
Role of Etiology in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Counterfactual Event-Based Mediation Analysis


 ,
,  , , , ,
, , , ,  , , ,
, , ,  ,
,  ,
, 
 , ,
, ,  ,
,  on behalf of A.I.G.O. (Italian Association of Hospital Gastroenterologists)add
Show full author list
on behalf of A.I.G.O. (Italian Association of Hospital Gastroenterologists)add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Treatment
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Patients
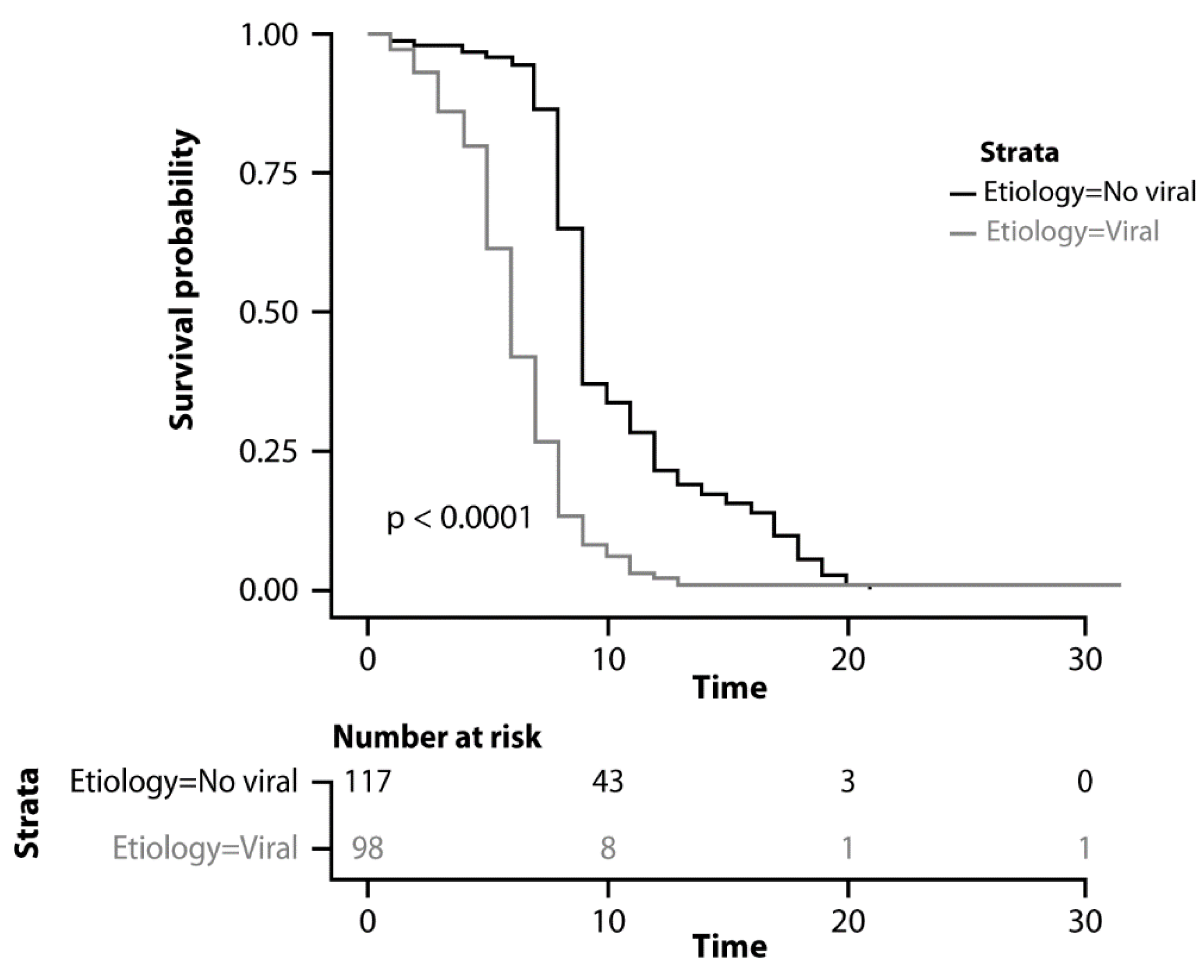
3.2. Overall Survival
3.3. Progression-Free Survival
3.4. Other Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [Green Version]
- Ponziani, F.R.; Bhoori, S.; Germini, A.; Bongini, M.; Flores, M.; Sposito, C.; Facciorusso, A.; Gasbarrini, A.; Mazzaferro, V. Inducing tolerability of adverse events increases sorafenib exposure and optimizes patient’s outcome in advanced hepatocellular carcinoma. Liver. Int. 2016, 36, 1033–1042. [Google Scholar] [CrossRef]
- Laface, C.; Fedele, P.; Maselli, F.M.; Ambrogio, F.; Foti, C.; Molinari, P.; Ammendola, M.; Lioce, M.; Ranieri, G. Targeted therapy for hepatocellular carcinoma: Old and new opportunities. Cancers 2022, 14, 4028. [Google Scholar] [CrossRef]
- Zhou, M.; Liu, B.; Shen, J. Immunotherapy for hepatocellular carcinoma. Clin. Exp. Med. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Cabibbo, G.; Aghemo, A.; Lai, Q.; Masarone, M.; Montagnese, S.; Ponziani, F.R.; Italian Association for the Study of the Liver (AISF). Optimizing systemic therapy for advanced hepatocellular carcinoma: The key role of liver function. Dig. Liver. Dis. 2022, 54, 452–460. [Google Scholar] [CrossRef]
- Falette Puisieux, M.; Pellat, A.; Assaf, A.; Ginestet, C.; Brezault, C.; Dhooge, M.; Soyer, P.; Coriat, R. Therapeutic management of advanced hepatocellular carcinoma: An updated review. Cancers 2022, 14, 2357. [Google Scholar] [CrossRef]
- Decraecker, M.; Toulouse, C.; Blanc, J.F. Is There still a place for tyrosine kinase inhibitors for the treatment of hepatocellular carcinoma at the time of immunotherapies? A focus on lenvatinib. Cancers 2021, 13, 6310. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Facciorusso, A.; Tartaglia, N.; Villani, R.; Serviddio, G.; Ramai, D.; Mohan, B.P.; Chandan, S.; Abd El Aziz, M.A.; Evangelista, J.; Cotsoglou, C.; et al. Lenvatinib versus sorafenib as first-line therapy of advanced hepatocellular carcinoma: A systematic review and meta-analysis. Am. J. Trans. Res. 2021, 13, 2379–2387. [Google Scholar]
- Rimini, M.; Kudo, M.; Tada, T.; Shigeo, S.; Kang, W.; Suda, G.; Jefremow, A.; Burgio, V.; Iavarone, M.; Tortora, R.; et al. Nonalcoholic steatohepatitis in hepatocarcinoma: New insights about its prognostic role in patients treated with lenvatinib. ESMO Open 2021, 6, 100330. [Google Scholar] [CrossRef] [PubMed]
