
Enucleation Is a Feasible Procedure for Well-Differentiated pNEN—A Matched Pair Analysis

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Identification
2.2. Clinical Data and Surgical Approach
2.3. Follow-Up
2.4. Matched Pair Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Matched Cohort
3.2. Pathology Data
3.3. Perioperative Outcome
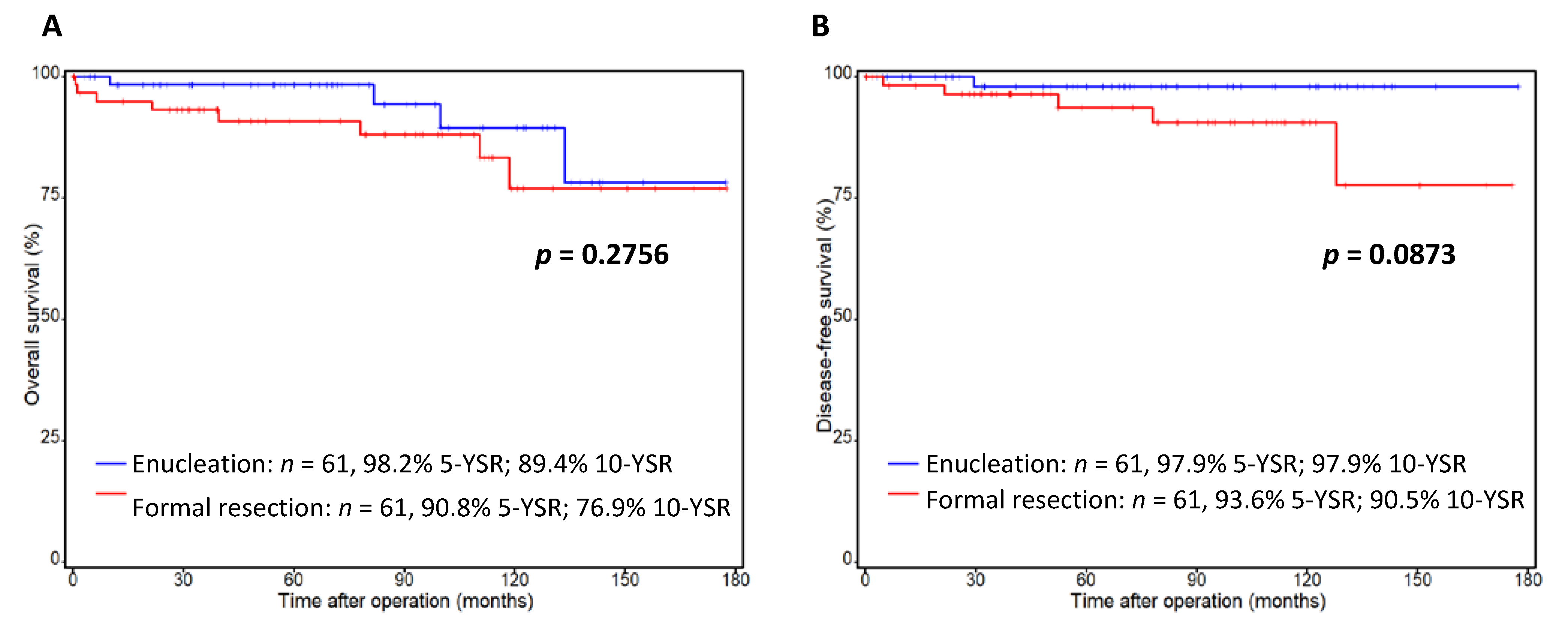
3.4. Long-Term Outcomes and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modlin, I.M.; Oberg, K.; Chung, D.C.; Jensen, R.T.; de Herder, W.W.; Thakker, R.V.; Caplin, M.; Delle Fave, G.; Kaltsas, G.A.; Krenning, E.P.; et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008, 9, 61–72. [Google Scholar] [CrossRef]
- Lawrence, B.; Gustafsson, B.I.; Chan, A.; Svejda, B.; Kidd, M.; Modlin, I.M. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol. Metab. Clin. N. Am. 2011, 40, 1–18, vii. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Tomlinson, J.S.; Merkow, R.P.; Stewart, A.K.; Ko, C.Y.; Talamonti, M.S.; Bentrem, D.J. Clinicopathologic features and treatment trends of pancreatic neuroendocrine tumors: Analysis of 9821 patients. J. Gastrointest Surg. 2007, 11, 1460–1467; discussion 1467–1469. [Google Scholar] [CrossRef] [Green Version]
- Strobel, O.; Buchler, M.W. Pancreatic Ductal Adenocarcinoma: A New TNM Staging System Is Needed! Ann. Surg. 2017, 266, e109–e110. [Google Scholar] [CrossRef]
- Vather, R.; Sammour, T.; Kahokehr, A.; Connolly, A.B.; Hill, A.G. Lymph node evaluation and long-term survival in Stage II and Stage III colon cancer: A national study. Ann. Surg. Oncol. 2009, 16, 585–593. [Google Scholar] [CrossRef]
- Bartsch, D.K.; Albers, M.; Knoop, R.; Kann, P.H.; Fendrich, V.; Waldmann, J. Enucleation and limited pancreatic resection provide long-term cure for insulinoma in multiple endocrine neoplasia type 1. Neuroendocrinology 2013, 98, 290–298. [Google Scholar] [CrossRef]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Kloppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [Green Version]
- Howe, J.R.; Merchant, N.B.; Conrad, C.; Keutgen, X.M.; Hallet, J.; Drebin, J.A.; Minter, R.M.; Lairmore, T.C.; Tseng, J.F.; Zeh, H.J.; et al. The North American Neuroendocrine Tumor Society Consensus Paper on the Surgical Management of Pancreatic Neuroendocrine Tumors. Pancreas 2020, 49, 1–33. [Google Scholar] [CrossRef]
- Bartsch, D.K.; Langer, P.; Rothmund, M. Surgical aspects of gastrinoma in multiple endocrine neoplasia type 1. Wien Klin Wochenschr 2007, 119, 602–608. [Google Scholar] [CrossRef]
- Fendrich, V.; Langer, P.; Waldmann, J.; Bartsch, D.K.; Rothmund, M. Management of sporadic and multiple endocrine neoplasia type 1 gastrinomas. Br. J. Surg. 2007, 94, 1331–1341. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, D.K.; Waldmann, J.; Fendrich, V.; Boninsegna, L.; Lopez, C.L.; Partelli, S.; Falconi, M. Impact of lymphadenectomy on survival after surgery for sporadic gastrinoma. Br. J. Surg. 2012, 99, 1234–1240. [Google Scholar] [CrossRef] [PubMed]
