
Predictive Value of 18F-FDG PET/CT Using Machine Learning for Pathological Response to Neoadjuvant Concurrent Chemoradiotherapy in Patients with Stage III Non-Small Cell Lung Cancer

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
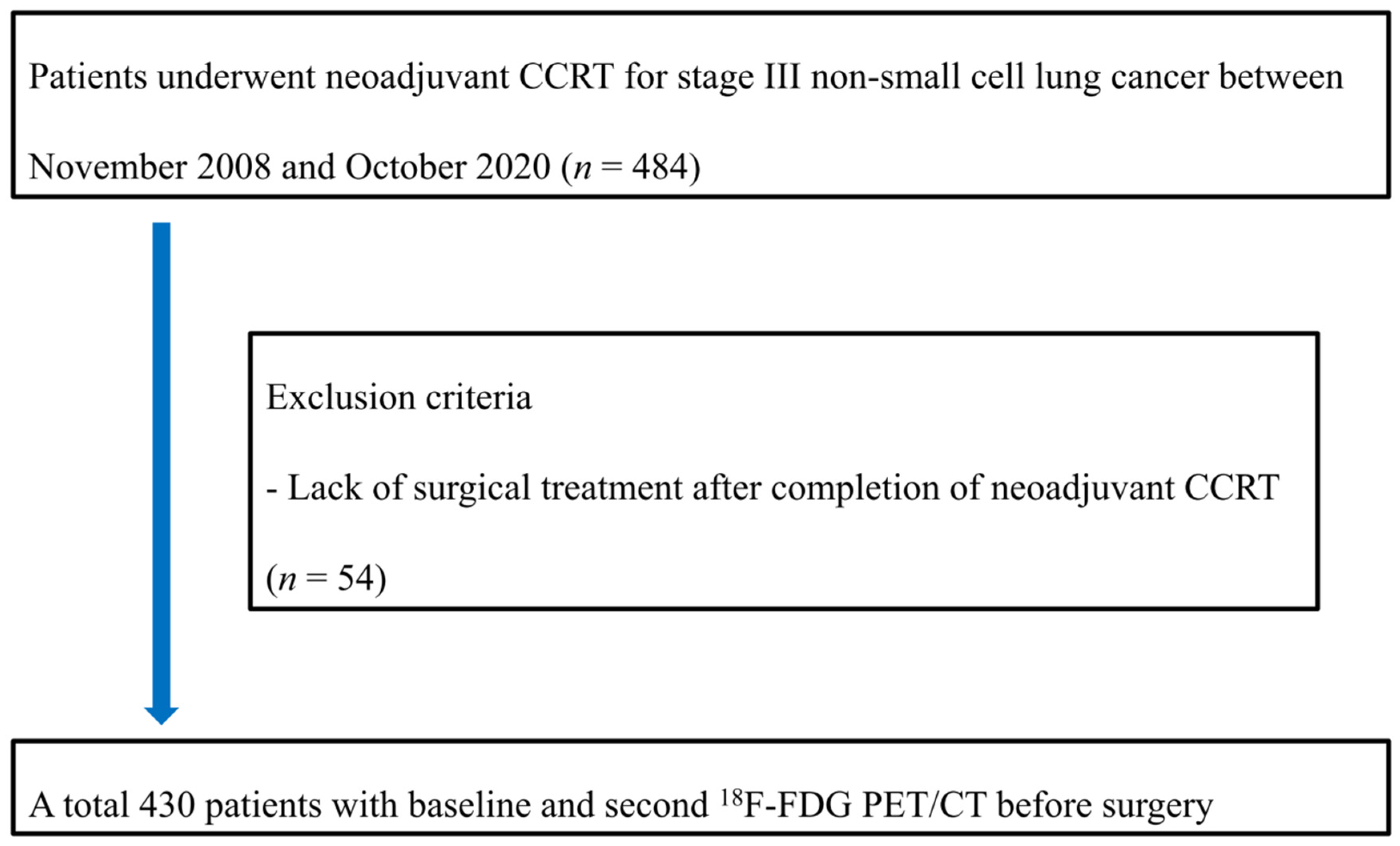
2.1. Subjects
2.2. Neoadjuvant CCRT and Histopathologic Evaluation
2.3. 18F-FDG PET/CT Analysis
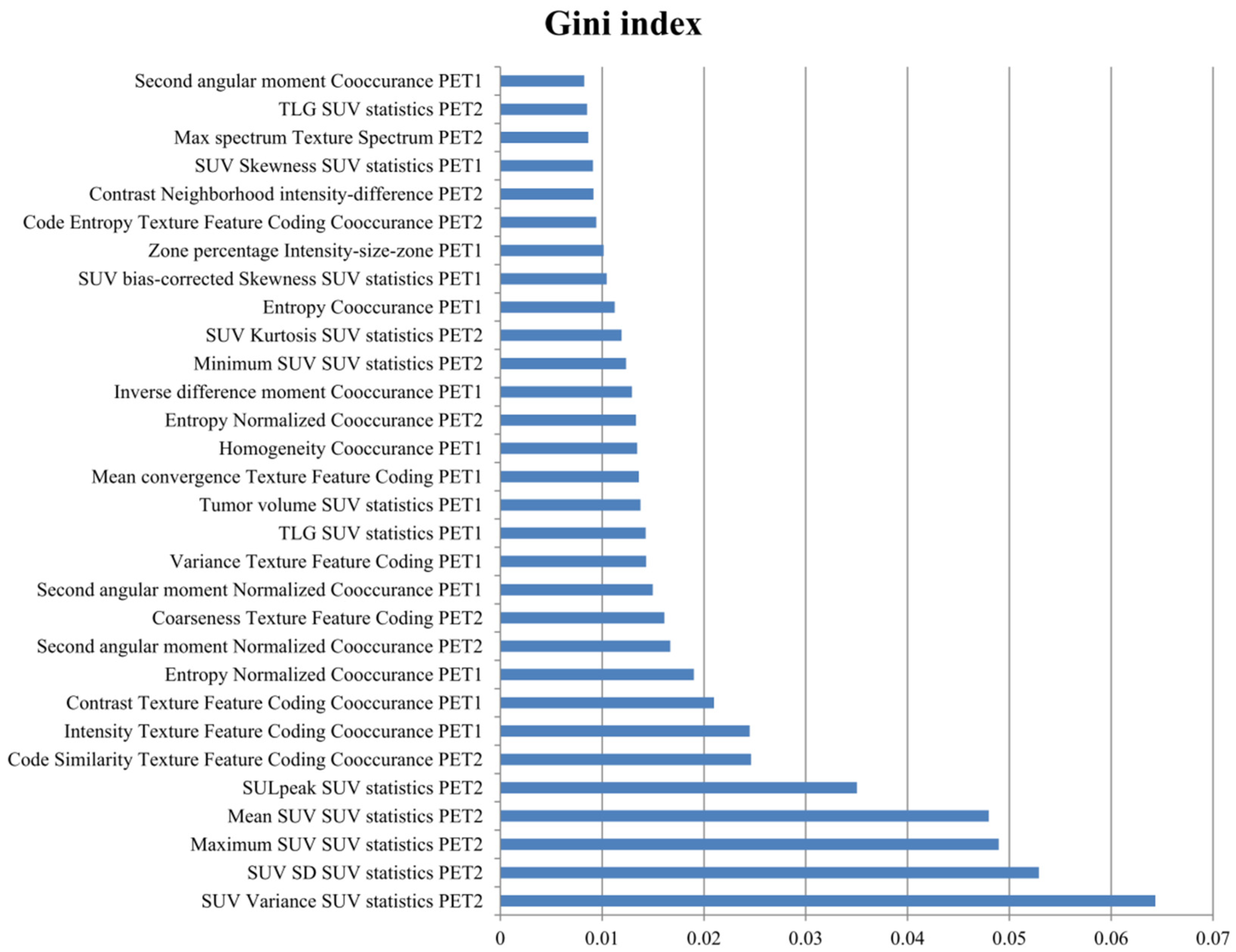
2.4. Machine Learning (ML) Model
2.5. Statistical Analysis
3. Results
3.1. Subject Characteristics
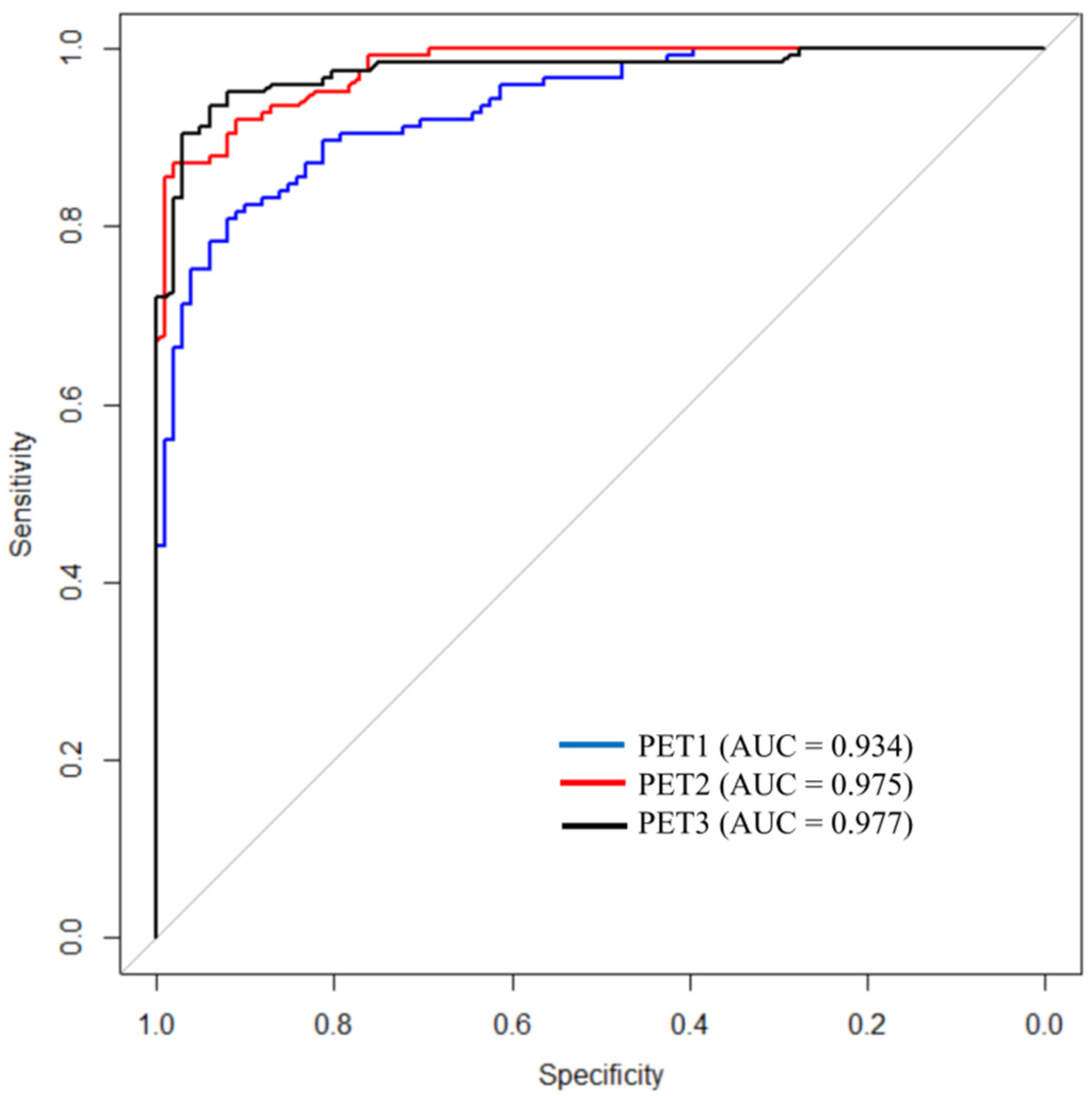
3.2. Predictive Performance of ML Model for pCR
3.3. Predictive Performances of Conventional PET Parameters and Physicians for pCR Prediction
3.4. Comparisons of the ML Model with Conventional PET Parameters and Physicians
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeSantis, C.E.; Lin, C.C.; Mariotto, A.B.; Siegel, R.L.; Stein, K.D.; Kramer, J.L.; Alteri, R.; Robbins, A.S.; Jemal, A. Cancer treatment and survivorship statistics, 2014. CA Cancer J. Clin. 2014, 64, 252–271. [Google Scholar] [CrossRef]
- Arbour, K.C.; Riely, G.J. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: A review. JAMA 2019, 322, 764–774. [Google Scholar] [CrossRef]
- Kim, H.K.; Cho, J.H.; Choi, Y.S.; Zo, J.I.; Shim, Y.M.; Park, K.; Ahn, M.-J.; Ahn, Y.C.; Kim, K.; Kim, J. Outcomes of neoadjuvant concurrent chemoradiotherapy followed by surgery for non-small-cell lung cancer with N2 disease. Lung Cancer 2016, 96, 56–62. [Google Scholar] [CrossRef]
- Hyun, S.H.; Ahn, H.K.; Ahn, M.J.; Ahn, Y.C.; Kim, J.; Shim, Y.M.; Choi, J.Y. Volume-based assessment with 18F-FDG PET/CT improves outcome prediction for patients with stage IIIA-N2 non-small cell lung cancer. AJR Am. J. Roentgenol. 2015, 205, 623–628. [Google Scholar] [CrossRef]
- Schreiner, W.; Gavrychenkova, S.; Dudek, W.; Rieker, R.J.; Lettmaier, S.; Fietkau, R.; Sirbu, H. Pathologic complete response after induction therapy-the role of surgery in stage IIIA/B locally advanced non-small cell lung cancer. J. Thorac. Dis. 2018, 10, 2795–2803. [Google Scholar] [CrossRef]
