
New Genetic Biomarkers of the Overlap Syndrome Tension-Type Headache and Arterial Hypertension
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
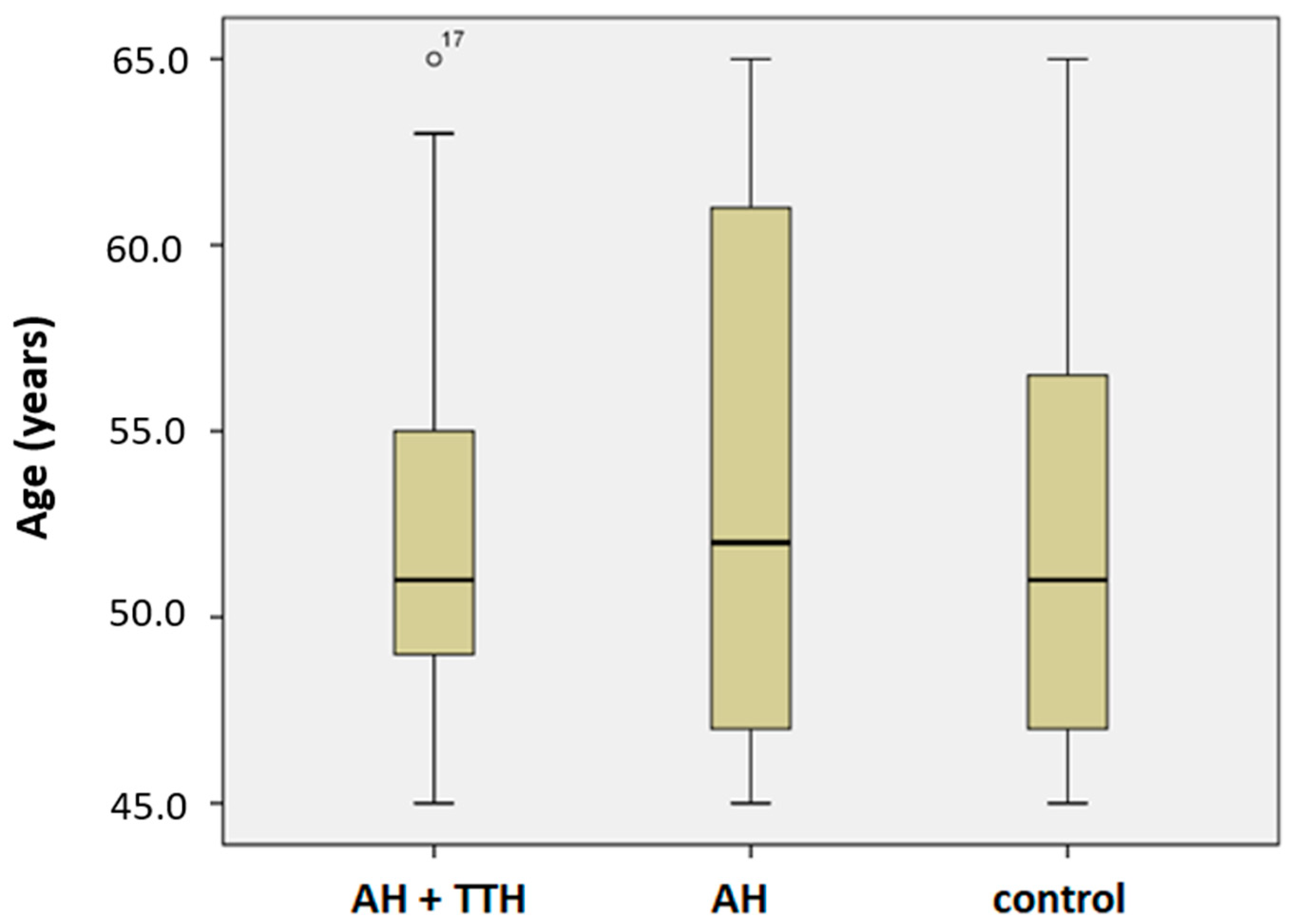
2.2. Study Population
- Russian-speaking residents of a large industrial city of the Siberian Federal District of the Russian Federation (Krasnoyarsk);
- Caucasians;
- Adults: World Health Organization (WHO) [26] first median age (male: 45 to 65 years old, female: 40 to 60 years old);
- AH (diagnosed by a cardiologist or general practitioner);
- TTH (diagnosed by a neurologist or general practitioner);
- Signed voluntary informed consent to participate in this study.
