
Azacitidine Plus Venetoclax for the Treatment of Relapsed and Newly Diagnosed Acute Myeloid Leukemia Patients


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Patient Samples Molecular Characterization
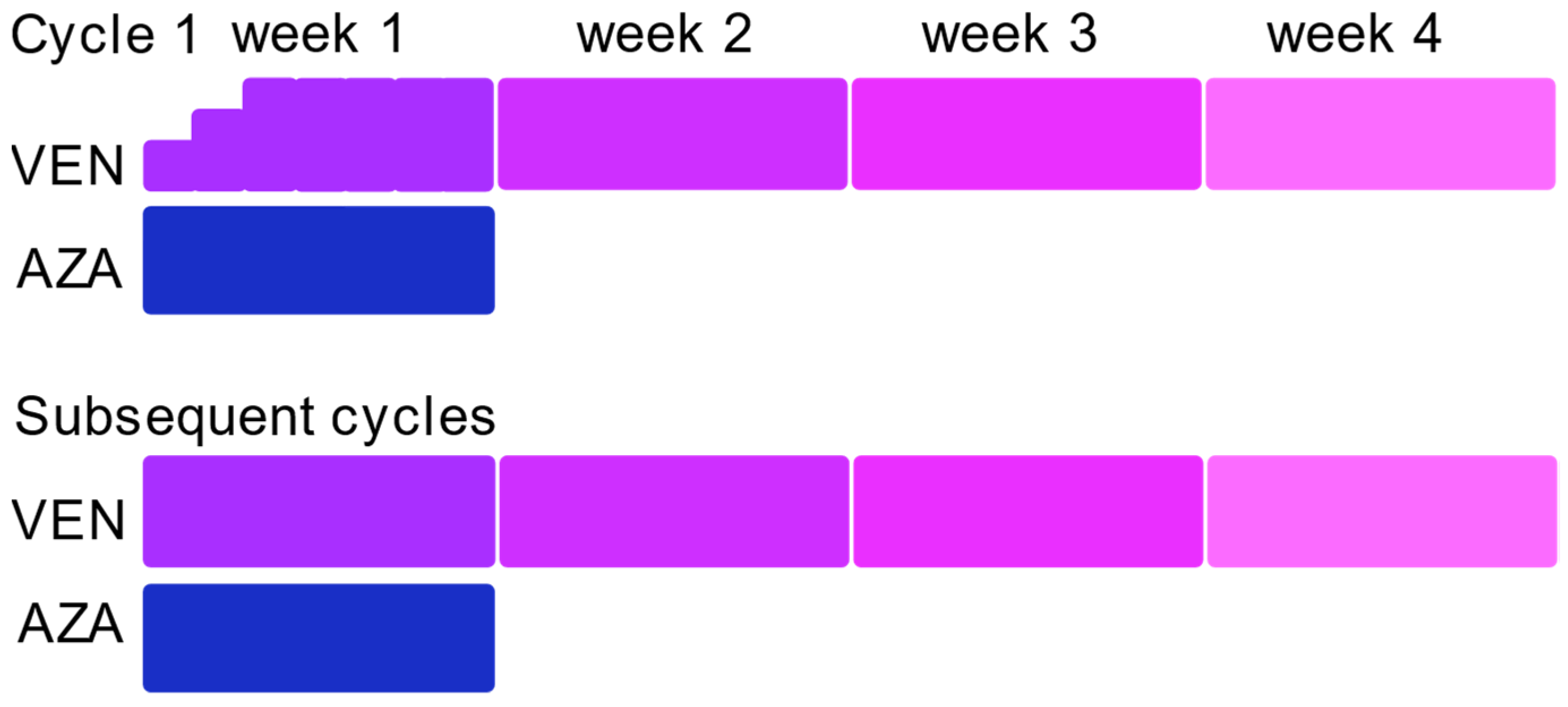
2.3. Treatment Modalities
2.4. Assessment of Response
2.5. Statistical Analysis
3. Results
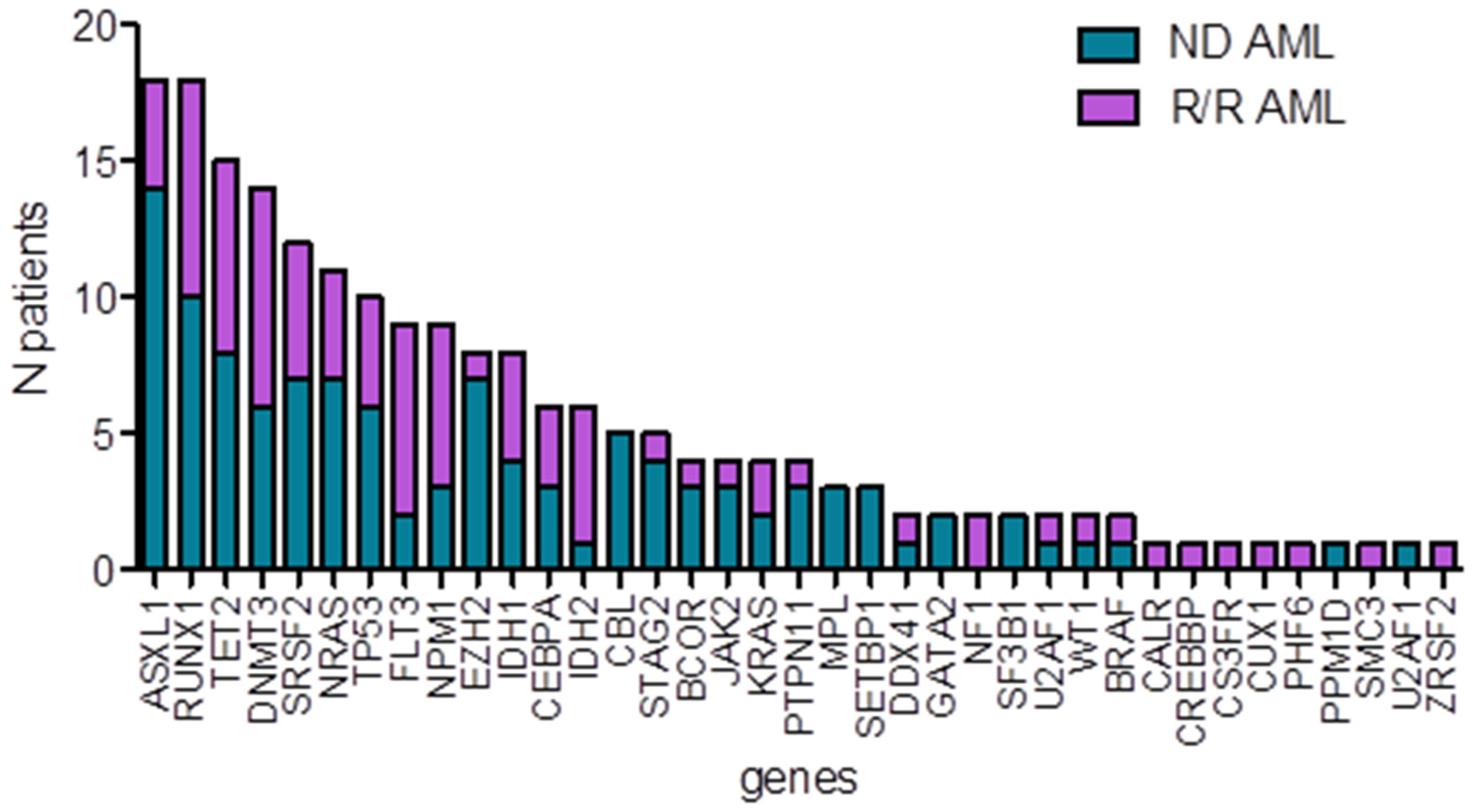
3.1. Patient Clinical and Molecular Characteristics
3.2. Treatment
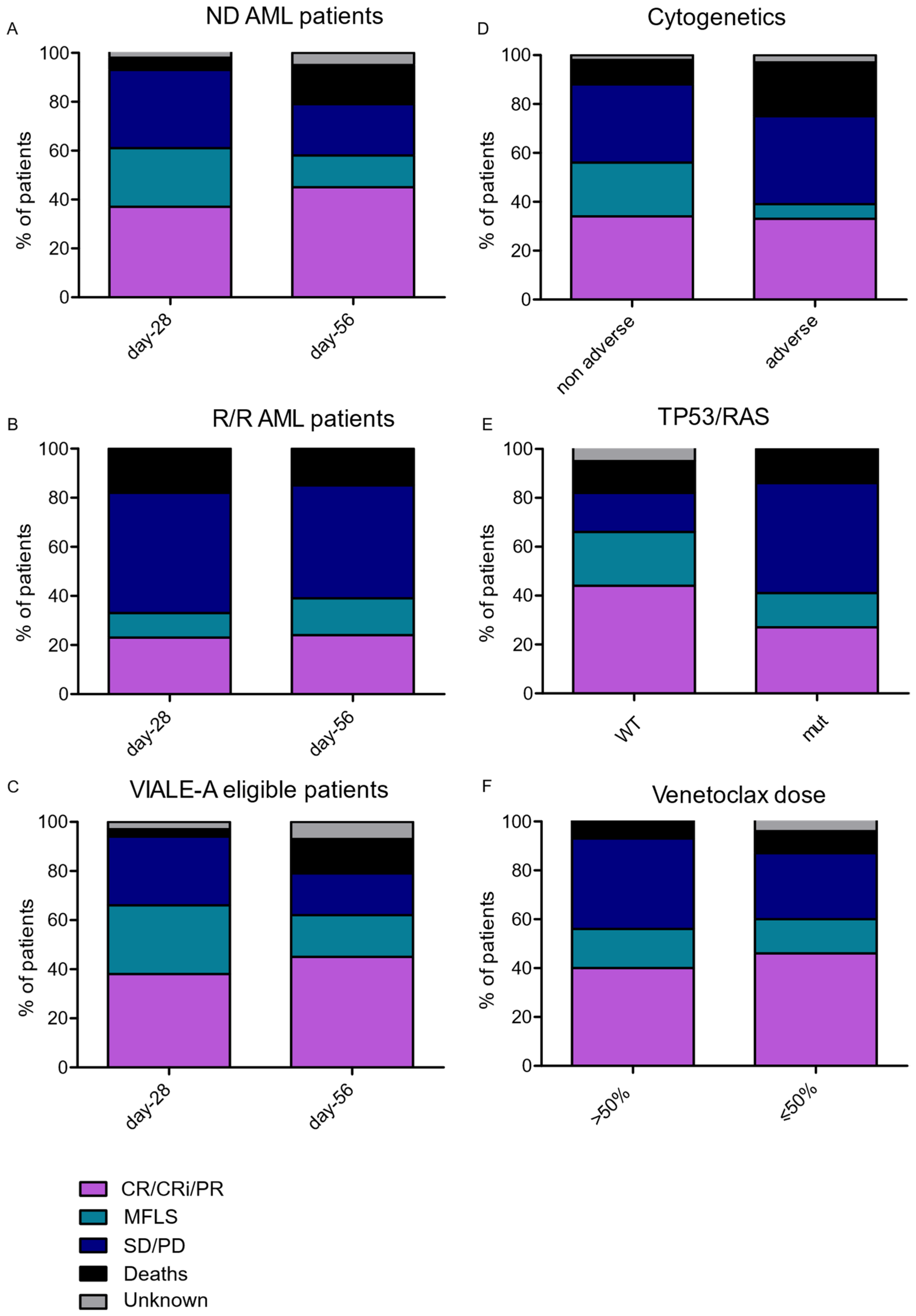
3.3. Treatment Response
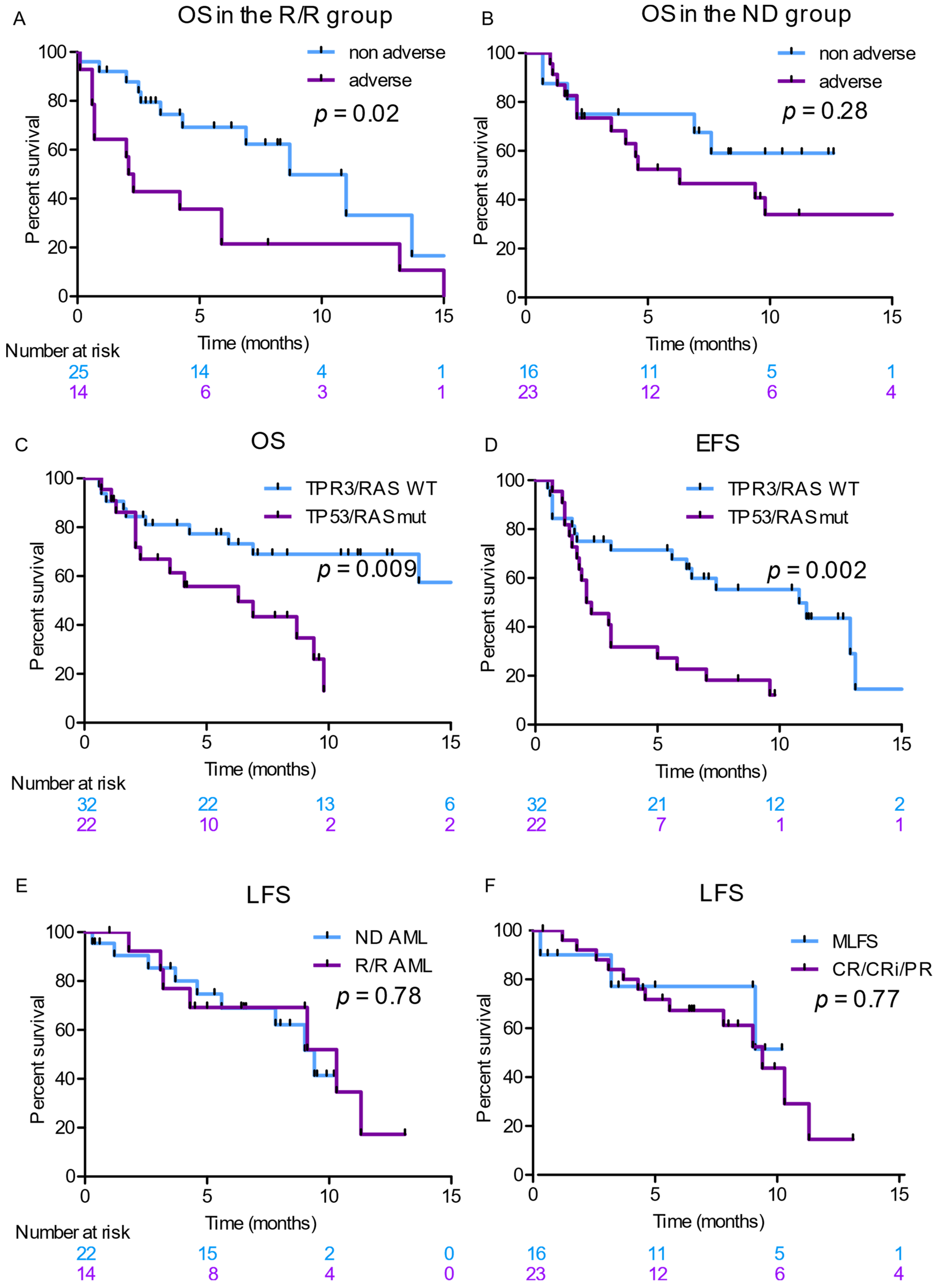
3.4. Survival Analyses
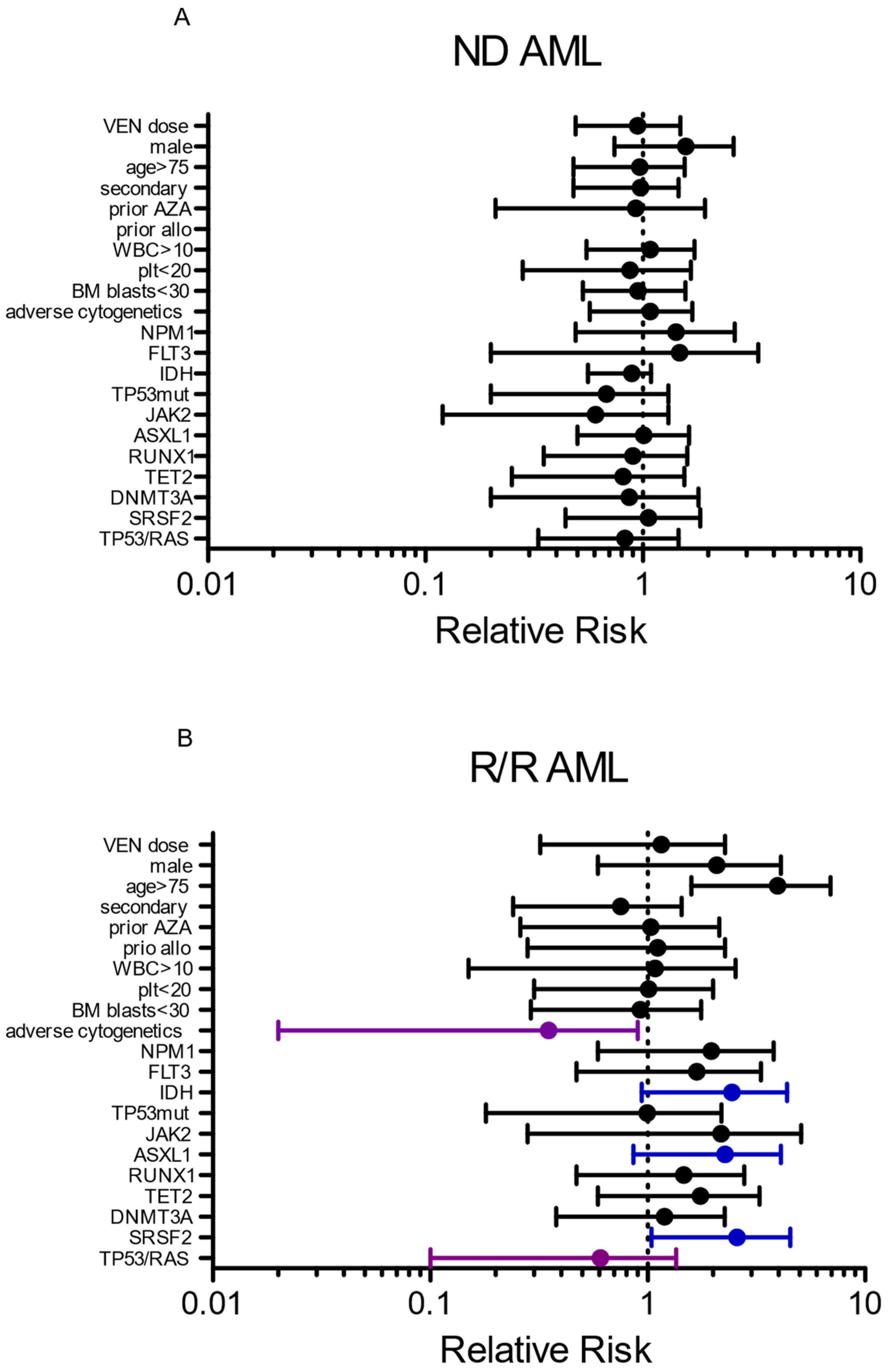
3.5. Risk Factor Associated with Response and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Döhner, H.; Weisdorf, D.J.; Bloomfield, C.D. Acute Myeloid Leukemia. N. Engl. J. Med. 2015, 373, 1136–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souers, A.J.; Leverson, J.D.; Boghaert, E.R.; Ackler, S.L.; Catron, N.D.; Chen, J.; Dayton, B.D.; Ding, H.; Enschede, S.H.; Fairbrother, W.J.; et al. ABT-199, a potent and selective BCL-2 inhibitor, achieves antitumor activity while sparing platelets. Nat. Med. 2013, 19, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Pan, R.; Hogdal, L.J.; Benito, J.M.; Bucci, D.; Han, L.; Borthakur, G.; Cortes, J.; De Angelo, D.J.; De Bose, L.; Mu, H.; et al. Selective BCL-2 inhibition by ABT-199 causes on-target cell death in acute myeloid leukemia. Cancer Discov. 2014, 4, 362–375. [Google Scholar] [CrossRef] [Green Version]
- Konopleva, M.; Letai, A. BCL-2 inhibition in AML: An unexpected bonus? Blood 2018, 132, 1007–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiNardo, C.D.; Pratz, K.W.; Letai, A.; Jonas, B.; Wei, A.H.; Thirman, M.; Arellano, M.; Frattini, M.G.; Kantarjian, H.; Popovic, R.; et al. Safety and preliminary efficacy of venetoclax with decitabine or azacitidine in elderly patients with previously untreated acute myeloid leukaemia: A non-randomised, open-label, phase 1b study. Lancet Oncol. 2018, 19, 216–228. [Google Scholar] [CrossRef]
- Dinardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Garciaz, S.; Saillard, C.; Hicheri, Y.; Hospital, M.-A.; Vey, N. Venetoclax in Acute Myeloid Leukemia: Molecular Basis, Evidences for Preclinical and Clinical Efficacy and Strategies to Target Resistance. Cancers 2021, 13, 5608. [Google Scholar] [CrossRef]
