
ASA Status, NPPA/NPPB Haplotype and Coronary Artery Disease Have an Impact on BNP/NT-proBNP Plasma Levels

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
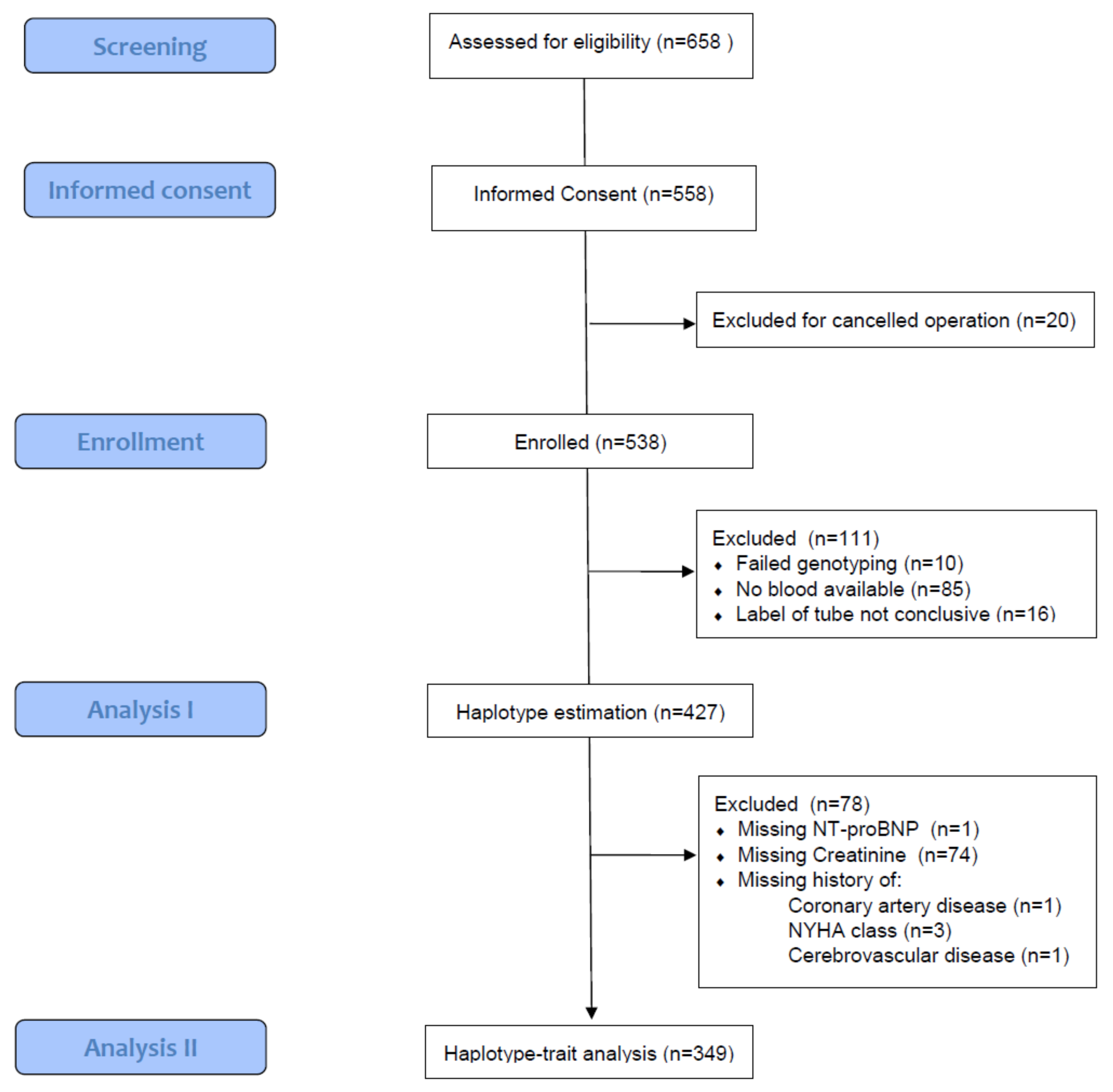
2.1. Study Design and Patients
2.2. BNP and NT-proBNP Assay
2.3. Genetic Analysis
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.1.1. BNP and NT-proBNP Distributions
3.1.2. BNP and NT-proBNP Concentrations by Level of Covariates
3.2. Genetic Effects on Natriuretic Peptides
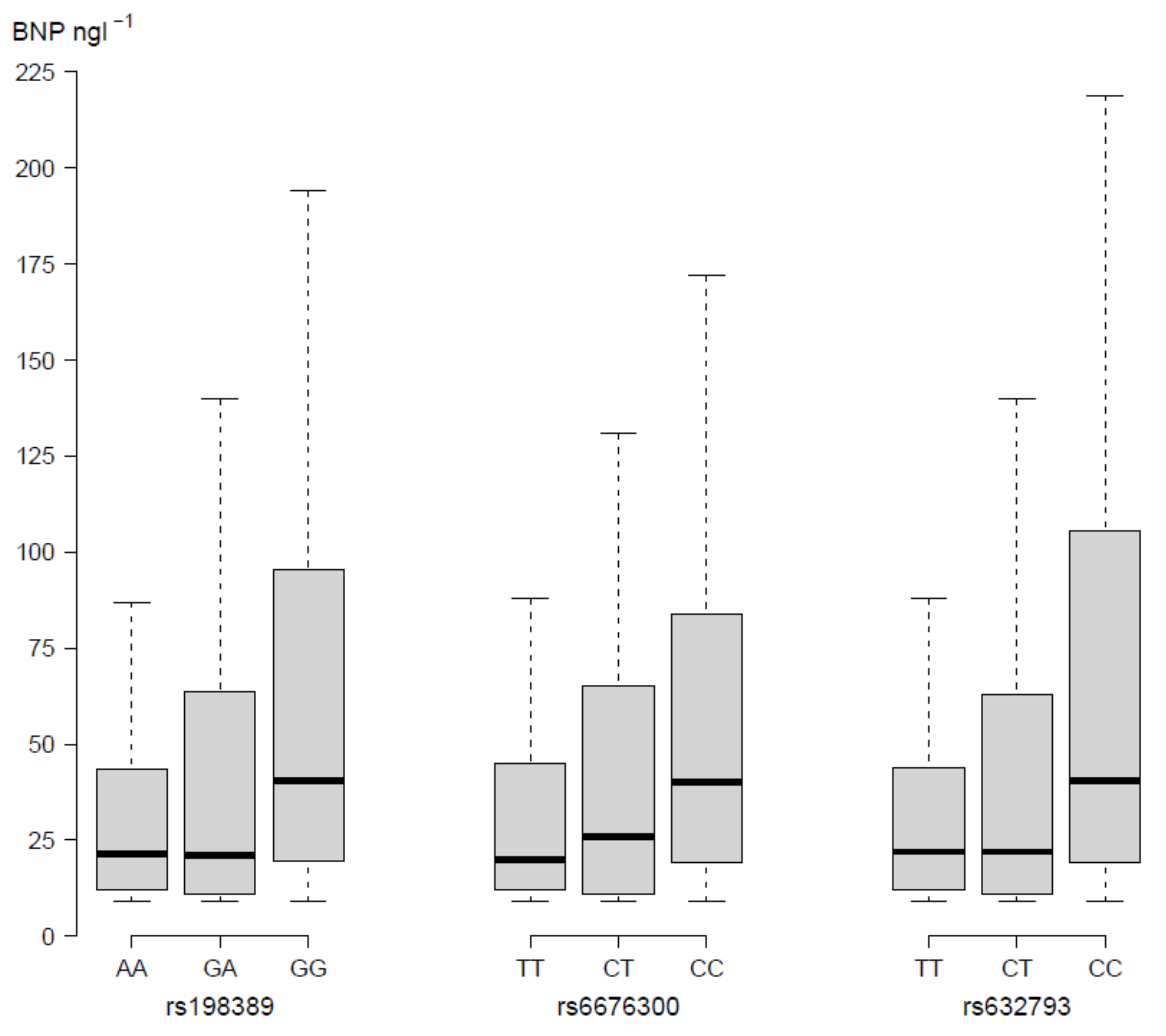
3.2.1. Single-SNP Effects on NP Plasma Levels
3.2.2. Haplotype Organization in the NPPA/NPPB Locus
3.2.3. Common Haplotypes in the NPPA/NPPB Locus Influence NP Plasma Levels
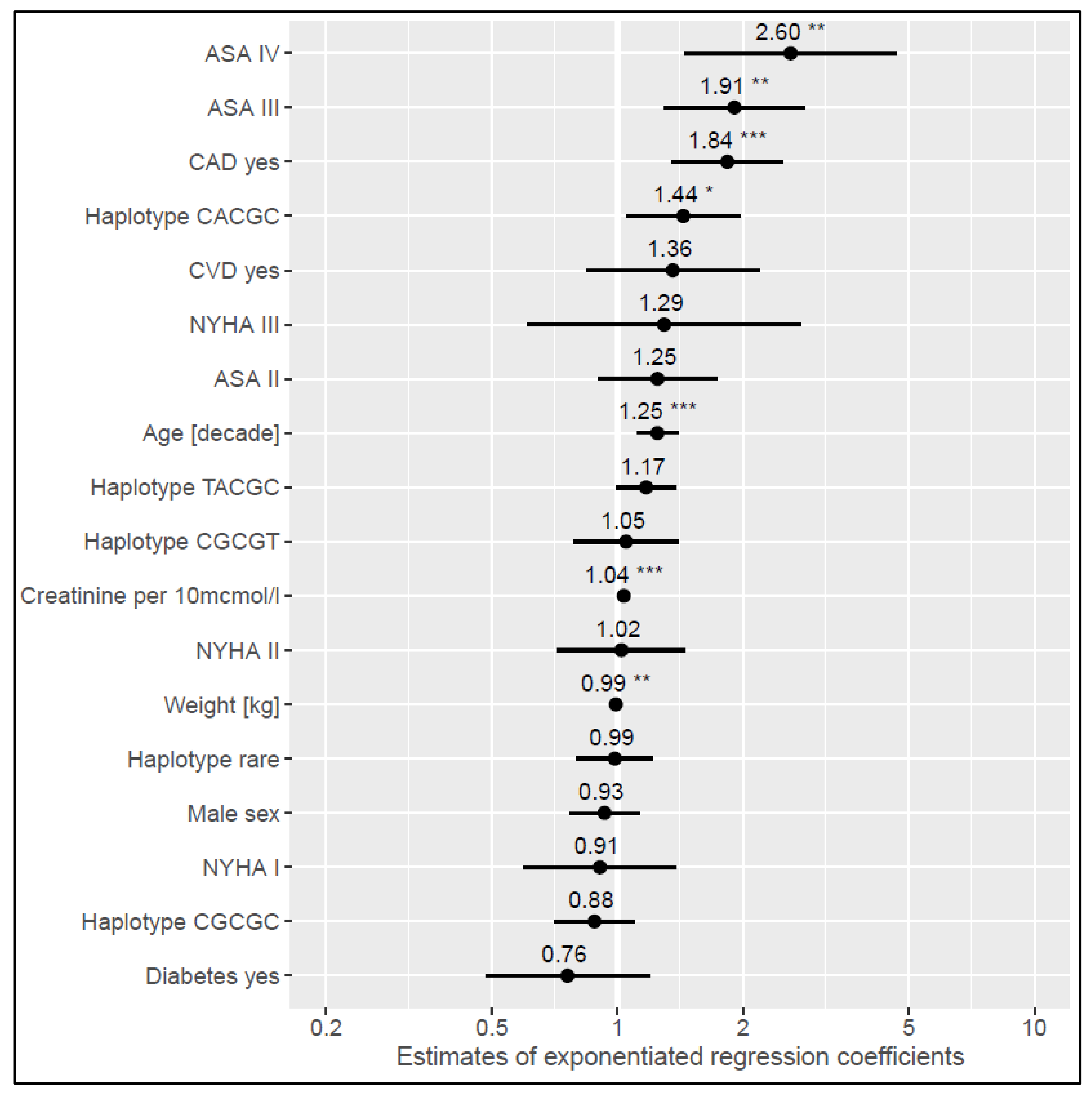
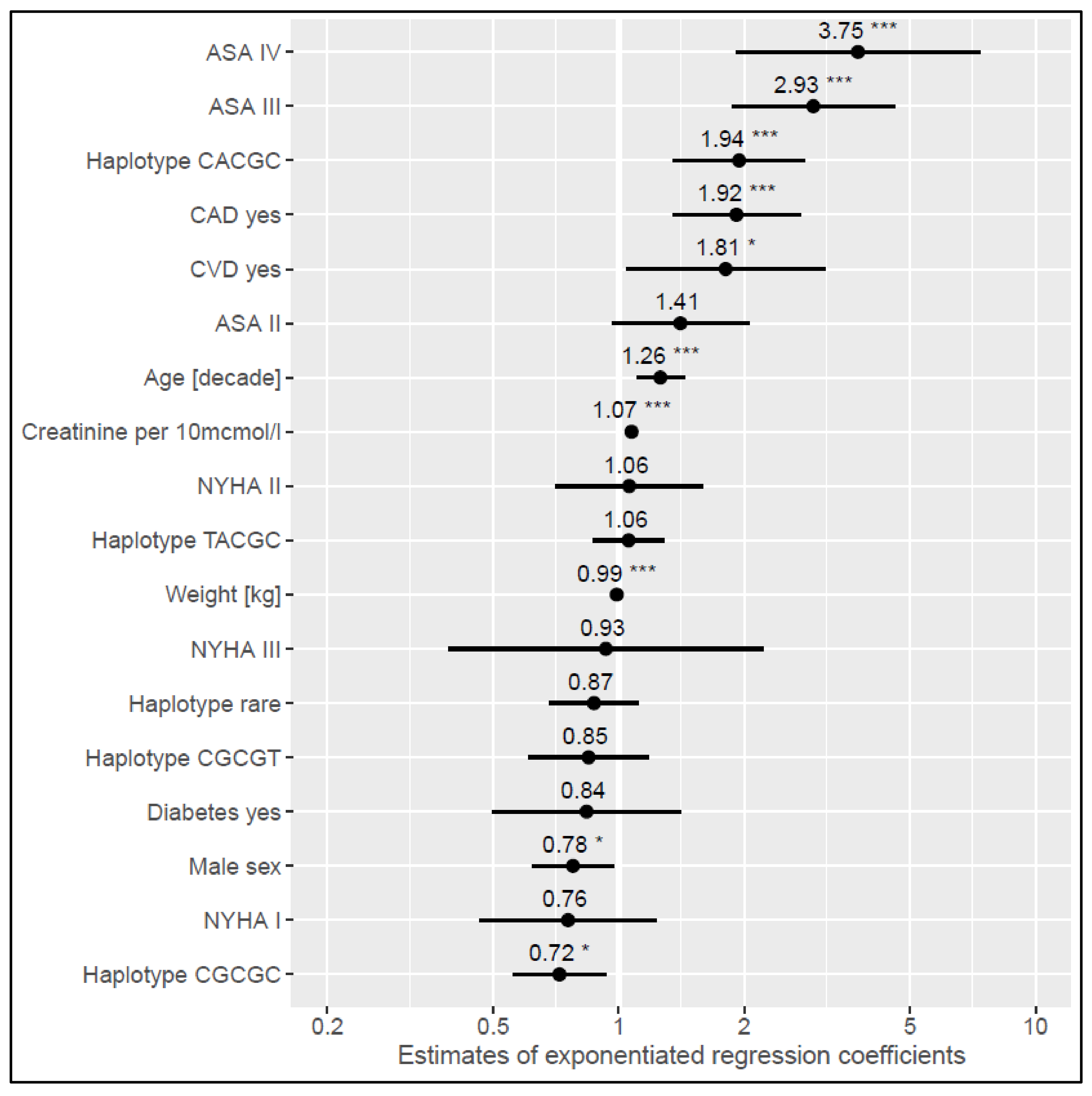
3.3. Influence of Common Haplotypes on Risk Estimation
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kristensen, S.D.; Knuuti, J.; Saraste, A.; Anker, S.; Botker, H.E.; De Hert, S.; Ford, I.; Gonzalez Juanatey, J.R.; Gorenek, B.; Heyndrickx, G.R.; et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: Cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur. J. Anaesthesiol. 2014, 31, 517–573. [Google Scholar] [CrossRef] [Green Version]