- Verdauungs- und Stoffwechselkrankheiten (DGVS); Netzwerk Neuroendokrine Tumoren (NeT) e.V. (Patientenvertretung); Bundesorganisation Selbsthilfe NeuroEndokrine Tumoren e.V. (NET-sgh) (Patientenvertretung); Deutsche Gesellschaft für Hämatologie und Medizinische Onkologie e.V. (DGHO), und Arbeitsgemeinschaft Internistische Onkologie (AIO) der Deutschen Krebsgesellschaft e.V.; Deutsche Gesellschaft für Allgemein- und Viszeralchirurgie e.V. (DGAV); Deutsche Gesellschaft für Chirurgie (DGCH); Deutsche Gesellschaft für Endoskopie und Bildgebende Verfahren (DGEBV); Deutsche Gesellschaft für Nuklearmedizin e.V. (DGNM); Deutsche Gesellschaft für Innere Medizin (DGIM); Deutsche Gesellschaft für Endokrinologie (DGE); et al. Practice guideline neuroendocrine tumors—AWMF-Reg. 021-27. Z Gastroenterol. 2018, 56, 583–681. [Google Scholar] [CrossRef] [Green Version]
- Kuo, E.J.; Salem, R.R. Population-level analysis of pancreatic neuroendocrine tumors 2 cm or less in size. Ann. Surg. Oncol. 2013, 20, 2815–2821. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Talamonti, M.S.; Tomlinson, J.S.; Stewart, A.K.; Winchester, D.P.; Ko, C.Y.; Bentrem, D.J. Prognostic score predicting survival after resection of pancreatic neuroendocrine tumors: Analysis of 3851 patients. Ann. Surg. 2008, 247, 490–500. [Google Scholar] [CrossRef]
- Fischer, L.; Bergmann, F.; Schimmack, S.; Hinz, U.; Prieß, S.; Müller-Stich, B.P.; Werner, J.; Hackert, T.; Büchler, M.W. Outcome of surgery for pancreatic neuroendocrine neoplasms. BJS 2014, 101, 1405–1412. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, M.; Ji, S.; Luo, G.; Xu, W.; Liu, W.; Hu, Q.; Sun, Q.; Ye, Z.; Qin, Y.; et al. Prognostic Value and Clinical Predictors of Lymph Node Metastases in Pancreatic Neuroendocrine Tumors. Pancreas 2020, 49, 381–386. [Google Scholar] [CrossRef]
- Heidsma, C.M.; Tsilimigras, D.I.; van Dieren, S.; Rocha, F.; Abbott, D.E.; Fields, R.; Smith, P.M.; Poultsides, G.A.; Cho, C.; Dillhoff, M.; et al. Indications and outcomes of enucleation versus formal pancreatectomy for pancreatic neuroendocrine tumors. HPB 2021, 23, 413–421. [Google Scholar] [CrossRef]
- Teo, R.; Goh, B.K.P.; Tai, D.W.M.; Allen, J.C.; Lim, T.K.H.; Hwang, J.S.G.; Tan, D.M.; Lee, S.Y.; Chan, C.Y.; Cheow, P.C.; et al. Validation and comparison between current prognostication systems for pancreatic neuroendocrine neoplasms: A single-institution experience with 176 patients. Surgery 2017, 161, 1235–1245. [Google Scholar] [CrossRef]
- Nießen, A.; Schimmack, S.; Sandini, M.; Fliegner, D.; Hinz, U.; Lewosinska, M.; Hackert, T.; Büchler, M.W.; Strobel, O. C-reactive protein independently predicts survival in pancreatic neuroendocrine neoplasms. Sci. Rep. 2021, 11, 23768. [Google Scholar] [CrossRef]