- Burgio, V.; Iavarone, M.; Di Costanzo, G.G.; Marra, F.; Lonardi, S.; Tamburini, E.; Piscaglia, F.; Masi, G.; Celsa, C.; Foschi, F.G.; et al. Real-life clinical data of lenvatinib versus sorafenib for unresectable hepatocellular carcinoma in Italy. Cancer Manag. Res. 2021, 13, 9379–9389. [Google Scholar] [CrossRef]
- Kuo, Y.H.; Lu, S.N.; Chen, Y.Y.; Kee, K.M.; Yen, Y.H.; Hung, C.H.; Hu, T.H.; Chen, C.H.; Wang, J.H. Real-world Lenvatinib versus sorafenib in patients with advanced hepatocellular carcinoma: A propensity score matching analysis. Front. Oncol. 2021, 11, 737767. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Tada, T.; Tani, J.; Kariyama, K.; Fukunishi, S.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; et al. Real-life Practice Experts for HCC (RELPEC) Study Group and HCC 48 Group (hepatocellular carcinoma experts from 48 clinics in Japan). Efficacy of lenvatinib for unresectable hepatocellular carcinoma based on background liver disease etiology: Multi-center retrospective study. Sci. Rep. 2021, 11, 16663. [Google Scholar]
- Tada, T.; Kumada, T.; Hiraoka, A.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; et al. Real-life Practice Experts for HCC (RELPEC) Study Group and the HCC 48 Group (hepatocellular carcinoma experts from 48 clinics in Japan). Impact of modified albumin-bilirubin grade on survival in patients with HCC who received lenvatinib. Sci. Rep. 2021, 11, 14474. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Takaguchi, K.; Atsukawa, M.; Itobayashi, E.; Tsuji, K.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Real-life Practice Experts for HCC (RELPEC) Study Group, HCC 48 Group (hepatocellular carcinoma experts from 48 clinics in Japan). Clinical features of lenvatinib for unresectable hepatocellular carcinoma in real-world conditions: Multicenter analysis. Cancer Med. 2019, 8, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Takaguchi, K.; Itobayashi, E.; Shimada, N.; Tajiri, K.; Tsuji, K.; Ishikawa, T.; Ochi, H.; et al. Real-life Practice Experts for HCC (RELPEC) Study Group and the HCC 48 Group (hepatocellular carcinoma experts from 48 clinics in Japan). Therapeutic potential of lenvatinib for unresectable hepatocellular carcinoma in clinical practice: Multicenter analysis. Hepatol. Res. 2019, 49, 111–117. [Google Scholar]
- Obi, S.; Sato, T.; Sato, S.; Kanda, M.; Tokudome, Y.; Kojima, Y.; Suzuki, Y.; Hosoda, K.; Kawai, T.; Kondo, Y.; et al. The efficacy and safety of lenvatinib for advanced hepatocellular carcinoma in a real-world setting. Hepatol. Int. 2019, 13, 199–204. [Google Scholar] [CrossRef]
- Rimini, M.; Shimose, S.; Lonardi, S.; Tada, T.; Masi, G.; Iwamoto, H.; Lai, E.; Burgio, V.; Hiraoka, A.; Ishikawa, T.; et al. Lenvatinib versus sorafenib as first-line treatment in hepatocellular carcinoma: A multi-institutional matched case-control study. Hepatol. Res. 2021, 51, 1229–1241. [Google Scholar] [CrossRef]