- Kim, K.; Maiti, A.; Loghavi, S.; Pourebrahim, R.; Kadia, T.M.; Rausch, C.R.; Furudate, K.; Daver, N.G.; Alvarado, Y.; Ohanian, M.; et al. Outcomes of TP53-mutant acute myeloid leukemia with decitabine and venetoclax. Cancer 2021, 127, 3772–3781. [Google Scholar] [CrossRef]
- Di Nardo, C.D.; Tiong, I.S.; Quaglieri, A.; MacRaild, S.; Loghavi, S.; Brown, F.C.; Thijssen, R.; Pomilio, G.; Ivey, A.; Salmon, J.; et al. Molecular patterns of response and treatment failure after frontline venetoclax combinations in older patients with AML. Blood 2020, 135, 791–803. [Google Scholar] [CrossRef]
- Feld, J.; Tremblay, D.; Dougherty, M.; Czaplinska, T.; Sanchez, G.; Brady, C.; Kremyanskaya, M.; Bar-Natan, M.; Keyzner, A.; Marcellino, B.K.; et al. Safety and Efficacy: Clinical Experience of Venetoclax in Combination with Hypomethylating Agents in Both Newly Diagnosed and Relapsed/Refractory Advanced Myeloid Malignancies. Hemasphere 2021, 5, e549. [Google Scholar] [CrossRef]
- Stomper, J.; Rotondo, J.C.; Greve, G.; Lübbert, M. Hypomethylating agents (HMA) for the treatment of acute myeloid leukemia and myelodysplastic syndromes: Mechanisms of resistance and novel HMA-based therapies. Leukemia 2021, 35, 1873–1889. [Google Scholar] [CrossRef] [PubMed]
- Thol, F.; Ganser, A. Treatment of Relapsed Acute Myeloid Leukemia. Curr. Treat. Options Oncol. 2020, 21, 66. [Google Scholar] [CrossRef] [PubMed]
- Bewersdorf, J.P.; Giri, S.; Wang, R.; Williams, R.T.; Tallman, M.S.; Zeidan, A.M.; Stahl, M. Venetoclax as monotherapy and in combination with hypomethylating agents or low dose cytarabine in relapsed and treatment refractory acute myeloid leukemia: A systematic review and meta-analysis. Haematologica 2020, 105, 2659–2663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morsia, E.; McCullough, K.; Joshi, M.; Cook, J.; Alkhateeb, H.B.; Al-Kali, A.; Begna, K.; Elliott, M.; Hogan, W.; Litzow, M.; et al. Venetoclax and hypomethylating agents in acute myeloid leukemia: Mayo Clinic series on 86 patients. Am. J. Hematol. 2020, 95, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Brancati, S.; Gozzo, L.; Romano, G.L.; Vetro, C.; Dulcamare, I.; Maugeri, C.; Parisi, M.; Longo, L.; Vitale, D.C.; Di Raimondo, F.; et al. Venetoclax in Relapsed/Refractory Acute Myeloid Leukemia: Are Supporting Evidences Enough? Cancers 2021, 14, 22. [Google Scholar] [CrossRef]