- Criteria for inclusion in group 2 (AH without headache):
- Russian-speaking residents of a large industrial city of the Siberian Federal District of the Russian Federation (Krasnoyarsk);
- Caucasians;
- Adults: WHO [26] first median age (male: 45 to 65 years old, female: 40 to 60 years old);
- AH (diagnosed by a cardiologist or general practitioner);
- Signed voluntary informed consent to participate in this study.
- Russian-speaking residents of a large industrial city of the Siberian Federal District of the Russian Federation (Krasnoyarsk);
- Caucasians;
- Adults: WHO [26] first median age (male: 45 to 65 years old, female: 40 to 60 years old);
- Signed voluntary informed consent to participate in this study.
- Non-Russian-speaking residents of a large industrial city in the Siberian Federal District of the Russian Federation (Krasnoyarsk): migrants, representatives of small ethnic groups in Siberia;
- Asians;
- Refusal to participate in this study;
- Refusal to comply with the full protocol of this study;
- Participation in other studies;
- Severe cognitive disorders and dementia of any etiology;
- Acute infectious diseases;
- Diabetes;
- Other primary headaches (except TTH);
- Secondary headaches;
- Traumatic brain injury;
- History of stroke and transient ischemic attacks;
- Epilepsy and epileptic syndromes;
- Chronic renal and hepatic insufficiency;
- Chronic heart failure (New York Heart Association Functional Classification: class II and above).
2.3. Genetic Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristic
3.2. Frequency Distribution of Genotypes and Alleles in the TTH and AH/AH Patients and Control
4. Discussion
5. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moskaleva, P.V.; Khramchenko, M.A.; Karpenkova, A.D.; Petrova, M.M.; Shnayder, N.A. Modern concepts about pathogenesis of the tension-type headache and mechanisms of development of the tension-type headache and arterial hypertension phenotype. Russ. Neurol. J. 2022, 27, 22–33. (In Russian) [Google Scholar] [CrossRef]
- Shnayder, N.; Petrova, M.; Moskaleva, P.; Shesternya, P.; Pozhilenkova, E.; Nasyrova, R. The Role of Single-Nucleotide Variants of NOS1, NOS2, and NOS3 Genes in the Comorbidity of Arterial Hypertension and Tension-Type Headache. Molecules 2021, 26, 1556. [Google Scholar] [CrossRef] [PubMed]
- Nasyrova, R.F.; Moskaleva, P.V.; Vaiman, E.E.; Shnayder, N.A.; Blatt, N.L.; Rizvanov, A.A. Genetic Factors of Nitric Oxide’s System in Psychoneurologic Disorders. Int. J. Mol. Sci. 2020, 21, 1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geller, D.A.; Lowenstein, C.J.; Shapiro, R.A.; Nussler, A.K.; Di Silvio, M.; Wang, S.C.; Nakayama, D.K.; Simmons, R.L.; Snyder, S.H.; Billiar, T.R. Molecular cloning and expression of inducible nitric oxide synthase from human hepatocytes. Proc. Natl. Acad. Sci. USA 1993, 90, 3491–3495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hancock, D.B.; Martin, E.R.; Vance, J.M.; Scott, W.K. Nitric oxide synthase genes and their interactions with environmental factors in Parkinson’s disease. Neurogenetics 2008, 9, 249–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomsen, L.L.; Olesen, J. Nitric oxide in primary headaches. Curr. Opin. Neurol. 2001, 14, 315–321. [Google Scholar] [CrossRef]