- Tenahashi, M.; Niwa, H.; Yukiue, H.; Suzuki, E.; Yoshii, N.; Watanabe, T.; Kaminuma, Y.; Chiba, K.; Tsuchida, H.; Yobita, S. Feasibility and prognostic benefit of induction chemoradiotherapy followed by surgery in patients with locally advanced non-small cell lung cancer. J. Thorc. Dis. 2020, 12, 2644–2653. [Google Scholar] [CrossRef]
- Kim, A.W.; Liptay, M.J.; Bonomi, P.; Kim, A.W.; Liptay, M.J.; Bonomi, P.; Warren, W.H.; Basu, S.; Farlow, E.C.; Faber, L.P. Neoadjuvamt chemoradiation for clinically advanced non-small-cell lung cancer: An analysis of 233 patients. Ann. Thorac. Surg. 2011, 92, 233–241, discussion 241–243. [Google Scholar] [CrossRef]
- Pottgen, C.; Eberhardt, W.; Graupner, B.; Theegarten, D.; Gauler, T.; Freitag, L.; Jawad, J.A.; Wohlschlaeger, J.; Welter, S.; Stamatis, G.; et al. Accelerated hyperfractionated radiotherapy within trimodality therapy concepts for stage IIIA/B non-small-cell lung cancer: Markedly higher rates of pathologic complete remissions than with conventional fractionation. Eur. J. Cancer 2013, 49, 2107–2115. [Google Scholar] [CrossRef]
- D’Angelillo, R.M.; Trodella, L.; Ciresa, M.; Cellini, F.; Fiore, M.; Greco, C.; Pompeo, E.; Mineo, T.C.; Paleari, L.; Granone, P.; et al. Multimodality treatment of stage III non-small cell lung cancer: Analysis of a phase III trial using preoperative cisplatin and gemcitabine with concurrent radiotherapy. J. Thorac. Oncol. 2009, 4, 1517–1523. [Google Scholar] [CrossRef]
- Stupp, R.; Mayer, M.; Kann, R.; Weder, W.; Zouhair, A.; Betticher, D.C.; Pless, M. Neoadjuvant chemotherapy and radiotherapy followed by surgery in selected patients with stage IIIB non-small-cell lung cancer: A multicetre phase III trial. Lancet Oncol. 2009, 10, 785–793. [Google Scholar] [CrossRef]
