
Neurobehavioral Impairment in Pediatric Brain Tumor Survivors: A Meta-Analysis

 , ,
, ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
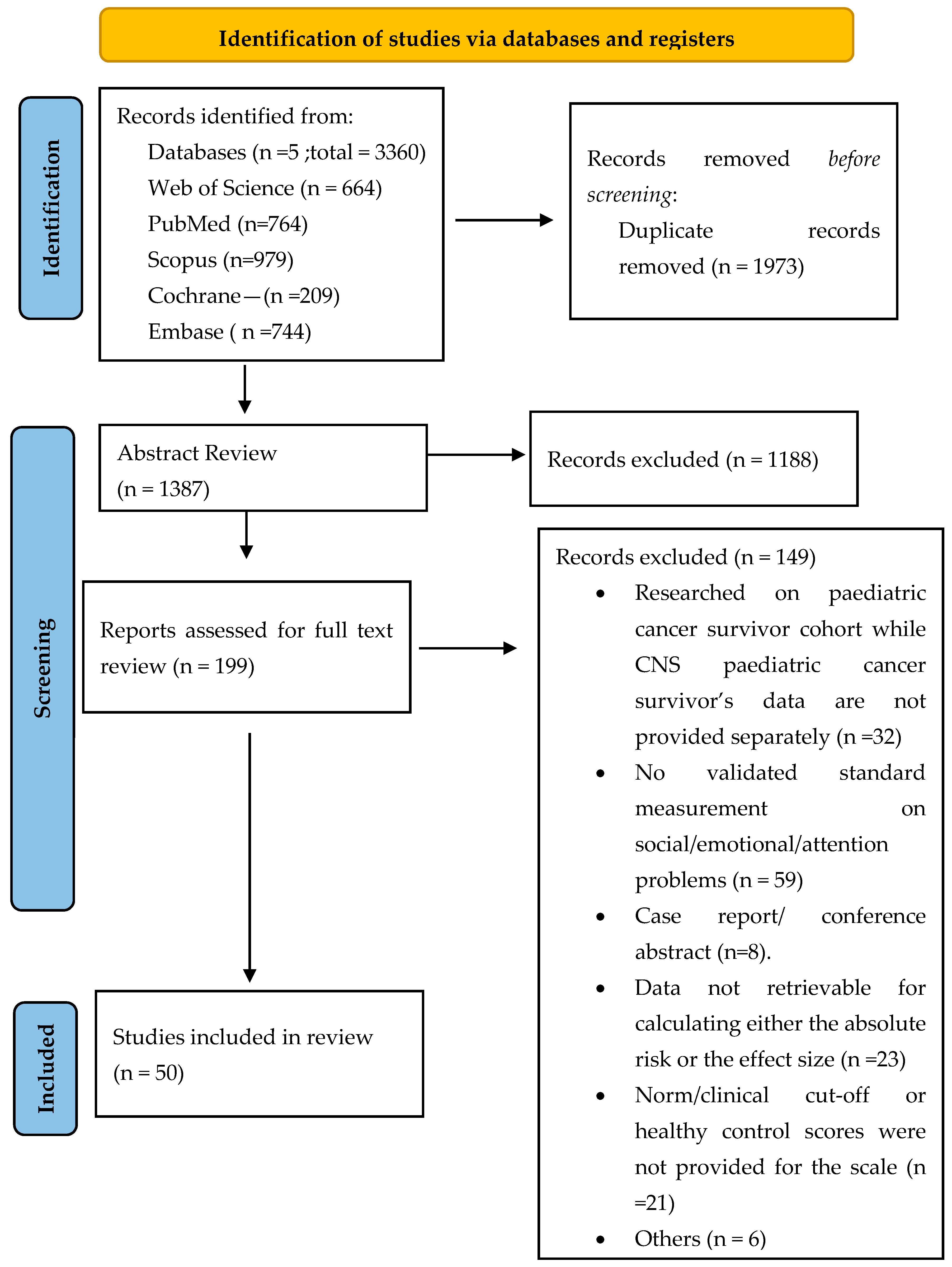
2.1. Searching Strategy
2.2. Study Selection
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.2.3. Selection Procedure
2.3. Data Extraction and Quality Assessment
2.4. Statistical Methods
3. Results
3.1. Study Characteristics
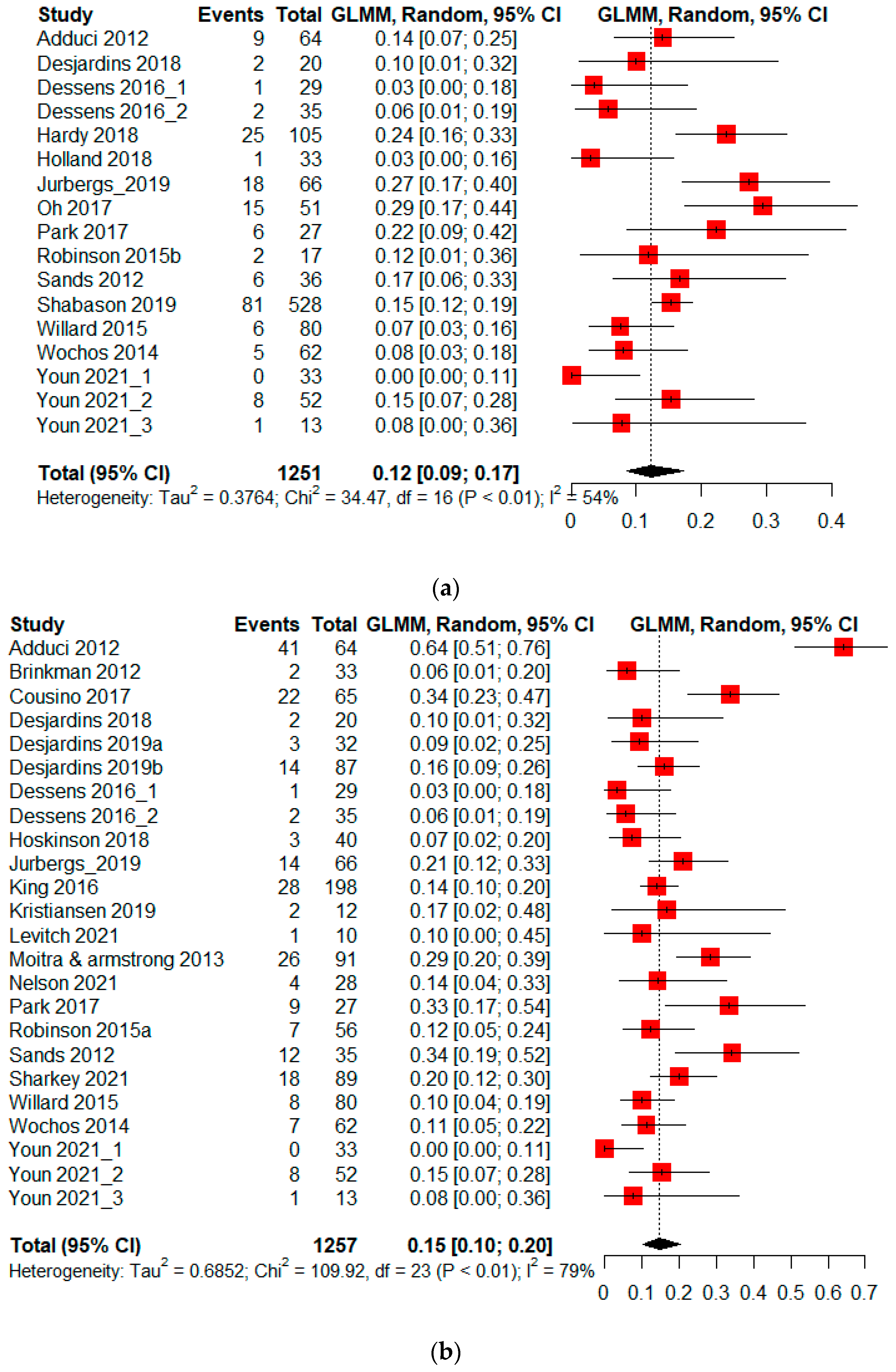
3.2. Absolute Risk of Neurobehavioral Problems in PBTS
3.2.1. Absolute Risk—Attention Problems
3.2.2. Absolute Risk—Emotional Difficulties
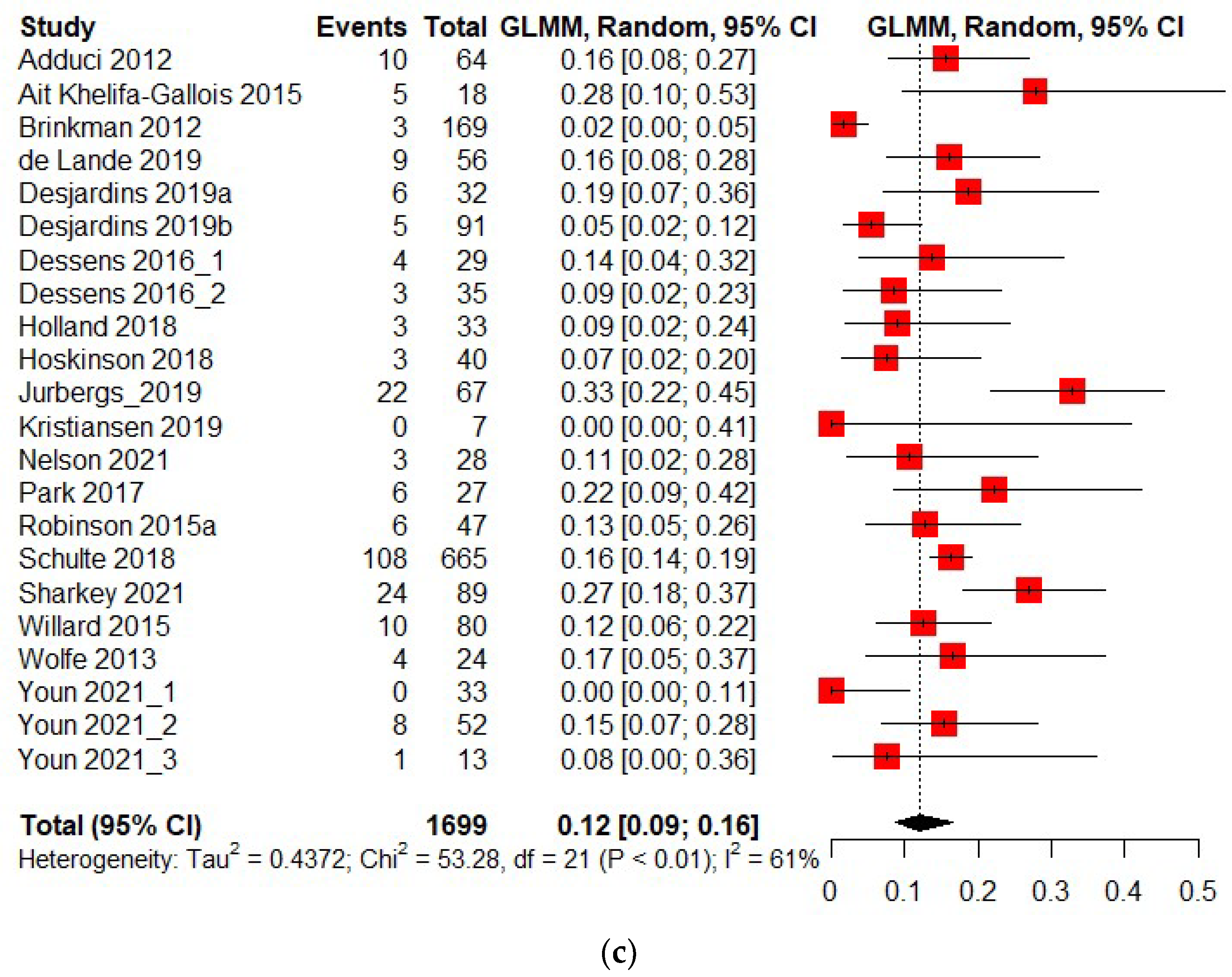
3.2.3. Absolute Risk—Psychosocial Problems
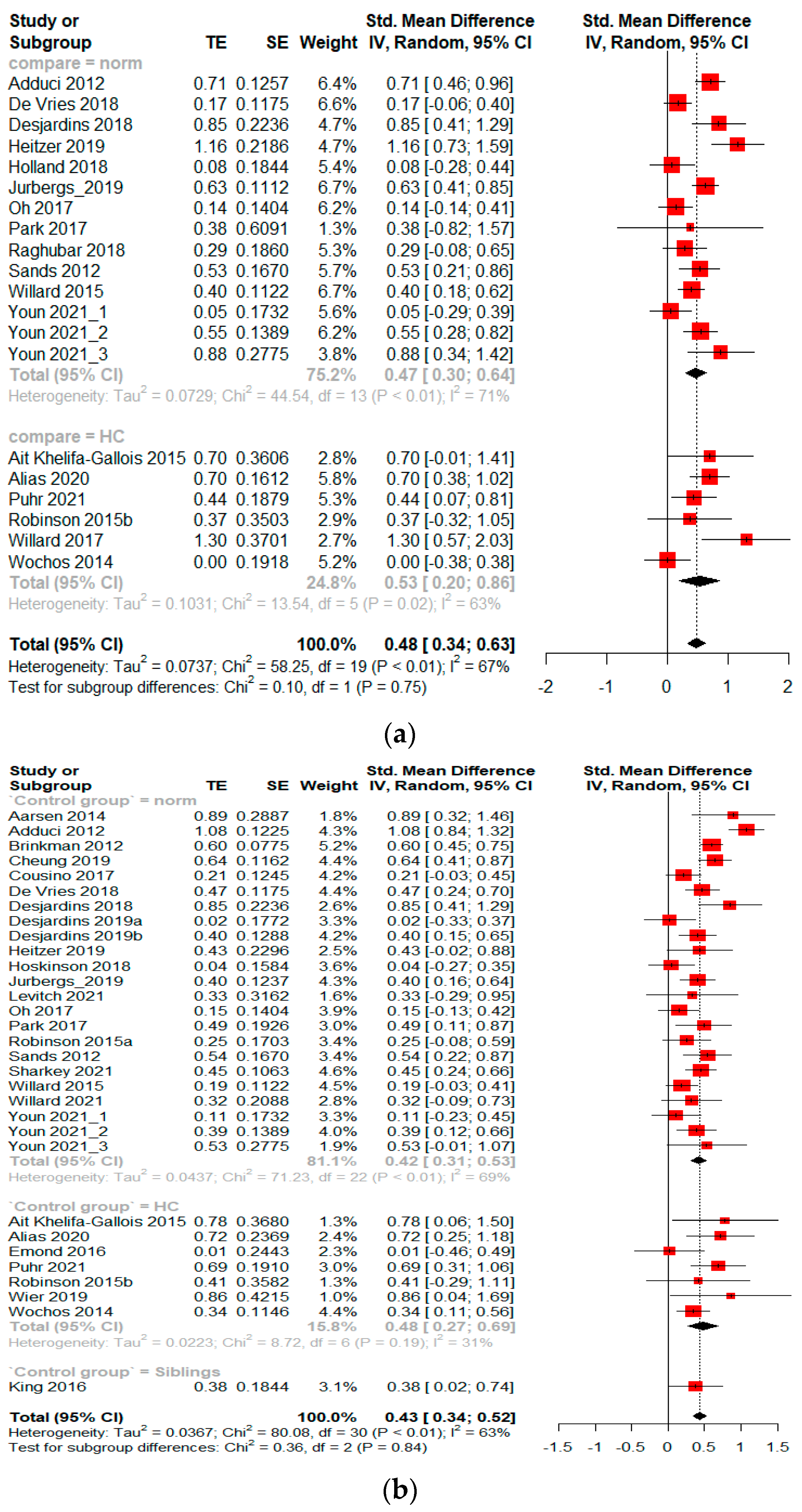
3.3. The Standard Mean Difference of Neurobehavioral Impairment in PBTS Compared to the Population Norm or Healthy Control
3.3.1. Standard Mean Difference—Attention Problems
3.3.2. Standard Mean Difference—Emotional Difficulties
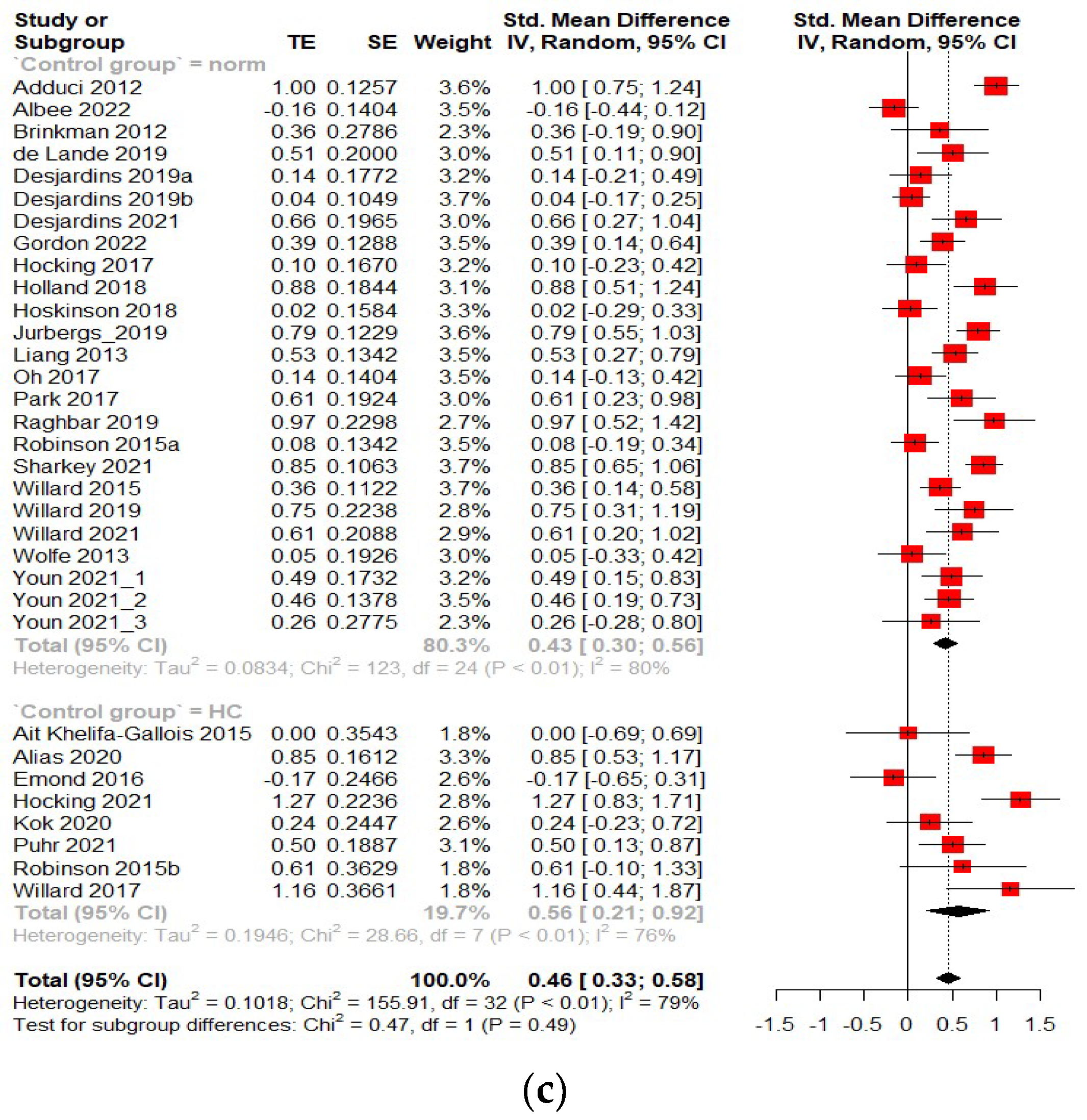
3.3.3. Standard Mean Difference—Psychosocial Problems
3.4. Subgroup Analysis
3.4.1. Reporting Method
3.4.2. Treatment
3.4.3. Meta-Regression
3.4.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Lamba, N.; Groves, A.; Torre, M.; Yeo, K.K.; Iorgulescu, J.B. The epidemiology of primary and metastatic brain tumors in infancy through childhood. J. Neurooncol. 2022, 156, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Pui, C.-H.; Gajjar, A.J.; Kane, J.R.; Qaddoumi, I.A.; Pappo, A.S. Challenging issues in pediatric oncology. Nat. Rev. Clin. Oncol. 2011, 8, 540. [Google Scholar] [CrossRef] [PubMed]
- Perreault, S.; Desjardins, L.; Scheinemann, K. (Eds.) Long Term Sequelae; Springer: Berlin/Heidelberg, Germany, 2022; in press. [Google Scholar]