- Rodseth, R.N.; Biccard, B.M.; Le Manach, Y.; Sessler, D.I.; Lurati Buse, G.A.; Thabane, L.; Schutt, R.C.; Bolliger, D.; Cagini, L.; Cardinale, D.; et al. The prognostic value of pre-operative and post-operative B-type natriuretic peptides in patients undergoing noncardiac surgery: B-type natriuretic peptide and N-terminal fragment of pro-B-type natriuretic peptide: A systematic review and individual patient data meta-analysis. J. Am. Coll. Cardiol. 2014, 63, 170–180. [Google Scholar] [CrossRef] [Green Version]
- Park, S.J.; Choi, J.H.; Cho, S.J.; Chang, S.A.; Choi, J.O.; Lee, S.C.; Park, S.W.; Oh, J.K.; Kim, D.K.; Jeon, E.S. Comparison of transthoracic echocardiography with N-terminal pro-brain natriuretic Peptide as a tool for risk stratification of patients undergoing major noncardiac surgery. Korean Circ. J. 2011, 41, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Karthikeyan, G.; Moncur, R.A.; Levine, O.; Heels-Ansdell, D.; Chan, M.T.; Alonso-Coello, P.; Yusuf, S.; Sessler, D.; Villar, J.C.; Berwanger, O.; et al. Is a pre-operative brain natriuretic peptide or N-terminal pro-B-type natriuretic peptide measurement an independent predictor of adverse cardiovascular outcomes within 30 days of noncardiac surgery? A systematic review and meta-analysis of observational studies. J. Am. Coll. Cardiol. 2009, 54, 1599–1606. [Google Scholar] [CrossRef] [Green Version]
- Lurati Buse, G.A.; Koller, M.T.; Burkhart, C.; Seeberger, M.D.; Filipovic, M. The predictive value of preoperative natriuretic peptide concentrations in adults undergoing surgery: A systematic review and meta-analysis. Anesth. Analg. 2011, 112, 1019–1033. [Google Scholar] [CrossRef]