- Sarchielli, P.; Alberti, A.; Floridi, A.; Gallai, V. L-Arginine/nitric oxide pathway in chronic tension-type headache: Relation with serotonin content and secretion and glutamate content. J. Neurol. Sci. 2002, 198, 9–15. [Google Scholar] [CrossRef]
- Ashina, M. Nitric oxide synthase inhibitors for the treatment of chronic tension-type headache. Expert Opin. Pharmacother. 2002, 3, 395–399. [Google Scholar] [CrossRef]
- Isaak, A.; Ellrich, J. Neuronal nitric oxide synthase is involved in the induction of nerve growth factor-induced neck muscle nociception. Headache 2011, 51, 734–743. [Google Scholar] [CrossRef]
- Wu, J.; Fang, L.; Lin, Q.; Willis, W.D. Nitric oxide synthase in spinal cord central sensitization following intradermal injection of capsaicin. Pain 2001, 94, 47–58. [Google Scholar] [CrossRef]
- Hermann, M.; Flammer, A.; Lüscher, T.F. Nitric oxide in hypertension. J. Clin. Hypertens. 2006, 8 (Suppl. S4), 17–29. [Google Scholar] [CrossRef] [PubMed]
- Kelm, M.; Preik, M.; Hafner, D.J.; Strauer, B.E. Evidence for a multifactorial process involved in the impaired flow response to nitric oxide in hypertensive patients with endothelial dysfunction. Hypertension 1996, 27 Pt 1, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Kiefer, F.N.; Neysari, S.; Humar, R.; Li, W.; Munk, V.C.; Battegay, E.J. Hypertension and angiogenesis. Curr. Pharm. Des. 2003, 9, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Schlaich, M.P.; Parnell, M.M.; Ahlers, B.A.; Finch, S.; Marshall, T.; Zhang, W.Z.; Kaye, D.M. Impaired L-arginine transport and endothelial function in hypertensive and genetically predisposed normotensive subjects. Circulation 2004, 110, 3680–3686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BioGPS. Available online: https://www.BioGPS.org (accessed on 1 September 2022).
- Moskaleva, P.; Shnayder, N.; Petrova, M.; Kaskaeva, D.; Gavrilyuk, O.; Radostev, S.; Garganeeva, N.; Sharavii, V.; Vaiman, E.; Nasyrova, R. The Role of Single Nucleotide Variants of NOS1, NOS2, and NOS3 Genes in the Development of the Phenotype of Migraine and Arterial Hypertension. Brain Sci. 2021, 11, 753. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.D.; Gus, M.; Moreira, L.B.; Moreira, W.D.; Gonçalves, S.C.; Nunes, G. Headache is not more frequent among patients with moderate to severe hypertension. J. Hum. Hypertens. 2003, 17, 787–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokar, O.O.; Zhmerenetsky, K.V.; Zadneprovskaya, V.V.; Nevrycheva, E.V. Evaluation of extracranial and intracranial arterial blood flow in young patients with arterial hypertension associated with migraine or tension-type headache. Dal’nevostochnyj Med. Zhurnal 2020, 1, 28–36. [Google Scholar]
- Levinsson, A.; Olin, A.-C.; Björck, L.; Rosengren, A.; Nyberg, F. Nitric oxide synthase (NOS) single nucleotide polymorphisms are associated with coronary heart disease and hypertension in the INTERGENE study. Nitric Oxide 2014, 39, 1–7. [Google Scholar] [CrossRef]
- WMA. Available online: https://www.wma.net/ (accessed on 1 September 2022).
- Altman, D.G. Practical Statistics for Medical Research; Chapman Hall/CRC Press: Boca Raton, FL, USA, 1990; pp. 456–624. [Google Scholar]
- MedStatistic Calculators. Available online: https://medstatistic.ru/calculators.html (accessed on 28 September 2022). (In Russian).
