
Effects of PM10 and Weather on Respiratory and Cardiovascular Diseases in the Ciuc Basin (Romanian Carpathians)

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
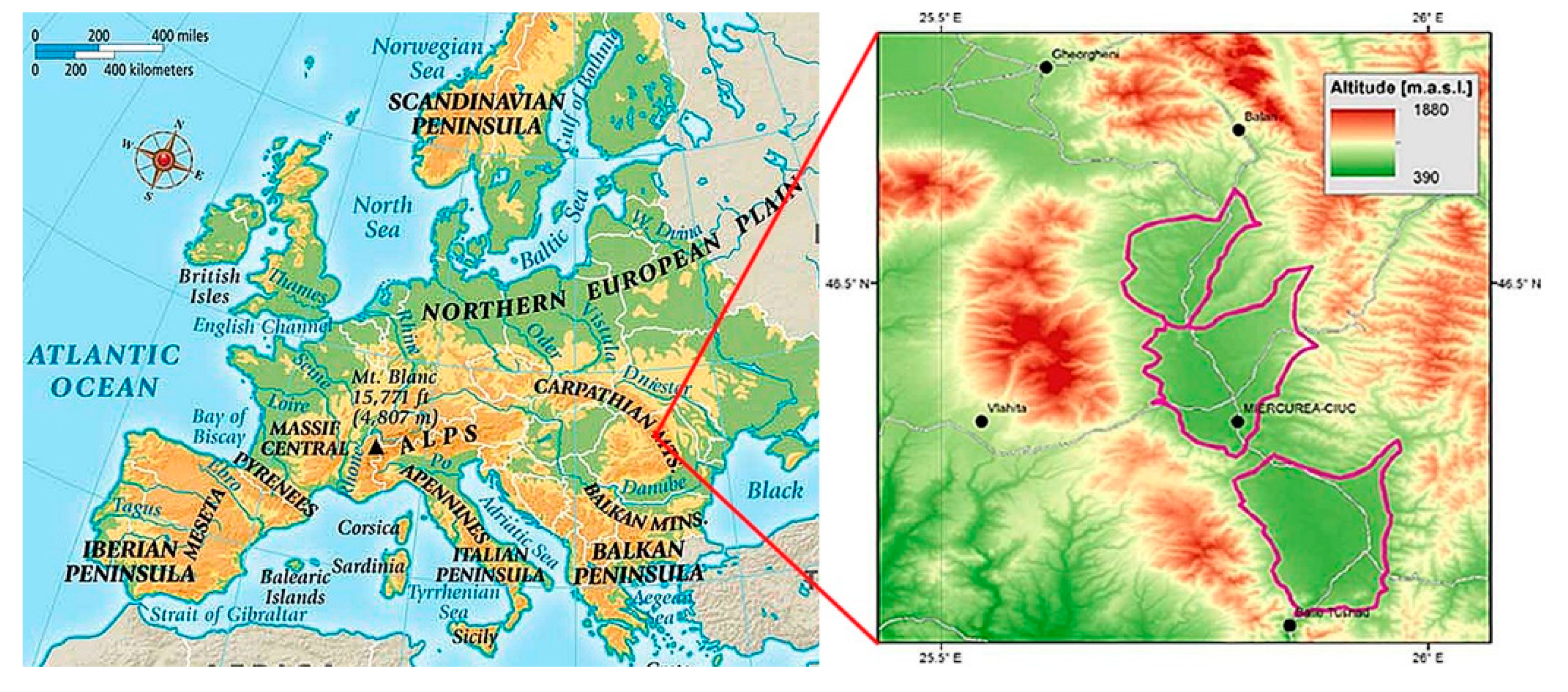
2.1. Studied Region
2.2. Air Pollution, Medical and Meteorological Data
2.3. Statistical Analysis
3. Results
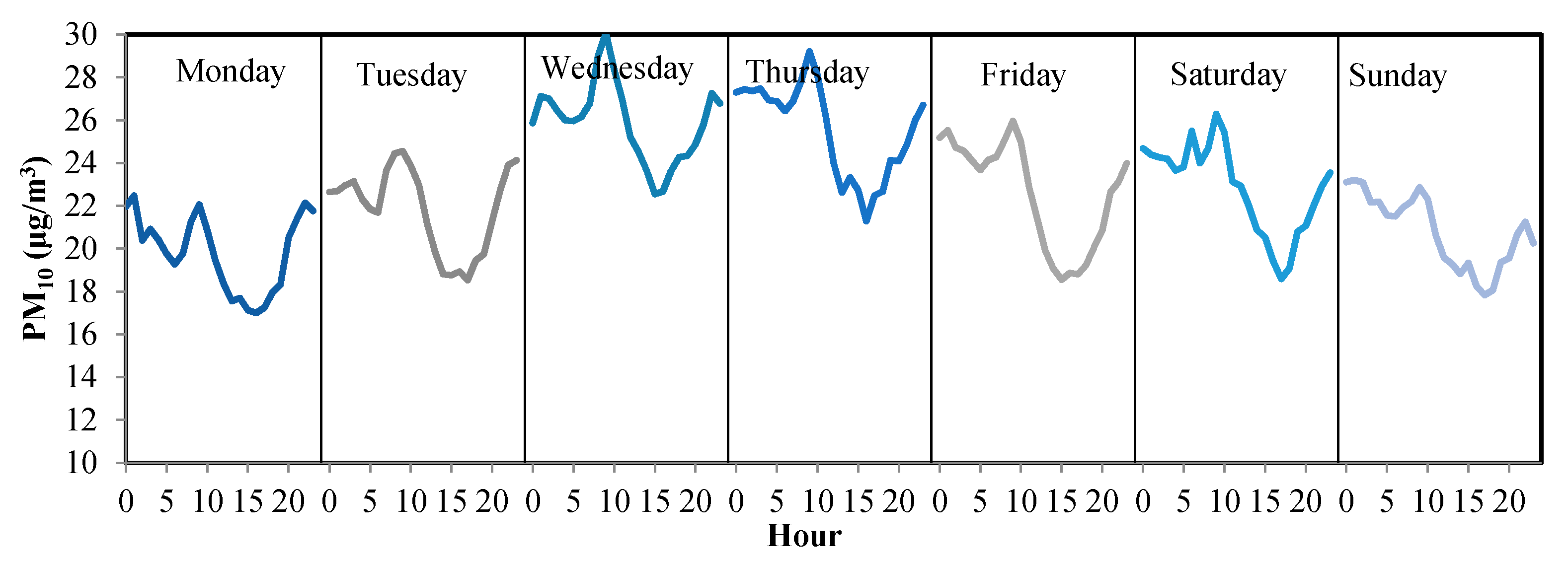
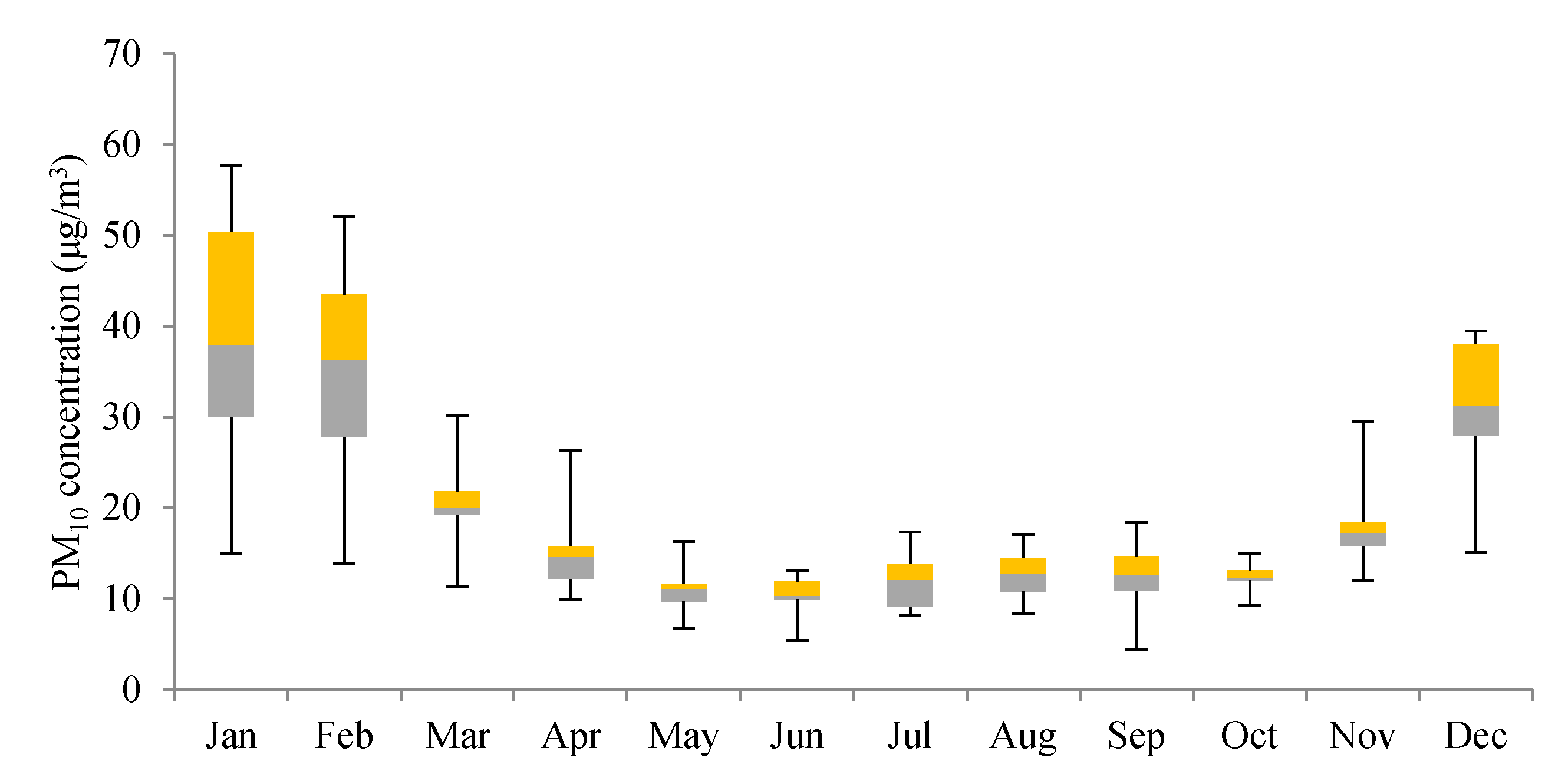
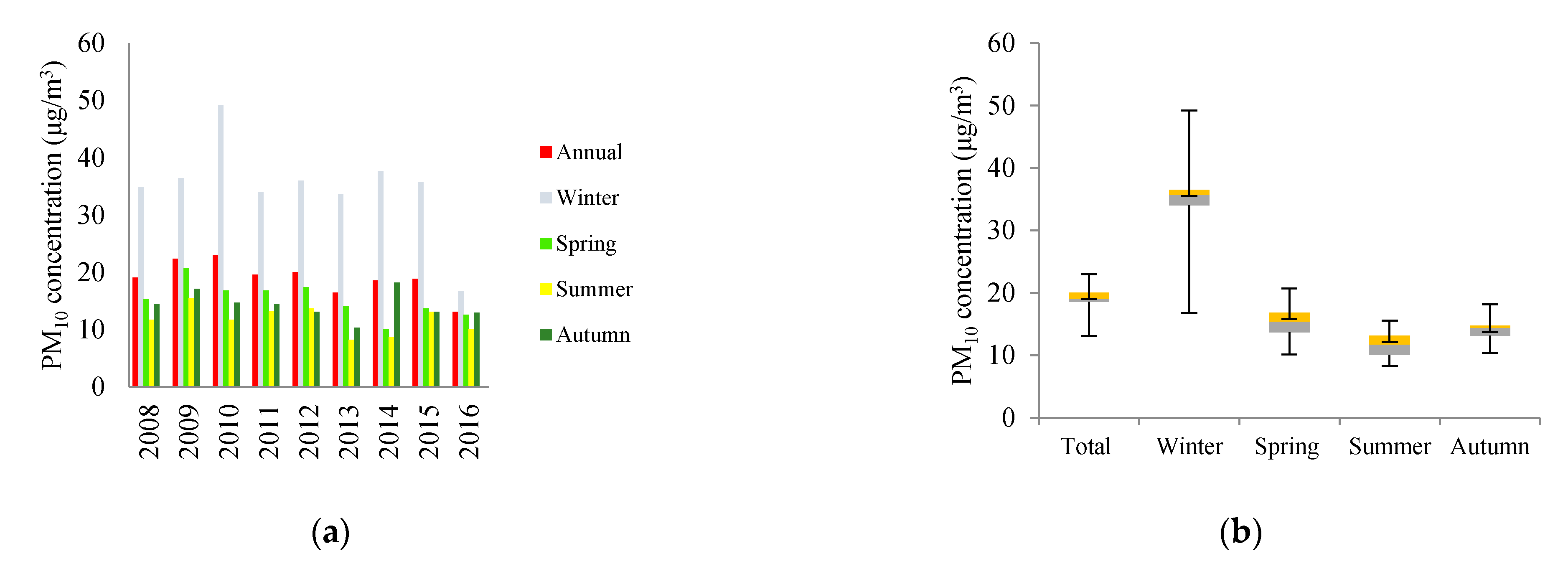
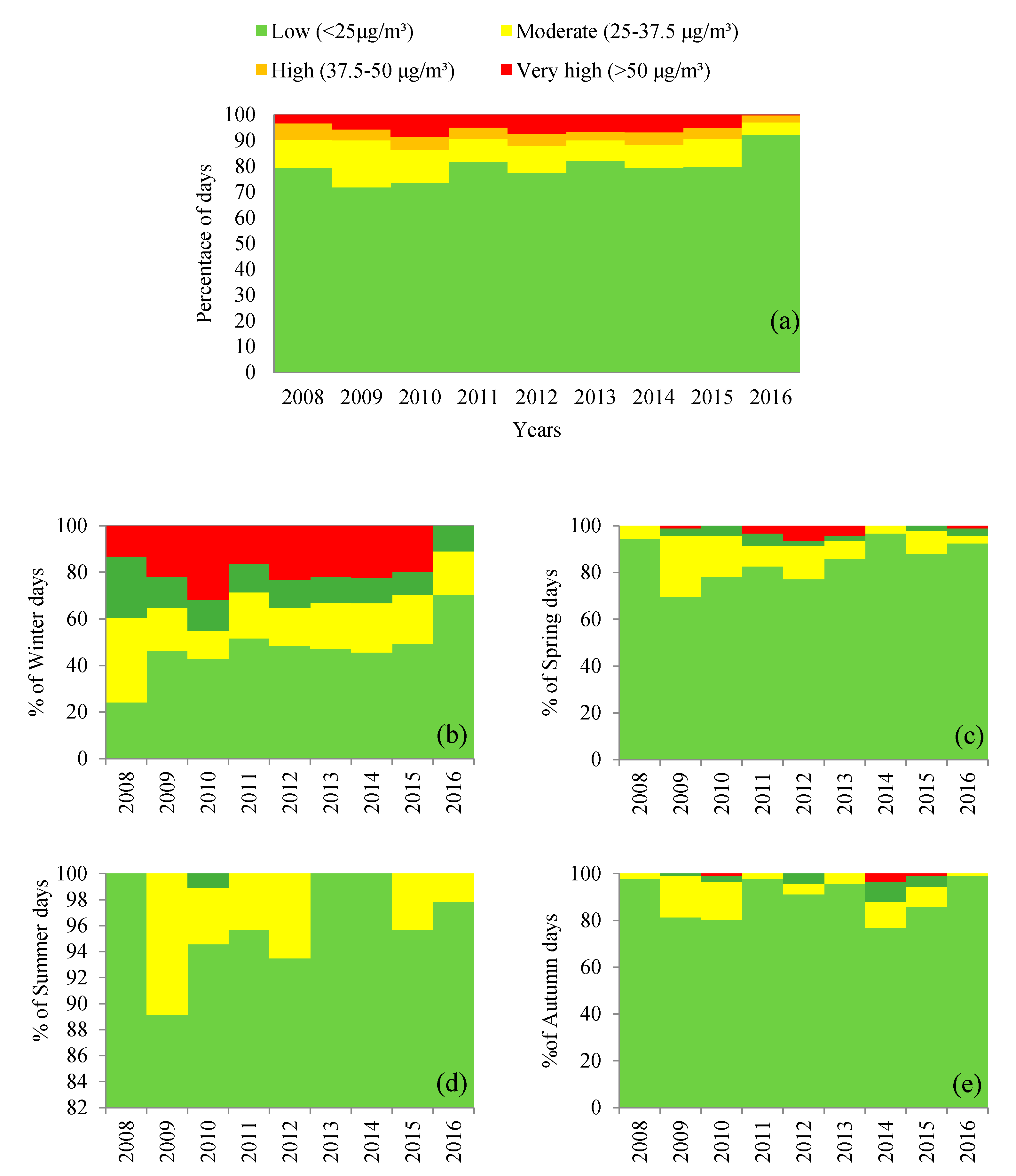
3.1. Ambient PM10 Trend