- Stahl, M.; Menghrajani, K.; Derkach, A.; Chan, A.; Xiao, W.; Glass, J.; King, A.C.; Daniyan, A.F.; Famulare, C.; Cuello, B.M.; et al. Clinical and molecular predictors of response and survival following venetoclax therapy in relapsed/refractory AML. Blood Adv. 2021, 5, 1552–1564. [Google Scholar] [CrossRef]
- Dinardo, C.D.; Rausch, C.R.; Benton, C.; Kadia, T.; Jain, N.; Pemmaraju, N.; Daver, N.; Covert, W.; Marx, K.R.; Mace, M.; et al. Clinical experience with the BCL2-inhibitor venetoclax in combination therapy for relapsed and refractory acute myeloid leukemia and related myeloid malignancies. Am. J. Hematol. 2018, 93, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Ram, R.; Amit, O.; Zuckerman, T.; Gurion, R.; Raanani, P.; Bar-On, Y.; Avivi, I.; Wolach, O. Venetoclax in patients with acute myeloid leukemia refractory to hypomethylating agents-a multicenter historical prospective study. Ann. Hematol. 2019, 98, 1927–1932. [Google Scholar] [CrossRef]
- Aldoss, I.; Yang, D.; Pillai, R.; Sanchez, J.F.; Mei, M.; Aribi, A.; Ali, H.; Sandhu, K.; Al Malki, M.M.; Salhotra, A.; et al. Association of leukemia genetics with response to venetoclax and hypomethylating agents in relapsed/refractory acute myeloid leukemia. Am. J. Hematol. 2019, 94, E253–E255. [Google Scholar] [CrossRef] [Green Version]
- Ganzel, C.; Ram, R.; Gural, A.; Wolach, O.; Gino-Moor, S.; Vainstein, V.; Nachmias, B.; Apel, A.; Koren-Michowitz, M.; Pasvolsky, O.; et al. Venetoclax is safe and efficacious in relapsed/refractory AML. Leuk. Lymphoma 2020, 61, 2221–2225. [Google Scholar] [CrossRef]
- Wang, Y.-W.; Tsai, C.; Lin, C.-C.; Tien, F.-M.; Chen, Y.-W.; Lin, H.-Y.; Yao, M.; Lin, Y.-C.; Cheng, C.-L.; Tang, J.-L.; et al. Cytogenetics and mutations could predict outcome in relapsed and refractory acute myeloid leukemia patients receiving BCL-2 inhibitor venetoclax. Ann. Hematol. 2020, 99, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Tenold, M.E.; Moskoff, B.N.; Benjamin, D.J.; Hoeg, R.T.; Rosenberg, A.S.; Abedi, M.; Tuscano, J.M.; Jonas, B.A. Outcomes of Adults With Relapsed/Refractory Acute Myeloid Leukemia Treated with Venetoclax Plus Hypomethylating Agents at a Comprehensive Cancer Center. Front. Oncol. 2021, 11, 649209. [Google Scholar] [CrossRef] [PubMed]