- Abd El Aziz, M.A.; Facciorusso, A.; Nayfeh, T.; Saadi, S.; Elnaggar, M.; Cotsoglou, C.; Sacco, R. Immune Checkpoint Inhibitors for Unresectable Hepatocellular Carcinoma. Vaccines 2020, 8, 616. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.; Núñez, N.G.; Pinyol, R.; Govaere, O.; Pinter, M.; Szydlowska, M.; Gupta, R.; Qiu, M.; Deczkowska, A.; Weiner, A.; et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature 2021, 592, 450–456. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Lencioni, R. mRECIST for HCC: Performance and novel refinements. J. Hepatol. 2020, 72, 288–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathurin, P.; Bataller, R. Trends in the management and burden of alcoholic liver disease. J. Hepatol. 2015, 62, S38–S46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasanelli, F.; Giraudo, M.T.; Ricceri, F.; Valeri, L.; Zugna, D. Marginal time-dependent causal effects in mediation analysis with survival data. Am. J. Epidemiol. 2019, 188, 967–974. [Google Scholar] [CrossRef]
- Facciorusso, A.; Abd El Aziz, M.A.; Sacco, R. Efficacy of Regorafenib in Hepatocellular Carcinoma Patients: A Systematic Review and Meta-Analysis. Cancers 2019, 12, 36. [Google Scholar] [CrossRef] [Green Version]
- Garuti, F.; Neri, A.; Avanzato, F.; Gramenzi, A.; Rampoldi, D.; Rucci, P.; Farinati, F.; Giannini, E.G.; Piscaglia, F.; Rapaccini, G.L.; et al. The changing scenario of hepatocellular carcinoma in Italy: An update. Liver. Int. 2021, 41, 585–597. [Google Scholar] [CrossRef]
- Kim, S.; Kim, K.H.; Kim, B.K.; Park, J.Y.; Ahn, S.H.; Kim, D.Y.; Kim, S.U. Lenvatinib is independently associated with the reduced risk of progressive disease when compared to sorafenib in patients with advanced hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2021, 36, 1317–1325. [Google Scholar] [CrossRef]
- Nakano, M.; Kuromatsu, R.; Niizeki, T.; Okamura, S.; Iwamoto, H.; Shimose, S.; Shirono, T.; Noda, Y.; Kamachi, N.; Koga, H.; et al. Primary Treatment with Molecular-Targeted Agents for Hepatocellular Carcinoma: A Propensity Score-matching Analysis. Hepatol. Commun. 2020, 4, 1218–1228. [Google Scholar] [CrossRef]
- Tomonari, T.; Sato, Y.; Tanaka, H.; Mitsuhashi, T.; Hirao, A.; Tanaka, T.; Taniguchi, T.; Okamoto, K.; Sogabe, M.; Miyamoto, H.; et al. Therapeutic efficacy of lenvatinib in nonviral unresectable hepatocellular carcinoma. JGH Open 2021, 5, 1275–1283. [Google Scholar] [CrossRef]
- Hatanaka, T.; Kakizaki, S.; Nagashima, T.; Namikawa, M.; Ueno, T.; Tojima, H.; Takizawa, D.; Naganuma, A.; Arai, H.; Harimoto, N.; et al. Lenvatinib for hepatocellular carcinoma patients with nonviral infection who were unlikely to respond to immunotherapy: A retrospective, comparative study. Oncology 2021, 99, 641–651. [Google Scholar] [CrossRef]
