
Breast Tumor Characterization Using [18F]FDG-PET/CT Imaging Combined with Data Preprocessing and Radiomics

 ,
,  , ,
, ,  ,
,  , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Histopathologic Analysis
2.3. PET/CT
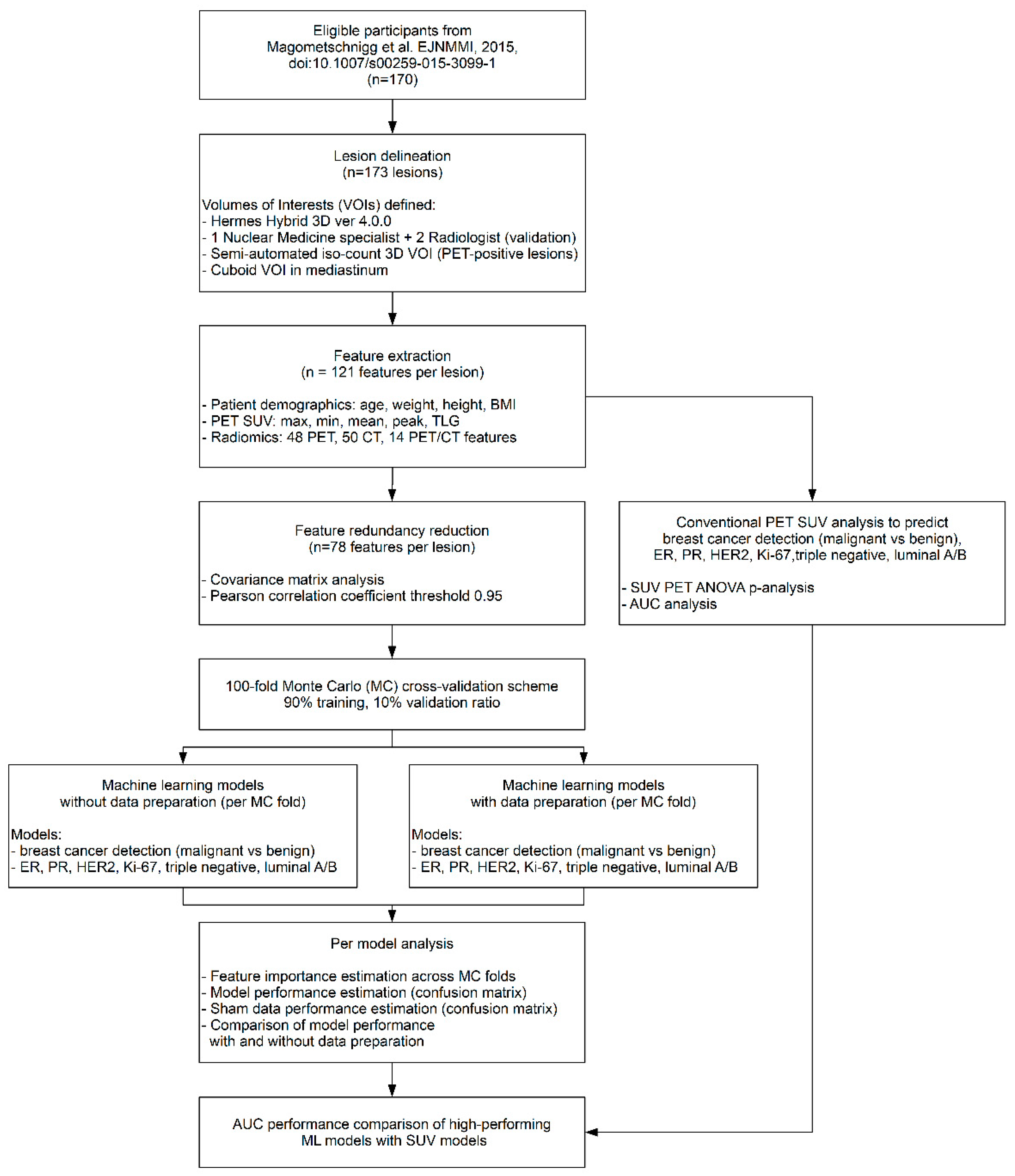
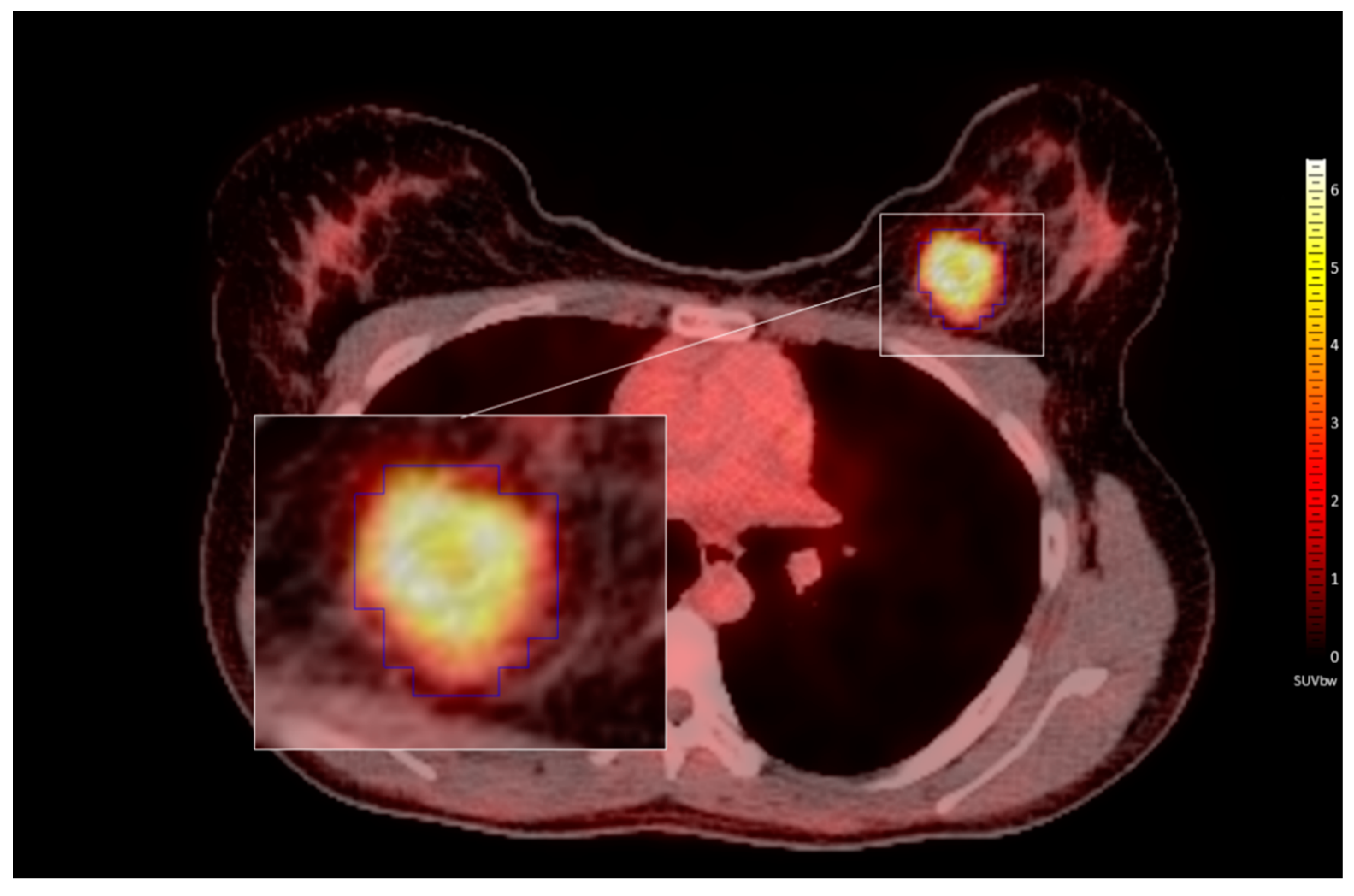
2.4. Lesion Delineation
2.5. Feature Extraction
2.6. Feature Redundancy Reduction
2.7. Predictive Model Establishment
