
Marginal Adaptation and Micropermeability of Class II Cavities Restored with Three Different Types of Resin Composites—A Comparative Ten-Month In Vitro Study

Abstract
:1. Introduction
- By reducing the reactive groups per unit volume of the polymer matrix.This goal can be achieved by:
- (a)
- Increasing the relative share of filler particles in the inorganic phase.
- (b)
- Increasing the molecular weight of the reactive groups in the organic matrix.
- By using a different type of organic matrix.
- Light-cured composites have a limited polymerization depth—2 mm.The polymerization of dental composites is a complex process, depending on their composition and heterogeneous structure. Manufacturers of dental resins give recommendations about the depth of cure as they relate to light activation. The most typical indication is the use of specific light intensity and exposure time, which can cure 2 mm of material. Depth of cure of 2 mm provides maximum conversion rate, hardness, and the composite material’s stability [25,26].
- Clinicians try to control the polymerization shrinkage stress of the material by incremental application of the composite. The concept of layer-by-layer application of composites is based on applying a small volume of material with minimal contact with the opposite walls of the cavity (C-factor) during polymerization. It has been found that the small volume of the composite causes less shrinkage [27]. Theoretically, each layer is compensated by the next, and the overall volumetric shrinkage is less destructive because the free surfaces allow stress release by providing flow [9,27].
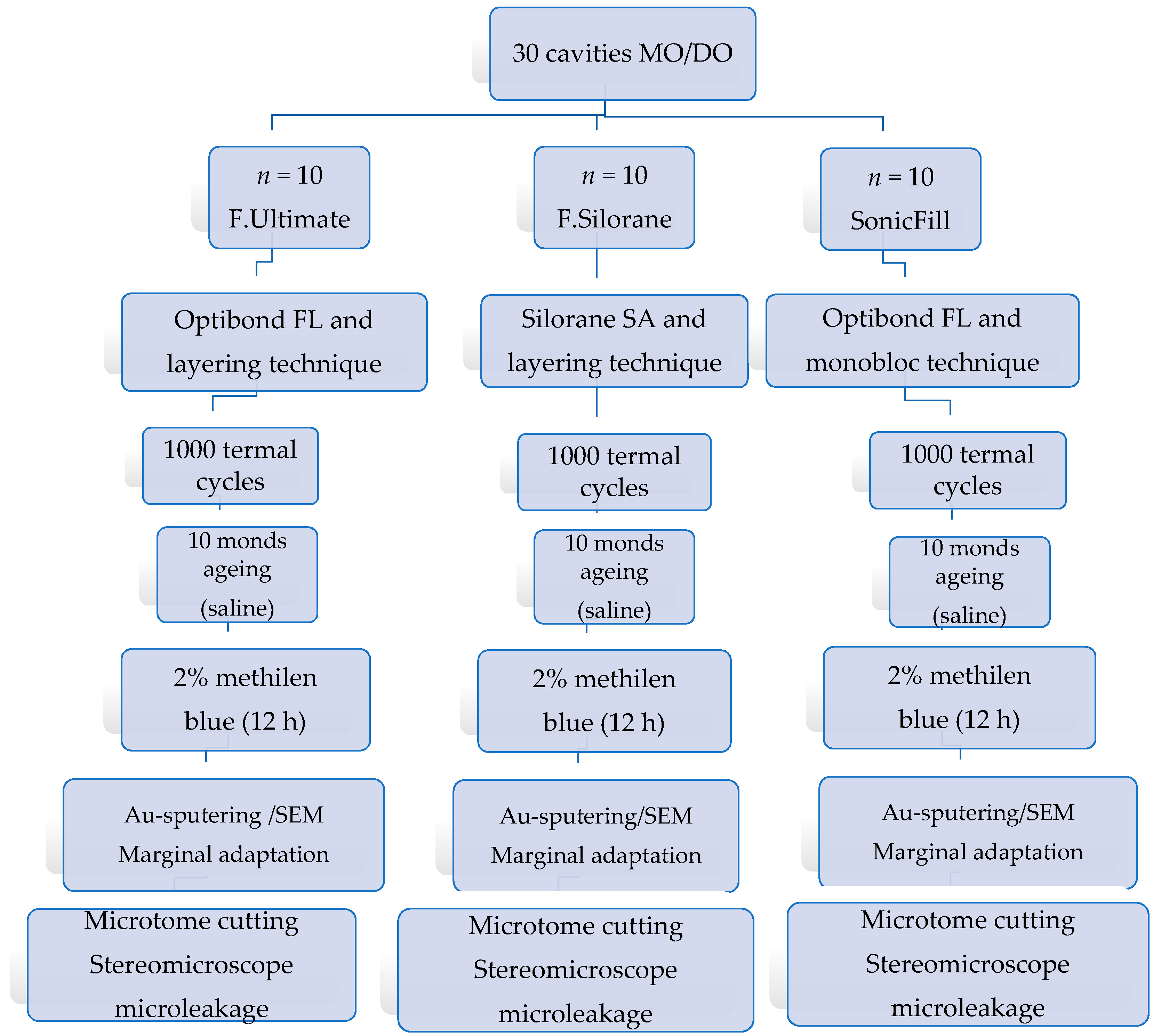
2. Materials and Methods
2.1. Specimen Preparation
2.2. Termocucling, Ageing, and Preparation for Microscopic Investigation
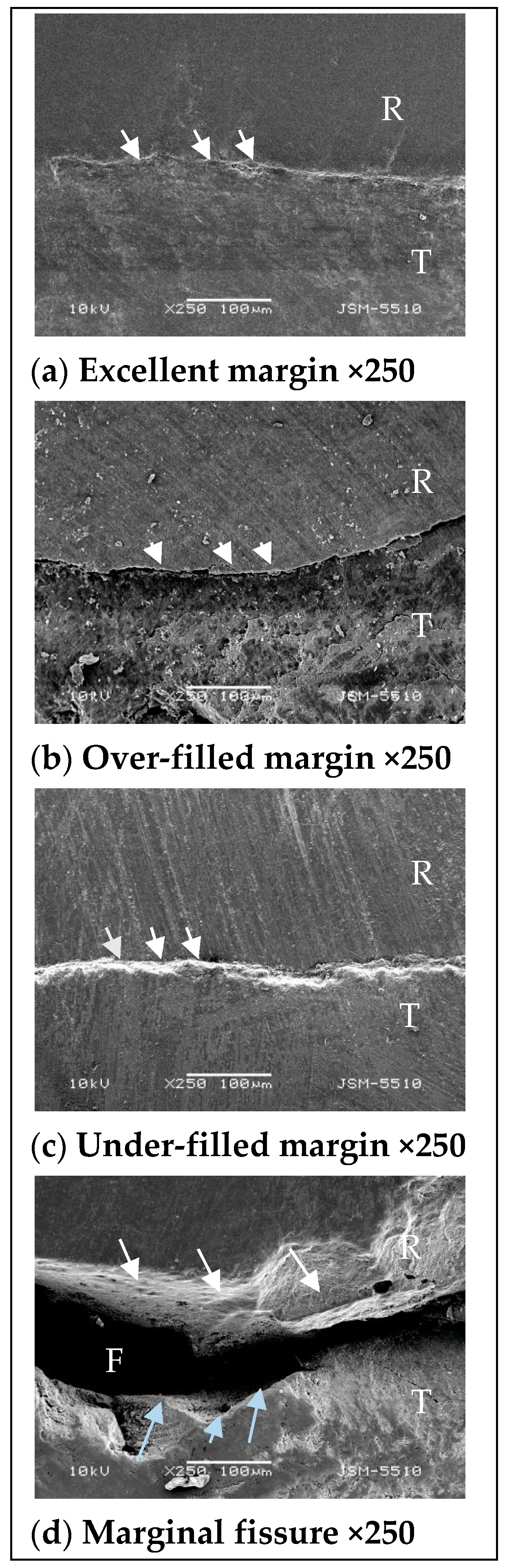
2.2.1. SEM Investigation—Marginal Integrity
- Excellent margin;
- Over-filled margin;
- Under-filled margin;
- Marginal fissure.