- Finkelstein, P.; Sharma, R.; Picado, O.; Gadde, R.; Stuart, H.; Ripat, C.; Livingstone, A.S.; Sleeman, D.; Merchant, N.; Yakoub, D. Pancreatic Neuroendocrine Tumors (panNETs): Analysis of Overall Survival of Nonsurgical Management Versus Surgical Resection. J. Gastrointest Surg. 2017, 21, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Jutric, Z.; Grendar, J.; Hoen, H.M.; Cho, S.W.; Cassera, M.A.; Newell, P.H.; Hammill, C.W.; Hansen, P.D.; Wolf, R.F. Regional Metastatic Behavior of Nonfunctional Pancreatic Neuroendocrine Tumors: Impact of Lymph Node Positivity on Survival. Pancreas 2017, 46, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Heckler, M.; Mihaljevic, A.L.; Probst, P.; Klaiber, U.; Heger, U.; Schimmack, S.; Buchler, M.W.; Hackert, T. Systematic Review and Metaanalysis of Lymph Node Metastases of Resected Pancreatic Neuroendocrine Tumors. Ann. Surg. Oncol. 2021, 28, 1614–1624. [Google Scholar] [CrossRef] [PubMed]
- Partelli, S.; Gaujoux, S.; Boninsegna, L.; Cherif, R.; Crippa, S.; Couvelard, A.; Scarpa, A.; Ruszniewski, P.; Sauvanet, A.; Falconi, M. Pattern and clinical predictors of lymph node involvement in nonfunctioning pancreatic neuroendocrine tumors (NF-PanNETs). JAMA Surg. 2013, 148, 932–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaujoux, S.; Partelli, S.; Maire, F.; D’Onofrio, M.; Larroque, B.; Tamburrino, D.; Sauvanet, A.; Falconi, M.; Ruszniewski, P. Observational study of natural history of small sporadic nonfunctioning pancreatic neuroendocrine tumors. J. Clin. Endocrinol. Metab. 2013, 98, 4784–4789. [Google Scholar] [CrossRef] [Green Version]
- Hill, J.S.; McPhee, J.T.; McDade, T.P.; Zhou, Z.; Sullivan, M.E.; Whalen, G.F.; Tseng, J.F. Pancreatic neuroendocrine tumors: The impact of surgical resection on survival. Cancer 2009, 115, 741–751. [Google Scholar] [CrossRef]
- Partelli, S.; Bartsch, D.K.; Capdevila, J.; Chen, J.; Knigge, U.; Niederle, B.; Nieveen van Dijkum, E.J.M.; Pape, U.F.; Pascher, A.; Ramage, J.; et al. ENETS Consensus Guidelines for Standard of Care in Neuroendocrine Tumours: Surgery for Small Intestinal and Pancreatic Neuroendocrine Tumours. Neuroendocrinology 2017, 105, 255–265. [Google Scholar] [CrossRef]
- Niederle, B.; Selberherr, A.; Bartsch, D.K.; Brandi, M.L.; Doherty, G.M.; Falconi, M.; Goudet, P.; Halfdanarson, T.R.; Ito, T.; Jensen, R.T.; et al. Multiple Endocrine Neoplasia Type 1 and the Pancreas: Diagnosis and Treatment of Functioning and Non-Functioning Pancreatic and Duodenal Neuroendocrine Neoplasia within the MEN1 Syndrome—An International Consensus Statement. Neuroendocrinology 2021, 111, 609–630. [Google Scholar] [CrossRef]
- Assi, H.A.; Mukherjee, S.; Kunz, P.L.; Machiorlatti, M.; Vesely, S.; Pareek, V.; Hatoum, H. Surgery Versus Surveillance for Well-Differentiated, Nonfunctional Pancreatic Neuroendocrine Tumors: An 11-Year Analysis of the National Cancer Database. Oncologist 2020, 25, e276–e283. [Google Scholar] [CrossRef] [Green Version]
- Chivukula, S.V.; Tierney, J.F.; Hertl, M.; Poirier, J.; Keutgen, X.M. Operative resection in early stage pancreatic neuroendocrine tumors in the United States: Are we over- or undertreating patients? Surgery 2020, 167, 180–186. [Google Scholar] [CrossRef]