- Piccini, M.; Pilerci, S.; Merlini, M.; Grieco, P.; Scappini, B.; Bencini, S.; Peruzzi, B.; Caporale, R.; Signori, L.; Pancani, F.; et al. Venetoclax-Based Regimens for Relapsed/Refractory Acute Myeloid Leukemia in a Real-Life Setting: A Retrospective Single-Center Experience. J. Clin. Med. 2021, 10, 1684. [Google Scholar] [CrossRef]
- Aldoss, I.; Dadwal, S.; Zhang, J.; Tegtmeier, B.; Mei, M.; Arslan, S.; Al Malki, M.M.; Salhotra, A.; Ali, H.; Aribi, A.; et al. Invasive fungal infections in acute myeloid leukemia treated with venetoclax and hypomethylating agents. Blood Adv. 2019, 3, 4043–4404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papayannidis, C.; Nanni, J.; Cristiano, G.; Marconi, G.; Sartor, C.; Parisi, S.; Zannoni, L.; Saed, R.; Ottaviani, E.; Bandini, L.; et al. Impact of infectious comorbidity and overall time of hospitalization in total outpatient management of acute myeloid leukemia patients following venetoclax and hypomethylating agents. Eur. J. Haematol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Devillier, R.; Gelsi-Boyer, V.; Brecqueville, M.; Carbuccia, N.; Murati, A.; Vey, N.; Birnbaum, D.; Mozziconacci, M.-J. Acute myeloid leukemia with myelodysplasia-related changes are characterized by a specific molecular pattern with high frequency of ASXL1 mutations. Am. J. Hematol. 2012, 87, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Tenny, S.; Hoffman, M.R. Relative Risk. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022; Available online: http://www.ncbi.nlm.nih.gov/books/NBK430824/ (accessed on 7 April 2022).
- Stel, V.S.; Dekker, F.W.; Tripepi, G.; Zoccali, C.; Jager, K.J. Survival analysis II: Cox regression. Nephron Clin. Pract. 2011, 119, c255–c260. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Konopleva, M.; Pollyea, D.A.; Potluri, J.; Chyla, B.; Hogdal, L.; Busman, T.; McKeegan, E.; Salem, A.H.; Zhu, M.; Ricker, J.L.; et al. Efficacy and Biological Correlates of Response in a Phase II Study of Venetoclax Monotherapy in Patients with Acute Myelogenous Leukemia. Cancer Discov. 2016, 6, 1106–1117. [Google Scholar] [CrossRef] [Green Version]