2.2.2. Stereomicroscopic Investigation—Micropermeability
- 0.
- No due penetration;
- 1.
- Due penetration up to 1/3 of the gingival wall;
- 2.
- Due penetration up to 1/2 of the gingival wall;
- 3.
- Due penetration over 1/2 of the gingival wall, but the axial wall is not affected;
- 4.
- Due penetration reaches and covers the axial wall of the cavity.
2.3. Statistical Analysis
3. Results
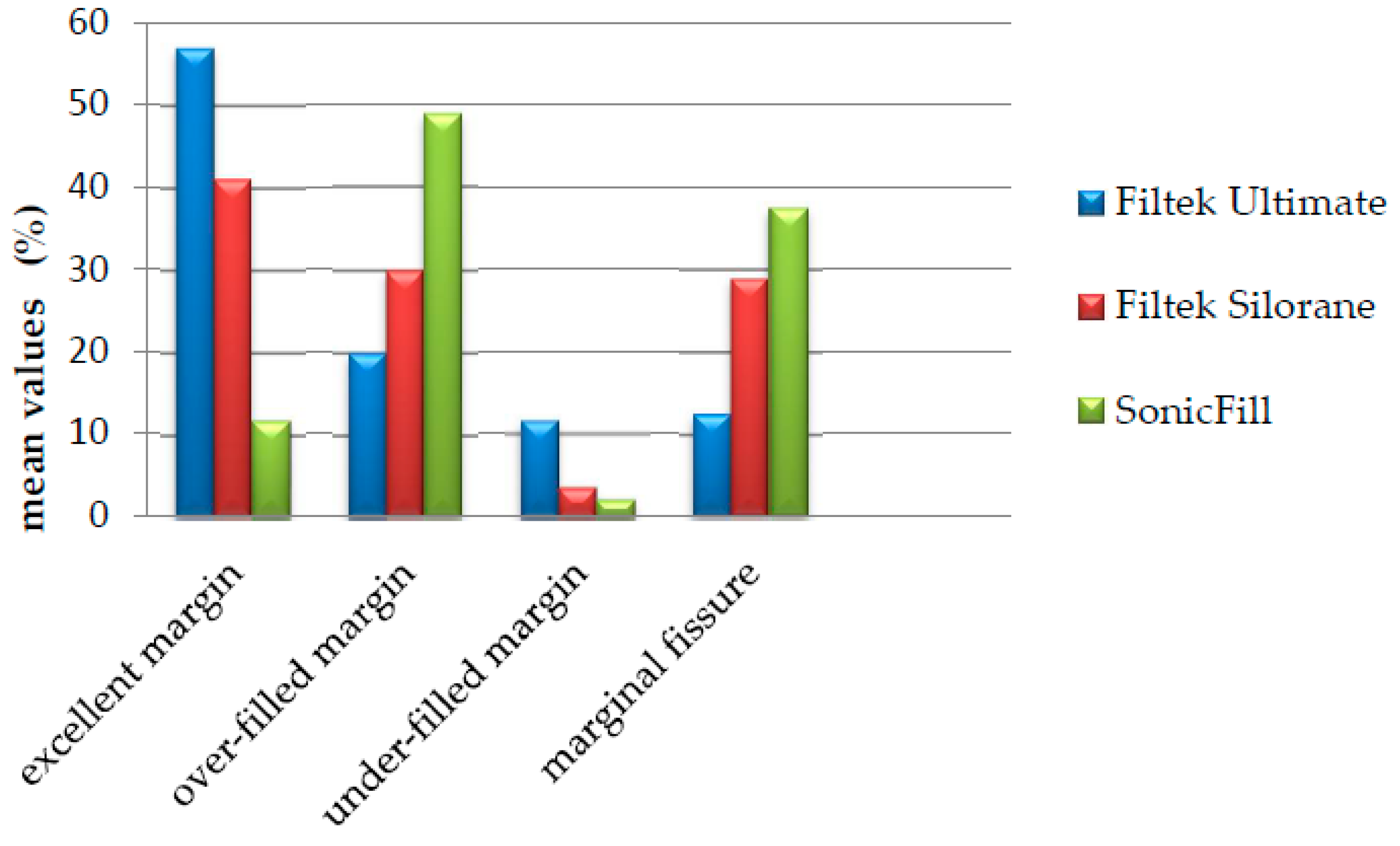
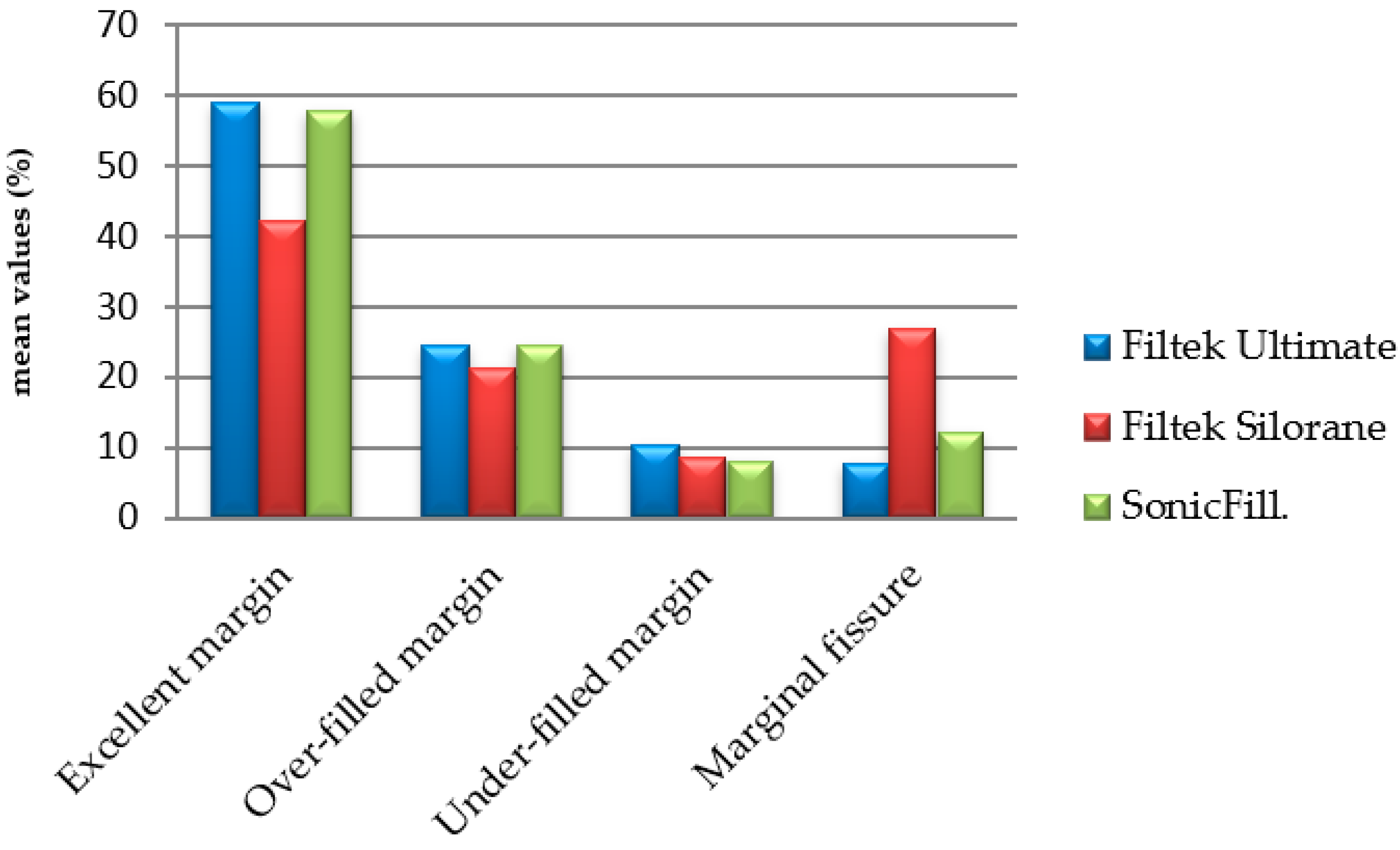
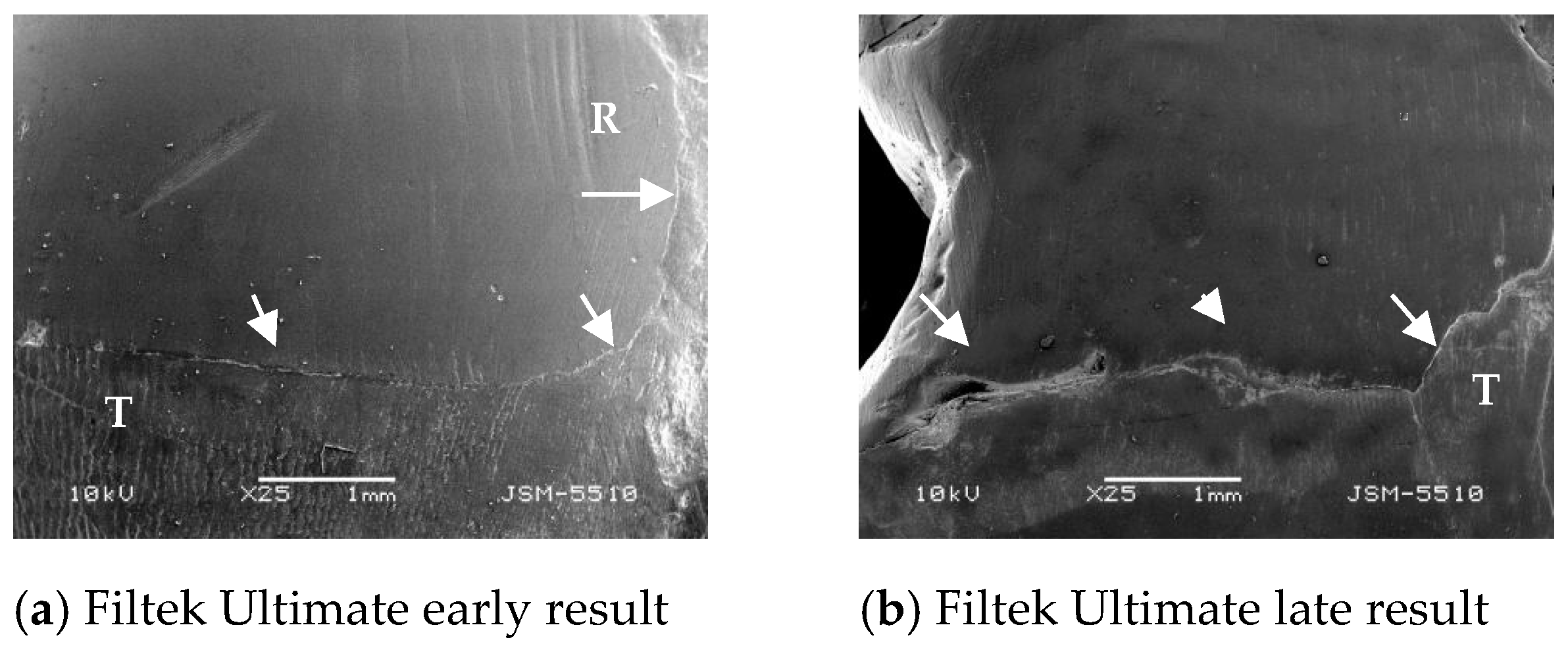
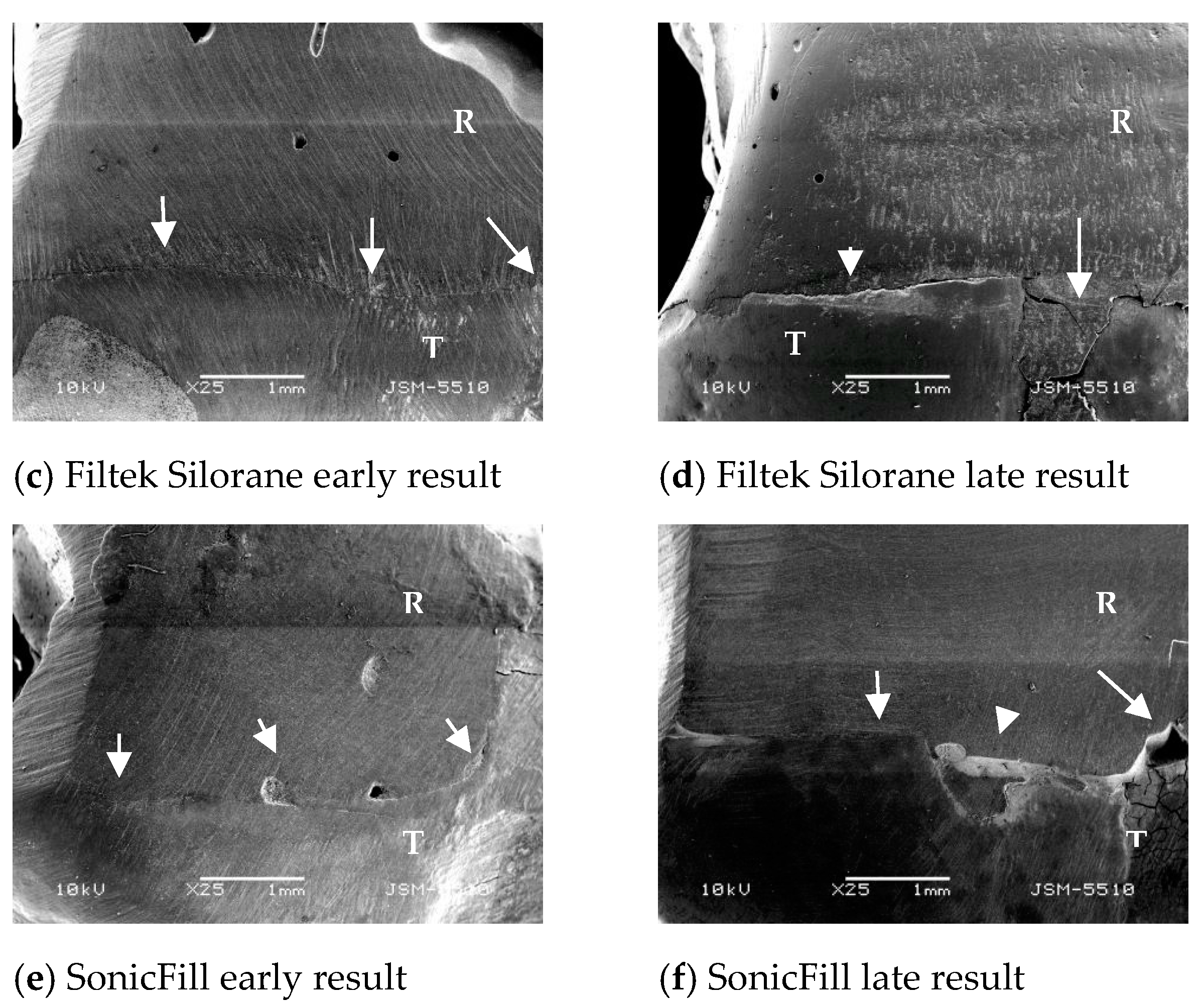
3.1. Marginal Integrity—Results
3.2. Micropermeability—Results
3.3. Correlation between Marginal Integrity and Microleakage
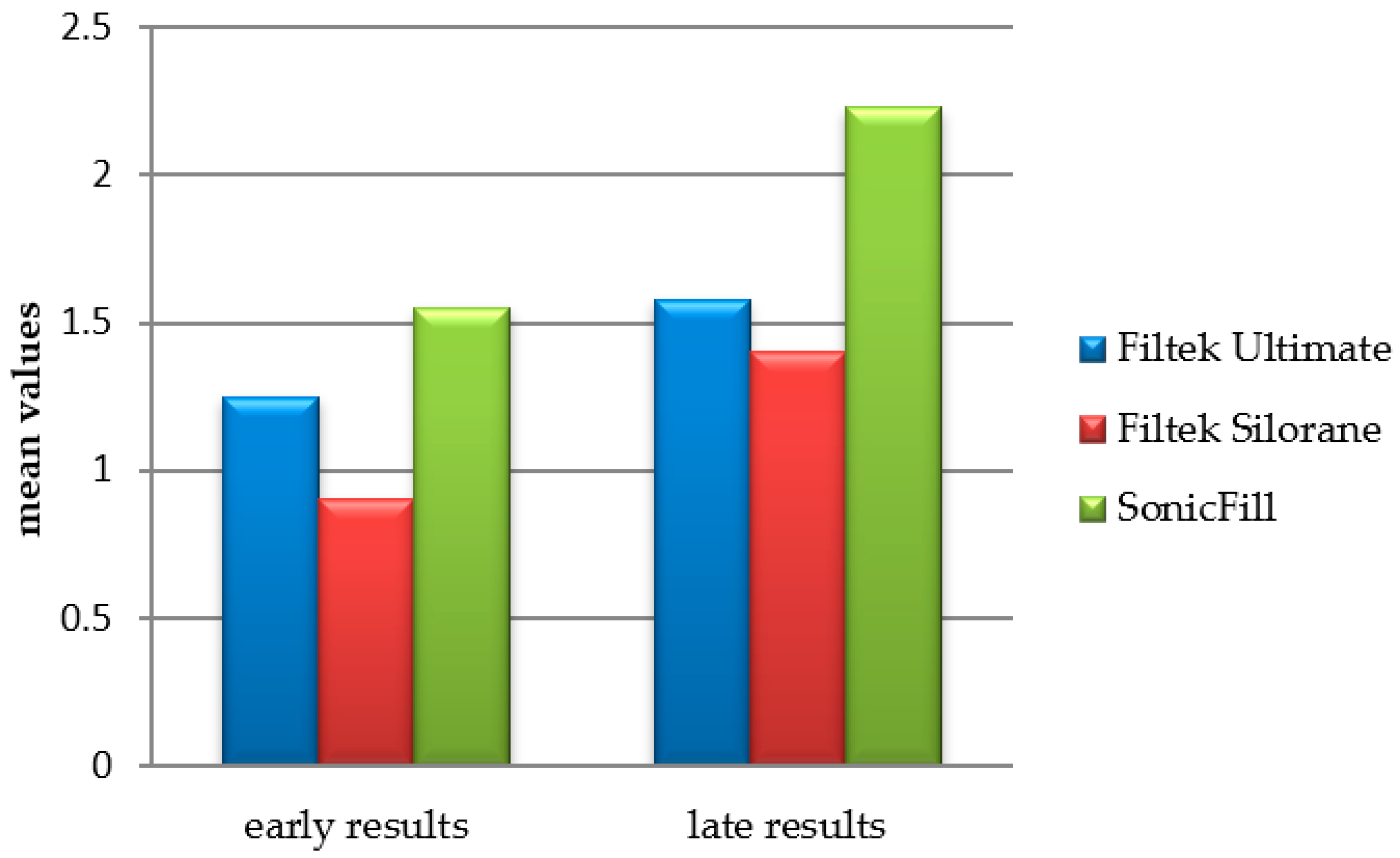
3.4. Comparison between Early and Late Results (Ageing and Material Influence)
4. Discussion
5. Conclusions
- F.Ultimate and F.Silorane differ statistically with more excellent results than SonicFill, for marginal adaptation to the gingival margin, located entirely in the dentin in class II cavities, after ten months of ageing in saline.