- Palmer, S.L.; Goloubeva, O.; Reddick, W.E.; Glass, J.O.; Gajjar, A.; Kun, L.; Merchant, T.E.; Mulhern, R.K. Patterns of intellectual development among survivors of pediatric medulloblastoma: A longitudinal analysis. J. Clin. Oncol. 2001, 19, 2302–2308. [Google Scholar] [CrossRef]
- Spiegler, B.J.; Kennedy, K.; Maze, R.; Greenberg, M.L.; Weitzman, S.; Hitzler, J.K.; Nathan, P.C. Comparison of long-term neurocognitive outcomes in young children with acute lymphoblastic leukemia treated with cranial radiation or high-dose or very high-dose intravenous methotrexate. J. Clin. Oncol. 2006, 24, 3858–3864. [Google Scholar] [CrossRef] [PubMed]
- Ellenberg, L.; Liu, Q.; Gioia, G.; Yasui, Y.; Packer, R.J.; Mertens, A.; Donaldson, S.S.; Stovall, M.; Kadan-Lottick, N.; Armstrong, G.; et al. Neurocognitive Status in Long-Term Survivors of Childhood CNS Malignancies: A Report from the Childhood Cancer Survivor Study. Neuropsychology 2009, 23, 705–717. [Google Scholar] [CrossRef] [Green Version]
- Brinkman, T.M.; Krasin, M.J.; Liu, W.; Armstrong, G.T.; Ojha, R.P.; Sadighi, Z.S.; Gupta, P.; Kimberg, C.; Srivastava, D.; Merchant, T.E. Long-term neurocognitive functioning and social attainment in adult survivors of pediatric CNS tumors: Results from the St Jude Lifetime Cohort Study. J. Clin. Oncol. 2016, 34, 1358. [Google Scholar] [CrossRef] [Green Version]
- Tso, W.W.Y.; Hui, E.S.K.; Lee, T.M.C.; Liu, A.P.Y.; Ip, P.; Vardhanabhuti, V.; Cheng, K.K.F.; Fong, D.Y.T.; Chang, D.H.F.; Ho, F.K.W.; et al. Brain Microstructural Changes Associated With Neurocognitive Outcome in Intracranial Germ Cell Tumor Survivors. Front. Oncol. 2021, 11, 573798. [Google Scholar] [CrossRef]
- Tso, W.W.Y.; Liu, A.P.Y.; Lee, T.M.C.; Cheuk, K.L.; Shing, M.K.; Luk, C.W.; Ling, S.C.; Ku, D.T.L.; Li, K.; Yung, A.W.Y.; et al. Neurocognitive function, performance status, and quality of life in pediatric intracranial germ cell tumor survivors. J. Neurooncol. 2019, 141, 393–401. [Google Scholar] [CrossRef]