2.8. Model Performance Estimation
2.9. Estimating the Effect of Data Preparation
2.10. Feature Importance Estimation
2.11. Conventional PET Correlation Analyses
3. Results
3.1. Patients
3.2. Model Performance Estimation
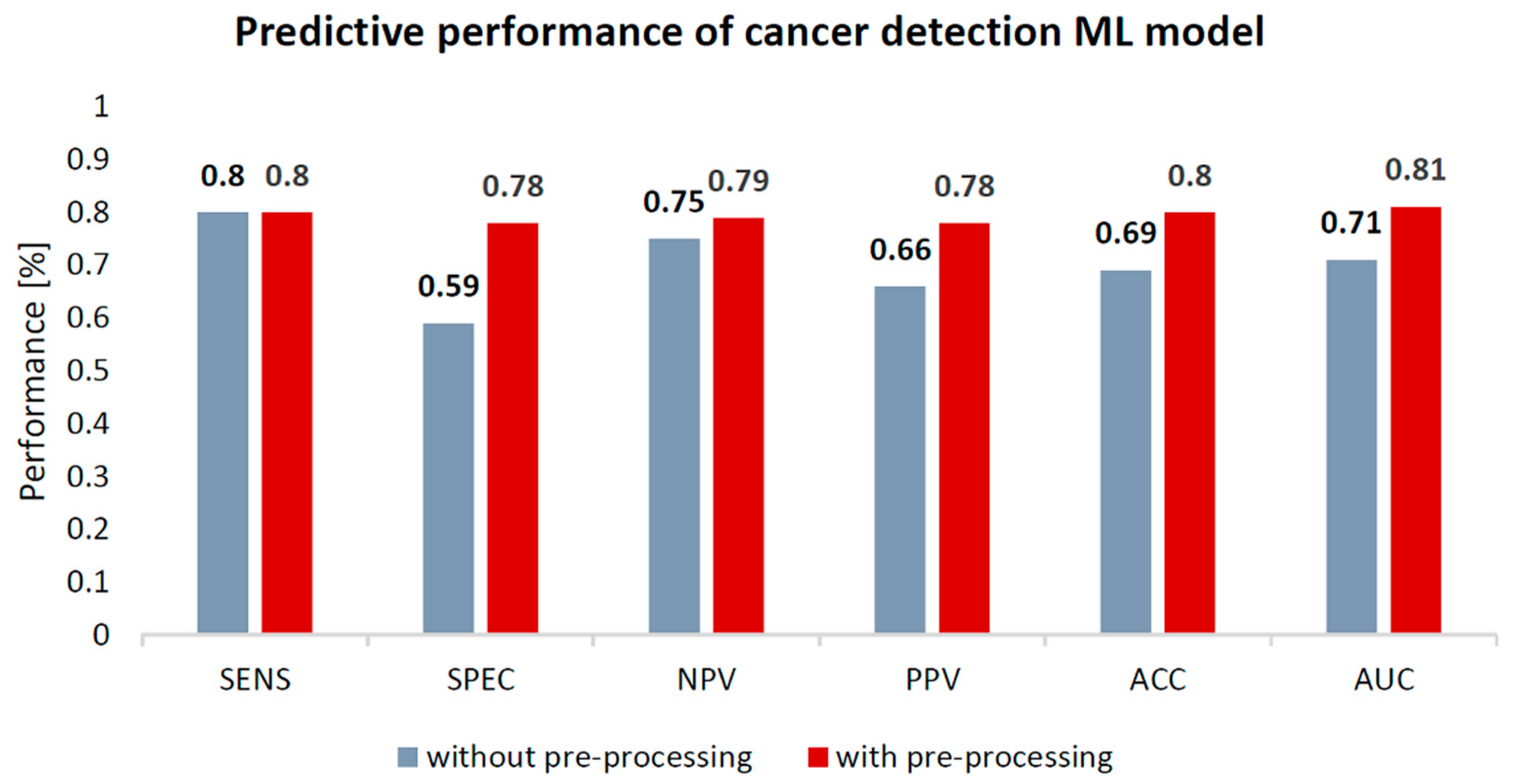
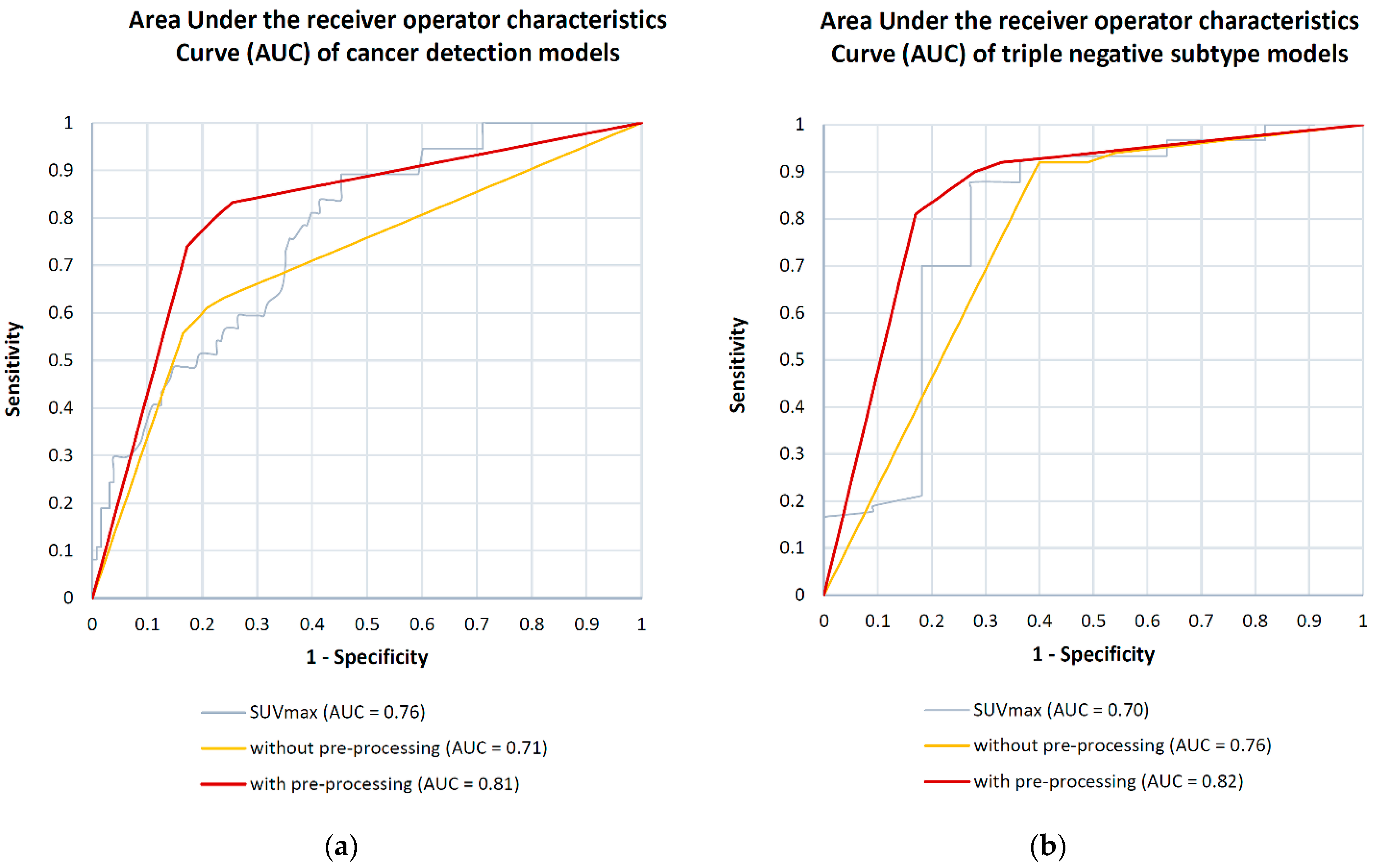
3.2.1. Breast Cancer Detection
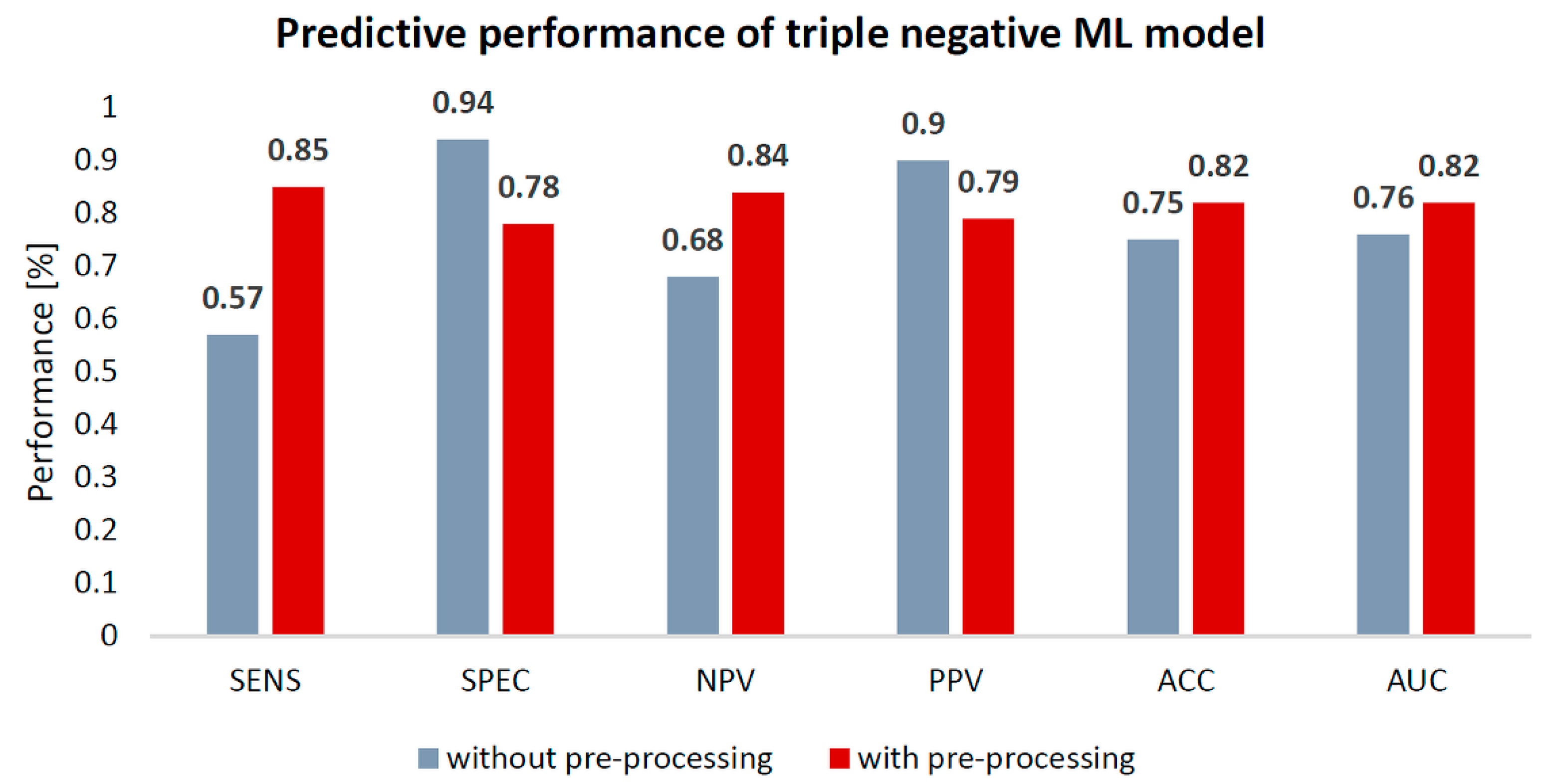
3.2.2. Breast Cancer Subtyping