- Rodseth, R.N.; Biccard, B.M.; Chu, R.; Lurati Buse, G.A.; Thabane, L.; Bakhai, A.; Bolliger, D.; Cagini, L.; Cahill, T.J.; Cardinale, D.; et al. Postoperative B-type natriuretic peptide for prediction of major cardiac events in patients undergoing noncardiac surgery: Systematic review and individual patient meta-analysis. Anesthesiology 2013, 119, 270–283. [Google Scholar] [CrossRef] [Green Version]
- Rodseth, R.N.; Lurati Buse, G.A.; Bolliger, D.; Burkhart, C.S.; Cuthbertson, B.H.; Gibson, S.C.; Mahla, E.; Leibowitz, D.W.; Biccard, B.M. The predictive ability of pre-operative B-type natriuretic peptide in vascular patients for major adverse cardiac events: An individual patient data meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Rodseth, R.N.; Padayachee, L.; Biccard, B.M. A meta-analysis of the utility of pre-operative brain natriuretic peptide in predicting early and intermediate-term mortality and major adverse cardiac events in vascular surgical patients. Anaesthesia 2008, 63, 1226–1233. [Google Scholar] [CrossRef]
- Ryding, A.D.; Kumar, S.; Worthington, A.M.; Burgess, D. Prognostic value of brain natriuretic peptide in noncardiac surgery: A meta-analysis. Anesthesiology 2009, 111, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Young, Y.R.; Sheu, B.F.; Li, W.C.; Hsieh, T.M.; Hung, C.W.; Chang, S.S.; Lee, C.C. Predictive value of plasma brain natriuretic peptide for postoperative cardiac complications--a systemic review and meta-analysis. J. Crit. Care 2014, 29, 696.e1–696.e10. [Google Scholar] [CrossRef]