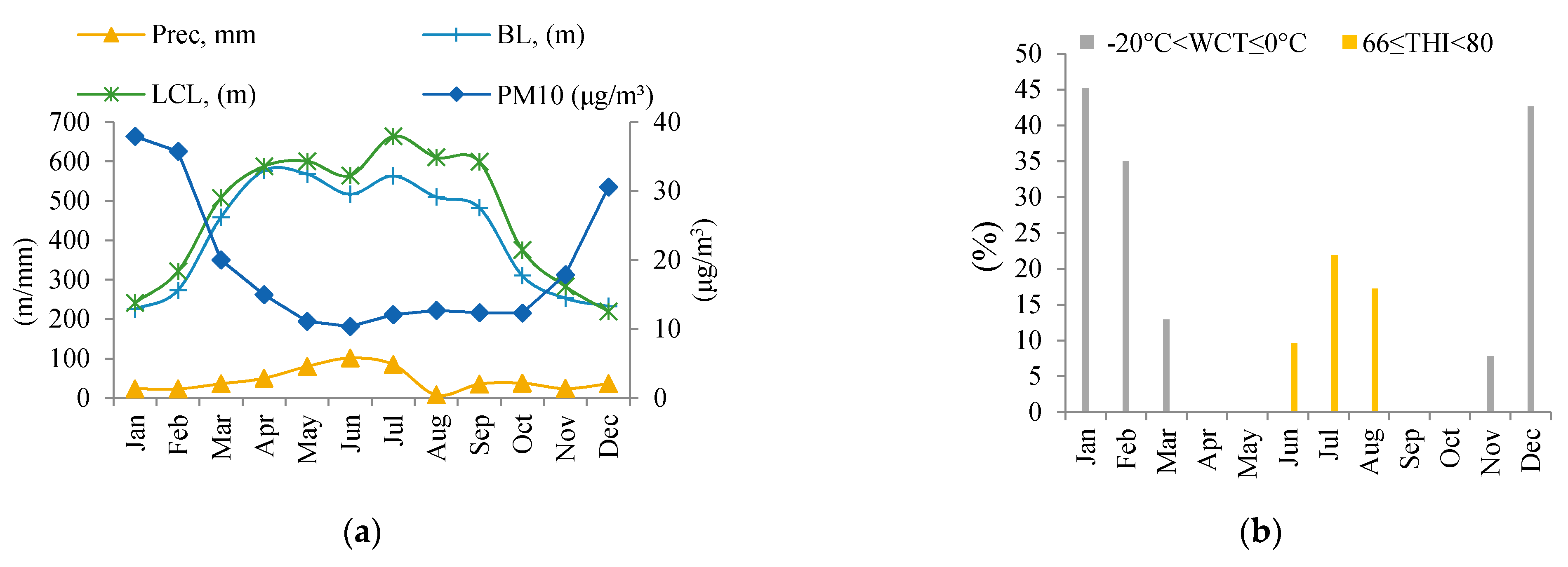
3.2. Relationship between PM10 Concentration and Meteorological Variables
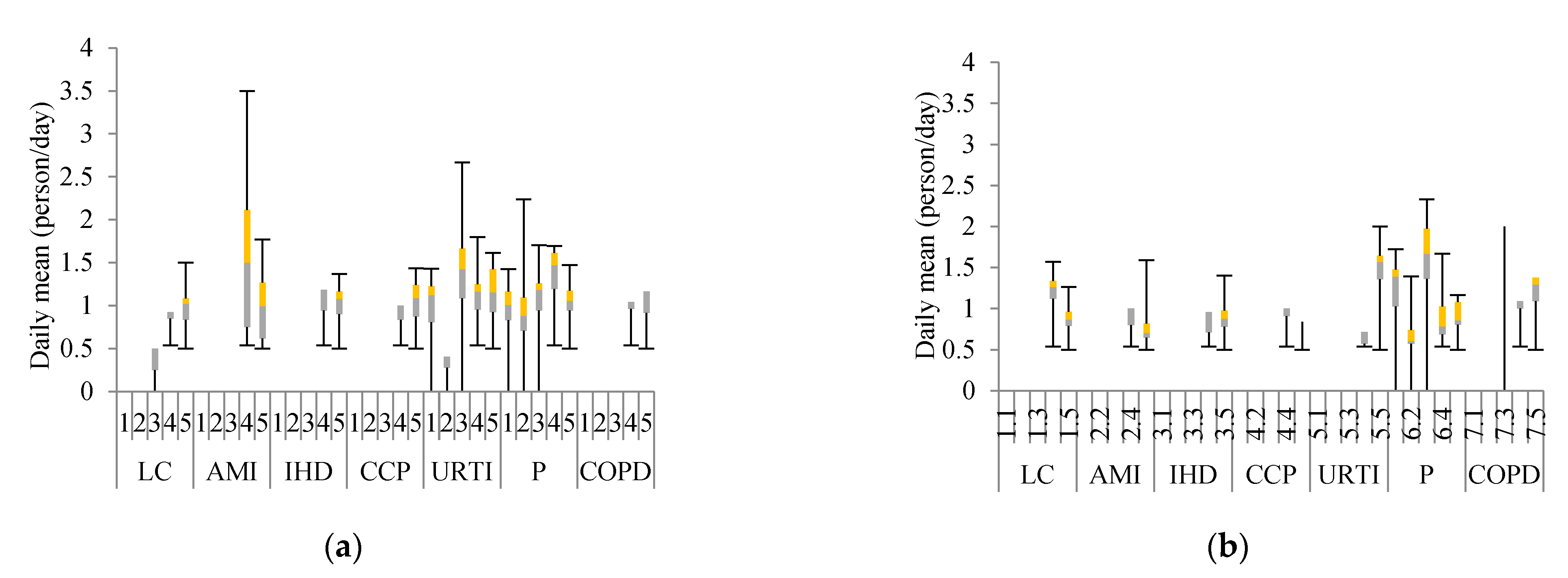
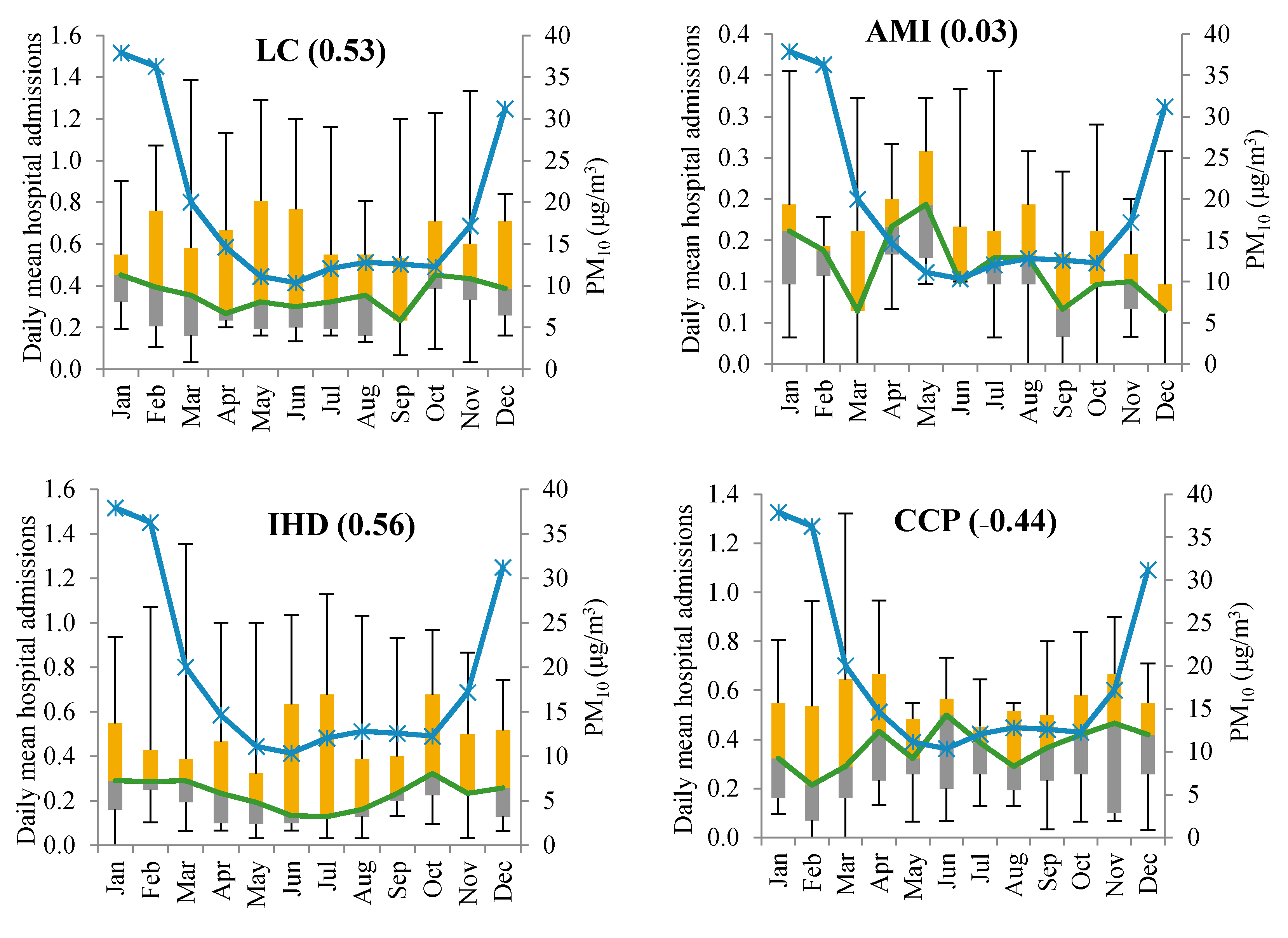
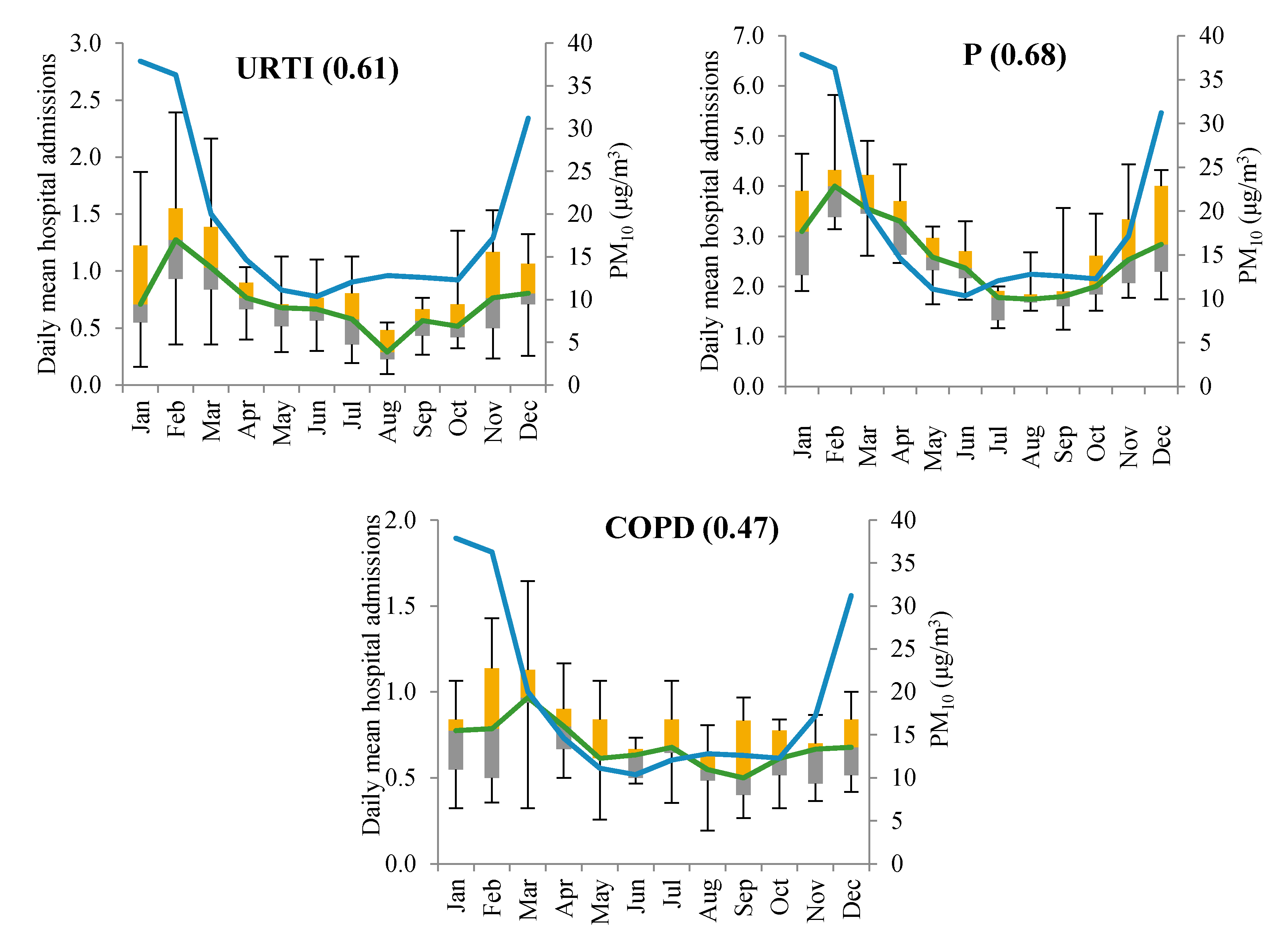
3.3. Hospital Admission Evaluation
3.4. Fourier Transformation
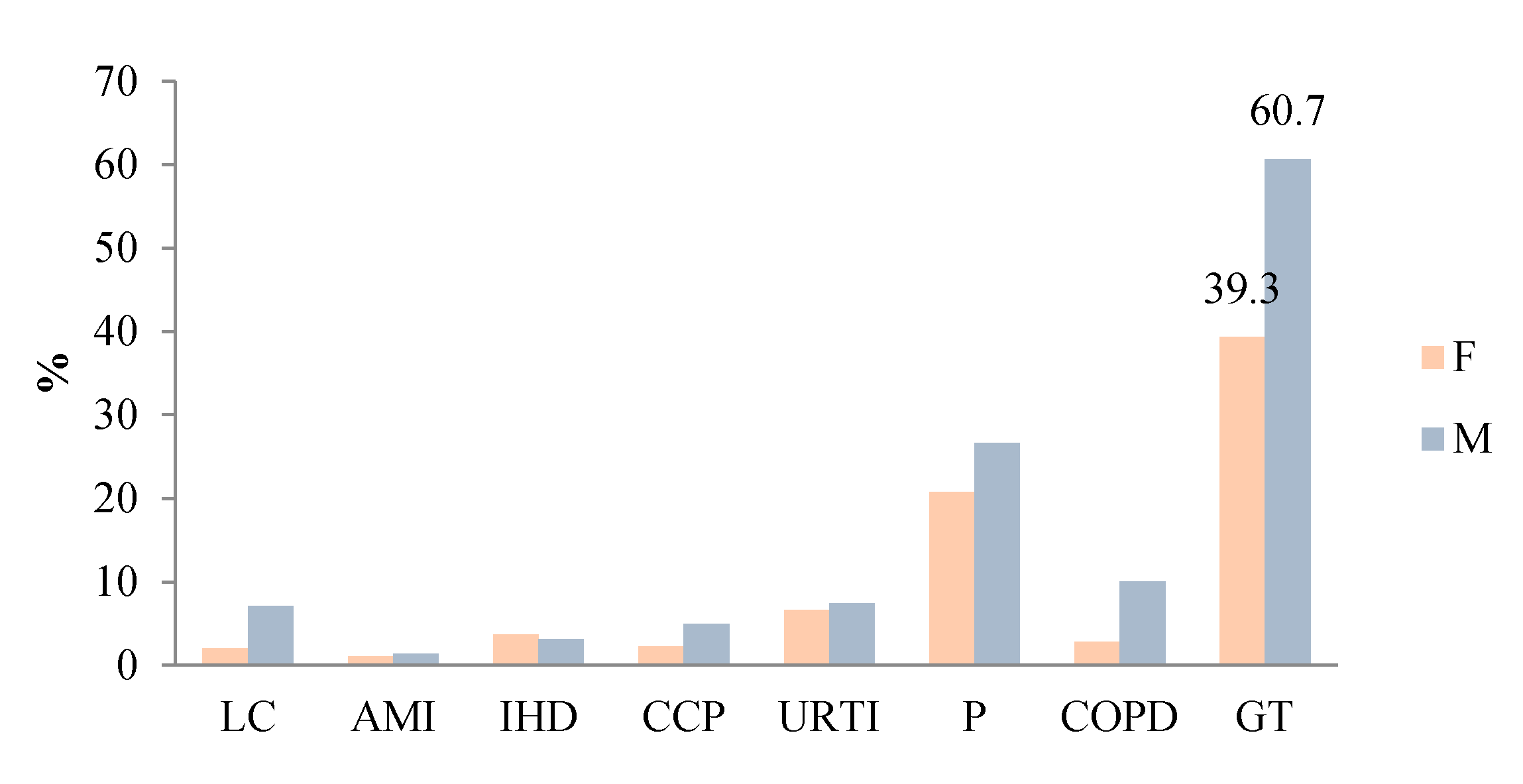
3.5. Gender Distribution of Morbidity and Relative Risk Calculation
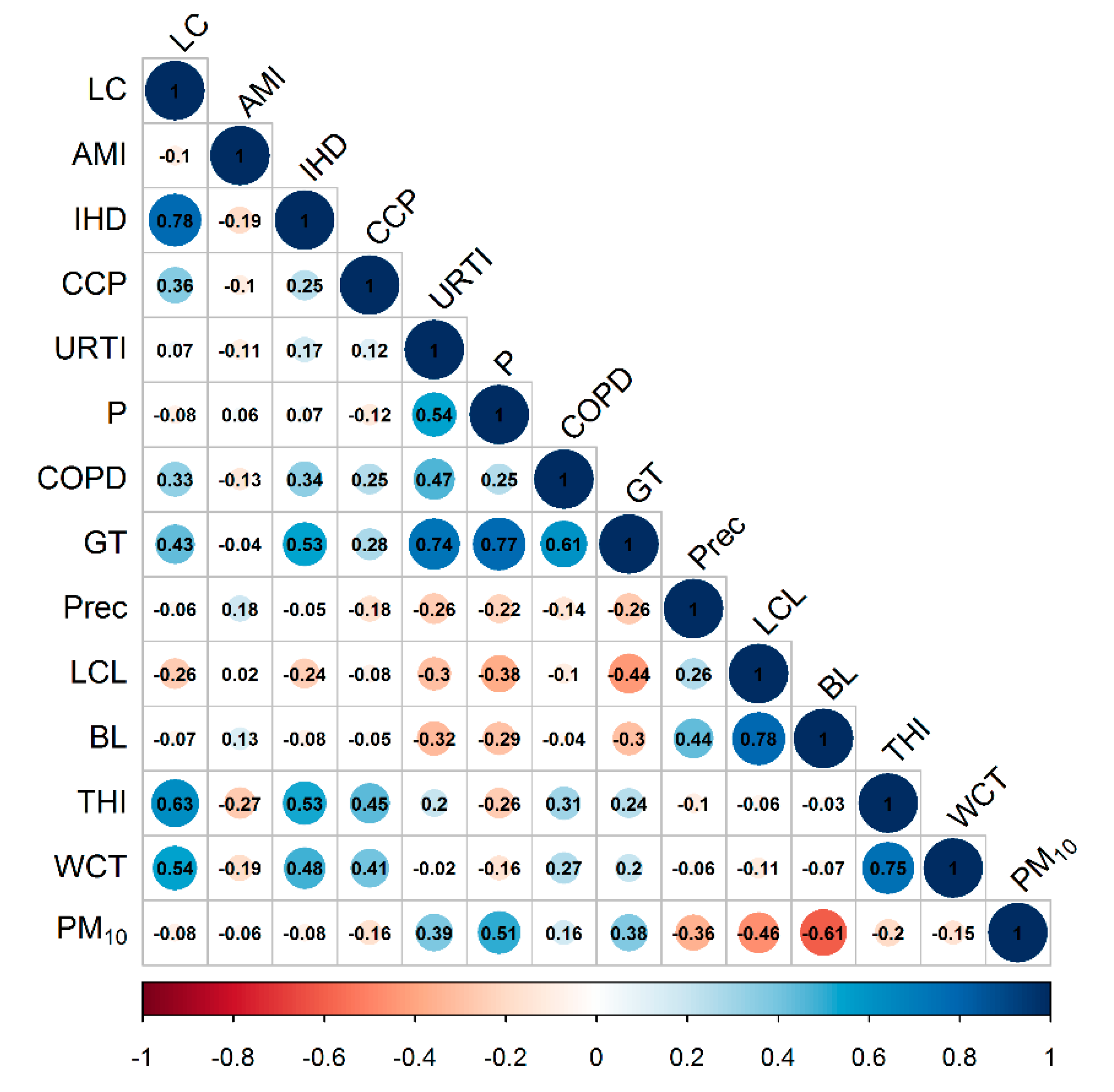
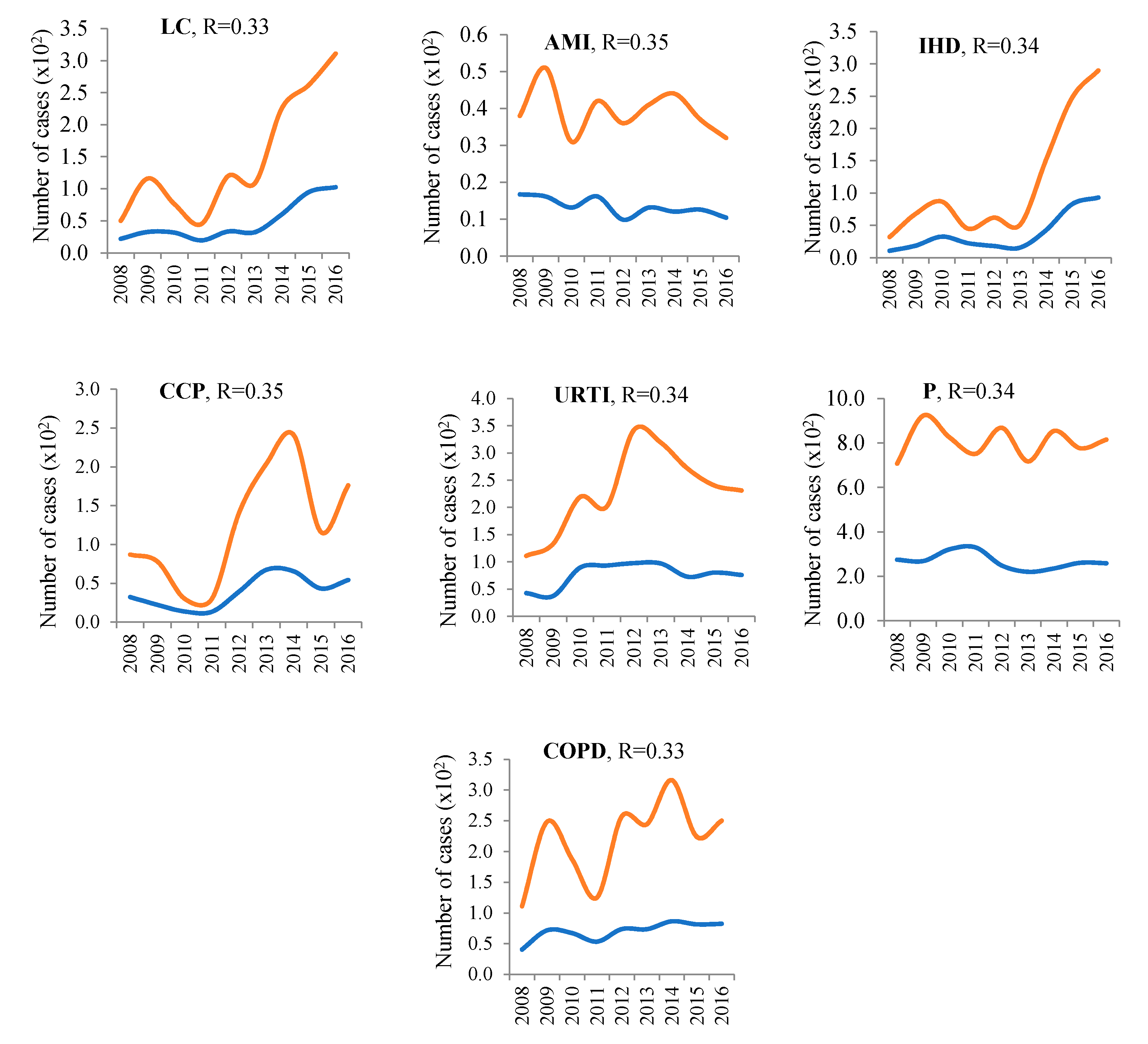