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. Hypertens 2018, 36, 1953–2041. [Google Scholar]
- Kobalava, Z.D.; Konradi, A.O.; Nedogoda, S.V.; Shlyakhto, E.V.; Arutyunov, G.P.; Baranova, E.I.; Barbarash, O.L.; Boitsov, S.A.; Vavilova, T.V.; Villevalde, S.V.; et al. Arterial hypertension in adults. Clinical guidelines. Russ. J. Cardiol. 2020, 25, 3786. [Google Scholar] [CrossRef] [Green Version]
- Olesen, J.; Dodick, D.W.; Ducros, A.; Evers, S.; First, M.B.; Goadsby, P.J. The International Classification of Headache Disorders. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Dyussenbayev, A. Age Periods of Human Life. Adv. Soc. Sci. Res. J. 2017, 4, 258–263. [Google Scholar] [CrossRef] [Green Version]
- Fouchier, S.; Defesche, J.; Umans-Eckenhausen, M.; Kastelein, J. The molecular basis of familial hypercholesterolemia in The Netherlands. Hum. Genet 2001, 109, 602–615. [Google Scholar] [CrossRef]
- Ariane, H.; Hughes, M. Overlap/Undifferentiated Syndromes. In Oxford Textbook of Rheumatology, 4th ed.; Watts, R.A., Conaghan, P.G., Denton, K., Foster, H., Jsaaks, J., Muller-Ladner, U., Eds.; Oxford University Press: Oxford, UK, 2013; Available online: https://doi.org/10.1093/med/9780199642489.003.0129_update_001 (accessed on 1 September 2022).
- Geography of Genetic Variants Browser. Available online: https://popgen.uchicago.edu/ggv/?data=%221000genomes%22&chr=12&pos=117771511 (accessed on 1 September 2022).
- Alaşehirli, B.; Akçalı, A.; Demiryürek, A.T.; Özel, A.; Erdal, M.E.; Neyal, M. Lack of Association Between the C276T Polymorphism of the Neuronal Nitric Oxide Synthase Gene and Migraine. Int. J. Neurosci 2012, 123, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Ishii, M.; Yahara, M.; Katoh, H.; Kawamura, M.; Shimizu, S. Polymorphisms of nitric oxide synthase and GTP cyclohy-drolase I genes in Japanese patients with medication overuse headaches. Neurol. Asia 2014, 19, 277–281. [Google Scholar]
- García-Martín, E.; Martinez, C.; Serrador, M.; Alonso-Navarro, H.; Navacerrada, F.; García-Albea, E.; Agundez, J.A.; Jiménez-Jiménez, F.J. Neuronal Nitric Oxide Synthase (nNOS, NOS1) rs693534 and rs7977109 Variants and Risk for Migraine. Headache J. Head Face Pain 2015, 55, 1209–1217. [Google Scholar] [CrossRef]
- Sapronova, M.R.; Shnaider, N.A. The epidemiological, clinical, and genetic characteristics of Parkinson’s disease (in case of Zheleznogorsk). Neurol. Neuropsychiatry Psychosom. 2014, 4, 59–64. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| General Characteristics | TTH and AH | AH | Control | p-Value |
|---|---|---|---|---|
| Duration of AH anamnesis (mean) | 12.4 ± 12.4 | 15.8 ± 9.9 | - | 0.060 |
| Age at onset of AH (mean) | 40.6 ± 11.7 | 37.8 ± 11.5 | - | 0.216 |
| Non-alcohol (%) | 26.7 | 26.7 | 22.6 | 0.914 |