- Duceppe, E.; Parlow, J.; MacDonald, P.; Lyons, K.; McMullen, M.; Srinathan, S.; Graham, M.; Tandon, V.; Styles, K.; Bessissow, A.; et al. Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery. Can. J. Cardiol. 2017, 33, 17–32. [Google Scholar] [CrossRef] [Green Version]
- Duceppe, E.; Patel, A.; Chan, M.T.V.; Berwanger, O.; Ackland, G.; Kavsak, P.A.; Rodseth, R.; Biccard, B.; Chow, C.K.; Borges, F.K.; et al. Preoperative N-Terminal Pro-B-Type Natriuretic Peptide and Cardiovascular Events After Noncardiac Surgery: A Cohort Study. Ann. Intern. Med. 2020, 172, 96–104. [Google Scholar] [CrossRef]
- Raymond, I.; Groenning, B.A.; Hildebrandt, P.R.; Nilsson, J.C.; Baumann, M.; Trawinski, J.; Pedersen, F. The influence of age, sex and other variables on the plasma level of N-terminal pro brain natriuretic peptide in a large sample of the general population. Heart 2003, 89, 745–751. [Google Scholar] [CrossRef]
- Takeishi, Y.; Toriyama, S.; Takabatake, N.; Shibata, Y.; Konta, T.; Emi, M.; Kato, T.; Kawata, S.; Kubota, I. Linkage disequilibrium analyses of natriuretic peptide precursor B locus reveal risk haplotype conferring high plasma BNP levels. Biochem. Biophys. Res. Commun. 2007, 362, 480–484. [Google Scholar] [CrossRef] [Green Version]