3.3. Feature Importance Estimation
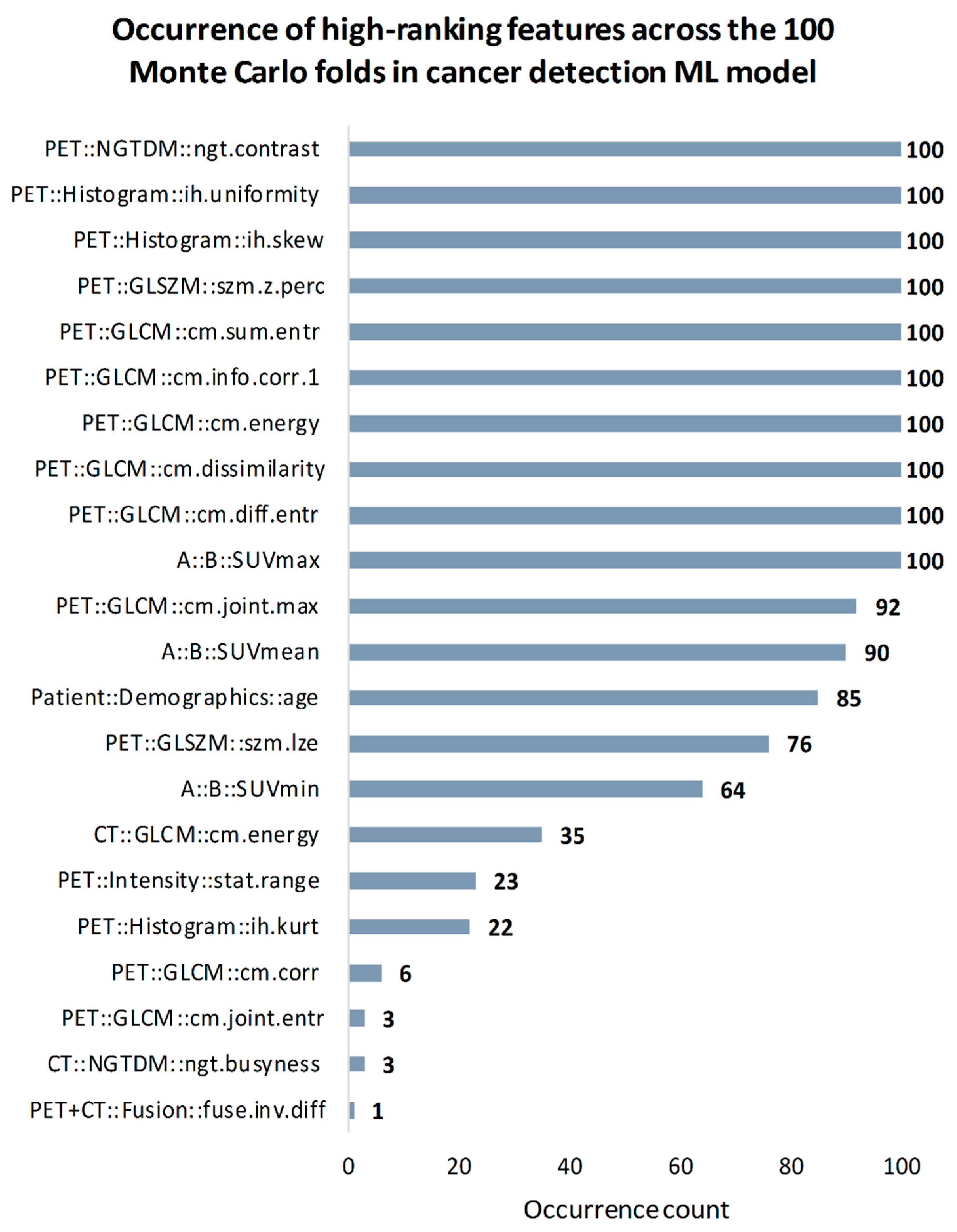
3.3.1. Breast Cancer Detection
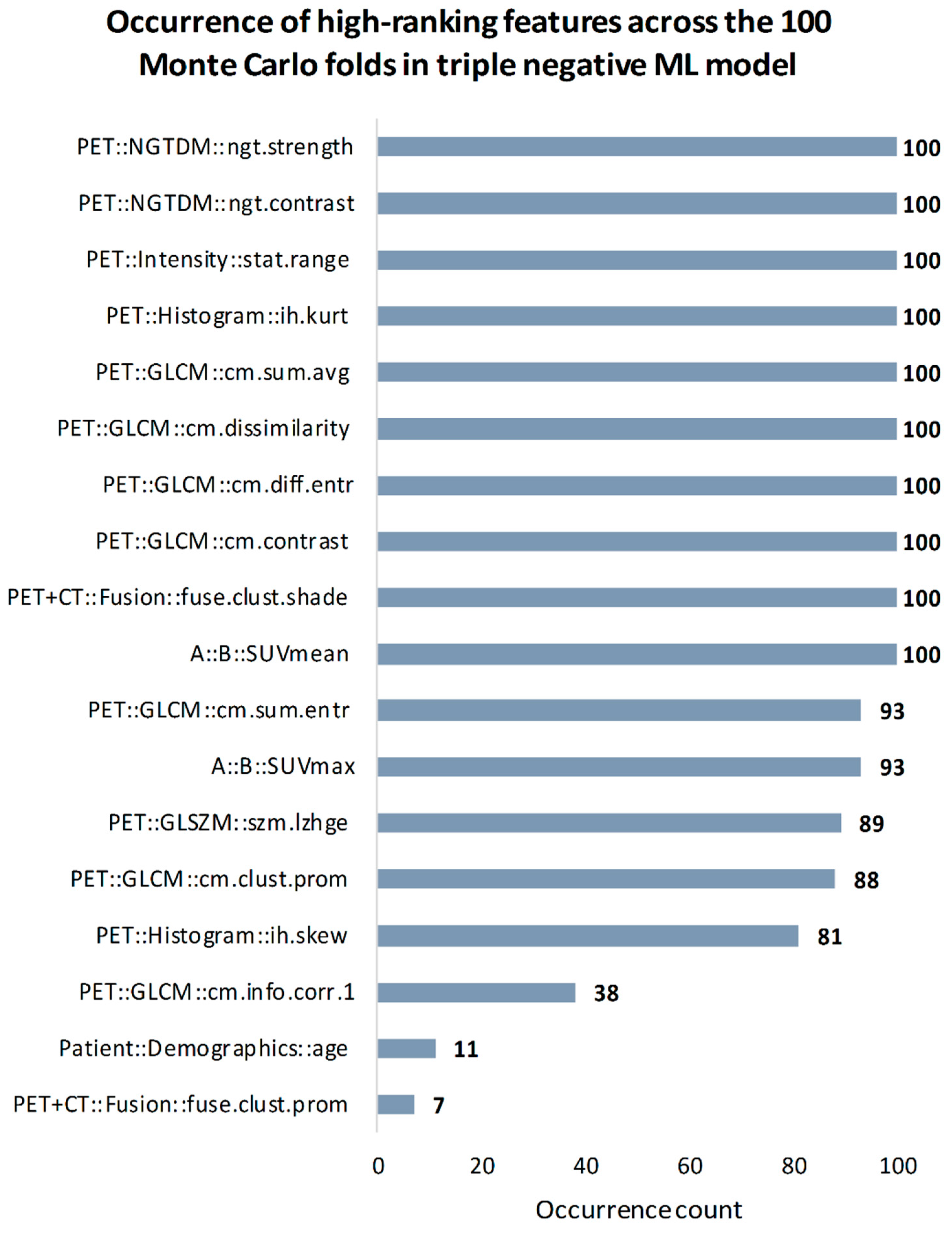
3.3.2. Breast Cancer Subtyping
3.4. Conventional PET Correlation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Estimated Age-Standardized Incidence and Mortality Rates (World) in 2020, Worldwide, Both Sexes, All Ages. Available online: https://gco.iarc.fr/today/online-analysis-multi-bars?v=2020&mode=cancer&mode_population=countries&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=10&group_cancer=1&include_nmsc=1&include_nmsc_other=1&type_multiple=%257B%2522inc%2522%253Atrue%252C%2522mort%2522%253Atrue%252C%2522prev%2522%253Afalse%257D&orientation=horizontal&type_sort=0&type_nb_items=%257B%2522top%2522%253Atrue%252C%2522bottom%2522%253Afalse%257D (accessed on 18 January 2021).