- F.Ultimate and F.Silorane differ statistically with less microleakage than SonicFill in class II cavities with gingival margin located entirely in the dentin.
- There is a strong correlation between excellent results for marginal adaptation to the marginal gingival ridge and micropermeability at the direction to the axial wall in class II cavities, with a gingival wall 1 mm below CEJ.
- Ageing affects most significantly the proximal gingival margin, complemented by an increase in microleakage to the axial wall of the cavity.
- Present data shows that the development of resin composite compositions by changing the inorganic phase through nanotechnology and changing the matrix of materials with silorane leads to comparable results over time.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Opdam, N.J.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.; van Dijken, J.W. Longevity of posterior composite restorations: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Pallesen, U.; van Dijken, J.W.; Halken, J.; Hallonsten, A.L.; Höigaard, R. Longevity of posterior resin composite restorations in permanent teeth in Public Dental Health Service: A prospective 8 years follow up. J. Dent. 2013, 41, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.S.; Amin, F.; Fareed, M.A.; Ghabbani, H.; Riaz, S.; Khurshid, Z.; Kumar, N. Biomimetic Aspects of Restorative Dentistry Biomaterials. Biomimetics 2020, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, R.L.; Ferracane, J.L.; Powers, J.M. Craig’s Restorative Dental Materials, 14th ed.; Elsevier Mosby: Philadelphia, PA, USA, 2018; pp. XVI–352. [Google Scholar]
- Dogon, IL Present and future value of dental composite materials and sealants. J. Technol. Assess. Health Care 1990, 6, 369–377. [CrossRef]
- Ferracane, J.L. Resin-based composite performance: Are there some things we can predict? Dent. Mater. 2013, 29, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulsamee, N.; Elkhadem, A.; Nagi, P. Shrinkage of Dental Composite Resin: Contemporary Understanding its Enigmas and How to Solve? A Review. EC Dent. Sci. 2020, 19, 3–17. [Google Scholar]
- Miletic, V. Dental Composite Materials for Direct Restorations; Springer: New York, NY, USA, 2017; pp. VIII–319. [Google Scholar]
- Braga, R.R.; Ballester, Y.R.; Ferracane, J.L. Factors involved in the development of polymerization shrinkage stress in the resin-composites: A systematic review. Dent. Mater. 2005, 21, 962–970. [Google Scholar] [CrossRef]
- Braga, R.; Yamamoto, T.; Tyler, K.; Boaro, L.; Ferracane, J.L.; Swain, M.V. A comparative study between crack analysis and a mechanical test for assessing the polymerization stress of restorative composites. Dent. Mater 2012, 28, 632–641. [Google Scholar] [CrossRef]
- Kahler, B.; Kotousov, A.; Borkowski, K. Effect of material properties on stresses at the restoration-dentin interface of composite restorations during polymerization. Dent. Mater. 2006, 22, 942–947. [Google Scholar] [CrossRef]
- Malarvizhi, D.; Karthick, A.; Gold Pearlin Mary, N.; Venkatesh, A. Shrinkage in composites: An enigma. J. Int. Oral Health 2019, 11, 244–248. [Google Scholar] [CrossRef]
- Kemp-Scholte, C.M.; Davidson, C.L. Marginal integrity, related to bond strength and strain capacity of composite resin restorative systems. J. Prosthet. Dent. 2009, 64, 658–663. [Google Scholar] [CrossRef]
- Weinmann, W.; Thalacker, C.; Guggenberg, R. Siloranes in dental composites. Dent. Mater. 2005, 21, 68–74. [Google Scholar] [CrossRef]
- Szczesio-Wlodarczyk, A.; Sokolowsky, J.; Kleczewska, J.; Bociong, K. Ageing of dental composites based on methacrylate resins-A critical review of the causes and method of assessment. Polymers 2020, 12, 882. [Google Scholar] [CrossRef]
- Vouvoudi, E.C.; Sideridou, I.D. Dental light-cured polymer nanocomposites: A brief review of experimental results obtained from the study of some physicochemical properties. J. Compos. Biodegrad. Polym. 2014, 2, 46–56. [Google Scholar]
- Alzraikat, H.; Burrow, M.F.; Maghaireh, G.A.; Taha, N.A. Nanofilled Resin Composite Properties and Clinical Performance: A Review. Oper. Dent. 2018, 43, E173–E190. [Google Scholar] [CrossRef]
- Melander, J.; Dunn, W.P.; Link, M.P.; Wang, Y.; Xu, C.; Walker, M.P. Comparison of flexural properties and surface roughness of nanohybrid and microhybrid dental composites. Gen. Dent. 2011, 59, 342–347. [Google Scholar]
- Ilie, N.; Hickel, R. Investigations on mechanical behaviour of dental composites. Clin. Oral Investig. 2009, 13, 427–438. [Google Scholar] [CrossRef]
- Sideridou, I.D.; Karabela, M.M.; Vouvoudi, E. Physical properties of current dental nanohybrid and nanofill light-cured resin composites. Dent. Mater. 2011, 27, 598–607. [Google Scholar] [CrossRef]
- Boaro, L.; Goncalves, F.; Guimaraes, T.; Ferracane, J.; Versluis, A.; Braga, R. Polymerization stress, shrinkage and elastic modulus of current low-shrinkage restorative composites. Dent. Mater. 2010, 26, 1144–1150. [Google Scholar] [CrossRef]