- Zureick, A.H.; Evans, C.L.; Niemierko, A.; Grieco, J.A.; Nichols, A.J.; Fullerton, B.C.; Hess, C.B.; Goebel, C.P.; Gallotto, S.L.; Weyman, E.A.; et al. Left hippocampal dosimetry correlates with visual and verbal memory outcomes in survivors of pediatric brain tumors. Cancer 2018, 124, 2238–2245. [Google Scholar] [CrossRef] [Green Version]
- Morrall, M.; Reed-Berendt, R.; Moss, K.; Stocks, H.; Houston, A.L.; Siddell, P.; Picton, S.; Grundy, R. Neurocognitive, academic and functional outcomes in survivors of infant ependymoma (UKCCSG CNS 9204). Childs Nerv. Syst. 2019, 35, 411–420. [Google Scholar] [CrossRef]
- Lassaletta, A.; Bouffet, E.; Mabbott, D.; Kulkarni, A.V. Functional and neuropsychological late outcomes in posterior fossa tumors in children. Childs Nerv. Syst. 2015, 31, 1877–1890. [Google Scholar] [CrossRef] [PubMed]
- Levitch, C.F.; Holland, A.A.; Bledsoe, J.; Kim, S.Y.; Barnett, M.; Ramjan, S.; Sands, S.A. Comparison of neuropsychological functioning in pediatric posterior fossa tumor survivors: Medulloblastoma, low-grade astrocytoma, and healthy controls. Pediatr Blood Cancer 2022, 69, e29491. [Google Scholar] [CrossRef] [PubMed]
- Kahalley, L.S.; Peterson, R.; Ris, M.D.; Janzen, L.; Okcu, M.F.; Grosshans, D.R.; Ramaswamy, V.; Paulino, A.C.; Hodgson, D.; Mahajan, A.; et al. Superior Intellectual Outcomes After Proton Radiotherapy Compared With Photon Radiotherapy for Pediatric Medulloblastoma. J. Clin. Oncol. 2020, 38, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Data and Statistics on Children’s Mental Health. Available online:; https://www.cdc.gov/childrensmentalhealth/data.html (accessed on 20 May 2022).