- Mishra, G.; Majeed, A.; Dev, A.; Eslick, G.D.; Pinato, D.J.; Izumoto, H.; Hiraoka, A.; Huo, T.-I.; Liu, P.-H.; Johnson, P.J.; et al. Clinical Utility of Albumin Bilirubin Grade as a Prognostic Marker in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization: A Systematic Review and Meta-analysis. J. Gastrointest. Cancer 2022, in press. [Google Scholar] [CrossRef]
- Facciorusso, A.; Del Prete, V.; Crucinio, N.; Serviddio, G.; Vendemiale, G.; Muscatiello, N. Lymphocyte-to-monocyte ratio predicts survival after radiofrequency ablation for colorectal liver metastases. World J. Gastroenterol. 2016, 22, 4211–4218. [Google Scholar] [CrossRef]
- Llamosas-Falcon, L.; Shield, K.D.; Gelovany, M.; Manthey, J.; Rehm, J. Alcohol use disorders and the risk of progression of liver disease in people with hepatitis C virus infection-a systematic review. Subst. Abus. Treat Prev. Policy 2020, 15, 45. [Google Scholar] [CrossRef]
- Luna-Cuadros, M.A.; Chen, H.W.; Hanif, H.; Ali, M.J.; Khan, M.M.; Lau, D.T. Risk of hepatocellular carcinoma after hepatitis C virus cure. World J. Gastroenterol. 2022, 28, 96–107. [Google Scholar] [CrossRef]
- Kai, K.; Koga, H.; Aishima, S.; Kawaguchi, A.; Yamaji, K.; Ide, T.; Ueda, J.; Noshiro, H. Impact of smoking habit on surgical outcomes in non-B non-C patients with curative resection for hepatocellular carcinoma. World J. Gastroenterol. 2017, 23, 1397–1405. [Google Scholar] [CrossRef]
- Costentin, C.E.; Mourad, A.; Lahmek, P.; Causse, X.; Pariente, A.; Hagège, H.; Dobrin, A.S.; Becker, C.; Marks, B.; Bader, R.; et al. Hepatocellular carcinoma is diagnosed at a later stage in alcoholic patients: Results of a prospective, nationwide study. Cancer 2018, 124, 1964–1972. [Google Scholar] [CrossRef]
- Zamor, P.J.; deLemos, A.S.; Russo, M.W. Viral hepatitis and hepatocellular carcinoma: Etiology and management. J. Gastrointest Oncol. 2017, 8, 229–242. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Nonviral Etiology (98 Patients) | Viral Etiology (215 Patients) | p-Value |
|---|---|---|---|
| Age (years) | 74 (56–82) | 72 (58–84) | 0.39 |
| Gender (male) | 77 (78.5%) | 172 (80%) | 0.77 |
| ECOG PS 0 | 79 (80.6%) | 174 (80.9%) | 0.94 |
| Child-Pugh A | 86 (87.7%) | 182 (84.6%) | 0.46 |
| BCLC: • Stage B • Stage C | 29 (39.8%) 59 (60.2%) | 82 (38.1%) 133 (61.9%) | 0.39 |
| AFP (UI/mL) | 255.9 (142.1–570) | 250.5 (139.2–615) | 0.71 |
| Sustained virological response * | – | 184 (85.5%) | – |
| Previous radical or locoregional therapy | 58 (59.1%) | 136 (63.2%) | 0.67 |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Age (reference ≤ 65 years) | 0.86 (0.56–1.45) | 0.26 | ||
| Gender (reference Female) | 1.06 (0.78–2.3) | 0.54 | ||
| Etiology (reference nonviral) | 2.34 (1.26–4.31) | <0.001 | 2.76 (1.32–5.21) | 0.002 |
| Child-Pugh (reference A) | 2.39 (1.88–4.11) | <0.001 | 2.64 (1.61–4.44) | <0.001 |
| AFP (reference ≤ 400 UI/mL) | 2.08 (1.09–3.1) | 0.01 | 1.71 (1.15–3.2) | 0.01 |
| BCLC (reference B) | 2.2 (1.28–4.3) | 0.001 | 2.15 (1.35–3.88) | 0.02 |