- Cremonesi, M.; Gilardi, L.; Ferrari, M.E.; Piperno, G.; Travaini, L.L.; Timmerman, R.; Botta, F.; Baroni, G.; Grana, C.M.; Ronchi, S.; et al. Role of interim 18F-FDG PET/CT for the early prediction of clinical outcomes of non-small cell lung cancer (NSCLC) during radiotherapy or chemo-radiotherapy. A systematic review. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1915–1927. [Google Scholar] [CrossRef]
- Roengvoraphoj, O.; Wijaya, C.; Eze, C.; Li, M.; Dantes, M.; Taugner, J.; Tufman, A.; Huber, R.M.; Belka, C.; Manapov, F. Analysis of primary tumor metabolic volume during chemoradiotherapy in locally advanced non-small cell lung cancer. Strahlenther. Onkol. 2018, 194, 107–115. [Google Scholar] [CrossRef]
- Pöttgen, C.; Levegrün, S.; Theegarten, D.; Marnitz, S.; Grehl, S.; Pink, R.; Eberhardt, W.; Stamatis, G.; Gauler, T.; Antoch, G.; et al. Value of 18F-fluoro-2-deoxy-D-glucose-positron emission tomography/computed tomography in non-small-cell lung cancer for prediction of pathologic response and times to relapse after neoadjuvant chemoradiotherapy. Clin. Cancer Res. 2006, 12, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Cerfolio, R.J.; Bryant, A.S.; Winokur, T.S.; Ohja, B.; Bartolucci, A.A. Repeat FDG-PET after neoadjuvant therapy is a predictor of pathologic response in patients with non-small cell lung cancer. Ann. Thorac. Surg. 2004, 78, 1903–1909. [Google Scholar] [CrossRef]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar] [CrossRef] [Green Version]
- Joo Hyun, O.; Lodge, M.A.; Wahl, R.L. Practical PERCIST: A simplified guide to PET response criteria in solid tumors 1.0. Radiology 2016, 280, 576–584. [Google Scholar]
- De Ruysscher, D.; Houben, A.; Aerts, H.J.; Dehing, C.; Wanders, R.; Öllers, M.; Lambin, P. Increased (18)F-deoxyglucose uptake in the lung during the first weeks of radiotherapy is correlated with subsequent radiation-induced lung toxicity (RILT): A prospective pilot study. Radiother. Oncol. 2009, 91, 415–420. [Google Scholar] [CrossRef]