- Asarnow, R.F.; Newman, N.; Weiss, R.E.; Su, E. Association of Attention-Deficit/Hyperactivity Disorder Diagnoses with Pediatric Traumatic Brain Injury: A Meta-analysis. JAMA Pediatr. 2021, 175, 1009–1016. [Google Scholar] [CrossRef]
- Noll, R.B.; Gartstein, M.A.; Vannatta, K.; Correll, J.; Bukowski, W.M.; Davies, W.H. Social, emotional, and behavioral functioning of children with cancer. Pediatrics 1999, 103, 71–78. [Google Scholar] [CrossRef]
- Bonanno, M.; Bourque, C.J.; Aramideh, J.; Cloutier, N.; Dumont, E.; Gomez-Tyo, M.; Julien-Lacoste, A.; Kosir, U.; Provost, C.; Laverdiere, C.; et al. Articulating viewpoints to better define and respond to the needs of adolescents and young adult survivors of pediatric brain tumors. J. Psychosoc. Oncol. 2021, 40, 347–365. [Google Scholar] [CrossRef]
- Hocking, M.C.; McCurdy, M.; Turner, E.; Kazak, A.E.; Noll, R.B.; Phillips, P.; Barakat, L.P. Social competence in pediatric brain tumor survivors: Application of a model from social neuroscience and developmental psychology. Pediatr Blood Cancer 2015, 62, 375–384. [Google Scholar] [CrossRef] [Green Version]
- Salley, C.G.; Hewitt, L.L.; Patenaude, A.F.; Vasey, M.W.; Yeates, K.O.; Gerhardt, C.A.; Vannatta, K. Temperament and social behavior in pediatric brain tumor survivors and comparison peers. J. Pediatr. Psychol. 2015, 40, 297–308. [Google Scholar] [CrossRef] [Green Version]
- Schulte, F.; Kunin-Batson, A.S.; Olson-Bullis, B.A.; Banerjee, P.; Hocking, M.C.; Janzen, L.; Kahalley, L.S.; Wroot, H.; Forbes, C.; Krull, K.R. Social attainment in survivors of pediatric central nervous system tumors: A systematic review and meta-analysis from the Children’s Oncology Group. J. Cancer Surviv. 2019, 13, 921–931. [Google Scholar] [CrossRef]
- Pastore, V.; Colombo, K.; Villa, F.; Galbiati, S.; Adduci, A.; Poggi, G.; Massimino, M.; Recla, M.; Liscio, M.; Strazzer, S. Psychological and adjustment problems due to acquired brain lesions in pre-school-aged patients. Brain Inj. 2013, 27, 677–684. [Google Scholar] [CrossRef]
- Poggi, G.; Liscio, M.; Galbiati, S.; Adduci, A.; Massimino, M.; Gandola, L.; Spreafico, F.; Clerici, C.A.; Fossati-Bellani, F.; Sommovigo, M.; et al. Brain tumors in children and adolescents: Cognitive and psychological disorders at different ages. Psychooncology 2005, 14, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Hardy, K.K.; Willard, V.W.; Gioia, A.; Sharkey, C.; Walsh, K.S. Attention-mediated neurocognitive profiles in survivors of pediatric brain tumors: Comparison to children with neurodevelopmental ADHD. Neuro-Oncology 2018, 20, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Gragert, M.N.; Ris, M.D. Neuropsychological late effects and rehabilitation following pediatric brain tumor. J. Pediatr. Rehabil. Med. 2011, 4, 47–58. [Google Scholar] [CrossRef]
- Vannatta, K.; Gartstein, M.A.; Short, A.; Noll, R.B. A controlled study of peer relationships of children surviving brain tumors: Teacher, peer, and self ratings. J. Pediatr. Psychol. 1998, 23, 279–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vannatta, K.; Gerhardt, C.A.; Wells, R.J.; Noll, R.B. Intensity of CNS treatment for pediatric cancer: Prediction of social outcomes in survivors. Pediatr Blood Cancer 2007, 49, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Trendowski, M.R.; Baedke, J.L.; Sapkota, Y.; Travis, L.B.; Zhang, X.; El Charif, O.; Wheeler, H.E.; Leisenring, W.M.; Robison, L.L.; Hudson, M.M.; et al. Clinical and genetic risk factors for radiation-associated ototoxicity: A report from the Childhood Cancer Survivor Study and the St. Jude Lifetime Cohort. Cancer 2021, 127, 4091–4102. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R.; Cooper, H.; Hedges, L. Parametric measures of effect size. Handb. Res. Synth. 1994, 621, 231–244. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Comparison of two methods to detect publication bias in meta-analysis. JAMA 2006, 295, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid.-Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selçuk, A.A. A guide for systematic reviews: PRISMA. Turk. Arch. Otorhinolaryngol. 2019, 57, 57. [Google Scholar] [CrossRef] [PubMed]
- Aarsen, F.K.; Arts, W.F.; Van Veelen-Vincent, M.L.; Lequin, M.H.; Catsman-Berrevoets, C.E. Long-term outcome in children with low grade tectal tumours and obstructive hydrocephalus. Eur. J. Paediatr. Neurol. 2014, 18, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Adduci, A.; Jankovic, M.; Strazzer, S.; Massimino, M.; Clerici, C.; Poggi, G. Parent-child communication and psychological adjustment in children with a brain tumor. Pediatric Blood Cancer 2012, 59, 290–294. [Google Scholar] [CrossRef]
- Ait Khelifa-Gallois, N.; Laroussinie, F.; Puget, S.; Sainte-Rose, C.; Dellatolas, G. Long-term functional outcome of patients with cerebellar pilocytic astrocytoma surgically treated in childhood. Brain Inj. 2015, 29, 366–373. [Google Scholar] [CrossRef]
- Albee, M.; Allende, S.; Cosgrove, V.; Hocking, M.C. A prospective study of social competence in survivors of pediatric brain and solid tumors. Pediatric Blood Cancer, 2022; online ahead of print. [Google Scholar] [CrossRef]
- Alias, H.; Morthy, S.K.; Zakaria, S.Z.S.; Muda, Z.; Tamil, A.M. Behavioral outcome among survivors of childhood brain tumor: A case control study. BMC Pediatrics 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Brinkman, T.M.; Palmer, S.L.; Chen, S.; Zhang, H.; Evankovich, K.; Swain, M.A.; Bonner, M.J.; Janzen, L.; Knight, S.; Armstrong, C.L. Parent-reported social outcomes after treatment for pediatric embryonal tumors: A prospective longitudinal study. J. Clin. Oncol. 2012, 30, 4134. [Google Scholar] [CrossRef] [Green Version]
- Cheung, A.T.; Li, W.H.C.; Ho, L.L.K.; Ho, K.Y.; Chiu, S.; Chan, C.-F.G.; Chung, O.K. Impact of brain tumor and its treatment on the physical and psychological well-being, and quality of life amongst pediatric brain tumor survivors. Eur. J. Oncol. Nurs. 2019, 41, 104–109. [Google Scholar] [CrossRef]
- Cousino, M.K.; Hazen, R.; Josie, K.L.; Laschinger, K.; de Blank, P.; Taylor, H.G. Childhood cancer and brain tumor late effects: Relationships with family burden and survivor psychological outcomes. J. Clin. Psychol. Med. Settings 2017, 24, 279–288. [Google Scholar] [CrossRef]