3.6. Correlation Analysis
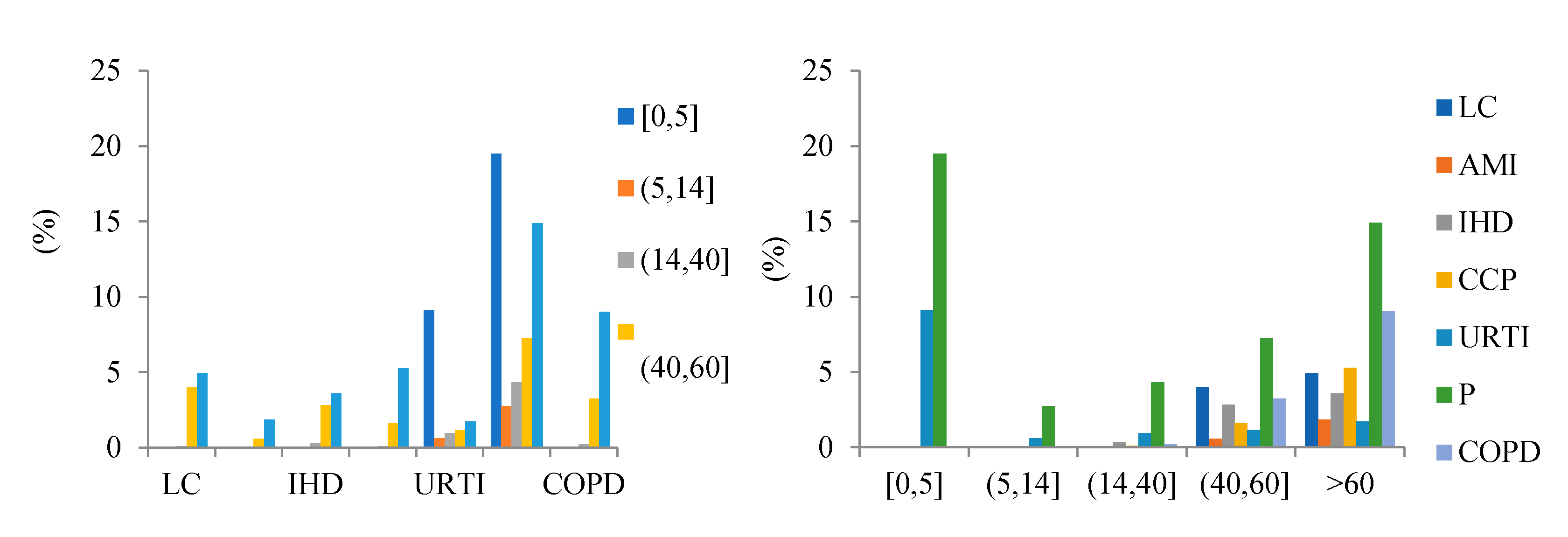
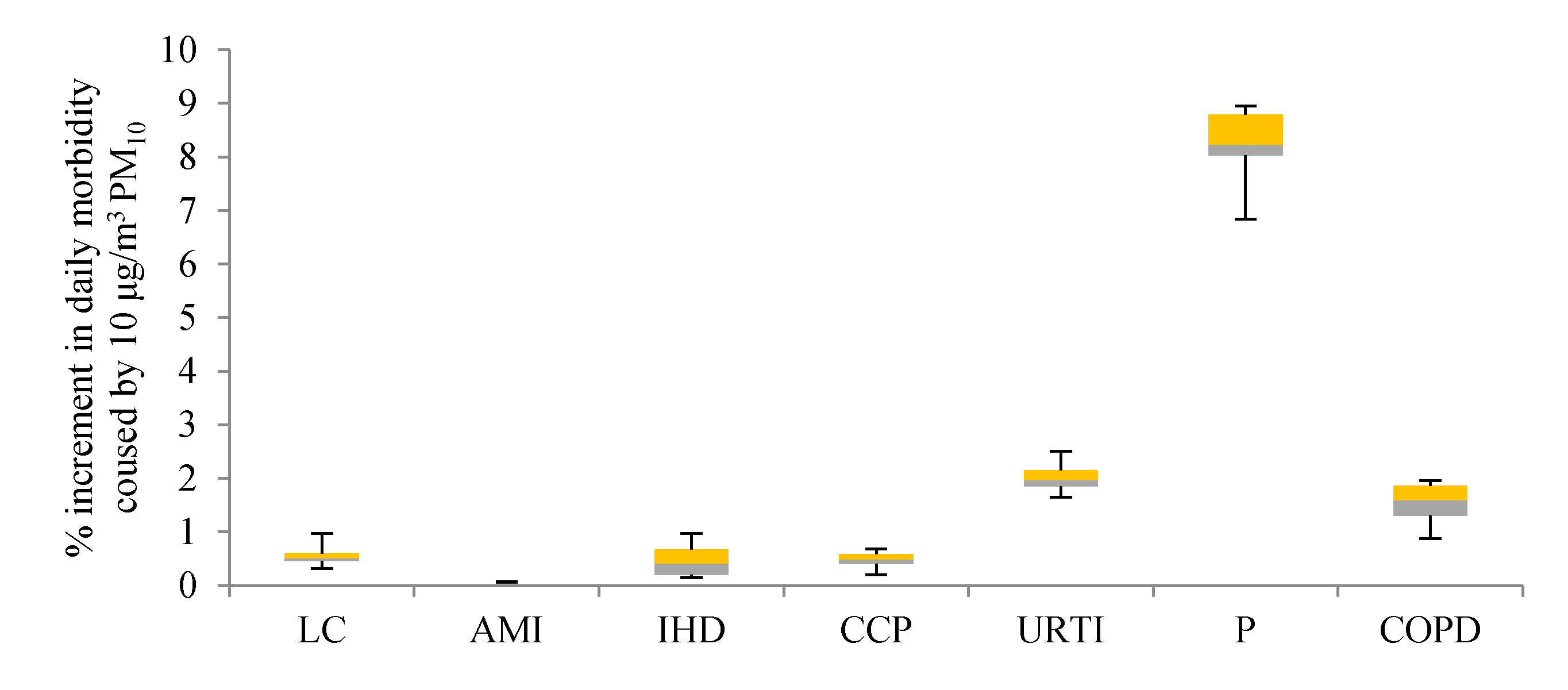
3.7. Morbidity Increase Due to a 10 μg/m3 Rise in PM10
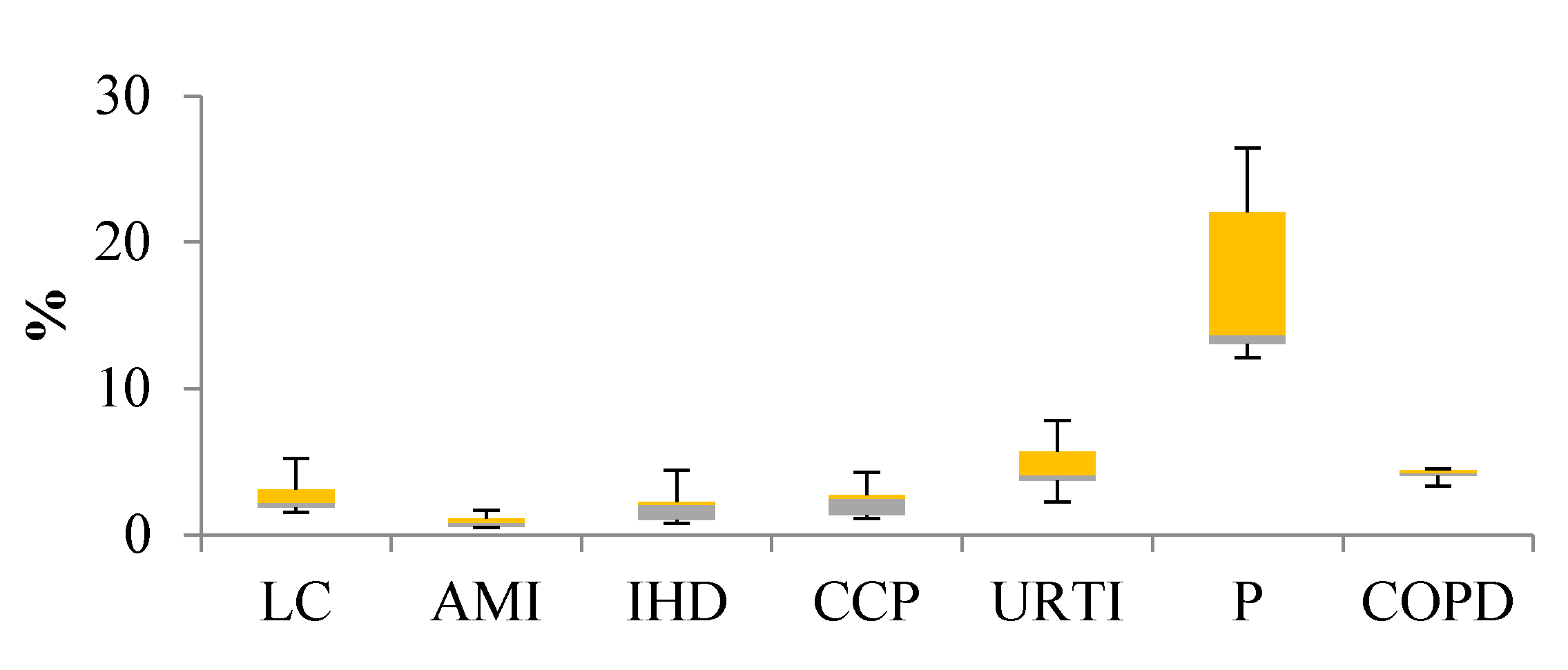
3.8. Theoretical Calculation of Hospital Admissions
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prüss-Ustün, A.; Wolf, J.; Corvalán, C.; Bos, R.; Neira, M. Global Burden of Diseases from Environmental Riks. World Health Organ. 2016, 1522. [Google Scholar] [CrossRef]