- DiNardo, C.D.; Maiti, A.; Rausch, C.R.; Pemmaraju, N.; Naqvi, K.; Daver, N.G.; Kadia, T.M.; Borthakur, G.; Ohanian, M.; Alvarado, Y.; et al. 10-day decitabine with venetoclax for newly diagnosed intensive chemotherapy ineligible, and relapsed or refractory acute myeloid leukaemia: A single-centre, phase 2 trial. Lancet Haematol. 2020, 7, e724–e736. [Google Scholar] [CrossRef]
- Cherry, E.M.; Abbott, D.; Amaya, M.; McMahon, C.; Schwartz, M.; Rosser, J.; Sato, A.; Schowinsky, J.T.; Inguva, A.; Minhajuddin, M.; et al. Venetoclax and azacitidine compared with induction chemotherapy for newly diagnosed patients with acute myeloid leukemia. Blood Adv. 2021, 5, 5565–5573. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Riley-Gillis, B.; Han, L.; Jia, Y.; Lodi, A.; Zhang, H.; Ganesan, S.; Pan, R.; Konoplev, S.N.; Sweeney, S.R.; et al. Activation of RAS/MAPK pathway confers MCL-1 mediated acquired resistance to BCL-2 inhibitor venetoclax in acute myeloid leukemia. Signal Transduct. Target. Ther. 2022, 7, 51. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, N.E.; Ramachandra, N.; Sahu, S.; Gitego, N.; Lopez, A.; Pradhan, K.; Bhagat, T.D.; Gordon-Mitchell, S.; Pena, B.R.; Kazemi, M.; et al. ASXL1 mutations are associated with distinct epigenomic alterations that lead to sensitivity to venetoclax and azacytidine. Blood Cancer J. 2021, 11, 157. [Google Scholar] [CrossRef]
- Traina, F.; Visconte, V.; Elson, P.; Tabarroki, A.; Jankowska, A.M.; Hasrouni, E.; Sugimoto, Y.; Szpurka, H.; Makishima, H.; O’Keefe, C.L.; et al. Impact of molecular mutations on treatment response to DNMT inhibitors in myelodysplasia and related neoplasms. Leukemia 2014, 28, 78–87. [Google Scholar] [CrossRef]
- Fleischmann, M.; Scholl, S.; Frietsch, J.J.; Hilgendorf, I.; Schrenk, K.; Hammersen, J.; Prims, F.; Thiede, C.; Hochhaus, A.; Schnetzke, U. Clinical experience with venetoclax in patients with newly diagnosed, relapsed, or refractory acute myeloid leukemia. J. Cancer Res. Clin. Oncol. 2022. [Google Scholar] [CrossRef]
