3.767 | 0.105 |
| Liver cirrhosis | 1.478 | 1.028–2.126 | 0.035 | 2.034 | 1.307–3.164 | 0.002 | 1.654 | 1.075–2.544 | 0.011 |
| Ascites | 1.26 | 0.709–2.24 | 0.43 | - | - | - | - | - | - |
| CTP class | |||||||||
| A | 1 | - | - | - | - | - | |||
| B | 2.684 | 1.542–4.671 | <0.001 | 1.123 | 0.55–2.295 | 0.75 | - | - | - |
| ECOG | |||||||||
| 0 | 1 | - | 0.024 | 1 | - | 0.763 | 1 | - | 0.448 |
| 1 | 1.467 | 1.024–2.103 | 0.037 | 1.164 | 0.775–1.747 | 0.464 | 1.276 | 0.854–1.907 | 0.238 |
| 2 | 2.221 | 1.124–4.39 | 0.022 | 1.064 | 0.45–2.517 | 0.887 | 0.962 | 0.415–2.248 | 0.929 |
| Laboratory variables | |||||||||
| Bilirubin (mg/dL) | 1.684 | 1.203–2.357 | 0.002 | - | - | - | - | - | - |
| Albumin (g/dL) | 0.539 | 0.394–0.738 | <0.001 | - | - | - | - | - | - |
| PT (INR) | 3.339 | 0.706–15.778 | 0.128 | - | - | - | - | - | - |
| AFP > 200 ng/mL | 1.434 | 1.013–2.029 | 0.042 | 0.9 | 0.593–1.366 | 0.62 | 0.902 | 0.605–1.344 | 0.611 |
| DCP > 15,000 mAU/mL | 2.308 | 1.483–3.592 | <0.001 | 1.734 | 1.064–2.825 | 0.027 | 1.549 | 0.926–2.589 | 0.041 |
| Tumor characteristics | |||||||||
| Size ≥ 10 cm | 1.873 | 1.236–2.838 | 0.003 | 0.893 | 0.517–1.542 | 0.684 | - | - | - |
| Tumor number (>3) | 1.966 | 1.37–2.82 | <0.001 | 1.355 | 0.833–2.205 | 0.221 | - | - | - |
| BCLC stage | |||||||||
| A | 1 | - | <0.001 | - | - | - | 1 | - | 0.001 |
| B | 1.531 | 0.955–2.454 | 0.077 | - | - | - | 1.42 | 0.831–2.426 | 0.236 |
| C | 3.421 | 2.152–5.437 | <0.001 | - | - | - | 2.544 | 1.518–4.261 | <0.001 |
| Presence of metastasis | 3.705 | 2.344–5.857 | <0.001 | 2.363 | 1.373-4.066 | 0.001 | - | - | - |
| Bilobar location | 1.177 | 0.834–1.66 | 0.353 | - | - | - | - | - | - |
| Tumor burden >25% | 1.529 | 1.046–2.234 | 0.028 | 1.197 | 0.691–2.074 | 0.521 | 0.946 | 0.604–1.481 | 0.807 |
| Portal vein thrombosis | 1.827 | 1.247–2.678 | 0.002 | 1.545 | 0.998–2.393 | 0.061 | - | - | - |
| Hepatic vein invasion | 3.365 | 1.865–6.069 | <0.001 | 1.294 | 0.649–2.579 | 0.453 | - | - | - |
| Bile duct invasion | 1.86 | 0.971–3.562 | 0.061 | - | - | - | - | - | - |
| Objective response | 0.39 | 0.253–0.601 | <0.001 | 0.46 | 0.298–0.709 | <0.001 | |||
| Post TARE treatment | |||||||||
| Curative | 1 | - | <0.001 | 1 | - | 0.016 | - | - | 0.007 |
| TACE | 15.801 | 2.183–114.381 | 0.006 | 2.024 | 0.949–4.317 | 0.097 | 2.311 | 1.093–4.888 | 0.063 |
| RTx/Systemic CTx/BSC | 53.702 | 7.232–398.797 | <0.001 | 3.512 | 1.5–8.225 | 0.017 | 3.841 | 1.629–9.061 | 0.004 |
| Toxicity | Grade 1/2 | Grade 3/4 |
|---|---|---|
| N (%) | N (%) | |
| Clinical toxicities | ||
| Nausea | 21 (17.1) | 1 (0.8) |
| Vomiting | 3 (0.2) | 0 (0.0) |
| Nausea and vomiting | 1 (0.8) | 0 (0.0) |
| Anorexia | 13 (10.6) | 1 (0.8) |
| Diarrhea | 1 (0.8) | 0 (0.0) |
| Weight loss | 1 (0.8) | 0 (0.0) |
| Abdominal pain | 32 (26) | 2 (1.6) |
| Fever | 12 (7.3) | 0 (0.0) |
| Fatigue | 9 (7.3) | 0 (0.0) |
| Cholecystitis | 0 (0.0) | 1 (0.8) |
| Gastritis | 2 (1.6) | 0 (0.0) |
| Other | ||
| Pruritus | 1 (0.8) | 0 (0.0) |
| Splenic infarction | 1 (0.8) | 0 (0.0) |
| Post-procedural bleeding | 1 (0.8) | 0 (0.0) |
| Sepsis | 0 (0.0) | 1 (0.8) |
| Celiac trunk dissection | 0 (0.0) | 1 (0.8) |
| HCC rupture a | 0 (0.0) | 1 (0.8) |
| Laboratory toxicities | ||
| AST/ALT elevation | 14 (11.4) | 3 (2.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yim, S.Y.; Chun, H.S.; Lee, J.S.; Lim, J.-H.; Kim, T.H.; Kim, B.K.; Kim, S.U.; Park, J.Y.; Ahn, S.H.; Kim, G.M.; et al. Transarterial Radioembolization for Unresectable Hepatocellular Carcinoma: Real-Life Efficacy and Safety Analysis of Korean Patients. Cancers 2022, 14, 385. https://doi.org/10.3390/cancers14020385
Yim SY, Chun HS, Lee JS, Lim J-H, Kim TH, Kim BK, Kim SU, Park JY, Ahn SH, Kim GM, et al. Transarterial Radioembolization for Unresectable Hepatocellular Carcinoma: Real-Life Efficacy and Safety Analysis of Korean Patients. Cancers. 2022; 14(2):385. https://doi.org/10.3390/cancers14020385
Chicago/Turabian StyleYim, Sun Young, Ho Soo Chun, Jae Seung Lee, Ji-Hwan Lim, Tae Hyung Kim, Beom Kyung Kim, Seung Up Kim, Jun Yong Park, Sang Hoon Ahn, Gyoung Min Kim, and et al. 2022. "Transarterial Radioembolization for Unresectable Hepatocellular Carcinoma: Real-Life Efficacy and Safety Analysis of Korean Patients" Cancers 14, no. 2: 385. https://doi.org/10.3390/cancers14020385
APA StyleYim, S. Y., Chun, H. S., Lee, J. S., Lim, J. -H., Kim, T. H., Kim, B. K., Kim, S. U., Park, J. Y., Ahn, S. H., Kim, G. M., Won, J. Y., Seo, Y. S., Kim, Y. H., Um, S. H., & Kim, D. Y. (2022). Transarterial Radioembolization for Unresectable Hepatocellular Carcinoma: Real-Life Efficacy and Safety Analysis of Korean Patients. Cancers, 14(2), 385. https://doi.org/10.3390/cancers14020385