- Hackert, T.; Hinz, U.; Fritz, S.; Strobel, O.; Schneider, L.; Hartwig, W.; Buchler, M.W.; Werner, J. Enucleation in pancreatic surgery: Indications, technique, and outcome compared to standard pancreatic resections. Langenbecks Arch. Surg. 2011, 396, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Zhu, J.; Peng, L.; Hong, L.; Sun, G.; Li, Y. The role of central pancreatectomy in pancreatic surgery: A systematic review and meta-analysis. HPB 2018, 20, 896–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strobel, O.; Cherrez, A.; Hinz, U.; Mayer, P.; Kaiser, J.; Fritz, S.; Schneider, L.; Klauss, M.; Büchler, M.W.; Hackert, T. Risk of pancreatic fistula after enucleation of pancreatic tumours. BJS 2015, 102, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Beger, H.G.; Siech, M.; Poch, B.; Mayer, B.; Schoenberg, M.H. Limited surgery for benign tumours of the pancreas: A systematic review. World J. Surg. 2015, 39, 1557–1566. [Google Scholar] [CrossRef] [PubMed]
- Jilesen, A.P.; van Eijck, C.H.; Busch, O.R.; van Gulik, T.M.; Gouma, D.J.; van Dijkum, E.J. Postoperative Outcomes of Enucleation and Standard Resections in Patients with a Pancreatic Neuroendocrine Tumor. World J. Surg. 2016, 40, 715–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grenacher, L.; Klauss, M. Computed tomography of pancreatic tumors. Der Radiol. 2009, 49, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Falconi, M.; Bartsch, D.K.; Eriksson, B.; Kloppel, G.; Lopes, J.M.; O’Connor, J.M.; Salazar, R.; Taal, B.G.; Vullierme, M.P.; O’Toole, D.; et al. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms of the digestive system: Well-differentiated pancreatic non-functioning tumors. Neuroendocrinology 2012, 95, 120–134. [Google Scholar] [CrossRef]
- Yamada, S.; Fujii, T.; Suzuki, K.; Inokawa, Y.; Kanda, M.; Nakayama, G.; Sugimoto, H.; Koike, M.; Nomoto, S.; Fujiwara, M.; et al. Preoperative Identification of a Prognostic Factor for Pancreatic Neuroendocrine Tumors Using Multiphase Contrast-Enhanced Computed Tomography. Pancreas 2016, 45, 198–203. [Google Scholar] [CrossRef]
- Yano, M.; Misra, S.; Carpenter, D.H.; Salter, A.; Hildebolt, C.F. Pancreatic Neuroendocrine Tumors: Computed Tomography Enhancement, But Not Histological Grade, Correlates with Tumor Aggression. Pancreas 2017, 46, 1366–1372. [Google Scholar] [CrossRef]
- Ricci, C.; Mosconi, C.; Ingaldi, C.; Vara, G.; Verna, M.; Pettinari, I.; Alberici, L.; Campana, D.; Ambrosini, V.; Minni, F.; et al. The 3-Dimensional-Computed Tomography Texture Is Useful to Predict Pancreatic Neuroendocrine Tumor Grading. Pancreas 2021, 50, 1392–1399. [Google Scholar] [CrossRef]
- D’Onofrio, M.; Ciaravino, V.; Cardobi, N.; De Robertis, R.; Cingarlini, S.; Landoni, L.; Capelli, P.; Bassi, C.; Scarpa, A. CT Enhancement and 3D Texture Analysis of Pancreatic Neuroendocrine Neoplasms. Sci. Rep. 2019, 9, 2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belousova, E.; Karmazanovsky, G.; Kriger, A.; Kalinin, D.; Mannelli, L.; Glotov, A.; Karelskaya, N.; Paklina, O.; Kaldarov, A. Contrast-enhanced MDCT in patients with pancreatic neuroendocrine tumours: Correlation with histological findings and diagnostic performance in differentiation between tumour grades. Clin. Radiol. 