- Bhatt, S.; Pioso, M.S.; Olesinski, E.A.; Yilma, B.; Ryan, J.A.; Mashaka, T.; Leutz, B.; Adamia, S.; Zhu, H.; Kuang, Y.; et al. Reduced Mitochondrial Apoptotic Priming Drives Resistance to BH3 Mimetics in Acute Myeloid Leukemia. Cancer Cell 2020, 38, 872–890.e6. [Google Scholar] [CrossRef]
- Herbaux, C.; Kornauth, C.; Poulain, S.; Chong, S.J.F.; Collins, M.C.; Valentin, R.; Hackett, L.; Tournilhac, O.; Lemonnier, F.; Dupuis, J.; et al. BH3 profiling identifies ruxolitinib as a promising partner for venetoclax to treat T-cell prolymphocytic leukemia. Blood 2021, 137, 3495–3506. [Google Scholar] [CrossRef]
- Ni Chonghaile, T.; Sarosiek, K.A.; Vo, T.-T.; Ryan, J.A.; Tammareddi, A.; Moore, V.D.G.; Deng, J.; Anderson, K.C.; Richardson, P.; Tai, Y.-T.; et al. Pretreatment mitochondrial priming correlates with clinical response to cytotoxic chemotherapy. Science 2011, 334, 1129–1133. [Google Scholar] [CrossRef] [Green Version]
- Diepstraten, S.T.; Anderson, M.A.; Czabotar, P.E.; Lessene, G.; Strasser, A.; Kelly, G.L. The manipulation of apoptosis for cancer therapy using BH3-mimetic drugs. Nat. Rev. Cancer 2022, 22, 45–64. [Google Scholar] [CrossRef]
- Garciaz, S.; Guirguis, A.A.; Müller, S.; Brown, F.C.; Chan, Y.-C.; Motazedian, A.; Rowe, C.L.; Kuzich, J.A.; Chan, K.L.; Tran, K.; et al. Pharmacologic Reduction of Mitochondrial Iron Triggers a Noncanonical BAX/BAK-Dependent Cell Death. Cancer Discov. 2022, 12, 774–791. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Ni, M.; Ma, D.; Fang, Q.; Zhang, Y.; Li, Y.; Huang, Y.; Chen, Y.; Chai, X.; Zhan, Y.; et al. Venetoclax plus azacitidine and donor lymphocyte infusion in treating acute myeloid leukemia patients who relapse after allogeneic hematopoietic stem cell transplantation. Ann. Hematol. 2022, 101, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Pollyea, D.A.; Winters, A.; McMahon, C.; Schwartz, M.; Jordan, C.T.; Rabinovitch, R.; Abbott, D.; Smith, C.A.; Gutman, J.A. Venetoclax and azacitidine followed by allogeneic transplant results in excellent outcomes and may improve outcomes versus maintenance therapy among newly diagnosed AML patients older than 60. Bone Marrow Transplant. 2022, 57, 160–166. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 77) | ND (n = 38) | R/R (n = 39) | |||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p Value | |