- Ellis, K.L.; Newton-Cheh, C.; Wang, T.J.; Frampton, C.M.; Doughty, R.N.; Whalley, G.A.; Ellis, C.J.; Skelton, L.; Davis, N.; Yandle, T.G.; et al. Association of genetic variation in the natriuretic peptide system with cardiovascular outcomes. J. Mol. Cell. Cardiol. 2011, 50, 695–701. [Google Scholar] [CrossRef]
- Maimaitiming, S.; Roussel, R.; Hadjadj, S.; Fumeron, F.; Aubert, R.; Emery, N.; Velho, G.; Mohammedi, K.; Travert, F.; Tichet, J.; et al. Association of common variants in NPPA and NPPB with blood pressure does not translate into kidney damage in a general population study. J. Hypertens. 2010, 28, 1230–1233. [Google Scholar] [CrossRef]
- Newton-Cheh, C.; Larson, M.G.; Vasan, R.S.; Levy, D.; Bloch, K.D.; Surti, A.; Guiducci, C.; Kathiresan, S.; Benjamin, E.J.; Struck, J.; et al. Association of common variants in NPPA and NPPB with circulating natriuretic peptides and blood pressure. Nat. Genet. 2009, 41, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Pfister, R.; Sharp, S.; Luben, R.; Welsh, P.; Barroso, I.; Salomaa, V.; Meirhaeghe, A.; Khaw, K.T.; Sattar, N.; Langenberg, C.; et al. Mendelian randomization study of B-type natriuretic peptide and type 2 diabetes: Evidence of causal association from population studies. PLoS Med. 2011, 8, e1001112. [Google Scholar] [CrossRef]