- De Lande, R.V.; Maurice-Stam, H.; Marchal, J.; Vuurden, D.V.; Vandertop, W.; Grootenhuis, M.; Schouten-van Meeteren, A. Adaptive behavior impaired in children with low-grade glioma. Pediatric Blood Cancer 2019, 66, e27419. [Google Scholar] [CrossRef]
- De Vries, M.; De Ruiter, M.; Oostrom, K.; Schouten-Van Meeteren, A.; Maurice-Stam, H.; Oosterlaan, J.; Grootenhuis, M. The association between the behavior rating inventory of executive functioning and cognitive testing in children diagnosed with a brain tumor. Child Neuropsychol. 2018, 24, 844–858. [Google Scholar] [CrossRef] [Green Version]
- Desjardins, L.; Thigpen, J.C.; Kobritz, M.; Bettis, A.H.; Gruhn, M.A.; Ichinose, M.; Hoskinson, K.; Fraley, C.; Vreeland, A.; McNally, C. Parent reports of children’s working memory, coping, and emotional/behavioral adjustment in pediatric brain tumor patients: A pilot study. Child Neuropsychol. 2018, 24, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, L.; Barrera, M.; Chung, J.; Cataudella, D.; Janzen, L.; Bartels, U.; Downie, A.; Fairclough, D. Are we friends? Best friend nominations in pediatric brain tumor survivors and associated factors. Supportive Care Cancer 2019, 27, 4237–4244. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, L.; Barrera, M.; Schulte, F.; Chung, J.; Cataudella, D.; Janzen, L.; Bartels, U.; Downie, A. Predicting social withdrawal, anxiety and depression symptoms in pediatric brain tumor survivors. J. Psychosoc. Oncol. 2019, 37, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, L.; Lai, M.-C.; Vorstman, J.; Bartels, U.; Barrera, M. A Novel Approach to Understanding Social Behaviors in Pediatric Brain Tumor Survivors: A Pilot Study. J. Pediatric Psychol. 2021, 46, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Dessens, A.B.; van Herwerden, M.C.; Aarsen, F.K.; Birnie, E.; Catsman-Berrevoets, C.E. Health-related quality of life and emotional problems in children surviving brain tumor treatment: A descriptive study of 2 cohorts. Pediatric Hematol. Oncol. 2016, 33, 282–294. [Google Scholar] [CrossRef] [Green Version]
- Emond, A.; Edwards, L.; Peacock, S.; Norman, C.; Evangeli, M. Social competence in children and young people treated for a brain tumour. Supportive Care Cancer 2016, 24, 4587–4595. [Google Scholar] [CrossRef]
- Gordon, M.L.; Means, B.; Jurbergs, N.; Conklin, H.M.; Gajjar, A.; Willard, V.W. Social Problem Solving in Survivors of Pediatric Brain Tumor. J. Pediatric Psychol. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Heitzer, A.M.; Ashford, J.M.; Hastings, C.; Liu, A.P.; Wu, S.; Bass, J.K.; Vestal, R.; Hoehn, M.; Chiang, J.; Ghazwani, Y. Neuropsychological outcomes of patients with low-grade glioma diagnosed during the first year of life. J. Neuro-Oncol. 2019, 141, 413–420. [Google Scholar] [CrossRef]
- Hocking, M.C.; Quast, L.F.; Brodsky, C.; Deatrick, J.A. Caregiver perspectives on the social competence of pediatric brain tumor survivors. Supportive Care Cancer 2017, 25, 3749–3757. [Google Scholar] [CrossRef] [PubMed]
- Hocking, M.C.; Albee, M.; Brodsky, C.; Shabason, E.; Wang, L.; Schultz, R.T.; Herrington, J. Face processing and social functioning in pediatric brain tumor survivors. J. Pediatric Psychol. 2021, 46, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.A.; Colaluca, B.; Bailey, L.; Stavinoha, P.L. Impact of attention on social functioning in pediatric medulloblastoma survivors. Pediatric Hematol. Oncol. 2018, 35, 76–89. [Google Scholar] [CrossRef]
- Hoskinson, K.R.; Wolfe, K.R.; Yeates, K.O.; Mahone, E.M.; Cecil, K.M.; Ris, M.D. Predicting changes in adaptive functioning and behavioral adjustment following treatment for a pediatric brain tumor: A report from the Brain Radiation Investigative Study Consortium. Psycho-Oncology 2018, 27, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Jurbergs, N.; Harman, J.L.; Kenney, A.E.; Semenkovich, K.; Molnar, A.E.; Willard, V.W. Cognitive and psychosocial development in young children with brain tumors: Observations from a clinical sample. Children 2019, 6, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.A.; Seidel, K.; Di, C.; Leisenring, W.M.; Perkins, S.M.; Krull, K.R.; Sklar, C.A.; Green, D.M.; Armstrong, G.T.; Zeltzer, L.K. Long-term neurologic health and psychosocial function of adult survivors of childhood medulloblastoma/PNET: A report from the Childhood Cancer Survivor Study. Neuro-Oncology 2017, 19, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Kok, T.B.; Koerts, J.; Lemiere, J.; Post, W.J.; de Bont, E.S.; Gidding, C.; Happé, F.; Jacobs, S.; Oostrom, K.; Schieving, J. Social competence in newly diagnosed pediatric brain tumor patients. Pediatric Hematol. Oncol. 2020, 37, 41–57. [Google Scholar] [CrossRef] [Green Version]
- Kristiansen, I.; Strinnholm, M.; Strömberg, B.; Frisk, P. Clinical characteristics, long-term complications and health-related quality of life (HRQoL) in children and young adults treated for low-grade astrocytoma in the posterior fossa in childhood. J. Neuro-Oncol. 2019, 142, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Levitch, C.F.; Malkin, B.; Latella, L.; Guerry, W.; Gardner, S.L.; Finlay, J.L.; Sands, S.A. Long-term neuropsychological outcomes of survivors of young childhood brain tumors treated on the Head Start II protocol. Neuro-Oncol. Pract. 2021, 8, 609–619. [Google Scholar] [CrossRef]
- Liang, S.-Y.; Yang, T.-F.; Chen, Y.-W.; Liang, M.-L.; Chen, H.-H.; Chang, K.-P.; Shan, I.-K.; Chen, Y.-S.; Wong, T.-T. Neuropsychological functions and quality of life in survived patients with intracranial germ cell tumors after treatment. Neuro-Oncology 2013, 15, 1543–1551. [Google Scholar] [CrossRef] [Green Version]
- Moitra, E.; Armstrong, C.L. Neural substrates for heightened anxiety in children with brain tumors. Dev. Neuropsychol. 2013, 38, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Baron Nelson, M.C.; O’Neil, S.H.; Tanedo, J.; Dhanani, S.; Malvar, J.; Nuñez, C.; Nelson, M.D., Jr.; Tamrazi, B.; Finlay, J.L.; Rajagopalan, V. Brain biomarkers and neuropsychological outcomes of pediatric posterior fossa brain tumor survivors treated with surgical resection with or without adjuvant chemotherapy. Pediatric Blood Cancer 2021, 68, e28817. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.; Seo, H.; Sung, K.W.; Joung, Y.S. The effects of attention problems on psychosocial functioning in childhood brain tumor survivors: A 2-year postcraniospinal irradiation follow-up. J. Pediatric Hematol. Oncol. 2017, 39, e46–e53. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Yu, E.-S.; Ha, B.; Park, H.-J.; Kim, J.-H.; Kim, J.-Y. Neurocognitive and psychological functioning of children with an intracranial germ cell tumor. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2017, 49, 960. [Google Scholar] [CrossRef] [PubMed]