- Loughran, C.F.; Keeling, C.R. Seeding of tumour cells following breast biopsy: A literature review. Br. J. Radiol. 2011, 84, 869–874. [Google Scholar] [CrossRef]
- White, R.R.; Halperin, T.J.; Olson, J.A., Jr.; Soo, M.S.; Bentley, R.C.; Seigler, H.F. Impact of Core-Needle Breast Biopsy on the Surgical Management of Mammographic Abnormalities. Ann. Surg. 2001, 233, 769–777. [Google Scholar] [CrossRef]
- Zaha, D.C. Significance of immunohistochemistry in breast cancer. World J. Clin. Oncol. 2014, 5, 382. [Google Scholar] [CrossRef]
- Boba, M.; Kołtun, U.; Bobek-Billewicz, B.; Chmielik, E.; Eksner, B.; Olejnik, T. False-negative results of breast core needle biopsies—Retrospective analysis of 988 biopsies. Pol. J. Radiol. 2011, 76, 25–29. [Google Scholar] [PubMed]
- Haynes, B.; Sarma, A.; Nangia-Makker, P.; Shekhar, M.P. Breast cancer complexity: Implications of intratumoral heterogeneity in clinical management. Cancer Metastasis Rev. 2017, 36, 547–555. [Google Scholar] [CrossRef]
- Cajal, S.R.Y.; Sesé, M.; Capdevila, C.; Aasen, T.; De Mattos-Arruda, L.; Diaz-Cano, S.J.; Hernández-Losa, J.; Castellví, J. Clinical implications of intratumor heterogeneity: Challenges and opportunities. J. Mol. Med. 2020, 98, 161–177. [Google Scholar] [CrossRef] [Green Version]
- Garg, P.K.; Deo, S.V.S.; Kumar, R.; Shukla, N.K.; Thulkar, S.; Gogia, A.; Sharma, D.N.; Mathur, S.R. Staging PET–CT Scanning Provides Superior Detection of Lymph Nodes and Distant Metastases than Traditional Imaging in Locally Advanced Breast Cancer. World J. Surg. 2016, 40, 2036–2042. [Google Scholar] [CrossRef] [PubMed]
- Humbert, O.; Riedinger, J.M.; Vrigneaud, J.M.; Kanoun, S.; Dygai-Cochet, I.; Berriolo-Riedinger, A.; Toubeau, M.; Depardon, E.; Lassere, M.; Tisserand, S.; et al. 18F-FDG PET-Derived Tumor Blood Flow Changes After 1 Cycle of Neoadjuvant Chemotherapy Predicts Outcome in Triple-Negative Breast Cancer. J. Nucl. Med. 2016, 57, 1707–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, S.; Alavi, A. PET-Based Personalized Management in Clinical Oncology. PET Clin. 2016, 11, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Magometschnigg, H.F.; Baltzer, P.A.; Fueger, B.; Helbich, T.H.; Karanikas, G.; Dubsky, P.; Rudas, M.; Weber, M.; Pinker, K. Diagnostic accuracy of 18F-FDG PET/CT compared with that of contrast-enhanced MRI of the breast at 3 T. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1656–1665. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Wang, L.; Jiang, X.; She, W.; He, L.; Hu, G. Diagnostic efficacy of 18F-FDG-PET or PET/CT in breast cancer with suspected recurrence. Nucl. Med. Commun. 2016, 37, 1180–1188. [Google Scholar] [CrossRef] [PubMed]
- Pinker, K.; Bogner, W.; Baltzer, P.; Karanikas, G.; Magometschnigg, H.; Brader, P.; Gruber, S.; Bickel, H.; Dubsky, P.; Bago-Horvath, Z.; et al. Improved differentiation of benign and malignant breast tumors with multiparametric 18fluorodeoxyglucose positron emission tomography magnetic resonance imaging: A feasibility study. Clin. Cancer Res. 2014, 20, 3540–3549. [Google Scholar] [CrossRef] [Green Version]
- Visvikis, D.; Hatt, M.; Tixier, F.; Le Rest, C.C. The age of reason for FDG PET image-derived indices. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1670–1672. [Google Scholar] [CrossRef] [Green Version]
- Papp, L.; Rausch, I.; Grahovac, M.; Hacker, M.; Beyer, T. Optimized feature extraction for radiomics analysis of 18 F-FDG-PET imaging. J. Nucl. Med. 2018. [Google Scholar] [CrossRef] [Green Version]
- Castiglioni, I.; Gallivanone, F.; Soda, P.; Avanzo, M.; Stancanello, J.; Aiello, M.; Interlenghi, M.; Salvatore, M. AI-based applications in hybrid imaging: How to build smart and truly multi-parametric decision models for radiomics. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2673–2699. [Google Scholar] [CrossRef]
- Veit-Haibach, P.; Buvat, I.; Herrmann, K. EJNMMI supplement: Bringing AI and radiomics to nuclear medicine. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2627–2629. [Google Scholar] [CrossRef] [Green Version]
- Chicklore, S.; Goh, V.; Siddique, M.; Roy, A.; Marsden, P.K.; Cook, G.J.R. Quantifying tumour heterogeneity in 18F-FDG PET/CT imaging by texture analysis. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 133–140. [Google Scholar] [CrossRef]
- Groheux, D.; Majdoub, M.; Tixier, F.; Le Rest, C.C.; Martineau, A.; Merlet, P.; Espié, M.; de Roquancourt, A.; Hindié, E.; Hatt, M.; et al. Do clinical, histological or immunohistochemical primary tumour characteristics translate into different 18F-FDG PET/CT volumetric and heterogeneity features in stage II/III breast cancer? Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1682–1691. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Wang, X.; Xu, C.; Liu, C.; Zheng, C.; Fulham, M.J.; Feng, D.; Wang, L.; Song, S.; Huang, G. 18F-FDG PET/CT radiomic predictors of pathologic complete response (pCR) to neoadjuvant chemotherapy in breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1116–1126. [Google Scholar] [CrossRef]