- Mayhew, D.; Mendonca, V.; Murthy, B.V.S. A review of ASA physical status - historical perspectives and modern developments. Anaesthesia 2019, 74, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Lake, S.L.; Lyon, H.; Tantisira, K.; Silverman, E.K.; Weiss, S.T.; Laird, N.M.; Schaid, D.J. Estimation and tests of haplotype-environment interaction when linkage phase is ambiguous. Hum. Hered. 2003, 55, 56–65. [Google Scholar] [CrossRef]
- Schaid, D.J.; Rowland, C.M.; Tines, D.E.; Jacobson, R.M.; Poland, G.A. Score tests for association between traits and haplotypes when linkage phase is ambiguous. Am. J. Hum. Genet. 2002, 70, 425–434. [Google Scholar] [CrossRef] [Green Version]
- Del Greco, M.F.; Pattaro, C.; Luchner, A.; Pichler, I.; Winkler, T.; Hicks, A.A.; Fuchsberger, C.; Franke, A.; Melville, S.A.; Peters, A.; et al. Genome-wide association analysis and fine mapping of NT-proBNP level provide novel insight into the role of the MTHFR-CLCN6-NPPA-NPPB gene cluster. Hum. Mol. Genet. 2011, 20, 1660–1671. [Google Scholar] [CrossRef]
- Warnes, G.; Gorjanc, G.; Leisch, F.; Man, M. Genetics: Population Genetics. R Package Version 1.3.8.1.3. Available online: https://CRAN.R-project.org/package=genetics (accessed on 1 October 2021).
- Sinnwell, J.; Schaid, D. haplo.stats: Statistical Analysis of Haplotypes with Traits and Covariates When Linkage Phase Is Ambiguous. R Package Version 1.8.7. Available online: https://CRAN.R-project.org/package=haplo.stats (accessed on 1 October 2021).
