
Radiomics-Based Deep Learning Prediction of Overall Survival in Non-Small-Cell Lung Cancer Using Contrast-Enhanced Computed Tomography


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Computed Tomography Data Acquisition
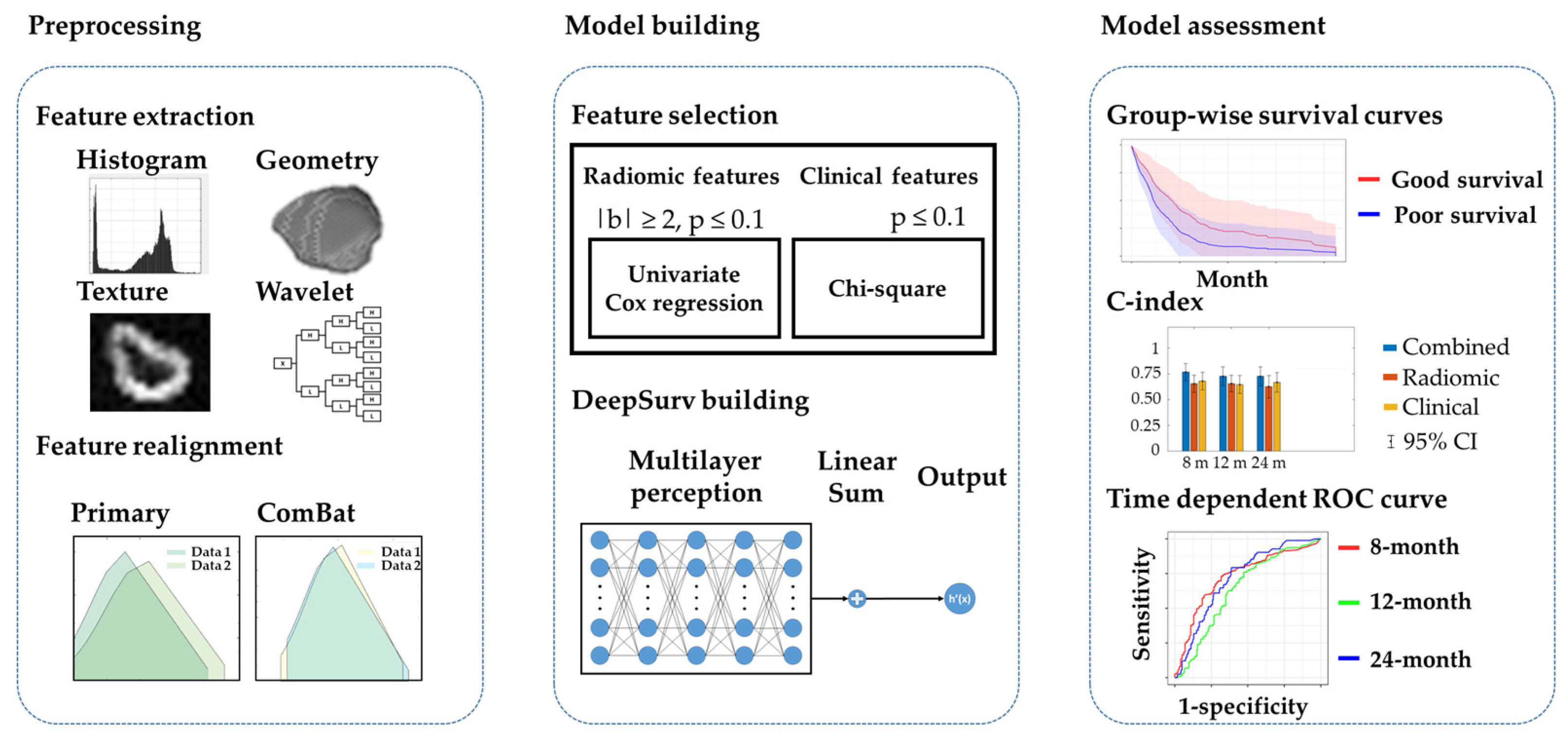
2.3. Tumor Segmentation and Radiomic Feature Extraction