- Ilie, N.; Hickel, R. Macro-, micro-and nano-mechanical investigations on silorane and methacrylate-based composites. Dent. Mater. 2009, 25, 810–819. [Google Scholar] [CrossRef]
- Ilie, N.; Hickel, R. Resin composite restorative materials. Aust. Dent. J. 2011, 56, 59–66. [Google Scholar] [CrossRef]
- Bagis, Y.H.; Baltacioglu, I.H.; Kahyaoglullati, S. Comparing microleakage and the layering methods of Silorane-based resin composite in wide class 2 MOD. cavities. Oper. Dent. 2009, 34, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.; Senevirante, C. Influence of light energy density on effectiveness of composite cure. Oper. Dent. 2001, 26, 460–466. [Google Scholar]
- Lombardini, M.; Chiesa, M.; Scribante, A.; Colombo, M.; Poggio, C. Influence of polymerization time and depth of cure of resin composites determined by Vickers hardness. Dent. Res. J. 2012, 6, 735–740. [Google Scholar]
- Braga, R.R.; Ferracane, J.L. Contraction stress related to degree of conversion and reaction kinetics. J. Dent. Res. 2002, 81, 114–118. [Google Scholar] [CrossRef]
- Veloso, S.R.M.; Lemos, C.A.A.; de Moraes, S.L.D.; do Egito Vasconcelos, B.C.; Pellizzer, E.P.; de Melo Monteiro, G.Q. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: A systematic review and meta-analysis. Clin. Oral Investig. 2019, 23, 221–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corral, C.; Vildysola, P.; Bersezio, C.; Alves Dos Campos, E.; Fernбndez, E. State of the art of bulk-fill resin-based composites: A review. Rev. Fac Odontol. Univ. Antioq. 2015, 27, 177–196. [Google Scholar]
- Campos, E.A.; Ardu, S.; Lefever, D.; Jassé, F.F.; Bortolotto, T.; Krejc, I. Marginal adaptation on class II cavities restored with bulk-fill composites. J. Dent. 2014, 42, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Alrahlah, A.; Silikas, N.; Watts, D.C. Post-cure depth of cure of bulk fill dental resin-composites. Dent. Mater. 2014, 30, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Goracci, C.; Cadenaro, M.; Fontanive, L.; Giangrosso, G.; Juloski, J.; Vichi, A.; Ferrari, M. Polymerization efficiency and flexural strength of low-stress restorative composites. Dent. Mater. 2014, 30, 688–694. [Google Scholar] [CrossRef]
- Lui, J.L.; Masutani, S.; Setcos, J.C.; Lutz, F.; Swartz, M.L.; Phillips, R.W. Margin quality and microleakage of Class II composite resin restorations. J. Am. Dent. Assoc. 1987, 114, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Ernst, C.-P.; Galler, P.; Willershausen, B.; Haller, B. Marginal integrity of class 5 restorations: SEM versus dye penetration. Dent. Mater. 2008, 24, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Yantcheva, S.; Vasileva, R. In vitro investigation of marginal adaptation and microleakage of class ΙΙ conventional and matrix-modified composite resin restorations. Dent. Med. 2013, 95, 19–28. [Google Scholar]
- Moosavi, H.; Yazdi, F.M.; Moghadam, F.V.; Soltani, S. Comparison of composite restorations microleakage: An in vitro study. Open J. Stomatol. 2013, 3, 209–214. [Google Scholar] [CrossRef] [Green Version]
- Sampaio, C.S.; Rodrigues, R.V.; Souza-Junior, E.J.; Freitas, A.Z.; Ambrosano, G.M.B.; Pascon, F.M.; Puppin-Rontani, R.M. Effect of restorative system and thermal cycling on the tooth-restoration interface-OCT evaluation. Oper. Dent. 2016, 41, 162–170. [Google Scholar] [CrossRef]
- Santerre, J.P.; Shajii, L.; Leung, B.W. Relation of dental composite formulations to their degradation and release of hydrolyzed polymer-resin-derived products. Crit. Rev. Oral Biol. Med. 2001, 12, 136–151. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, P.J.; Silva, M.S.; Alonso, R.C.B.; Alpino, D. PHP Hydrolytic degradation of silorane- and methacrylate-based composite restorations: Evaluation of push-out strength and marginal adaptation. Acta Odontol. Scand. 2013, 71, 1273–1279. [Google Scholar] [CrossRef]
- Drummond, J.L. Degradation, fatigue and failure of resin dental composite materials. J. Dent. Res. 2008, 87, 710–719. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Godoy, F.; Krämer, N.; Feilzer, A.J.; Frankenberger, R. Long-term degradation of enamel and dentin bonds: 6-year results in vitro vs. in vivo. Dent. Mater. 2010, 26, 1113–1118. [Google Scholar] [CrossRef]
- Mjor, I.A.; Dahl, J.E.; Moorhead, J.E. Age of restorations at a replacement in permanent teeth in general dental practice. Acta Odontol. Scand. 2000, 58, 97–101. [Google Scholar] [CrossRef]
- Spencer, P.; Ye, Q.; Park, J.; Topp, E.M.; Misra, A.; Marangos, O.; Wang, Y.; Bohaty, B.S.; Singh, V.; Sene, F.; et al. Adhesive/Dentin Interface: The Weak Link in the Composite Restoration. Ann. Biomed. Eng. 2010, 38, 1989–2003. [Google Scholar] [CrossRef] [Green Version]
- Heintze, S.D.; Fofjani, C.M.; Cavalleri, A. Microleakage of class 2 restorations with different tracers-comparison with SEM quantitative analysis. J. Est Dent. 2008, 10, 259–267. [Google Scholar]