- Cannone, V.; Boerrigter, G.; Cataliotti, A.; Costello-Boerrigter, L.C.; Olson, T.M.; McKie, P.M.; Heublein, D.M.; Lahr, B.D.; Bailey, K.R.; Averna, M.; et al. A genetic variant of the atrial natriuretic peptide gene is associated with cardiometabolic protection in the general community. J. Am. Coll. Cardiol. 2011, 58, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Cannone, V.; Cefalu, A.B.; Noto, D.; Scott, C.G.; Bailey, K.R.; Cavera, G.; Pagano, M.; Sapienza, M.; Averna, M.R.; Burnett, J.C., Jr. The atrial natriuretic peptide genetic variant rs5068 is associated with a favorable cardiometabolic phenotype in a Mediterranean population. Diabetes Care 2013, 36, 2850–2856. [Google Scholar] [CrossRef] [Green Version]
- Cannone, V.; Scott, C.G.; Decker, P.A.; Larson, N.B.; Palmas, W.; Taylor, K.D.; Wang, T.J.; Gupta, D.K.; Bielinski, S.J.; Burnett, J.C., Jr. A favorable cardiometabolic profile is associated with the G allele of the genetic variant rs5068 in African Americans: The Multi-Ethnic Study of Atherosclerosis (MESA). PloS ONE 2017, 12, e0189858. [Google Scholar] [CrossRef] [Green Version]
- Seidelmann, S.B.; Vardeny, O.; Claggett, B.; Yu, B.; Shah, A.M.; Ballantyne, C.M.; Selvin, E.; MacRae, C.A.; Boerwinkle, E.; Solomon, S.D. An NPPB Promoter Polymorphism Associated With Elevated N-Terminal pro-B-Type Natriuretic Peptide and Lower Blood Pressure, Hypertension, and Mortality. J. Am. Heart Assoc. 2017, 6, e005257. [Google Scholar] [CrossRef] [Green Version]
- Conen, D.; Cheng, S.; Steiner, L.L.; Buring, J.E.; Ridker, P.M.; Zee, R.Y. Association of 77 polymorphisms in 52 candidate genes with blood pressure progression and incident hypertension: The Women’s Genome Health Study. J. Hypertens. 2009, 27, 476–483. [Google Scholar] [CrossRef]
- Johansson, A.; Eriksson, N.; Lindholm, D.; Varenhorst, C.; James, S.; Syvanen, A.C.; Axelsson, T.; Siegbahn, A.; Barratt, B.J.; Becker, R.C.; et al. Genome-wide association and Mendelian randomization study of NT-proBNP in patients with acute coronary syndrome. Hum. Mol. Genet. 2016, 25, 1447–1456. [Google Scholar] [CrossRef]
- Pfister, R.; Luben, R.N.; Khaw, K.T.; Wareham, N.J. Common genetic variants of the natriuretic peptide gene locus are not associated with heart failure risk in participants in the EPIC-Norfolk study. Eur. J. Heart Fail. 2013, 15, 624–627. [Google Scholar] [CrossRef]
- Fox, A.A.; Collard, C.D.; Shernan, S.K.; Seidman, C.E.; Seidman, J.G.; Liu, K.Y.; Muehlschlegel, J.D.; Perry, T.E.; Aranki, S.F.; Lange, C.; et al. Natriuretic peptide system gene variants are associated with ventricular dysfunction after coronary artery bypass grafting. Anesthesiology 2009, 110, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Malhotra, A.K.; Ramakrishna, H. N-terminal pro B type natriuretic peptide in high cardiovascular-risk patients for noncardiac surgery: What is the current prognostic evidence? Ann. Card. Anaesth. 2016, 19, 314–320. [Google Scholar] [CrossRef]
- Fleisher, L.A.; Fleischmann, K.E.; Auerbach, A.D.; Barnason, S.A.; Beckman, J.A.; Bozkurt, B.; Davila-Roman, V.G.; Gerhard-Herman, M.D.; Holly, T.A.; Kane, G.C.; et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 2014, 64, e77–e137. [Google Scholar] [CrossRef] [Green Version]
- Vasile, V.C.; Jaffe, A.S. Natriuretic Peptides and Analytical Barriers. Clin. Chem. 2017, 63, 50–58. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Covariate | Subgroup | n (%) | BNP [ng l−1] | NT-proBNP [ng l−1] |
|---|---|---|---|---|
| Sex | Female | 187 (44) | 26.0 (14.0, 55.0) | 72.0 (43.5, 155.5) |