| Patients characteristics | |||||||
| Male | 45 | 58 | 21 | 55 | 24 | 62 | 0.54 |
| Age, median (range) | 72 | (22–86) | 73 | (61–81) | 69 | (22–86) | <0.001 |
| WBC, median (range) | 3 | (0.1–73) | 4 | (0.4–63) | 2.9 | (0.1–73) | 0.153 |
| ANC, median (range) | 0.8 | (0–19) | 1.05 | (0–19) | 0.65 | (0–10) | 0.011 |
| plt count, median (range) | 48 | (3–471) | 90 | (3–365) | 23 | (7–471) | 0.221 |
| BM blasts, median (range) | 31 | 7–92 | 36 | 7–88 | 31 | 8–92 | 0.827 |
| AML classification | |||||||
| Secondary AML | 47 | 61 | 28 | 74 | 19 | 49 | 0.035 |
| AML-MRC | 27 | 35 | 15 | 39 | 12 | 31 | - |
| therapy-related | 7 | 9 | 4 | 11 | 3 | 8 | - |
| post MPN | 13 | 17 | 9 | 24 | 4 | 10 | - |
| Previous treatments | |||||||
| Azacitidine | 16 | 21 | 6 | 16 | 10 | 26 | 0.401 |
| median cycle (range) | 6 | (3–20) | 6 | (3–13) | 5 | (3–20) | - |
| Chemotherapy | 33 | 43 | - | - | 33 | 85 | - |
| Median number of line | 1 | 1–4 | - | - | 1 | 1–4 | - |
| Allogenic transplantation | 10 | 13 | - | - | 10 | 26 | - |
| Cytogenetics | |||||||
| Adverse cytogenetics | 36 | 47 | 22 | 58 | 14 | 36 | 0.468 |
| monosomal | 24 | 31 | 13 | 34 | 11 | 28 | 0.628 |
| complex | 23 | 30 | 13 | 34 | 10 | 26 | 0.462 |
| Genomic alteration | |||||||
| NPM1 | 9 | 12 | 3 | 8 | 6 | 15 | 0.481 |
| FLT3 | 9 | 12 | 2 | 5 | 7 | 18 | 0.154 |
| ITD | 6 | 8 | 0 | 0 | 6 | 15 | - |
| TKD | 3 | 4 | 2 | 5 | 1 | 3 | - |
| IDH (n = 75) | 18 | 24 | 8 | 21 | 10 | 27 | 0.827 |
| IDH1 | 10 | 13 | 7 | 18 | 3 | 8 | - |
| IDH2 | 8 | 11 | 1 | 3 | 7 | 19 | - |
| TP53 (n = 68) | 15 | 22 | 8 | 23 | 7 | 22 | 1 |
| JAK2 (n = 62) | 10 | 16 | 8 | 24 | 2 | 7 | 0.092 |
| ASXL1 (n = 54) | 18 | 33 | 14 | 47 | 4 | 17 | 0.162 |
| RUNX1 (n = 54) | 18 | 33 | 10 | 33 | 8 | 33 | 1 |
| TET2 (n = 54) | 15 | 28 | 8 | 27 | 7 | 29 | 1 |
| DNMT3A (n = 54) | 14 | 26 | 6 | 20 | 8 | 33 | 0.353 |
| RAS (n = 54) | 14 | 26 | 8 | 27 | 6 | 25 | 1 |
| NRAS | 11 | 20 | 7 | 23 | 4 | 17 | - |
| KRAS | 3 | 6 | 1 | 3 | 2 | 8 | - |
| SFSR2 (n = 54) | 12 | 22 | 7 | 23 | 5 | 21 | 1 |
| Overall Response Rate | Multivariate | |||
|---|---|---|---|---|
| Variable | OR | Confidence Interval | p Value | |
| Inferior | Superior | |||
| age | 1.038 | 0.99 | 1.089 | 0.12 |
| prior vidaza exposure | 0.404 | 0.108 | 1.507 | 0.177 |