- Szyszko, T.A.; Yip, C.; Szlosarek, P.; Goh, V.; Cook, G.J. The role of new PET tracers for lung cancer. Lung Cancer 2019, 94, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, J.; Cheon, M.; Park, Y.J.; Hyun, S.H.; Zo, J.I.; Um, S.W.; Choi, J.Y. Machine learning-based diagnostic method of pre-therapeutic 18F-FDG PET/CT for evaluating mediastinal lymph nodes in non-small cell lung cancer. Eur. Radiol. 2021, 31, 4184–4194. [Google Scholar] [CrossRef]
- Rami-Porta, R.; Crowley, J.J.; Goldstraw, P. The revised TNM staging system for lung cancer. Ann. Thorac. Cardiovasc. Surg. 2009, 15, 4–9. [Google Scholar]
- Shin, S.; Kim, H.K.; Cho, J.H.; Choi, Y.S.; Kim, K.; Kim, J.; Zo, J.I.; Sun, J.; Ahn, M.; Park, K.; et al. Adjuvant therapy in stage IIIA-N2 non-small cell lung cancer after neoadjuvant concurrent chemotherapy followed surgery. J. Thorac. Dis. 2020, 12, 2602–2613. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, T.R.; Thompson, E.D.; Forde, P.M.; Stein, J.E.; Duffield, A.S.; Anagnostou, V.; Rekhtman, N.; Anders, R.A.; Cuda, J.D.; Illei, P.B.; et al. Pathologic features of response to neoadjuvant anti-PD-1 in resected non-small-cell lung carcinoma: A proposal for quantitative immune-related pathologic response criteria (irPRC). Ann. Oncol. 2018, 29, 1853–1860. [Google Scholar] [CrossRef] [PubMed]
- Mouillet, G.; Monnet, E.; Milleron, B.; Puyraveau, M.; Quoix, E.; David, P.; Ducoloné, A.; Molinier, O.; Zalcman, G.; Depierre, A.; et al. Pathologic complete response to preoperative chemotherapy predicts cure in early-stage non-small-cell lung cancer: Combined analysis of two IFCT radomized trials. J. Thorac. Oncol. 2012, 7, 841–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, P.; Wang, X.; Xu, C.; Liu, C.; Zheng, C.; Fulham, M.J.; Feng, D.; Wang, L.; Song, S.; Huang, G. (18)F-FDG PET/CT radiomic predictors of pathologic complete response (pCR) to neoadjuvant chemotherapy in breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1116–1126. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.C.; Chen, S.W.; Wu, K.C.; Lee, P.Y.; Feng, C.L.; Hsieh, T.C.; Yen, K.; Kao, C. Predicting pathological complete response in rectal cancer after chemoradiotherapy with a random forest using 18F-fluorodeoxyglucose positron emission tomography and computed tomography radiomics. Ann. Transl. Med. 2020, 8, 207. [Google Scholar] [CrossRef] [PubMed]