- Ha, S.; Park, S.; Bang, J.-I.; Kim, E.-K.; Lee, H.-Y. Metabolic Radiomics for Pretreatment 18F-FDG PET/CT to Characterize Locally Advanced Breast Cancer: Histopathologic Characteristics, Response to Neoadjuvant Chemotherapy, and Prognosis. Sci. Rep. 2017, 7, 1556. [Google Scholar] [CrossRef]
- Antunovic, L.; De Sanctis, R.; Cozzi, L.; Kirienko, M.; Sagona, A.; Torrisi, R.; Tinterri, C.; Santoro, A.; Chiti, A.; Zelic, R.; et al. PET/CT radiomics in breast cancer: Promising tool for prediction of pathological response to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Giacchetti, S.; Moretti, J.-L.; Porcher, R.; Espié, M.; Lehmann-Che, J.; de Roquancourt, A.; Hamy, A.-S.; Cuvier, C.; Vercellino, L.; et al. Correlation of high 18F-FDG uptake to clinical, pathological and biological prognostic factors in breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Koo, H.R.; Park, J.S.; Kang, K.W.; Han, W.; Park, I.A.; Moon, W.K. Correlation between 18F-FDG uptake on PET/CT and prognostic factors in triple-negative breast cancer. Eur. Radiol. 2015, 25, 3314–3321. [Google Scholar] [CrossRef] [PubMed]
- Papp, L.; Spielvogel, C.P.; Rausch, I.; Hacker, M.; Beyer, T. Personalizing Medicine Through Hybrid Imaging and Medical Big Data Analysis. Front. Phys. 2018, 6. [Google Scholar] [CrossRef]
- Vallières, M.; Zwanenburg, A.; Badic, B.; Le Rest, C.C.; Visvikis, D.; Hatt, M. Responsible Radiomics Research for Faster Clinical Translation. J. Nucl. Med. 2018, 59, 189–193. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. A Postreconstruction Harmonization Method for Multicenter Radiomic Studies in PET. J. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef]
- Raudys, S.J.; Jain, A.K. Small sample size effects in statistical pattern recognition: Recommendations for practitioners. IEEE Trans. Pattern Anal. Mach. Intell. 1991, 13, 252–264. [Google Scholar] [CrossRef]
- Luque, A.; Carrasco, A.; Martín, A.; de las Heras, A. The impact of class imbalance in classification performance metrics based on the binary confusion matrix. Pattern Recognit. 2019, 91, 216–231. [Google Scholar] [CrossRef]
- Krawczyk, B. Learning from imbalanced data: Open challenges and future directions. Prog. Artif. Intell. 2016, 5, 221–232. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, C.C.; Hinneburg, A.; Keim, D.A. On the Surprising Behavior of Distance Metrics in High Dimensional Space; Springer: Berlin/Heidelberg, Germany, 2001; pp. 420–434. [Google Scholar]
- Zhao, H.; Wang, Z.; Nie, F. A New Formulation of Linear Discriminant Analysis for Robust Dimensionality Reduction. IEEE Trans. Knowl. Data Eng. 2019, 31, 629–640. [Google Scholar] [CrossRef]
- Liu, F.T.; Ting, K.M.; Zhou, Z.H. Isolation forest. In Proceedings of the IEEE International Conference on Data Mining, ICDM, Pisa, Italy, 15–19 December 2008; pp. 413–422. [Google Scholar] [CrossRef]
- Hadi, A.S.; Imon, A.H.M.R.; Werner, M. Detection of outliers. Wiley Interdiscip. Rev. Comput. Stat. 2009, 1, 57–70. [Google Scholar] [CrossRef]
- Xie, C.; Du, R.; Ho, J.W.K.; Pang, H.H.; Chiu, K.W.H.; Lee, E.Y.P.; Vardhanabhuti, V. Effect of machine learning re-sampling techniques for imbalanced datasets in 18F-FDG PET-based radiomics model on prognostication performance in cohorts of head and neck cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Cysouw, M.C.F.; Jansen, B.H.E.; van de Brug, T.; Oprea-Lager, D.E.; Pfaehler, E.; de Vries, B.M.; van Moorselaar, R.J.A.; Hoekstra, O.S.; Vis, A.N.; Boellaard, R. Machine learning-based analysis of [18F] DCFPyL PET radiomics for risk stratification in primary prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef]
- Leithner, D.; Baltzer, P.A.; Magometschnigg, H.F.; Wengert, G.J.; Karanikas, G.; Helbich, T.H.; Weber, M.; Wadsak, W.; Pinker, K. Quantitative assessment of breast parenchymal uptake on 18F-FDG PET/CT: Correlation with age, background parenchymal enhancement, and amount of fibroglandular tissue on MRI. J. Nucl. Med. 2016, 57, 1518–1522. [Google Scholar] [CrossRef] [Green Version]
- Hoon Tan, P.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 WHO classification of tumours of the breast. Histopathology 2020. [Google Scholar] [CrossRef]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Perry, N.; Broeders, M.; de Wolf, C.; Törnberg, S.; Holland, R.; von Karsa, L. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition—Summary document. Ann. Oncol. 2008, 19, 614–622. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Guideline Update. Arch. Pathol. Lab. Med. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human epidermal growth factor receptor 2 testing in breast cancer: American society of clinical oncology/ college of American pathologists clinical practice guideline focused update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [Green Version]
- Knäusl, B.; Hirtl, A.; Dobrozemsky, G.; Bergmann, H.; Kletter, K.; Dudczak, R.; Georg, D. PET based volume segmentation with emphasis on the iterative TrueX algorithm. Z. Med. Phys. 2012, 22, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, E.; Bettinardi, V.; Thielemans, K.; Gilardi, M.C. Image-based point spread function implementation in a fully 3D OSEM reconstruction algorithm for PET. Phys. Med. Biol. 2010, 55, 4131–4151. [Google Scholar] [CrossRef] [PubMed]