| Rare alcohol (%) | 66.7 | 60.0 | 77.4 | 0.111 |
| Active alcohol (%) | 6.6 | 13.3 | 0.0 | 0.048 |
| Non-smokers (%) | 46.6 | 56.7 | 70.9 | 0.047 |
| Active smokers (%) | 36.7 | 30.0 | 19.3 | 0.319 |
| Low-salt diet (%) | 16.6 | 23.3 | 22.6 | 0.784 |
| High-salt diet (%) | 26.8 | 10.0 | 3.2 | 0.021 |
| Low physical activity (%) | 43.3 | 20.0 | 16.1 | 0.034 |
| Moderate physical activity (%) | 46.7 | 53.3 | 51.6 | 0.866 |
| Intense physical activity (%) | 10.0 | 26.7 | 32.3 | 0.101 |
| Alleles, Genotypes | TTH and AH | AH | Control | p-Value |
|---|---|---|---|---|
| C | 44 (73.3%) | 55 (91.7%) | 61 (98.4%) | 0.000065 *, 0.08 ** |
| T | 16 (26.7%) | 5 (8.3%) | 1 (1.6%) | |
| CC | 16 (53.3%) | 25 (83.3%) | 30 (96.8%) | 0.000419 *, 0.078 ** |
| CT | 12 (40.0%) | 5 (16.7%) | 1 (3.2%) | |
| TT | 2 (6.7%) | 0 (0%) | 0 (0%) | N/A *,** |
| Alleles, Genotypes | χ2 | p-Value | OR | 95% CI |
|---|---|---|---|---|
| TTH and AH vs. Control | ||||
| C | 15.959 | 0.000065 | 0.05 | 0.01–0.35 |
| T | 22.18 | 2.84–173.54 | ||
| CC | 15.556 | 0.000419 | 0.04 | 0.01–0.32 |
| CT | 20.0 | 2.4–166.97 | ||
| TT | - | - | ||
| AH vs. Control | ||||
| C | 2.945 | 0.086 | 0.18 | 0.02–1.59 |
| T | 5.55 | 0.63–48.95 | ||
| CC | 3.1 | 0.078 | 0.17 | 0.02–1.52 |
| CT | 6.0 | 0.66–54.79 | ||
| TT | - | - | ||
| TTH and AH vs. AH | ||||
| C | 6.984 | 0.008 | 0.25 | 0.09–0.74 |
| T | 4.0 | 1.36–11.77 | ||
| CC | 6.858 | 0.032 | 0.23 | 0.07–0.76 |
| CT | 3.33 | 0.99–11.14 | ||
| TT | - | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alyabyeva, P.V.; Chastina, O.V.; Petrova, M.M.; Lareva, N.V.; Garganeeva, N.P.; Chumakova, G.A.; Cherniaeva, M.S.; Shnayder, N.A. New Genetic Biomarkers of the Overlap Syndrome Tension-Type Headache and Arterial Hypertension. Genes 2022, 13, 1823. https://doi.org/10.3390/genes13101823
Alyabyeva PV, Chastina OV, Petrova MM, Lareva NV, Garganeeva NP, Chumakova GA, Cherniaeva MS, Shnayder NA. New Genetic Biomarkers of the Overlap Syndrome Tension-Type Headache and Arterial Hypertension. Genes. 2022; 13(10):1823. https://doi.org/10.3390/genes13101823
Chicago/Turabian StyleAlyabyeva, Polina V., Olga V. Chastina, Marina M. Petrova, Natalia V. Lareva, Natalia P. Garganeeva, Galina A. Chumakova, Marina S. Cherniaeva, and Natalia A. Shnayder. 2022. "New Genetic Biomarkers of the Overlap Syndrome Tension-Type Headache and Arterial Hypertension" Genes 13, no. 10: 1823. https://doi.org/10.3390/genes13101823
APA StyleAlyabyeva, P. V., Chastina, O. V., Petrova, M. M., Lareva, N. V., Garganeeva, N. P., Chumakova, G. A., Cherniaeva, M. S., & Shnayder, N. A. (2022). New Genetic Biomarkers of the Overlap Syndrome Tension-Type Headache and Arterial Hypertension. Genes, 13(10), 1823. https://doi.org/10.3390/genes13101823