2017, 72, 150–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassi, C.; Dervenis, C.; Butturini, G.; Fingerhut, A.; Yeo, C.; Izbicki, J.; Neoptolemos, J.; Sarr, M.; Traverso, W.; Buchler, M. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surgery 2005, 138, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu Hilal, M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Bosman, F.T.; World Health Organization; International Agency for Research on Cancer. WHO Classification of Tumours of the Digestive System, 4th ed.; International Agency for Research on Cancer: Lyon, French, 2010; 417p. [Google Scholar]
- Brierley, J.; Gospodarowicz, M.K.; Wittekind, C.; Union for International Cancer, C. TNM Classification of Malignant Tumours; John Wiley & Sons, Ltd: Chichester, UK, 2017. [Google Scholar]
- Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J. WHO Classification of Tumours of Endocrine Organs; International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Hansen, B.B.; Klopfer, S.O. Optimal full matching and related designs via network flows. J. Comput. Graph. Stat. 2006, 15, 609–627. [Google Scholar] [CrossRef] [Green Version]
- Huttner, F.J.; Koessler-Ebs, J.; Hackert, T.; Ulrich, A.; Buchler, M.W.; Diener, M.K. Meta-analysis of surgical outcome after enucleation versus standard resection for pancreatic neoplasms. Br. J. Surg. 2015, 102, 1026–1036. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhao, M.; Wu, L.; Ye, F.; Si, X. Short- and long-term outcomes after enucleation of pancreatic tumors: An evidence-based assessment. Pancreatology 2016, 16, 1092–1098. [Google Scholar] [CrossRef]
- Kaiser, J.; Fritz, S.; Klauss, M.; Bergmann, F.; Hinz, U.; Strobel, O.; Schneider, L.; Buchler, M.W.; Hackert, T. Enucleation: A treatment alternative for branch duct intraductal papillary mucinous neoplasms. Surgery 2017, 161, 602–610. [Google Scholar] [CrossRef]
- Beane, J.D.; Borrebach, J.D.; Billderback, A.; Onuma, A.E.; Adam, M.A.; Zureikat, A.H.; Pitt, H.A. Small pancreatic neuroendocrine tumors: Resect or enucleate? Am. J. Surg. 2021, 222, 29–34. [Google Scholar] [CrossRef]
- Weilin, M.; Xu, H.; Yang, L.; Wenqi, C.; Huanyu, W.; Wentao, Z.; Dayong, J.; Wenchuan, W.; Dansong, W.; Tiantao, K.; et al. Propensity score-matched analysis of clinical outcome after enucleation versus regular pancreatectomy in patients with small non-functional pancreatic neuroendocrine tumors. Pancreatology 2020, 20, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Sallinen, V.; Le Large, T.Y.; Galeev, S.; Kovalenko, Z.; Tieftrunk, E.; Araujo, R.; Ceyhan, G.O.; Gaujoux, S. Surveillance strategy for small asymptomatic non-functional pancreatic neuroendocrine tumors—A systematic review and meta-analysis. HPB 2017, 19, 310–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, S.; Viera, F.T.; Ghittoni, G.; Cobianchi, L.; Rosa, L.L.; Siciliani, L.; Bortolotto, C.; Veronese, L.; Vercelli, A.; Gallotti, A.; et al. Radiofrequency ablation of pancreatic neuroendocrine tumors: A pilot study of feasibility, efficacy, and safety. Pancreas 2014, 43, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Marx, M.; Godat, S.; Caillol, F.; Poizat, F.; Ratone, J.