- Puhr, A.; Ruud, E.; Anderson, V.; Due-Tønnessen, B.J.; Skarbø, A.-B.; Finset, A.; Andersson, S. Executive Function and Psychosocial Adjustment in Adolescent Survivors of Pediatric Brain Tumor. Dev. Neuropsychol. 2021, 46, 149–168. [Google Scholar] [CrossRef] [PubMed]
- Raghubar, K.P.; Mahone, E.M.; Yeates, K.O.; Ris, M.D. Performance-based and parent ratings of attention in children treated for a brain tumor: The significance of radiation therapy and tumor location on outcome. Child Neuropsychol. 2018, 24, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Raghubar, K.P.; Orobio, J.; Ris, M.D.; Heitzer, A.M.; Roth, A.; Brown, A.L.; Okcu, M.F.; Chintagumpala, M.; Grosshans, D.R.; Paulino, A.C. Adaptive functioning in pediatric brain tumor survivors: An examination of ethnicity and socioeconomic status. Pediatric Blood Cancer 2019, 66, e27800. [Google Scholar] [CrossRef]
- Robinson, K.E.; Wolfe, K.R.; Yeates, K.O.; Mahone, E.M.; Cecil, K.M.; Ris, M.D. Predictors of adaptive functioning and psychosocial adjustment in children with pediatric brain tumor: A report from the brain radiation investigative study consortium. Pediatric Blood Cancer 2015, 62, 509–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, K.E.; Pearson, M.M.; Cannistraci, C.J.; Anderson, A.W.; Kuttesch, J.F., Jr.; Wymer, K.; Smith, S.E.; Park, S.; Compas, B.E. Functional neuroimaging of working memory in survivors of childhood brain tumors and healthy children: Associations with coping and psychosocial outcomes. Child Neuropsychol. 2015, 21, 779–802. [Google Scholar] [CrossRef] [PubMed]
- Sands, S.A.; Zhou, T.; O’Neil, S.H.; Patel, S.K.; Allen, J.; Cullen, P.M.; Kaleita, T.A.; Noll, R.; Sklar, C.; Finlay, J.L. Long-term follow-up of children treated for high-grade gliomas: Children’s oncology group L991 final study report. J. Clin. Oncol. 2012, 30, 943. [Google Scholar] [CrossRef] [Green Version]
- Schulte, F.; Brinkman, T.M.; Li, C.; Fay-McClymont, T.; Srivastava, D.K.; Ness, K.K.; Howell, R.M.; Mueller, S.; Wells, E.; Strother, D. Social adjustment in adolescent survivors of pediatric central nervous system tumors: A report from the C hildhood C ancer S urvivor S tudy. Cancer 2018, 124, 3596–3608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shabason, E.K.; Brodsky, C.; Baran, J.; Isaac, L.; Minturn, J.E.; Ginsberg, J.P.; Hobbie, W.; Fisher, M.; Blum, N.; Hocking, M.C. Clinical diagnosis of attention-deficit/hyperactivity disorder in survivors of pediatric brain tumors. J. Neuro-Oncol. 2019, 143, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, C.M.; Mullins, L.L.; Clawson, A.H.; Gioia, A.; Hawkins, M.A.; Chaney, J.M.; Walsh, K.S.; Hardy, K.K. Assessing neuropsychological phenotypes of pediatric brain tumor survivors. Psycho-Oncology 2021, 30, 1366–1374. [Google Scholar] [CrossRef]
- Wier, R.; Aleksonis, H.A.; Pearson, M.M.; Cannistraci, C.J.; Anderson, A.W.; Kuttesch, J.F.; Compas, B.E.; Hoskinson, K.R. Fronto-limbic white matter microstructure, behavior, and emotion regulation in survivors of pediatric brain tumor. J. Neuro-Oncol. 2019, 143, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Willard, V.W.; Conklin, H.M.; Wu, S.; Merchant, T.E. Prospective longitudinal evaluation of emotional and behavioral functioning in pediatric patients with low-grade glioma treated with conformal radiation therapy. J. Neuro-Oncol. 2015, 122, 161–168. [Google Scholar] [CrossRef]
- Willard, V.W.; Allen, T.M.; Hardy, K.K.; Bonner, M.J. Social functioning in survivors of pediatric brain tumors: Contribution of neurocognitive and social-cognitive skills. Child. Health Care 2017, 46, 181–195. [Google Scholar] [CrossRef]
- Willard, V.W.; Russell, K.M.; Long, A.; Phipps, S. The impact of connectedness on social functioning in youth with brain tumors. Pediatric Blood Cancer 2019, 66, e27607. [Google Scholar] [CrossRef]
- Willard, V.W.; Gordon, M.L.; Means, B.; Brennan, R.C.; Conklin, H.M.; Merchant, T.E.; Vinitsky, A.; Harman, J.L. Social–emotional functioning in preschool-aged children with cancer: Comparisons between children with brain and non-CNS solid tumors. J. Pediatric Psychol. 2021, 46, 790–800. [Google Scholar] [CrossRef]
- Wochos, G.; Semerjian, C.; Walsh, K.S. Differences in parent and teacher rating of everyday executive function in pediatric brain tumor survivors. Clin. Neuropsychol. 2014, 28, 1243–1257. [Google Scholar] [CrossRef]
- Wolfe, K.R.; Walsh, K.S.; Reynolds, N.C.; Mitchell, F.; Reddy, A.T.; Paltin, I.; Madan-Swain, A. Executive functions and social skills in survivors of pediatric brain tumor. Child Neuropsychol. 2013, 19, 370–384. [Google Scholar] [CrossRef] [Green Version]
- Youn, S.H.; Ha, B.; Lee, E.H.; Park, B.; Yang, S.E.; Yu, E.S.; Kim, J.Y. Neurocognitive and psychological functioning of pediatric brain tumor patients undergoing proton beam therapy for three different tumor types. Pediatric Blood Cancer 2022, 69, e29430. [Google Scholar] [CrossRef] [PubMed]
- Riehm, K.E.; Mojtabai, R. Trends in parent-rated emotional symptoms, conduct problems, and hyperactivity/inattention among U.S. children and adolescents, 2004–2019. J. Affect Disord. 2022, 299, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Bot, M.; De Leeuw den Bouter, B.J.; Adriaanse, M.C. Prevalence of psychosocial problems in Dutch children aged 8–12 years and its association with risk factors and quality of life. Epidemiol. Psychiatr. Sci. 2011, 20, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Hudson, M.M.; Bhatia, S.; Casillas, J.; Landier, W.; Rogers, Z.R.; Allen, C.; Harper, J.; Hord, J.; Jain, J.; Warwick, A. Long-term Follow-up Care for Childhood, Adolescent, and Young Adult Cancer Survivors. Pediatrics 2021, 148, e2021053127. [Google Scholar] [CrossRef]
- Liptak, C.; Manley, P.; Recklitis, C.J. The feasibility of psychosocial screening for adolescent and young adult brain tumor survivors: The value of self-report. J. Cancer Surviv. 2012, 6, 379–387. [Google Scholar] [CrossRef]