2.4. Realignment of Multicenter Radiomic Datasets
2.5. Selection of Survival Predictors
2.6. Survival Prediction with Deep Neural Networks
2.7. Statistical Analysis
3. Results
3.1. Demographic Data of Multicenter Datasets
3.2. Variation Estimation of Lesion Contouring and Radiomic Features
3.3. Selected Radiomic and Clinical Features for the Prediction Model (ICC)
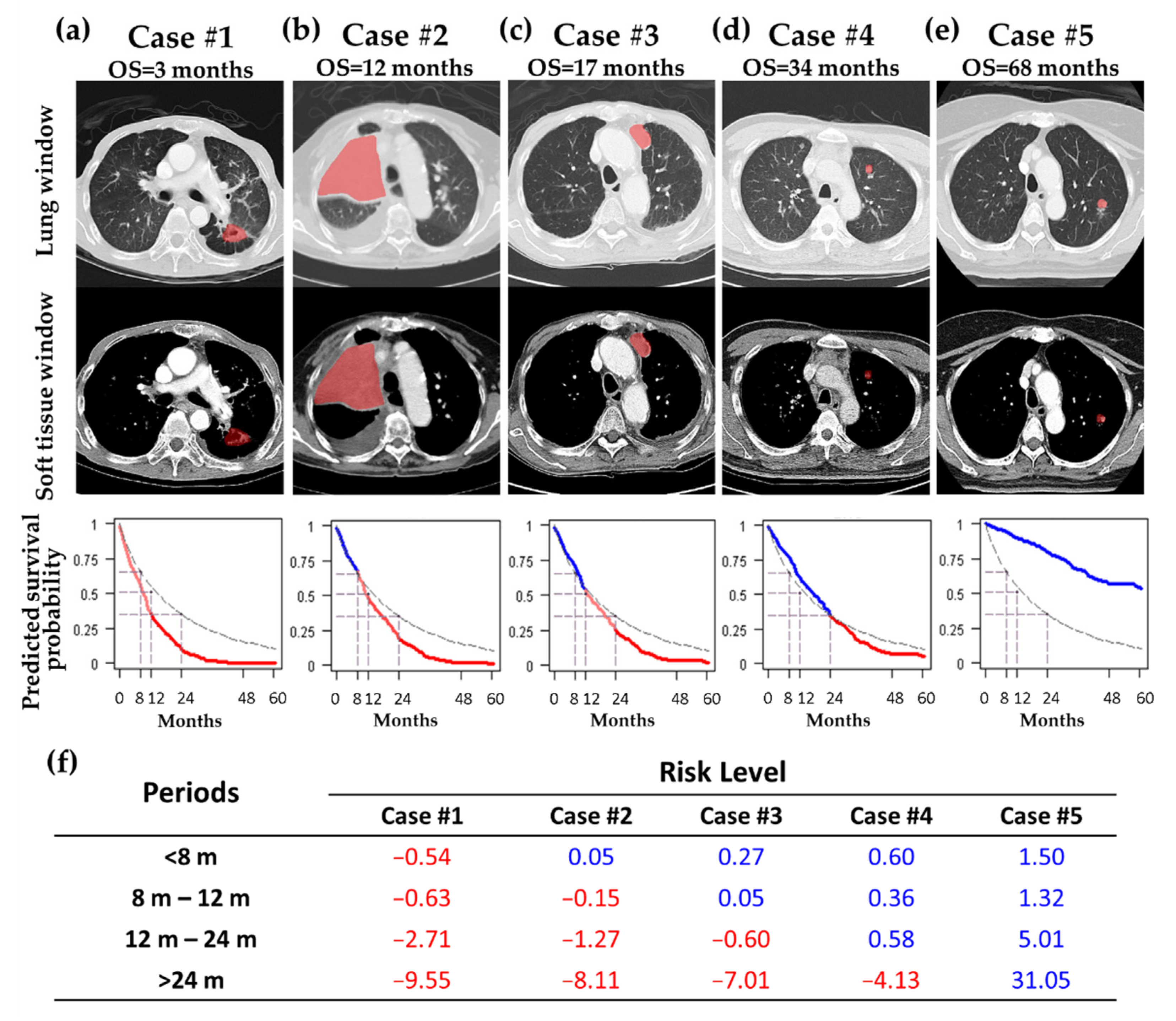
3.4. Representative Cases for Predicting Personalized Survival Curves
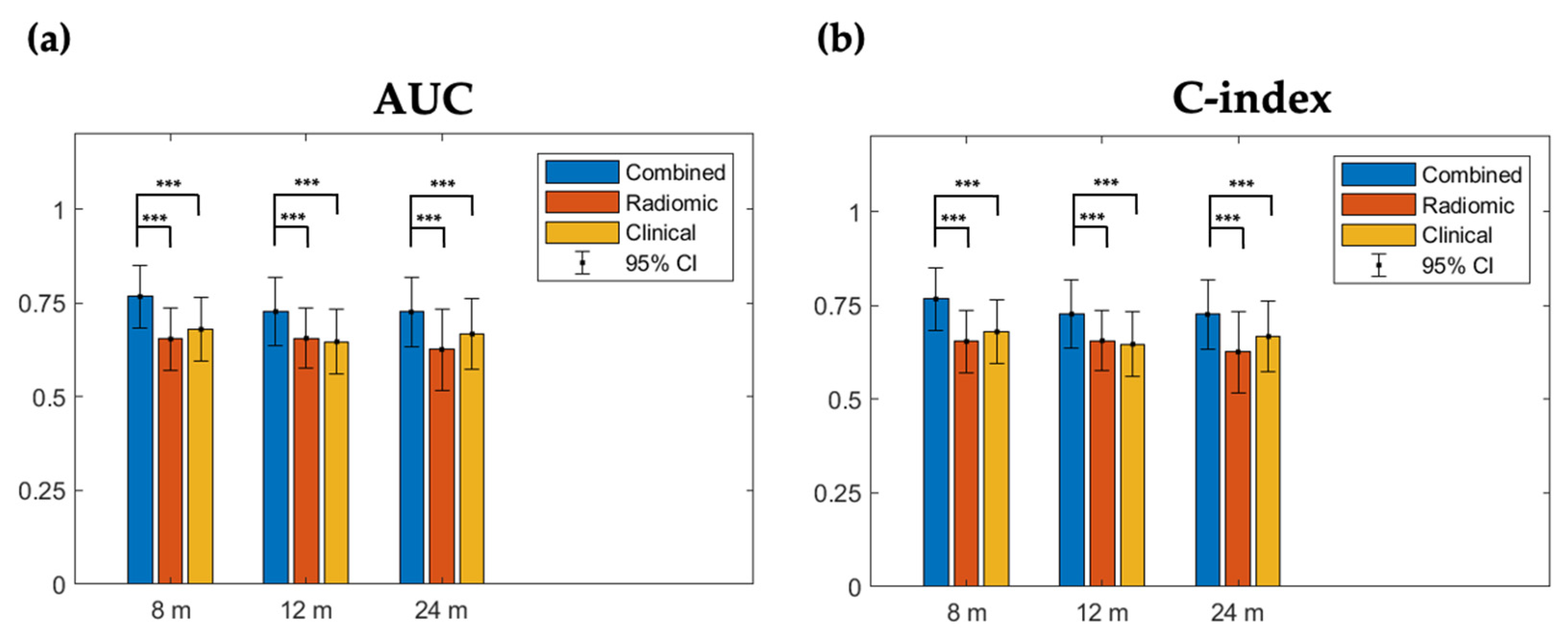
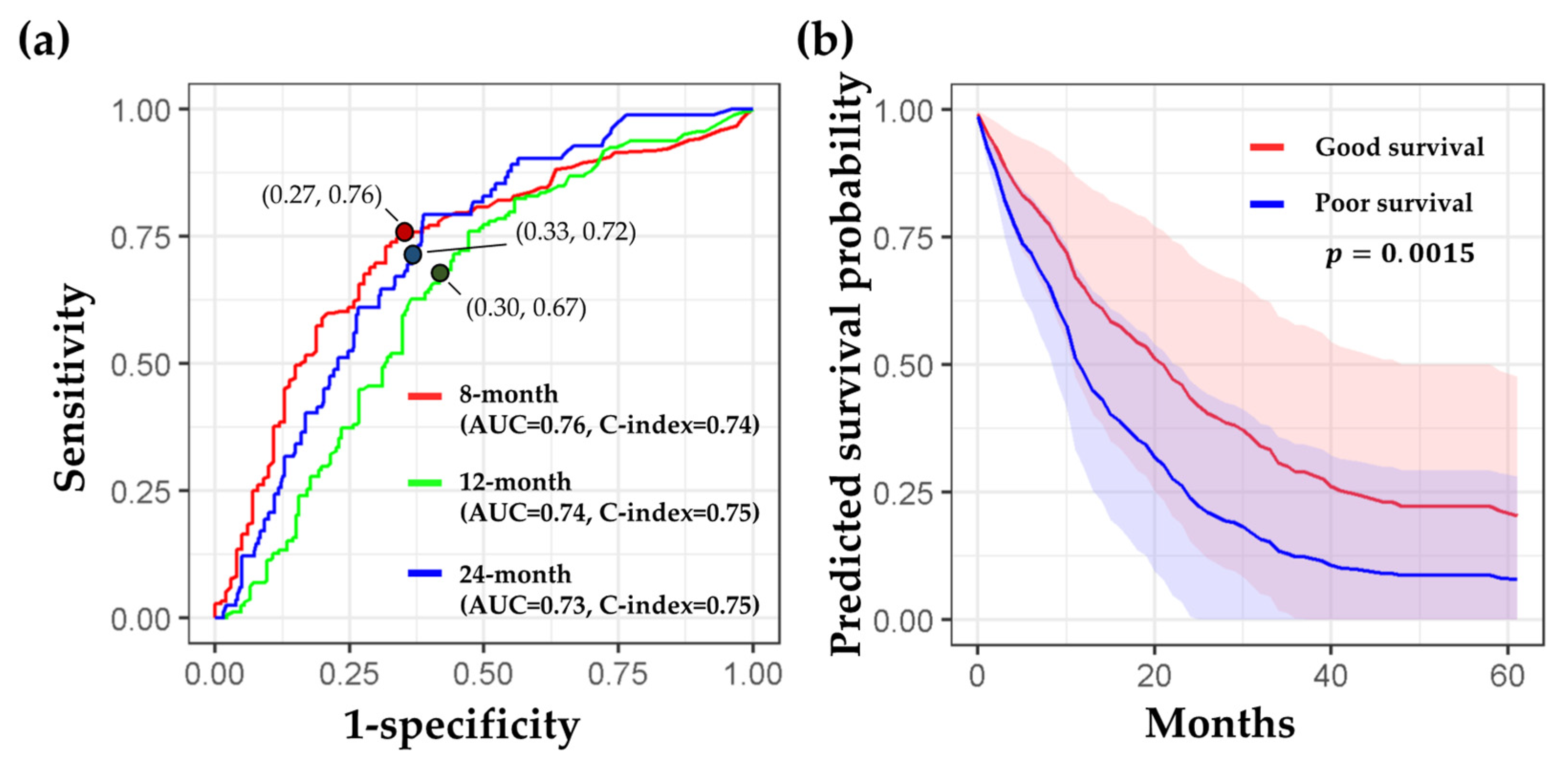
3.5. Superior Performance of the Prediction Model Based on Combined Features
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The United States Food and Drug Administration. Good Machine Learning Practice for Medical Device Development: Guiding Principles. Available online: https://www.fda.gov/medical-devices/software-medical-device-samd/good-machine-learning-practice-medical-device-development-guiding-principles (accessed on 3 August 2022).