- Tahmassebi, A.; Wengert, G.J.; Helbich, T.H.; Bago-Horvath, Z.; Alaei, S.; Bartsch, R.; Dubsky, P.; Baltzer, P.; Clauser, P.; Kapetas, P.; et al. Impact of machine learning with parametric magnetic resonance imaging of the breast for early prediction of response to neoadjuvant chemotherapy and survival outcomes in breast cancer patients. Investig. Radiol. 2019, 54, 110–117. [Google Scholar] [CrossRef]
- Yakar, M.; Etiz, D.; Metintas, M.; Ak, G.; Celik, O. Prediction of radiation pneumonitis with machine learning in stage III lung cancer: A pilot study. Technol. Cancer Res. Treat. 2021, 20, 15330338211016373. [Google Scholar] [CrossRef]
- Meti, N.; Saednia, K.; Lagree, A.; Tabbarah, S.; Mohebpour, M.; Kiss, A.; Lu, F.; Slodkowska, E.; Gandhi, S.; Jerzak, K.J.; et al. Machine learning frameworks to predict neoadjuvant chemotherapy response in breast cancer using clinical and pathological features. JCO Clin. Cancer Inform. 2021, 5, 66–80. [Google Scholar] [CrossRef]
- Lo Gullo, R.; Eskreis-Winkler, S.; Morris, E.A.; Pinker, K. Machine learning with multiparametric magnetic resonance imaging of the breast for early prediction of response to neoadjuvant chemotherapy. Breast 2020, 49, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Huang, M.; Huang, C.; Tsai, H.; Su, W.; Chang, W.; Wang, J.; Shi, H. Machine learning for predicting pathological complete response in patients with locally advanced rectal cancer after neoadjuvant chemoradiotherapy. Sci. Rep. 2020, 10, 12555. [Google Scholar] [CrossRef]