- Barr, R.D.; Ferrari, A.; Ries, L.; Whelan, J.; Bleyer, W.A. Cancer in Adolescents and Young Adults: A Narrative Review of the Current Status and a View of the Future. JAMA Pediatr. 2016, 170, 495–501. [Google Scholar] [CrossRef]
- Raj, S.P.; Narad, M.E.; Salloum, R.; Platt, A.; Thompson, A.; Baum, K.T.; Wade, S.L. Development of a Web-Based Psychosocial Intervention for Adolescent and Young Adult Survivors of Pediatric Brain Tumor. J. Adolesc. Young Adult Oncol. 2018, 7, 187–195. [Google Scholar] [CrossRef]
- Wade, S.L.; Narad, M.E.; Moscato, E.L.; LeBlond, E.I.; King, J.A.; Raj, S.P.; Platt, A.; Thompson, A.N.; Baum, K.T.; Salloum, R. A Survivor’s Journey: Preliminary efficacy of an online problem-solving therapy for survivors of pediatric brain tumor. Pediatr Blood Cancer 2020, 67, e28043. [Google Scholar] [CrossRef]
- Barrera, M.; Atenafu, E.G.; Sung, L.; Bartels, U.; Schulte, F.; Chung, J.; Cataudella, D.; Hancock, K.; Janzen, L.; Saleh, A.; et al. A randomized control intervention trial to improve social skills and quality of life in pediatric brain tumor survivors. Psychooncology 2018, 27, 91–98. [Google Scholar] [CrossRef]
- Conklin, H.M.; Reddick, W.E.; Ashford, J.; Ogg, S.; Howard, S.C.; Morris, E.B.; Brown, R.; Bonner, M.; Christensen, R.; Wu, S.; et al. Long-term efficacy of methylphenidate in enhancing attention regulation, social skills, and academic abilities of childhood cancer survivors. J. Clin. Oncol. 2010, 28, 4465–4472. [Google Scholar] [CrossRef] [Green Version]
- Achenbach, T.M. and C. Edelbrock, Child behavior checklist. Burlington (Vt) 1991, 7, 371–392. [Google Scholar]
- Gray, S.A.O.; Carter, A.S. Adaptive Behavior Assessment System, Second Edition. In Encyclopedia of Autism Spectrum Disorders; Volkmar, F.R., Ed.; Springer New York: New York, NY, USA, 2013; pp. 52–55. [Google Scholar]
- Roth, R.M.; Gioia, G.A.; Guy, S.C.; Kenworthy, L.; Isquith, P.K. Behavior Rating Inventory of Executive Function: BRIEF; Psychological Assessment Resources: Odessa, FL, USA, 2000. [Google Scholar]
- Reynolds, C.R. Behavior assessment system for children. Corsini Encycl. Psychol. 2010, 1–2. [Google Scholar] [CrossRef]
- Gresham, F.M.; Elliott, S.N. Social Skills Improvement System: Rating Scales Manual; NCS Pearson: Bloomington, MN, USA, 2008. [Google Scholar]
- Achenbach, T.M. Manual for the Youth Self-Report and 1991 Profile; Department of Psychiatry, University of Vermont: Burlington, VT, USA, 1991. [Google Scholar]
- Sparrow, S.; Cicchetti, D.; Saulnier, C. Vineland Adaptive Behavior Scales, 3rd ed.; Pearson: Bloomington, MN, USA, 2016. [Google Scholar]
- Muris, P.; Meesters, C.; van den Berg, F. The strengths and difficulties questionnaire (SDQ). Eur. Child Adolesc. Psychiatry 2003, 12, 1–8. [Google Scholar] [CrossRef]
- Gershon, R.C.; Cella, D.; A Fox, N.; Havlik, R.J.; Hendrie, H.C.; Wagster, M.V. Assessment of neurological and behavioural function: The NIH Toolbox. Lancet Neurol. 2010, 9, 138–139. [Google Scholar] [CrossRef]
- Gresham, F.M.; Elliott, S.N.; Service, A.G. Social Skills Rating System Manual; American Guidance Service: Circle Pines, MN, USA, 1990. [Google Scholar]
- Constantino, J.N.; Gruber, C. Social Responsiveness Scale (SRS); Western Psychological Services: Los Angeles, CA, USA, 2005. [Google Scholar]
- Shahid, A.; Wilkinson, K.; Marcu, S.; Shapiro, C.M.; Center for Epidemiological Studies Depression Scale for Children (CES-DC). STOP, THAT and One Hundred Other Sleep Scales; Springer: New York, NY, USA, 2011; pp. 93–96. [Google Scholar] [CrossRef]
- Harter, S. Self-Perception Profile for Children: Manual and Questionnaires (Grades 3–8); University of Denver: Denver, CO, USA, 2012. [Google Scholar]
- Pappas, D. ADHD Rating Scale-IV: Checklists, norms, and clinical interpretation. J. Psychoeduc. Assess. 2006, 24, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Derogatis, L. BSI-18: Brief Symptom Inventory 18—Administration, Scoring, and Procedures Manual; NCS Pearson: Minneapolis, MN, USA, 2001. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R. Beck Anxiety Inventory Manual; Psychological Corp: San Antonia, TX, USA, 1993. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory; Harcourt Brace Jovanovich: New York, NY, USA, 1987. [Google Scholar]
- Monga, S.; Birmaher, B.; Chiappetta, L.; Brent, D.; Kaufman, J.; Bridge, J.; Cully, M. Screen for child anxiety-related emotional disorders (SCARED): Convergent and divergent validity. Depress. Anxiety 2000, 12, 85–91. [Google Scholar] [CrossRef]
- Beck, J.S.; Beck, A.T.; Jolly, J.B. Beck Youth Inventories of Emotional & Social Impairment: Depression Inventory for Youth, Anxiety Inventory for Youth, Anger Inventory for Youth, Disruptive Behavior for Youth, Self-Concept Inventory for Youth: Manual; Psychological Corporation: New York, NY, USA, 2001. [Google Scholar]
- Cho, S. A standardization study of the Korean Personality Rating Scale for Children (KPRC). Korean J. Clin. Psychol. 2006, 25, 825–848. [Google Scholar]
- Sandberg, M.A. Neurobehavioral Functioning Inventory. In Encyclopedia of Clinical Neuropsychology; Springer International Publishing: Cham, Switzerland, 2018; pp. 2383–2384. [Google Scholar]
- Torki, R.N.; Doerner, E.E.; Kaye, N.C.; Tsutsui, E.M.; Merrell, K.W. Social Emotional Assets and Resilience Scales: Status and New Developments. Psychology 2010. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Tumor Type | Assessment Tool | Age at Diagnosis | Age at Assessment | Sample Size | Psychosocial Measure | Emotion Measure | Attention Measure | Report Type | Comparison Group | Risk of Bias | Radio Therapy | Region |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aarsen 2014 [35] | low grade tectal tumor | CBCL & YSR | 10.02 | 14.30 | 12 | N | Y | N | parent-& self-reports | norm | Low | N | EU |
| Adduci 2012 [36] | mix | CBCL & VABS | 6.76 | 9.47 | 64 | Y | Y | Y | parent-report | norm | Low | mix | EU |
| Ait Khelifa-Gallois 2015 [37] | pilocytic astrocytoma | scale adapted from CBCL, SDQ and Conners Scale | 6.80 | 15.10 | 18 | Y | Y | Y | parent-report | HC | Low | N | EU |
| Albee 2022 [38] | mix | SSIS | 8.87 | 10.62 | 51 | Y | N | N | parent-report | norm | Low | mix | NA |
| Alias 2020 [39] | mix | CBCL | 7.20 | 12.50 | 38 | Y | Y | Y | parent-report | HC | Low | mix | Asia |
| Brinkman 2012 [40] | embryonal tumor | CBCL | 10.70 | 11.00 | 169 | Y | Y | N | parent-report | norm | Low | Y | NA |