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975–2018; National Cancer Institute: Bethesda, MD, USA. Available online: https://seer.cancer.gov/csr/1975_2018/ (accessed on 3 August 2022).
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; Van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Langen, A.J.; van den Boogaart, V.; Lubberink, M.; Backes, W.H.; Marcus, J.T.; van Tinteren, H.; Pruim, J.; Brans, B.; Leffers, P.; Dingemans, A.-M.C. Monitoring response to antiangiogenic therapy in non–small cell lung cancer using imaging markers derived from PET and dynamic contrast-enhanced MRI. J. Nucl. Med. 2011, 52, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.-F.; Hsu, F.-T.; Hsieh, K.L.-C.; Kao, Y.-C.J.; Cheng, S.-J.; Hsu, J.B.-K.; Tsai, P.-H.; Chen, R.-J.; Huang, C.-C.; Yen, Y. Machine learning–based radiomics for molecular subtyping of gliomas. Clin. Cancer Res. 2018, 24, 4429–4436. [Google Scholar] [CrossRef] [Green Version]
- Salem, A.; Asselin, M.-C.; Reymen, B.; Jackson, A.; Lambin, P.; West, C.M.; O’Connor, J.P.; Faivre-Finn, C. Targeting hypoxia to improve non–small cell lung cancer outcome. JNCI J. Natl. Cancer Inst. 2018, 110, 14–30. [Google Scholar] [CrossRef] [Green Version]
- Fornacon-Wood, I.; Faivre-Finn, C.; O’Connor, J.P.; Price, G.J. Radiomics as a personalized medicine tool in lung cancer: Separating the hope from the hype. Lung Cancer 2020, 146, 197–208. [Google Scholar] [CrossRef]
- Berenguer, R.; Pastor-Juan, M.D.R.; Canales-Vázquez, J.; Castro-García, M.; Villas, M.V.; Mansilla Legorburo, F.; Sabater, S. Radiomics of CT features may be nonreproducible and redundant: Influence of CT acquisition parameters. Radiology 2018, 288, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R. The image biomarker standardization initiative: Standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8, 118–127. [Google Scholar] [CrossRef]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. A postreconstruction harmonization method for multicenter radiomic studies in PET. J. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Orlhac, F.; Frouin, F.; Nioche, C.; Ayache, N.; Buvat, I. Validation of a method to compensate multicenter effects affecting CT radiomic features. Radiology 2019, 291, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Mahon, R.; Ghita, M.; Hugo, G.D.; Weiss, E. ComBat harmonization for radiomic features in independent phantom and lung cancer patient computed tomography datasets. Phys. Med. Biol. 2020, 65, 015010. [Google Scholar] [CrossRef]
- Orlhac, F.; Lecler, A.; Savatovski, J.; Goya-Outi, J.; Nioche, C.; Charbonneau, F.; Ayache, N.; Frouin, F.; Duron, L.; Buvat, I. How can we combat multicenter variability in MR radiomics? Validation of a correction procedure. Eur. Radiol. 2021, 31, 2272–2280. [Google Scholar] [CrossRef] [PubMed]