-P.; Pesenti, C.; Schoepfer, A.; Hoibian, S.; Dahel, Y.; Giovannini, M. Management of non-functional pancreatic neuroendocrine tumors by endoscopic ultrasound-guided radiofrequency ablation: Retrospective study in two tertiary centers. Dig. Endosc. 2021. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Barthet, M.; Giovannini, M.; Lesavre, N.; Boustiere, C.; Napoleon, B.; Koch, S.; Gasmi, M.; Vanbiervliet, G.; Gonzalez, J.M. Endoscopic ultrasound-guided radiofrequency ablation for pancreatic neuroendocrine tumors and pancreatic cystic neoplasms: A prospective multicenter study. Endoscopy 2019, 51, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Krampitz, G.W.; Norton, J.A.; Poultsides, G.A.; Visser, B.C.; Sun, L.; Jensen, R.T. Lymph nodes and survival in pancreatic neuroendocrine tumors. Arch. Surg. 2012, 147, 820–827. [Google Scholar] [CrossRef] [Green Version]
- Hashim, Y.M.; Trinkaus, K.M.; Linehan, D.C.; Strasberg, S.S.; Fields, R.C.; Cao, D.; Hawkins, W.G. Regional lymphadenectomy is indicated in the surgical treatment of pancreatic neuroendocrine tumors (PNETs). Ann. Surg. 2014, 259, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Curran, T.; Pockaj, B.A.; Gray, R.J.; Halfdanarson, T.R.; Wasif, N. Importance of lymph node involvement in pancreatic neuroendocrine tumors: Impact on survival and implications for surgical resection. J. Gastrointest Surg. 2015, 19, 152–160, discussion 160. [Google Scholar] [CrossRef]
- Conrad, C.; Kutlu, O.C.; Dasari, A.; Chan, J.A.; Vauthey, J.N.; Adams, D.B.; Kim, M.; Fleming, J.B.; Katz, M.H.; Lee, J.E. Prognostic Value of Lymph Node Status and Extent of Lymphadenectomy in Pancreatic Neuroendocrine Tumors Confined To and Extending Beyond the Pancreas. J. Gastrointest Surg. 2016, 20, 1966–1974. [Google Scholar] [CrossRef]
- Gratian, L.; Pura, J.; Dinan, M.; Roman, S.; Reed, S.; Sosa, J.A. Impact of extent of surgery on survival in patients with small nonfunctional pancreatic neuroendocrine tumors in the United States. Ann. Surg. Oncol. 2014, 21, 3515–3521. [Google Scholar] [CrossRef] [Green Version]
- Slagter, A.E.; Ryder, D.; Chakrabarty, B.; Lamarca, A.; Hubner, R.A.; Mansoor, W.; O’Reilly, D.A.; Fulford, P.E.; Klumpen, H.J.; Valle, J.W.; et al. Prognostic factors for disease relapse in patients with neuroendocrine tumours who underwent curative surgery. Surg. Oncol. 2016, 25, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Pomianowska, E.; Gladhaug, I.P.; Grzyb, K.; Rosok, B.I.; Edwin, B.; Bergestuen, D.S.; Mathisen, O. Survival following resection of pancreatic endocrine tumors: Importance of R-status and the WHO and TNM classification systems. Scand. J. Gastroenterol. 2010, 45, 971–979. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Enucleation n = 61 | Formal Resection n = 61 | p-Value |