- Ishikiriama, S.K.; Mondelli, R.F.; Kano, S.C.; Ishikiriama, A.; Mondelli, J. Role of additional retention on marginal adaptation and sealing of large resin composite Class II restorations. Oper. Dent. 2007, 32, 564–570. [Google Scholar] [CrossRef]
- Kidd, E.A.; Beighton, D. Prediction of secondary caries around tooth-coloured restorations: A clinical and microbiological study. J. Dent. Res. 1996, 75, 1942–1946. [Google Scholar] [CrossRef] [PubMed]
- Shibasaki, S.; Takamizawa, T.; Nojiri, K.; Imai, A.; Tsujimoto, A.; Endo, H.; Suzuki, S.; Suda, S.; Barkmeier, W.W.; Latta, M.A.; et al. Polymerization Behavior and Mechanical Properties of High-Viscosity Bulk Fill and Low Shrinkage Resin Composites. Oper. Dent. 2017, 42, E177–E187. [Google Scholar] [CrossRef]
- Satterthwaite, J.D.; Vogel, K.; Watts, D.C. Effect of resin-composite filler particle size and shape on shrinkage-strain. Dent. Mater. 2009, 25, 1612–1615. [Google Scholar] [CrossRef]
- Dos Santos, G.O.; dos Santos, M.E.; Sampaio, E.M.; Dias, K.R.; da Silva, E.M. Influence of C-factor and light-curing mode on gap formation in resin composite restorations. Oper. Dent. 2009, 34, 544–550. [Google Scholar] [CrossRef]
- Yantcheva, S.; Vasileva, R. Sorption and solubility of low-shrinkage resin-based dental composites. J. IMAB 2016, 22, 1114–1119. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, E.M.; Almeida, G.S.; Poskus, L.T.; Guimaraes, J.G. Relationship between the degree of conversion, solubility and salivary sorption of a hybrid and a nanofilled resin composite. J. Appl. Oral Sci. 2008, 16, 161–166. [Google Scholar] [CrossRef] [Green Version]
- De Moraes, R.R.; Goncalves, S.; Lancellotti, A.C.; Consani, S.; Correr-Sobrinho, L.; Sinhoreti, M.A. Nanohybrid resin composites: Nanofiller loaded materials or traditional microhybrid resins? Oper. Dent. 2009, 34, 551–557. [Google Scholar] [CrossRef]
- Arhun, N.; Tuncer, D.; Chelik, C.; Ehreli, S.B. Microleakage of a multi-mode adhesive system in class II restorations. J. Adhes. Sci. Technol. 2014, 28, 1279–1288. [Google Scholar]
- Van Meerbeek, B.; De Munck, J.; Yoshida, Y.; Inoue, S.; Vargas, M.; Vijay, P.; Van Landuyt, K.; Lambrechts, P.; Vanherle, G. Adhesion to enamel and dentin: Current status and future challenges. Buonocore Memorial Lecture. Oper. Dent. 2003, 28, 215–235. [Google Scholar] [PubMed]
- Marchesi, G.; Breschi, L.; Antoniolli, F.; Di Lenarda, R.; Ferracane, J.; Cadenaro, M. Contraction stress of low-shrinkage composite materials assessed with different testing systems. Dent. Mater. 2010, 26, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Naoum, S.J.; Ellakwa, A.; Morgan, L.; White, K.; Martin, F.E.; Lee, I.B. Polymerization profile analysis of resin composite dental restorative materials in real-time. J. Dent. 2012, 40, 64–70. [Google Scholar] [CrossRef]
- Schneider, L.F.J.; Cavalcante, L.M.; Silikas, N.; Watts, D.C. Degradation resistance of silorane, experimental ormocer and dimethacrylate resin-based dental composites. J. Oral Sci. 2011, 53, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Mine, A.; De Munck, J.; Van Ende, A.; Cardoso, M.V.; Kuboki, T.; Yoshida, Y.; Van Meerbeek, B. TEM characterization of a silorane composite bonded to enamel/dentin. Dent. Mater. 2010, 26, 524–532. [Google Scholar] [CrossRef]
- Van Ende, A.; De Munck, J.; Mine, A.; Lambrechts, P.; Van Meerbeek, B. Does a low-shrinking composite induce less stress at the adhesive interface? Dent. Mater. 2010, 26, 215–222. [Google Scholar] [CrossRef]
- Navarra, C.O.; Cadenaro, M.; Armstrong, S.R.; Jessop, J.; Antoniolli, F.; Sergo, V.; Di Lenarda, R.; Breschi, L. Degree of conversion of Filtek Silorane Adhesive System and Clearfil SE Bond within the hybrid and adhesive layer: An in situ Raman analysis. Dent. Mater. 2009, 25, 1178–1185. [Google Scholar] [CrossRef]
- Duarte, S.; Botta, A.C.; Phark, J.-H.; Sadan, A. Selected mechanical and physical properties and clinical application of a new low-shrinkage composite restoration. Quintessence Int. 2009, 40, 631–638. [Google Scholar]
- Khosravi, K.; Ataei, E.; Mousavi, M.; Khodaeian, N. Effect of phosphoric acid etching of enamel margins on the microleakage of a simplified all-in-one and self-etch adhesive system. Oper. Dent. 2009, 34, 531–536. [Google Scholar] [CrossRef]
- Luu, C.; Drechsler, U. Viscosity Change of SonicFill™ When Subjected to Sonic Vibration; Kerr Dental Materials Center: Orange, CA, USA, 2011; Volume 4–5, p. 2. [Google Scholar]
- Rueggeberg, F. Georgia Health Sciences University, Augusta, GA. Monomer Conversion of various thicknesses of SonicFill™ and competitive products. Kerr Corp. Sonicfill. Portf. Sci. Res. 2011, 3, 34. [Google Scholar]
- Soygun, K.; Unal, M.; Ozer, A.; Gulnahar, E.; Bolayr, G. Effects of different curing units on Bulk Fill composites. Int. J. Oral Dent. Health 2015, 1, 13. [Google Scholar] [CrossRef] [Green Version]
- Tiba, A.; Zeller, G.; Estrich, C.; Hong, A. A laboratory evaluation of bulk-fill versus traditional multi-increment-fill resin-based composites. J. Am. Dent. Assoc. 2013, 8, 13–26. [Google Scholar] [CrossRef] [Green Version]