- Eun, N.L.; Kang, D.; Son, E.J.; Park, J.S.; Youk, J.H.; Kim, J.A.; Gweon, H.M. Texture analysis with 3.0-T MRI for association of response to neoadjuvant chemotherapy in breast cancer. Radiology 2020, 294, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Antunovic, L.; de Sanctis, R.; Cozzi, L.; Kirienko, M.; Sagona, A.; Torrisi, R.; Tinterri, C.; Santoro, A.; Chiti, A.; Zelic, R.; et al. PET/CT radiomics in breast cancer: Promising tool for prediction of pathological response to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Park, S.; Bang, J.I.; Kim, E.K.; Lee, H.Y. Metabolic radiomics for pretreatment (18)F-FDG PET/CT to characterize locally advanced breast cancer: Histopathologic characteristics, response to neoadjuvant chemotherapy, and prognosis. Sci. Rep. 2017, 7, 1556. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, B.; Frenzel, T.; Schmitz, R.; Schumacher, U.; Wedemann, G. Modeling growth of tumors and their spreading behavior using mathematical functions. Methods Mol. Biol. 2019, 1878, 263–277. [Google Scholar] [PubMed]
- Sollini, M.; Cozzi, L.; Antunovic, L.; Chiti, A.; Kirienko, M. PET radiomics in NSCLC: State of the art and a proposal for harmonization of methodology. Sci. Rep. 2017, 7, 358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iravani, A.; Turgeon, G.A.; Akhurst, T.; Callahan, J.W.; Bressel, M.; Everitt, S.J.; Siva, S.; Hofman, M.S.; Hicks, R.J.; Ball, D.L.; et al. PET-detected pneumonitis following curative-intent chemoradiation in non-small cell lung cancer (NSCLC): Recognizing patterns and assessing the impact on the predictive ability of FDG-PET/CT response assessment. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1869–1877. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. | |
|---|---|---|
| Sex | Male | 309 (71.9%) |
| Female | 121 (28.1%) | |
| Age (years) | Mean (range) | 61.8 (31.1–79.5) |
| Tumor pathology | Adenocarcinoma | 289 (67.2%) |
| Squamous cell carcinoma | 125 (29.1%) | |
| Others | 16 (3.7%) | |
| Stage (AJCC 7th) | IIIa | 415 (96.5%) |
| IIIb | 15 (3.5%) | |
| Type of surgery | Lobectomy | 339 (78.8%) |
| Bilobectomy | 32 (7.4%) | |
| Pneumonectomy | 23 (5.4%) | |
| Lobectomy with en bloc wedge resection | 36 (8.4%) | |
| Viable tumor on pathologic specimen | Mean % (range) | 28.8 (0–95.0) |