|---|---|---|---|
| Age, Median (IQR) | 61 (50–68) | 62 (52–67) | 0.8840 |
| Median size (IQR) [cm] | 1.2 (0.9–2.0) | 1.2 (0.8–1.8) | 0.8395 |
| Grading (WHO 2017) | 1.0 | ||
| G1 | 53 (86.9%) | 53 (86.9%) | |
| G2 | 8 (13.1%) | 8 (13.1%) | |
| Sex [M:F] | 20:41 | 30:31 | 0.0971 |
| BMI (2 missing values), Median (IQR) | 26 (23–29) | 27 (25–29) | 0.1106 |
| ASA classification (5 missing values) | 0.6720 | ||
| I | 3 (5.1%) | 5 (8.6%) | |
| II | 41 (69.5%) | 41 (70.7%) | |
| III | 15 (25.4%) | 12 (20.7%) | |
| Localization | 0.2689 | ||
| Head | 29 (47.5%) | 30 (49.2%) | |
| Body | 23 (37.7%) | 15 (24.6%) | |
| Tail | 9 (14.8%) | 16 (26.2%) | |
| Laparoscopic/robotic surgery | 8 (13.1%) | 11 (18.0%) | 0.6185 |
| Length of operation [min.], Median (IQR) | 128 (95–170) | 263 (172–337) | <0.0001 * |
| pT (TNM 8th) | 1.0 | ||
| T1 | 44 (72.1%) | 45 (73.8%) | |
| T2 | 15 (24.6%) | 14 (22.9%) | |
| T3 | 2 (3.3%) | 2 (3.3%) | |
| R classification | 0.0356 * | ||
| R0 | 45 (73.8%) | 55 (90.2%) | |
| R1 | 9 (14.8%) | 5 (8.2%) | |
| RX | 7 (11.5%) | 1 (1.6%) | |
| pN (TNM 8th) | <0.0001 * | ||
| N0 | 17 (27.9%) | 57 (93.4%) | |
| N1 | 2 (3.3%) | 4 (6.6%) | |
| NX | 42 (68.8%) | 0 (0.0%) |
| Parameter | Enucleation n = 61 | Formal Resection n = 61 | p-Value |
|---|---|---|---|
| 30-day mortality | 0 (0%) | 1 (1.6%) | 1.0 |
| POPF | 0.3295 | ||
| BL (biochemical leak) | 5 (8.2%) | 4 (6.6%) | |
| B | 8 (13.1%) | 12 (19.7%) | |
| C | 3 (4.9%) | 0 (0.0%) | |
| POPF B/C | 11 (18.0%) | 12 (19.7%) | 1.0 |
| Clavien−Dindo classification | 0.5189 | ||
| 0/I/II | 49 (80.3%) | 45 (73.8%) | |
| ≥IIIa | 12 (19.7%) | 16 (26.2%) | |
| Length of hospital stay (days), Median (IQR) | 8 (7–11) | 10 (8–17) | 0.0652 |
| Postoperative diabetes mellitus (7 missing values) | 1 (1.8%) | 12 (20.7%) | 0.0020 * |
| Readmission (1 missing value) | 7 (11.5%) | 9 (15.0%) | 0.6022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nießen, A.; Bechtiger, F.A.; Hinz, U.; Lewosinska, M.; Billmann, F.; Hackert, T.; Büchler, M.W.; Schimmack, S. Enucleation Is a Feasible Procedure for Well-Differentiated pNEN—A Matched Pair Analysis. Cancers 2022, 14, 2570. https://doi.org/10.3390/cancers14102570
Nießen A, Bechtiger FA, Hinz U, Lewosinska M, Billmann F, Hackert T, Büchler MW, Schimmack S. Enucleation Is a Feasible Procedure for Well-Differentiated pNEN—A Matched Pair Analysis. Cancers. 2022; 14(10):2570. https://doi.org/10.3390/cancers14102570
Chicago/Turabian StyleNießen, Anna, Fabiola A. Bechtiger, Ulf Hinz, Magdalena Lewosinska, Franck Billmann, Thilo Hackert, Markus W. Büchler, and Simon Schimmack. 2022. "Enucleation Is a Feasible Procedure for Well-Differentiated pNEN—A Matched Pair Analysis" Cancers 14, no. 10: 2570. https://doi.org/10.3390/cancers14102570
APA StyleNießen, A., Bechtiger, F. A., Hinz, U., Lewosinska, M., Billmann, F., Hackert, T., Büchler, M. W., & Schimmack, S. (2022). Enucleation Is a Feasible Procedure for Well-Differentiated pNEN—A Matched Pair Analysis. Cancers, 14(10), 2570. https://doi.org/10.3390/cancers14102570