| Cheung 2019 [41] | mix | CES-DC | 9.70 | 11.70 | 77 | N | Y | N | self-report | norm | Medium | mix | Asia |
| Cousino 2017 [42] | mix | BASC | 6.16 | 14.30 | 65 | N | Y | N | parent- report | norm | Low | mix | NA |
| De Lande 2019 [43] | low-grade glioma | VABS | 7.16 | 12.08 | 56 | Y | N | N | parent- report | norm | Low | mix | EU |
| De Vries 2018 [44] | mix | BRIEF | 6.90 | 13.80 | 73 | N | Y | Y | parent-report | norm | Low | mix | EU |
| Desjardins 2018 [45] | mix | CBCL | 9.79 | 10.79 | 20 | N | Y | Y | parent-report | norm | Medium | mix | NA |
| Desjardins 2019a [46] | mix | SSRS & BRIEF | 5.87 | 10.41 | 32 | Y | Y | N | parent-report | norm | Low | mix | NA |
| Desjardins 2019b [47] | mix | SSRS & BRIEF | 5.22 | 11.21 | 91 | Y | Y | N | parent-report | norm | Low | mix | NA |
| Desjardins 2021 [48] | mix | CBCL | 6.09 | 14.00 | 26 | Y | N | N | parent-report | norm | Low | mix | NA |
| Dessens 2016 [49] | mix | CBCL | 5.80 | 11.70 | 13 | Y | Y | Y | child- & parent-reports | norm | Low | mix | EU |
| Emond 2016 [50] | mix | SSIS, SRS & SDQ | 6.71 | 12.59 | 33 | Y | Y | N | self-, parent- & teacher-reports | HC | Medium | mix | EU |
| Gordon 2022 [51] | mix | SPPC & NTEM | 4.14 | 10.59 | 65 | Y | N | N | self- & parent-reports | norm | Low | mix | NA |
| Hardy 2018 [24] | mix | ADHD-RS-IV | 6.20 | 12.00 | 105 | N | N | Y | parent-& teacher-reports | norm | Low | mix | NA |
| Heitzer 2019 [52] | low-grade glioma | CBCL | 0.51 | 9.90 | 19 | N | Y | Y | parent-report | norm | Low | mix | NA |
| Hocking 2017 [53] | mix | SSIS | 5.66 | 14.46 | 36 | Y | N | N | parent-report | norm | Low | mix | NA |
| Hocking 2021 [54] | mix | SRS | 6.10 | 13.72 | 54 | Y | N | N | parent-report | HC | Low | mix | NA |
| Holland 2018 [55] | medulloblastoma | CBCL | 8.02 | 13.96 | 33 | Y | N | Y | parent-report | norm | Low | Y | NA |
| Hoskinson 2018 [56] | mix | ABAS-II; BASC | 10.72 | 12.76 | 40 | Y | Y | N | parent-report | norm | Low | mix | NA |
| Jurbergs 2019 [57] | mix | ABAS-II CBCL | 2.39 | 4.52 | 67 | Y | Y | Y | parent-report | norm | High | mix | NA |
| King 2016 [58] | medulloblastoma | BSI | 9.00 | NR | 198 | N | Y | N | self-report | Siblings | Low | mix | NA |
| Kok 2020 [59] | mix | CBCL | 9.17 | 8.33 | 21 | Y | N | N | parent-& teacher-reports | HC | Medium | N | EU |
| Kristiansen 2019 [60] | low-grade astrocytoma | BYI, BDI, BAI | 8.70 | 20.8 | 7 | Y | Y | N | self-report | norm | Medium | mix | EU |
| Levitch 2021 [61] | mix | BASC | 2.98 | 10.23 | 10 | N | Y | N | parent-report | norm | Low | mix | NA |
| Liang 2013 [62] | intracranial germ cell tumor | ABAS | 11.90 | 17.70 | 56 | Y | N | N | parent-report | norm | Low | Y | Asia |
| Moitra & Armstrong 2013 [63] | mix | SCARED–C | 6.56 | 11.40 | 91 | N | Y | N | self-report | norm | Medium | N/A | NA |
| Nelson 2021 [64] | posterior fossa brain tumor | CBCL | 11.32 | 5.00 | 28 | Y | Y | N | parent-report | norm | Low | mix | NA |
| Oh 2017 [65] | mix | K-PRC | 10.06 | 10.33 | 51 | Y | Y | Y | parent-report | norm | High | Y | Asia |
| Park 2017 [66] | intracranial germ cell tumor | CBCL | 12.30 | 12.60 | 27 | Y | Y | Y | parent-report | norm | Medium | Y | Asia |
| Puhr 2021 [67] | mix | CBCL & YSR | 6.80 | 15.70 | 48 | Y | Y | Y | parent- & self-report | HC | Low | mix | EU |
| Raghubar 2018 [68] | mix | BASC | 9.12 | 11.54 | 29 | N | N | Y | parent-report | norm | Low | mix | NA |
| Raghbar 2019 [69] | mix | ABAS-II | 6.39 | 13.37 | 114 | Y | N | N | parent-report | norm | Low | Y | NA |
| Robinson 2015a [70] | mix | ABAS-II | 10.67 | 10.72 | 47 | Y | Y | N | parent-report | norm | Low | Y | NA |
| Robinson 2015b [71] | mix | YSR &CBCL | 6.94 | 12.60 | 17 | Y | Y | Y | self- & parent-reports | HC | Low | mix | NA |
| Sands 2012 [72] | mix | NFI | 8.80 | 23.60 | 35 | N | Y | Y | parent-report & Self-report | norm | Low | Y | NA |
| Schulte 2018 [73] | mix | CBCL | N/A | 15.00 | 665 | Y | N | N | parent-report | norm * | Low | mix | NA |
| Shabason 2019 [74] | mix | ADHD diagnosis | 8.15 | 15.50 | 528 | N | N | Y | clinical diagnosis | norm | Low | mix | NA |
| Sharkey 2021 [75] | mix | CBCL | 6.57 | 12.60 | 89 | Y | Y | N | parent-report | norm | Low | mix | NA |
| Wier 2019 [76] | mix | CBCL | N/A | 12.83 | 11 | Y | N | N | parent-report | HC | Low | mix | NA |
| Willard 2015 [77] | low-grade glioma | CBCL | 6.80 | 8.90 | 80 | Y | Y | Y | parent-report | norm | Low | Y | NA |
| Willard 2017 [78] | mix | CBCL | 5.19 | 11.79 | 10 | Y | N | Y | parent-report | HC | Low | mix | NA |
| Willard 2019 [79] | mix | SEARS | 8.53 | 14.70 | 20 | Y | N | N | self-, parent-& teacher-reports | norm | Low | mix | NA |
| Willard 2021 [80] | mix | NTEM &BASC | 3.61 | 5.46 | 23 | Y | Y | N | parent-report | norm | Low | mix | NA |
| Wochos 2014 [81] | mix | BRIEF | 4.68 | 5.81 | 62 | N | Y | Y | parent-report | HC | Low | mix | NA |
| Wolfe 2013 [82] | mix | SSIS & BRIEF | 4.50 | 9.10 | 24 | Y | N | N | parent-& self-reports | norm | Low | mix | NA |
| Youn 2021 [83] | mix | CBCL | 9.30 | 0.60 | 33 | Y | Y | Y | parent-report | norm | Low | Y | Asia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Liu, A.P.Y.; Lee, T.M.-C.; Wong, W.H.S.; Fong, D.Y.T.; Leung, L.K.; Shing, M.M.K.; Ku, D.T.-L.; Chan, G.C.-F.; Tso, W.W.-Y. Neurobehavioral Impairment in Pediatric Brain Tumor Survivors: A Meta-Analysis. Cancers 2022, 14, 3269. https://doi.org/10.3390/cancers14133269
Wang Y, Liu APY, Lee TM-C, Wong WHS, Fong DYT, Leung LK, Shing MMK, Ku DT-L, Chan GC-F, Tso WW-Y. Neurobehavioral Impairment in Pediatric Brain Tumor Survivors: A Meta-Analysis. Cancers. 2022; 14(13):3269. https://doi.org/10.3390/cancers14133269
Chicago/Turabian StyleWang, Yuliang, Anthony Pak Yin Liu, Tatia Mei-Chun Lee, Wilfred Hing Sang Wong, Daniel Yee Tak Fong, Lok Kan Leung, Matthew Ming Kong Shing, Dennis Tak-Loi Ku, Godfrey Chi-Fung Chan, and Winnie Wan-Yee Tso. 2022. "Neurobehavioral Impairment in Pediatric Brain Tumor Survivors: A Meta-Analysis" Cancers 14, no. 13: 3269. https://doi.org/10.3390/cancers14133269
APA StyleWang, Y., Liu, A. P. Y., Lee, T. M. -C., Wong, W. H. S., Fong, D. Y. T., Leung, L. K., Shing, M. M. K., Ku, D. T. -L., Chan, G. C. -F., & Tso, W. W. -Y. (2022). Neurobehavioral Impairment in Pediatric Brain Tumor Survivors: A Meta-Analysis. Cancers, 14(13), 3269. https://doi.org/10.3390/cancers14133269