- Orlowski, M.; Tarczydlo, B.; Chalas, R. Evaluation of marginal integrity of four bulk-fill dental composite materials: In vitro study. Hindawi Publ. Corp. Sci. World J. 2015, 2015, 701262. [Google Scholar]
- Sun, J.; Eidelman, N.; Lin-Gibson, S. 3D mapping of polymerization shrinkage using X-ray micro-computed tomography to predict microleakage. Dent. Mater. 2009, 25, 314–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferracane, J.L. Buonocore Lecture. Placing dental composites—A stressful experience. Oper Dent. 2008, 33, 247–257. [Google Scholar] [CrossRef] [Green Version]
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Organic Matrix | Material Type and Filler Loading |
|---|---|---|
| Filtek Ultimate (3M ESPE) A3 shade/body mass | Bis-GMA; TEGDMA; PEGDMA UDMA; Bis-EMA | Nanocomposite Filled 79 wt % |
| Filtek Silorane LS (3M ESPE) A3 shade | Silorane | Microhybrid Filled 76 wt % |
| SonicFill (Kerr) A3 shade | Bis-GMA; TEGDMA; UDMA; Bis-EMA | Nanohybrid, filled 84 wt % Bulk-fill |
| Values (%) | Excellent Margin | Over-Filled Margin | Under-Filled Margin | Marginal Fissure | ||
|---|---|---|---|---|---|---|
| Materials | n | Mean ± sd | Mean ± sd | Mean ± sd | Mean ± sd | |
| 1 | Filtek Ultimate | 10 | 41.61 ± 27.04 | 20.50 ± 32.51 | 2.44 ± 7.72 | 35.37 ± 32.31 |
| 2 | Filtek Silorane | 10 | 41.24 ± 33.45 | 29.99 ± 26.88 | 3.54 ± 11.18 | 28.87 ± 18.88 |
| 3 | SonicFill | 10 | 11.70 ± 17.01 | 48.84 ± 31.50 | 2.08 ± 6.57 | 37.38 ± 26.43 |
| p. sign | 0.005 | 0.137 | 0.465 | 0.487 | ||
| Values (%) | Excellent Margin | Over-Filled Margin | Under-Filled Margin | Marginal Fissure | ||
|---|---|---|---|---|---|---|
| Materials | n | Mean ± sd | Mean ± sd | Mean ± sd | Mean ± sd | |
| 1 | Filtek Ultimate | 10 | 56.65 ± 29.88 | 19.52 ± 9.26 | 11.50 ± 21.81 | 12.43 ± 15.40 |
| 2 | Filtek Silorane | 10 | 41.01 ± 4.34 | 24.45 ± 6.37 | 6.94 ± 15.03 | 27.60 ± 19.52 |
| 3 | SonicFill. | 10 | 51.68 ± 6.27 | 23.01 ± 7.97 | 10.05 ± 12.02 | 21.47 ± 12.27 |
| p. sign | 0.012 | 0.397 | 0.243 | 0.156 | ||
| Values (%) | Excellent Margin | Over-Filled Margin | Under-Filled Margin | Marginal Fissure | ||
|---|---|---|---|---|---|---|
| Materials | n | Mean ± sd | Mean ± sd | Mean ± sd | Mean ± sd | |
| 1 | Filtek Ultimate | 10 | 61.39 ± 19.36 | 29.55 ± 15.82 | 9.26 ± 16.65 | 3.07 ± 4.31 |
| 2 | Filtek Silorane | 10 | 44.37 ± 31.28 | 18.21 ± 18.04 | 10.25 ± 20.81 | 27.16 ± 39.63 |
| 3 | SonicFill. | 10 | 63.97 ± 11.57 | 26.41 ± 12.83 | 6.29 ± 15.42 | 3.33 ± 6.60 |
| p. sign | 0.025 | 0.376 | 0.298 | 0.024 | ||
| Materials | Values | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | Total | ||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||
| 1 | Filtek Ultimate | 7 | 17.5 | 15 | 37.5 | 10 | 25 | 4 | 10 | 4 | 10 | 40 | 100 |
| 2 | Filtek Silorane | 10 | 25 | 12 | 30 | 10 | 25 | 8 | 20 | 0 | 0 | 40 | 100 |
| 3 | SonicFill | 4 | 10 | 10 | 25 | 7 | 17.5 | 11 | 27.5 | 8 | 20 | 40 | 100 |
| p = 0.005 | |||||||||||||
| Values (%) | Excellent Margin (Mean ± sd) | Over-Filled Margin (Mean ± sd) | Under-Filled Margin (Mean ± sd) | Marginal Fissure (Mean ± sd) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Materials | n | Early Results | Late Results | Early Results | Late Results | Early Results | Late Results | Early Results | Late Results | |
| 1 | Filtek Ultimate | 20 | 47.98 ± 25.95 | 41.61 ± 27.04 | 46.42 ± 23.30 | 20.50 ± 32.51 | 2.04 ± 6.55 | 5.41 ± 9.04 | 3.49 ± 6.10 | 35.37 ± 32.31 |
| 2 | Filtek Silorane | 20 | 55.78 ± 30.89 | 41.24 ± 33.45 | 36.51 ± 26.84 | 29.99 ± 26.88 | 1.67 ± 5.29 | 3.24 ± 10.23 | 6.02 ± 10.22 | 28.87 ± 18.88 |
| 3 | SonicFill | 20 | 27.85 ± 8.44 | 11.70 ± 17.01 | 49.90 ± 25.04 | 48.84 ± 31.50 | 5.38 ± 8.47 | 5.89 ± 11.94 | 21.84 ± 17.21 | 37.38 ± 26.43 |
| p sign. | p = 0.084 | p = 0.125 | p = 0.885 | p = 0.001 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yantcheva, S.M. Marginal Adaptation and Micropermeability of Class II Cavities Restored with Three Different Types of Resin Composites—A Comparative Ten-Month In Vitro Study. Polymers 2021, 13, 1660. https://doi.org/10.3390/polym13101660
Yantcheva SM. Marginal Adaptation and Micropermeability of Class II Cavities Restored with Three Different Types of Resin Composites—A Comparative Ten-Month In Vitro Study. Polymers. 2021; 13(10):1660. https://doi.org/10.3390/polym13101660
Chicago/Turabian StyleYantcheva, Sevda Mihailova. 2021. "Marginal Adaptation and Micropermeability of Class II Cavities Restored with Three Different Types of Resin Composites—A Comparative Ten-Month In Vitro Study" Polymers 13, no. 10: 1660. https://doi.org/10.3390/polym13101660
APA StyleYantcheva, S. M. (2021). Marginal Adaptation and Micropermeability of Class II Cavities Restored with Three Different Types of Resin Composites—A Comparative Ten-Month In Vitro Study. Polymers, 13(10), 1660. https://doi.org/10.3390/polym13101660