- Peacock, J.L.; Ross Anderson, H.; Bremner, S.A.; Marston, L.; Seemungal, T.A.; Strachan, D.P.; Wedzicha, J.A. Outdoor air pollution and respiratory health in patients with COPD. Thorax 2011, 66, 591–596. [Google Scholar] [CrossRef] [Green Version]
- Künzli, N.; Ackermann-Liebrich, U.; Brändli, O.; Tschopp, J.M.; Schindler, C.; Leuenberger, P. Clinically “small” effects of air pollution on FVC have a large public health impact. Eur. Respir. J. 2000, 15, 131–136. [Google Scholar] [CrossRef]
- Mariani, E.; Bonati, E.; Veronesi, L.; Colucci, M.; Zanelli, R.; Sansebastiano, G.; Olivieri, D.; Marangio, E. Respiratory function in subjects with chronic obstructive pulmonary disease (COPD) and atmospheric pollution in the city of parma. preliminary analysis. Acta Biomed. 2010, 81, 109–114. [Google Scholar] [PubMed]
- Lagorio, S.; Forastiere, F.; Pistelli, R.; Iavarone, I.; Michelozzi, P.; Fano, V.; Marconi, A.; Ziemacki, G.; Ostro, B.D. Air pollution and lung function among susceptible adult subjects: A