- Kakino, R.; Nakamura, M.; Mitsuyoshi, T.; Shintani, T.; Hirashima, H.; Matsuo, Y.; Mizowaki, T. Comparison of radiomic features in diagnostic CT images with and without contrast enhancement in the delayed phase for NSCLC patients. Phys. Med. 2020, 69, 176–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, F.; Li, M.; Sun, Y.; Xiao, L.; Hua, Y. Diagnostic value of contrast-enhanced CT scans in identifying lung adenocarcinomas manifesting as GGNs (ground glass nodules). Medicine 2017, 96, e7742. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Park, C.M.; Keam, B.; Park, S.J.; Kim, M.; Kim, T.M.; Kim, D.-W.; Heo, D.S.; Goo, J.M. The prognostic value of CT radiomic features for patients with pulmonary adenocarcinoma treated with EGFR tyrosine kinase inhibitors. PLoS ONE 2017, 12, e0187500. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Yang, J.; Zhou, X.; Huang, L.; Zhao, W.; Wang, T.; Zhuang, J.; Tian, J. Development of a radiomics nomogram based on the 2D and 3D CT features to predict the survival of non-small cell lung cancer patients. Eur. Radiol. 2019, 29, 2196–2206. [Google Scholar] [CrossRef]
- Fried, D.V.; Tucker, S.L.; Zhou, S.; Liao, Z.; Mawlawi, O.; Ibbott, G.; Court, L.E. Prognostic value and reproducibility of pretreatment CT texture features in stage III non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 834–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishino, M.; Hatabu, H.; Johnson, B.E.; McLoud, T.C. State of the art: Response assessment in lung cancer in the era of genomic medicine. Radiology 2014, 271, 6–27. [Google Scholar] [CrossRef] [Green Version]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Weibull, W. A statistical distribution function of wide applicability. J. Appl. Mech. 1951, 18, 290–293. [Google Scholar] [CrossRef]
- Huang, L.; Chen, J.; Hu, W.; Xu, X.; Liu, D.; Wen, J.; Lu, J.; Cao, J.; Zhang, J.; Gu, Y. Assessment of a radiomic signature developed in a general NSCLC cohort for predicting overall survival of ALK-positive patients with different treatment types. Clin. Lung Cancer 2019, 20, e638–e651. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; van Elmpt, W.; Leijenaar, R.T.; Reymen, B.; Monshouwer, R.; Bussink, J.; Paelinck, L.; Bogaert, E.; de Wagter, C.; Elhaseen, E. Longitudinal radiomics of cone-beam CT images: Prognostic value for non-small cell lung cancer patients. Radiother. Oncol. 2019, 136, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Peng, H.; Xue, T.; Li, J.; Ge, Y.; Wang, G.; Feng, F. Prediction and verification of survival in patients with non-small-cell lung cancer based on an integrated radiomics nomogram. Clin. Radiol. 2022, 77, e222–e230. [Google Scholar] [CrossRef]
- Chen, W.; Li, M.; Mao, D.; Ge, X.; Wang, J.; Tan, M.; Ma, W.; Huang, X.; Lu, J.; Li, C.; et al. Radiomics signature on CECT as a predictive factor for invasiveness of lung adenocarcinoma manifesting as subcentimeter ground glass nodules. Sci. Rep. 2021, 11, 3633. [Google Scholar] [CrossRef]
- Kamarudin, A.N.; Cox, T.; Kolamunnage-Dona, R. Time-dependent ROC curve analysis in medical research: Current methods and applications. BMC Med. Res. Methodol. 2017, 17, 53. [Google Scholar] [CrossRef] [Green Version]