| Hepatitis virus (reference HBV) * | 1.11 (0.8–2.3) | 0.32 | ||
| ECOG PS (reference 0) | 1.75 (1.07–2.8) | 0.02 | 1.23 (0.65–4.81) | 0.14 |
| Effects | Hazard Ratio (95% CI) |
|---|---|
| Current tobacco consumption as the only mediator: • Pure direct effect • Total indirect effect • Total effect | 1.86 (1.16–2.45) 1.02 (0.78–1.34) 2.62 (1.15–3.45) |
| Current alcohol consumption as the only mediator: • Pure direct effect • Total indirect effect • Total effect | 1.67 (1.13–2.5) 1.05 (0.82–2.13) 2.61 (1.15–3.45) |
| Current injection drug abuse as the only mediator: • Pure direct effect • Total indirect effect • Total effect | 1.59 (1.14–2.34) 1.13 (0.88–2.43) 2.60 (1.15–3.34) |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Age (reference ≤ 65 years) | 0.89 (0.64–1.75) | 0.31 | ||
| Gender (reference Female) | 1.16 (0.65–2.1) | 0.58 | ||
| Etiology (reference nonviral) | 2.49 (1.51–4.56) | <0.001 | 2.54 (1.54–4.89) | 0.004 |
| Child-Pugh (reference A) | 1.54 (1.08–2.11) | 0.04 | 1.61 (0.89–3.42) | 0.11 |
| AFP (reference ≤ 400 UI/mL) | 2.18 (1.21–4.23) | 0.003 | 1.72 (1.05–2.6) | 0.05 |
| BCLC (reference B) | 1.8 (0.88–2.3) | 0.09 | ||
| Hepatitis virus (reference HBV) * | 1.01 (0.6–1.8) | 0.76 | ||
| ECOG PS (reference 0) | 1.45 (0.87–2.9) | 0.42 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacco, R.; Ramai, D.; Tortora, R.; di Costanzo, G.G.; Burlone, M.E.; Pirisi, M.; Federico, P.; Daniele, B.; Silletta, M.; Gallo, P.; et al. Role of Etiology in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Counterfactual Event-Based Mediation Analysis. Cancers 2023, 15, 381. https://doi.org/10.3390/cancers15020381
Sacco R, Ramai D, Tortora R, di Costanzo GG, Burlone ME, Pirisi M, Federico P, Daniele B, Silletta M, Gallo P, et al. Role of Etiology in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Counterfactual Event-Based Mediation Analysis. Cancers. 2023; 15(2):381. https://doi.org/10.3390/cancers15020381
Chicago/Turabian StyleSacco, Rodolfo, Daryl Ramai, Raffaella Tortora, Giovan Giuseppe di Costanzo, Michela Emma Burlone, Mario Pirisi, Piera Federico, Bruno Daniele, Marianna Silletta, Paolo Gallo, and et al. 2023. "Role of Etiology in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Counterfactual Event-Based Mediation Analysis" Cancers 15, no. 2: 381. https://doi.org/10.3390/cancers15020381
APA StyleSacco, R., Ramai, D., Tortora, R., di Costanzo, G. G., Burlone, M. E., Pirisi, M., Federico, P., Daniele, B., Silletta, M., Gallo, P., Cocuzza, C., Russello, M., Cabibbo, G., Rancatore, G., Cesario, S., Masi, G., Marzi, L., Mega, A., Granito, A., ... Facciorusso, A., on behalf of A.I.G.O. (Italian Association of Hospital Gastroenterologists). (2023). Role of Etiology in Hepatocellular Carcinoma Patients Treated with Lenvatinib: A Counterfactual Event-Based Mediation Analysis. Cancers, 15(2), 381. https://doi.org/10.3390/cancers15020381