| Male | 239 (56) | 22.0 (10.0, 56.0) | 58.0 (25.0, 195.0) | |
| Coronary artery disease | No | 383 (90) | 21.0 (12.0, 48.0) | 58.0 (30.0, 129.5) |
| Yes | 42 (10) | 101.5 (40.0, 202.5) | 331.0 (107.2, 597.2) | |
| Cerebrovascular disease | No | 410 (96) | 22.5 (12.0, 52.5) | 65.0 (31.25, 147.5) |
| Yes | 15 (4) | 97.0 (59.5, 154.0) | 478.0 (218.5, 958.5) | |
| Diabetes mellitus | No | 407 (96) | 24.0 (12.0, 54.0) | 65.0 (32.0, 151.0) |
| Yes | 17 (4) | 48.0 (15.0, 84.0) | 236.0 (67.0, 466.0) | |
| ASA physical classification | 1 | 60 (14) | 15.5 (9.0, 22.0) | 33.5 (21.8, 53.3) |
| 2 | 147 (35) | 15.0 (9.0, 26.0) | 41.0 (21.0, 69.0) | |
| 3 | 205 (48) | 44.0 (21.0, 90.0) | 132.0 (66.0, 335.0) | |
| 4 | 14 (3) | 98.0 (78.5, 163.0) | 446.0 (189.2, 874.2) | |
| NYHA class | 0 | 375 (89) | 22.0 (12.0, 51.0) | 60.0 (31.0, 141.5) |
| 1 | 18 (4) | 26.0 (15.0, 76.0) | 81.5 (36.0, 176.8) | |
| 2 | 25 (6) | 37.0 (25.0, 102.0) | 132.0 (82.0, 289.0) | |
| 3 | 5 (1) | 126.0 (38.0, 174.0) | 248.0 (161.0, 466.0) |
| Genotype (n) | BNP [ng l−1] | p | NT-proBNP [ng l−1] | p | |
|---|---|---|---|---|---|
| rs198358 | TT (256) | 24.5 (12.0, 56.0) | 69.5 (34.0, 196.0) | ||
| CT (142) | 24.0 (11.0, 59.5) | 67.5 (28.3, 158.3) | |||
| CC (28) | 21.5 (16.8, 40.8) | 0.879 | 66.0 (44.0, 123.8) | 0.562 | |
| rs5068 | AA (283) | 25.0 (13.0, 62.0) | 73.0 (35.5, 206.5) | ||
| AG (126) | 22.0 (11.0, 51.0) | 58.0 (27.3, 148.0) | |||
| GG (17) | 21.0 (16.0, 32.0) | 0.565 | 66.0 (44.0, 77.0) | 0.110 | |
| rs632793 | TT (152) | 21.5 (11.8, 44.3) | 62.0 (33.0, 123.8) | ||
| TC (210) | 22.0 (11.3, 62.5) | 65.5 (29.0, 166.0) | |||
| CC (64) | 40.5 (19.0, 103.3) | <0.001 * | 99.5 (54.8, 346.0) | 0.010 | |
| rs198389 | AA (143) | 21.0 (12.0, 43.0) | 60.0 (33.5, 125.5) | ||
| GA (215) | 21.0 (11.0, 63.5) | 65.0 (27.5, 174.0) | |||
| GG (68) | 40.5 (19.8, 92.6) | <0.001 * | 83.5 (56.5, 273.5) | 0.015 | |
| rs6676300 | TT (176) | 20.0 (12.0, 45.3) | 57.0 (31.8, 123.8) | ||
| CT (189) | 26.0 (11.0, 65.0) | 71.0 (29.0, 176.0) | |||
| CC (61) | 40.0 (19.0, 84.0) | 0.003 * | 82.0 (54.0, 338.0) | 0.022 |
| Haplotype | rs198358 | rs5068 | rs632793 | rs198389 | rs6676300 | Frequency |
|---|---|---|---|---|---|---|
| 1 | C | A | C | G | C | 0.04 |
| 2 | C | G | C | G | C | 0.09 |
| 3 | C | G | C | G | T | 0.05 |
| 4 | C | G | T | A | C | 0.02 |
| 5 | C | G | T | A | T | 0.01 |
| 6 | C | G | T | G | C | 0.01 |
| 7 | T | A | C | G | C | 0.18 |
| 8 | T | A | C | G | T | 0.02 |
| 9 | T | A | T | A | T | 0.53 |
| 10 | T | A | T | G | C | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hahn, M.; Stamer, U.M.; Luedi, M.M.; Book, M.; Rieder, H.U.; Stüber, F. ASA Status, NPPA/NPPB Haplotype and Coronary Artery Disease Have an Impact on BNP/NT-proBNP Plasma Levels. Cells 2022, 11, 766. https://doi.org/10.3390/cells11050766
Hahn M, Stamer UM, Luedi MM, Book M, Rieder HU, Stüber F. ASA Status, NPPA/NPPB Haplotype and Coronary Artery Disease Have an Impact on BNP/NT-proBNP Plasma Levels. Cells. 2022; 11(5):766. https://doi.org/10.3390/cells11050766
Chicago/Turabian StyleHahn, Markus, Ulrike M. Stamer, Markus M. Luedi, Malte Book, Heinz U. Rieder, and Frank Stüber. 2022. "ASA Status, NPPA/NPPB Haplotype and Coronary Artery Disease Have an Impact on BNP/NT-proBNP Plasma Levels" Cells 11, no. 5: 766. https://doi.org/10.3390/cells11050766
APA StyleHahn, M., Stamer, U. M., Luedi, M. M., Book, M., Rieder, H. U., & Stüber, F. (2022). ASA Status, NPPA/NPPB Haplotype and Coronary Artery Disease Have an Impact on BNP/NT-proBNP Plasma Levels. Cells, 11(5), 766. https://doi.org/10.3390/cells11050766