- Chang, E.; Joel, M.Z.; Chang, H.Y.; Du, J.; Khanna, O.; Omuro, A.; Chiang, V.; Aneja, S. Comparison of radiomic feature aggregation methods for patients with multiple tumors. Sci. Rep. 2021, 11, 9758. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A. Non–Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef]
- Franceschini, D.; Cozzi, L.; De Rose, F.; Navarria, P.; Fogliata, A.; Franzese, C.; Pezzulla, D.; Tomatis, S.; Reggiori, G.; Scorsetti, M. A radiomic approach to predicting nodal relapse and disease-specific survival in patients treated with stereotactic body radiation therapy for early-stage non-small cell lung cancer. Strahlenther. Onkol. 2020, 196, 922–931. [Google Scholar] [CrossRef]
- Huynh, E.; Coroller, T.P.; Narayan, V.; Agrawal, V.; Hou, Y.; Romano, J.; Franco, I.; Mak, R.H.; Aerts, H.J. CT-based radiomic analysis of stereotactic body radiation therapy patients with lung cancer. Radiother. Oncol. 2016, 120, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Xiang, P.; Ye, J.; Pang, P.; Wang, S.; Xu, M. Can texture features improve the differentiation of infiltrative lung adenocarcinoma appearing as ground glass nodules in contrast-enhanced CT? Eur. J. Radiol. 2019, 117, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Park, C.M. Can artificial intelligence fix the reproducibility problem of radiomics? Radiology 2019, 292, 374–375. [Google Scholar] [CrossRef] [PubMed]
- Coroller, T.P.; Agrawal, V.; Huynh, E.; Narayan, V.; Lee, S.W.; Mak, R.H.; Aerts, H.J. Radiomic-based pathological response prediction from primary tumors and lymph nodes in NSCLC. J. Thorac. Oncol. 2017, 12, 467–476. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | CGH (n = 338) | SCGH (n = 154) | p Value |
|---|---|---|---|
| Age (y) | 66.98 ± 12.24 | 66.62 ± 11.84 | 0.56 |
| Gender | 0.75 | ||
| Male | 183 (54.14%) | 81 (52.60%) | |
| Female | 155 (45.86%) | 73 (47.40%) | |
| Histology | 0.16 | ||
| Adenocarcinoma | 218 (64.50%) | 111 (72.08%) | |
| Squamous cell carcinoma | 73 (21.60%) | 23 (14.94%) | |
| Adenosquamous carcinoma | 11 (3.25%) | 1 (0.65%) | |
| Large cell cancer | 4 (1.18%) | 2 (1.30%) | |
| Other NSCLC | 32 (9.47%) | 17 (11.04%) | |
| Clinical T stage | 0.47 | ||
| 0 | 1 (0.30%) | 0 (0.00%) | |
| 1 | 40 (11.83%) | 18 (11.69%) | |
| 2 | 93 (27.51%) | 32 (20.78%) | |
| 3 | 70 (20.71%) | 39 (25.32%) | |
| 4 | 134 (39.64%) | 65 (42.21%) | |
| Clinical N stage | 0.59 | ||
| 0 | 108 (31.95%) | 54 (35.06%) | |
| 1 | 27 (7.99%) | 11 (7.14%) | |
| 2 | 85 (24.85%) | 44 (28.57%) | |
| 3 | 118 (34.91%) | 45 (29.22%) | |
| Clinical M stage | 0.07 | ||
| 0 | 110 (32.54%) | 63 (40.91%) | |
| 1 | 228 (67.46%) | 91 (59.09%) | |
| Clinical stage | 0.16 | ||
| I | 48 (14.20%) | 23 (14.94%) | |
| II | 12 (3.55%) | 11 (7.14%) | |
| III | 50 (14.79%) | 29 (18.83%) | |
| IV | 228 (67.46%) | 91 (59.09%) | |
| Surgery | 0.66 | ||
| None | 250 (73.96%) | 111 (72.08%) | |
| Yes | 88 (26.04%) | 43 (27.92%) | |
| Chemotherapy | 0.06 | ||
| None | 202 (59.76%) | 78 (50.65%) | |
| Yes | 136 (40.24%) | 76 (49.35%) | |
| Radiation therapy | 0.02 * | ||
| None | 217 (64.20%) | 115 (74.68%) | |
| Yes | 121 (35.80%) | 39 (25.32%) | |
| Targeted therapy | 0.36 | ||