| Pathologic response | pCR | 54 (12.6%) |
| Non-pCR | 376 (87.4%) | |
| Response by PERCIST | CMR | 72 (16.7%) |
| PMR | 281 (65.4%) | |
| SMD | 72 (16.7%) | |
| PMD | 5 (1.2%) |
| ML Model | AUC | ACC | F1 | Precision | Recall |
|---|---|---|---|---|---|
| PET1 | 0.934 *,† | 0.827 *,† | 0.853 *,† | 0.802 *,† | 0.912 † |
| PET2 | 0.975 * | 0.902 *,‡ | 0.912 *,‡ | 0.905 *,‡ | 0.920 |
| PET3 | 0.977 † | 0.934 †,‡ | 0.940 †,‡ | 0.937 †,‡ | 0.944 † |
| Pathologic Response | p-Value | ||||
|---|---|---|---|---|---|
| pCR | Non-pCR | ||||
| PET1 | SUVmax | Median | 13.59 | 11.58 | 0.029 * |
| IQR | 10.01–17.47 | 8.35–15.53 | |||
| SUVmean | Median | 5.91 | 5.28 | 0.037 * | |
| IQR | 4.86–7.48 | 3.97–6.69 | |||
| MTV (cm3) | Median | 42.96 | 21.13 | 0.003 * | |
| IQR | 16.02–74.89 | 7.38–47.48 | |||
| TLG | Median | 223.26 | 113.63 | 0.001 * | |
| IQR | 96.29–436.26 | 30.77–279.36 | |||
| PET2 | SUVmax | Median | 3.17 | 4.57 | <0.001 * |
| IQR | 2.22–4.13 | 2.92–6.98 | |||
| SUVmean | Median | 1.69 | 2.35 | <0.001 * | |
| IQR | 1.43–2.15 | 1.74–3.33 | |||
| MTV (cm3) | Median | 10.40 | 8.71 | 0.327 | |
| IQR | 3.64–27.11 | 3.64–19.46 | |||
| TLG | Median | 19.42 | 22.00 | 0.475 | |
| IQR | 6.32–47.35 | 8.61–56.52 | |||
| Delta PET parameters (%) | dSUVmax | Median | 74.68 | 58.14 | <0.001 * |
| IQR | 64.25–84.25 | 36.07–74.20 | |||
| dSUVmean | Median | 70.17 | 50.79 | <0.001 * | |
| IQR | 54.34–78.57 | 31.58–66.28 | |||
| dMTV (cm3) | Median | 68.63 | 48.18 | 0.003 * | |
| IQR | 42.81–82.49 | 14.76–71.75 | |||
| dTLG | Median | 89.52 | 73.68 | <0.001 * | |
| IQR | 79.40–95.47 | 50.80–88.83 | |||
| Cutoff | AUC | Sen (%) | Spe (%) | PPV (%) | NPV (%) | ACC (%) | |
|---|---|---|---|---|---|---|---|
| PET1-SUVmax | >13.15 | 0.592 | 57.4 | 61.7 | 17.7 | 90.9 | 61.2 |
| PET1-SUVmean | >4.70 | 0.588 | 79.6 | 39.1 | 15.8 | 93.0 | 44.2 |
| PET1-MTV (cm3) | >41.11 | 0.627 | 53.7 | 70.2 | 20.6 | 91.3 | 68.1 |
| PET1-TLG | >142.97 | 0.635 | 68.5 | 57.1 | 18.9 | 92.7 | 59.1 |