| status (R/R versus ND) | 0.403 | 0.131 | 1.238 | 0.113 |
| adverse cytogenetics | 0.404 | 0.139 | 1.171 | 0.095 |
| Overall survival | Multivariate | |||
| variable | HR | Confidence interval | p value | |
| Inferior | Superior | |||
| age | 1.011 | 0.986 | 1.037 | 0.393 |
| prior vidaza exposure | 0.885 | 0.416 | 1.886 | 0.752 |
| status (R/R versus ND) | 0.483 | 0.247 | 0.944 | 0.033 |
| adverse cytogenetics | 0.442 | 0.227 | 0.862 | 0.017 |
| Event-free survival | Multivariate | |||
| variable | HR | Confidence interval | p value | |
| Inferior | Superior | |||
| age | 0.99 | 0.971 | 1.01 | 0.319 |
| prior vidaza exposure | 0.756 | 0.389 | 1.472 | 0.411 |
| status (R/R versus ND) | 0.499 | 0.27 | 0.923 | 0.027 |
| adverse cytogenetics | 0.466 | 0.262 | 0.83 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garciaz, S.; Hospital, M.-A.; Alary, A.-S.; Saillard, C.; Hicheri, Y.; Mohty, B.; Rey, J.; D’Incan, E.; Charbonnier, A.; Villetard, F.; et al. Azacitidine Plus Venetoclax for the Treatment of Relapsed and Newly Diagnosed Acute Myeloid Leukemia Patients. Cancers 2022, 14, 2025. https://doi.org/10.3390/cancers14082025
Garciaz S, Hospital M-A, Alary A-S, Saillard C, Hicheri Y, Mohty B, Rey J, D’Incan E, Charbonnier A, Villetard F, et al. Azacitidine Plus Venetoclax for the Treatment of Relapsed and Newly Diagnosed Acute Myeloid Leukemia Patients. Cancers. 2022; 14(8):2025. https://doi.org/10.3390/cancers14082025
Chicago/Turabian StyleGarciaz, Sylvain, Marie-Anne Hospital, Anne-Sophie Alary, Colombe Saillard, Yosr Hicheri, Bilal Mohty, Jérôme Rey, Evelyne D’Incan, Aude Charbonnier, Ferdinand Villetard, and et al. 2022. "Azacitidine Plus Venetoclax for the Treatment of Relapsed and Newly Diagnosed Acute Myeloid Leukemia Patients" Cancers 14, no. 8: 2025. https://doi.org/10.3390/cancers14082025
APA StyleGarciaz, S., Hospital, M. -A., Alary, A. -S., Saillard, C., Hicheri, Y., Mohty, B., Rey, J., D’Incan, E., Charbonnier, A., Villetard, F., Maisano, V., Lombardi, L., Ittel, A., Mozziconacci, M. -J., Gelsi-Boyer, V., & Vey, N. (2022). Azacitidine Plus Venetoclax for the Treatment of Relapsed and Newly Diagnosed Acute Myeloid Leukemia Patients. Cancers, 14(8), 2025. https://doi.org/10.3390/cancers14082025