| None | 215 (63.61%) | 104 (67.53%) | |
| Yes | 123 (36.39%) | 50 (32.47%) | |
| Smoke | 0.91 | ||
| None | 188 (55.62%) | 88 (57.14%) | |
| Yes | 138 (40.83%) | 66 (42.86%) | |
| Not available | 12 (3.55%) | 0 (0.00%) | |
| Betel nut use | <0.001 | ||
| None | 300 (88.76%) | 114 (74%) | |
| Yes | 27 (7.99%) | 22 (14.3%) | |
| Not available | 11 (3.25%) | 18 (11.7%) | |
| Alcohol use | <0.001 | ||
| None | 240 (71.01%) | 92 (59.74%) | |
| Quit drinking | 33 (9.76%) | 18 (11.69%) | |
| Sometimes | 20 (5.92%) | 11 (7.14%) | |
| Always | 34 (10.06%) | 15 (9.74%) | |
| Not available | 11 (3.25%) | 18 (11.69%) | |
| Survival Status | 0.20 | ||
| Alive | 97 (28.70%) | 53 (34.42%) | |
| Dead | 241 (71.30%) | 101 (65.58%) | |
| Duration (months) | 20.15 ± 19.95 | 12.75 ± 11.70 | <0.001 |
| Median | 12 | 11 |
| Radiomic Features | Good Outcome (n = 83) | Poor Outcome (n = 86) | b Value | p Value |
|---|---|---|---|---|
| LLL_LBP_Uniformity | 0.18 ± 0.05 | 0.20 ± 0.05 | −4.57 | 0.03 |
| LLH_Short Run Emphasis | 0.86 ± 0.08 | 0.88 ± 0.08 | −2.23 | 0.04 |
| LHL_Homogeneity 1 | 0.46 ± 0.11 | 0.40 ± 0.12 | 2.02 | 0.02 |
| HLL_Homogeneity 1 | 0.41 ± 0.09 | 0.37 ± 0.09 | 2.58 | 0.01 |
| HLL_Short Run Emphasis | 0.90 ± 0.05 | 0.92 ± 0.04 | −4.22 | 0.04 |
| HLH_Inverse variance | 0.34 ± 0.07 | 0.29 ± 0.09 | 3.45 | 0.01 |
| HLH_Short Run Emphasis | 0.90 ± 0.04 | 0.92 ± 0.04 | −4.77 | 0.02 |
| HHH_Correlation | 0.04 ± 0.06 | 0.05 ± 0.06 | 3.07 | 0.05 |
| Clinical Features | Good Outcome (n = 83) | Poor Outcome (n = 86) | chi2 Value | pValue |
| Histology | 1 [1–2] | 1 [1–2] | 8.22 | 0.08 |
| Clinical T stage | 3 [2–4] | 3 [2–4] | 50.47 | <0.001 |
| Clinical N stage | 2 [2–3] | 1 [0–2] | 15.74 | 0.03 |
| Clinical stage | IV [III–IV] | IV [II–IV] | 17.17 | 0.02 |
| Surgery | 0 [0–0] | 0 [0–1] | 7.18 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, K.-Y.; Chen, J.-R.; Wang, Y.-C.; Chiu, M.-H.; Lin, S.-P.; Mo, Y.-H.; Peng, S.-C.; Lu, C.-F. Radiomics-Based Deep Learning Prediction of Overall Survival in Non-Small-Cell Lung Cancer Using Contrast-Enhanced Computed Tomography. Cancers 2022, 14, 3798. https://doi.org/10.3390/cancers14153798
Hou K-Y, Chen J-R, Wang Y-C, Chiu M-H, Lin S-P, Mo Y-H, Peng S-C, Lu C-F. Radiomics-Based Deep Learning Prediction of Overall Survival in Non-Small-Cell Lung Cancer Using Contrast-Enhanced Computed Tomography. Cancers. 2022; 14(15):3798. https://doi.org/10.3390/cancers14153798
Chicago/Turabian StyleHou, Kuei-Yuan, Jyun-Ru Chen, Yung-Chen Wang, Ming-Huang Chiu, Sen-Ping Lin, Yuan-Heng Mo, Shih-Chieh Peng, and Chia-Feng Lu. 2022. "Radiomics-Based Deep Learning Prediction of Overall Survival in Non-Small-Cell Lung Cancer Using Contrast-Enhanced Computed Tomography" Cancers 14, no. 15: 3798. https://doi.org/10.3390/cancers14153798
APA StyleHou, K. -Y., Chen, J. -R., Wang, Y. -C., Chiu, M. -H., Lin, S. -P., Mo, Y. -H., Peng, S. -C., & Lu, C. -F. (2022). Radiomics-Based Deep Learning Prediction of Overall Survival in Non-Small-Cell Lung Cancer Using Contrast-Enhanced Computed Tomography. Cancers, 14(15), 3798. https://doi.org/10.3390/cancers14153798