- Hofheinz, F.; Hoff, J.V.D.; Steffen, I.G.; Lougovski, A.; Ego, K.; Amthauer, H.; Apostolova, I. Comparative evaluation of SUV, tumor-to-blood standard uptake ratio (SUR), and dual time point measurements for assessment of the metabolic uptake rate in FDG PET. EJNMMI Res. 2016, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuzé, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A Freeware for Radiomic Feature Calculation in Multimodality Imaging to Accelerate Advances in the Characterization of Tumor Heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [Green Version]
- Gatta, R.; Depeursinge, A.; Ratib, O.; Michielin, O.; Leimgruber, A. Integrating radiomics into holomics for personalised oncology: From algorithms to bedside. Eur. Radiol. Exp. 2020, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Papp, L.; Spielvogel, C.P.; Grubmüller, B.; Grahovac, M.; Krajnc, D.; Ecsedi, B.; Sareshgi, R.A.M.; Mohamad, D.; Hamboeck, M.; Rausch, I.; et al. Supervised machine learning enables non-invasive lesion characterization in primary prostate cancer with [68Ga]Ga-PSMA-11 PET/MRI. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef]
- Papp, L.; Pötsch, N.; Grahovac, M.; Schmidbauer, V.; Woehrer, A.; Preusser, M.; Mitterhauser, M.; Kiesel, B.; Wadsak, W.; Beyer, T.; et al. Glioma Survival Prediction with Combined Analysis of In Vivo 11 C-MET PET Features, Ex Vivo Features, and Patient Features by Supervised Machine Learning. J. Nucl. Med. 2018, 59, 892–899. [Google Scholar] [CrossRef] [Green Version]
- Lacroix, M.; Frouin, F.; Dirand, A.-S.; Nioche, C.; Orlhac, F.; Bernaudin, J.-F.; Brillet, P.-Y.; Buvat, I. Correction for Magnetic Field Inhomogeneities and Normalization of Voxel Values Are Needed to Better Reveal the Potential of MR Radiomic Features in Lung Cancer. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef] [Green Version]
- Elhassan, T.; Aljurf, M.; Al-Mohanna, F.; Shoukri, M.M. Classification of Imbalance Data Using Tomek Link (T-Link) Combined with Random Under-sampling (RUS) as A Data Reduction Method Sampling-based Methods Basic Sampling Methods. J. Inform. Data Min. 2016, 1, 1–12. [Google Scholar]
- Marcano-Cedeno, A.; Quintanilla-Dominguez, J.; Cortina-Januchs, M.G.; Andina, D. Feature selection using Sequential Forward Selection and classification applying Artificial Metaplasticity Neural Network. In Proceedings of the IECON 2010—36th Annual Conference on IEEE Industrial Electronics Society, Glendale, AZ, USA, 7–10 November 2010; Institute of Electrical and Electronics Engineers (IEEE): Los Alamitos, CA, USA, 2010; pp. 2845–2850. [Google Scholar] [CrossRef]
- Vanaja, S.; Kumar, K.R. Analysis of Feature Selection Algorithms on Classification: A Survey. Int. J. Comput. Appl. 2014, 96, 29–35. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-Sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Nguyen, H.M.; Cooper, E.W.; Kamei, K. Borderline over-sampling for imbalanced data classification. Int. J. Knowl. Eng. Soft Data Paradig. 2011, 3, 4–21. [Google Scholar] [CrossRef]
- Barua, S.; Islam, M.M.; Yao, X.; Murase, K. MWMOTE—Majority weighted minority oversampling technique for imbalanced data set learning. IEEE Trans. Knowl. Data Eng. 2014, 26, 405–425. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Leijenaar, R.T.H.; van Elmpt, W.; Reymen, B.; Oberije, C.; Monshouwer, R.; Bussink, J.; Brink, C.; Hansen, O.; Lambin, P. Survival prediction of non-small cell lung cancer patients using radiomics analyses of cone-beam CT images. Radiother. Oncol. 2017, 123, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Leithner, D.; Mayerhoefer, M.E.; Martinez, D.F.; Jochelson, M.S.; Morris, E.A.; Thakur, S.B.; Pinker, K. Non-Invasive Assessment of Breast Cancer Molecular Subtypes with Multiparametric Magnetic Resonance Imaging Radiomics. J. Clin. Med. 2020, 9, 1853. [Google Scholar] [CrossRef] [PubMed]
- Leithner, D.; Horvat, J.V.; Marino, M.A.; Bernard-Davila, B.; Jochelson, M.S.; Ochoa-Albiztegui, R.E.; Martinez, D.F.; Morris, E.A.; Thakur, S.; Pinker, K. Radiomic signatures with contrast-enhanced magnetic resonance imaging for the assessment of breast cancer receptor status and molecular subtypes: Initial results. Breast Cancer Res. 2019, 21, 106. [Google Scholar] [CrossRef] [Green Version]
- Leithner, D.; Bernard-Davila, B.; Martinez, D.F.; Horvat, J.V.; Jochelson, M.S.; Marino, M.A.; Avendano, D.; Ochoa-Albiztegui, R.E.; Sutton, E.J.; Morris, E.A.; et al. Radiomic Signatures Derived from Diffusion-Weighted Imaging for the Assessment of Breast Cancer Receptor Status and Molecular Subtypes. Mol. Imaging Biol. 2020, 22, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Beyer, T.; Townsend, D.W.; Brun, T.; Kinahan, P.; Charron, M.; Roddy, R.; Jerin, J.; Young, J.; Byars, L.; Nutt, R. A Combined PET/CT scanner for clinical oncology. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2000, 41, 1369–1379. [Google Scholar]
- McGuire, A.; Brown, J.; Malone, C.; McLaughlin, R.; Kerin, M. Effects of Age on the Detection and Management of Breast Cancer. Cancers 2015, 7, 908–929. [Google Scholar] [CrossRef] [PubMed]