| PET2-SUVmax | ≤3.97 | 0.687 | 74.1 | 58.8 | 20.5 | 94.0 | 60.7 |
| PET2-SUVmean | ≤1.83 | 0.726 | 66.7 | 71.5 | 25.2 | 93.7 | 70.9 |
| dSUVmax | >56.5% | 0.737 | 88.9 | 48.7 | 19.9 | 96.8 | 53.7 |
| dSUVmean | >43.9% | 0.745 | 94.4 | 42.8 | 19.2 | 98.2 | 49.3 |
| dMTV (cm3) | >55.4% | 0.625 | 68.5 | 56.6 | 18.5 | 92.6 | 58.1 |
| dTLG | >86.2% | 0.703 | 68.5 | 69.1 | 24.2 | 93.9 | 69.1 |
| Physicians | 33.9 | 86.4 | 29.2 | 90.8 | 80.5 | ||
| ML model | 0.977 | 94.4 | 92.2 | 93.7 | 93.1 | 93.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J.; Lee, J.; Cheon, M.; Woo, S.-K.; Ahn, M.-J.; Pyo, H.R.; Choi, Y.S.; Han, J.H.; Choi, J.Y. Predictive Value of 18F-FDG PET/CT Using Machine Learning for Pathological Response to Neoadjuvant Concurrent Chemoradiotherapy in Patients with Stage III Non-Small Cell Lung Cancer. Cancers 2022, 14, 1987. https://doi.org/10.3390/cancers14081987
Yoo J, Lee J, Cheon M, Woo S-K, Ahn M-J, Pyo HR, Choi YS, Han JH, Choi JY. Predictive Value of 18F-FDG PET/CT Using Machine Learning for Pathological Response to Neoadjuvant Concurrent Chemoradiotherapy in Patients with Stage III Non-Small Cell Lung Cancer. Cancers. 2022; 14(8):1987. https://doi.org/10.3390/cancers14081987
Chicago/Turabian StyleYoo, Jang, Jaeho Lee, Miju Cheon, Sang-Keun Woo, Myung-Ju Ahn, Hong Ryull Pyo, Yong Soo Choi, Joung Ho Han, and Joon Young Choi. 2022. "Predictive Value of 18F-FDG PET/CT Using Machine Learning for Pathological Response to Neoadjuvant Concurrent Chemoradiotherapy in Patients with Stage III Non-Small Cell Lung Cancer" Cancers 14, no. 8: 1987. https://doi.org/10.3390/cancers14081987
APA StyleYoo, J., Lee, J., Cheon, M., Woo, S. -K., Ahn, M. -J., Pyo, H. R., Choi, Y. S., Han, J. H., & Choi, J. Y. (2022). Predictive Value of 18F-FDG PET/CT Using Machine Learning for Pathological Response to Neoadjuvant Concurrent Chemoradiotherapy in Patients with Stage III Non-Small Cell Lung Cancer. Cancers, 14(8), 1987. https://doi.org/10.3390/cancers14081987