- Ou, X.; Zhang, J.; Wang, J.; Pang, F.; Wang, Y.; Wei, X.; Ma, X. Radiomics based on 18 F-FDG PET/CT could differentiate breast carcinoma from breast lymphoma using machine-learning approach: A preliminary study. Cancer Med. 2020, 9, 496–506. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.-Y.; Franc, B.L.; Harnish, R.J.; Liu, G.; Mitra, D.; Copeland, T.P.; Arasu, V.A.; Kornak, J.; Jones, E.F.; Behr, S.C.; et al. Exploration of PET and MRI radiomic features for decoding breast cancer phenotypes and prognosis. NPJ Breast Cancer 2018, 4, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Lu, J.; Gao, C.; Zeng, J.; Zhou, C.; Lai, X.; Cai, W.; Xu, M. Predicting the response to neoadjuvant chemotherapy for breast cancer: Wavelet transforming radiomics in MRI. BMC Cancer 2020, 20, 100. [Google Scholar] [CrossRef]
- Xiong, H.; Gaurav, P.; Steinbach, M.; Vipin, K. Enhancing data analysis with noise removal. IEEE Trans. Knowl. Data Eng. 2006, 18, 304–319. [Google Scholar] [CrossRef] [Green Version]
- Nazari, Z.; Nazari, M.; Sayed, M.; Danish, S. Evaluation of Class Noise Impact on Performance of Machine Learning Algorithms. IJCSNS Int. J. Comput. Sci. Netw. Secur. 2018, 18, 149. [Google Scholar]
- Zhu, X.; Wu, X. Class Noise vs. Attribute Noise: A Quantitative Study of Their Impacts. Artif. Intell. Rev. 2004, 22, 177–210. [Google Scholar] [CrossRef]
- Moy, L.; Noz, M.E.; Maguire, G.Q.; Ponzo, F.; Deans, A.E.; Murphy-Walcott, A.D.; Kramer, E.L. Prone MammoPET Acquisition Improves the Ability to Fuse MRI and PET Breast Scans. Clin. Nucl. Med. 2007, 32, 194–198. [Google Scholar] [CrossRef]
- Imbriaco, M.; Caprio, M.G.; Limite, G.; Pace, L.; De Falco, T.; Capuano, E.; Salvatore, M. Dual-Time-Point 18 F-FDG PET/CT Versus Dynamic Breast MRI of Suspicious Breast Lesions. Am. J. Roentgenol. 2008, 191, 1323–1330. [Google Scholar] [CrossRef]
- Misra, S.; Wu, Y. Chapter 10—Machine learning assisted segmentation of scanning electron microscopy images of organic-rich shales with feature extraction and feature ranking. In Machine Learning for Subsurface Characterization; Misra, S., Li, H., He, J., Eds.; Gulf Professional Publishing: Houston, TX, USA, 2020; pp. 289–314. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics (n = 170) | Value |
|---|---|
| Age (years), median (IQR) | 57.6 (18–86) |
| Lesion volume (cm3), median (IQR) | 12.8 (6.2–26.9) |
| Malignancy | n (%) |
| Malignant | 132 (78) |
| Benign | 38 (22) |
| Estrogen (ER) | n (%) |
| − | 17 (10) |
| + | 88 (52) |
| NA | 65 (38) |
| Progesterone (PR) | n (%) |
| − | 27 (16) |
| + | 78 (46) |
| NA | 65 (38) |
| Ki-67 | n (%) |
| − | 26 (15) |
| + | 73 (43) |
| NA | 71 (42) |
| HER2 | n (%) |
| − | 84 (49) |
| + | 22 (13) |
| NA | 64 (38) |
| Triple negative | n (%) |
| Yes | 11 (6) |
| No | 95 (56) |
| NA | 64 (38) |
| Luminal A/B | n (%) |
| A | 14 (8) |
| B | 81 (48) |
| NA | 75 (44) |
| Model | Data Preprocessing | SENS | SPEC | NPV | PPV | ACC | AUC |
|---|---|---|---|---|---|---|---|
| ER | No | 83 | 40 | 70 | 58 | 62 | 0.63 |
| Yes | 82 | 56↑ | 78↑ | 65↑ | 69↑ | 0.68↑ | |
| PR | No | 74 | 36 | 58 | 54 | 55 | 0.56 |
| Yes | 78↑ | 35 | 61↑ | 54 | 56↑ | 0.55 | |
| Ki-67 | No | 68 | 39 | 55 | 53 | 53 | 0.63 |
| Yes | 65 | 45↑ | 56↑ | 54↑ | 55↑ | 0.65↑ | |
| HER2 | No | 17 | 84 | 50 | 51 | 50 | 0.46 |
| Yes | 17 | 84 | 50 | 51 | 50 | 0.46 | |
| Luminal A/B | No | 17 | 87 | 51 | 57 | 52 | 0.62 |
| Yes | 16 | 89↑ | 51 | 59↑ | 53↑ | 0.52 | |
| Triple negative | No | 57 | 94 | 68 | 90 | 75 | 0.76 |
| Yes | 85↑ | 78 | 84↑ | 79 | 82↑ | 0.82↑ | |
| Breast Cancer Detection (Malignant vs. Benign) | No | 80 | 59 | 75 | 66 | 69 | 0.71 |
| Yes | 80 | 78↑ | 79↑ | 78↑ | 80↑ | 0.81↑ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krajnc, D.; Papp, L.; Nakuz, T.S.; Magometschnigg, H.F.; Grahovac, M.; Spielvogel, C.P.; Ecsedi, B.; Bago-Horvath, Z.; Haug, A.; Karanikas, G.; et al. Breast Tumor Characterization Using [18F]FDG-PET/CT Imaging Combined with Data Preprocessing and Radiomics. Cancers 2021, 13, 1249. https://doi.org/10.3390/cancers13061249
Krajnc D, Papp L, Nakuz TS, Magometschnigg HF, Grahovac M, Spielvogel CP, Ecsedi B, Bago-Horvath Z, Haug A, Karanikas G, et al. Breast Tumor Characterization Using [18F]FDG-PET/CT Imaging Combined with Data Preprocessing and Radiomics. Cancers. 2021; 13(6):1249. https://doi.org/10.3390/cancers13061249
Chicago/Turabian StyleKrajnc, Denis, Laszlo Papp, Thomas S. Nakuz, Heinrich F. Magometschnigg, Marko Grahovac, Clemens P. Spielvogel, Boglarka Ecsedi, Zsuzsanna Bago-Horvath, Alexander Haug, Georgios Karanikas, and et al. 2021. "Breast Tumor Characterization Using [18F]FDG-PET/CT Imaging Combined with Data Preprocessing and Radiomics" Cancers 13, no. 6: 1249. https://doi.org/10.3390/cancers13061249
APA StyleKrajnc, D., Papp, L., Nakuz, T. S., Magometschnigg, H. F., Grahovac, M., Spielvogel, C. P., Ecsedi, B., Bago-Horvath, Z., Haug, A., Karanikas, G., Beyer, T., Hacker, M., Helbich, T. H., & Pinker, K. (2021). Breast Tumor Characterization Using [18F]FDG-PET/CT Imaging Combined with Data Preprocessing and Radiomics. Cancers, 13(6), 1249. https://doi.org/10.3390/cancers13061249