panel study. Environ. Health A Glob. Access Sci. Source 2006, 5. [Google Scholar] [CrossRef] [Green Version]
- Brunekreef, B.; Dockery, D.W.; Krzyzanowski, M. Epidemiologic Studies on Short-Term Effects of Low Levels of Major Ambient Air Pollution Components. Environ. Health Perspect. 1986, 103 (Suppl. 2), 3–13. [Google Scholar]
- Consonni, D.; Carugno, M.; De Matteis, S.; Nordio, F.; Randi, G.; Bazzano, M.; Caporaso, N.E.; Tucker, M.A.; Bertazzi, P.A.; Pesatori, A.C.; et al. Outdoor particulate matter (PM10) exposure and lung cancer risk in the EAGLE study. PLoS ONE 2018, 13, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Micheu, M.M.; Birsan, M.V.; Szép, R.; Keresztesi, Á.; Nita, I.A. From air pollution to cardiovascular diseases: The emerging role of epigenetics. Mol. Biol. Rep. 2020, 47, 5559–5567. [Google Scholar] [CrossRef]
- Polichetti, G.; Cocco, S.; Spinali, A.; Trimarco, V.; Nunziata, A. Effects of particulate matter (PM10, PM2.5 and PM1) on the cardiovascular system. Toxicology 2009, 261, 1–8. [Google Scholar] [CrossRef]
- Kannel, W.B.; D’Agostino, R.B.; Sullivan, L.; Wilson, P.W.F. Concept and usefulness of cardiovascular risk profiles. Am. Heart J. 2004. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Xu, X.; Chu, M.; Guo, Y.; Wang, J. Air particulate matter and cardiovascular disease: The epidemiological, biomedical and clinical evidence. J. Thorac. Dis. 2016, 8, E8–E19. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate Matter Air Pollution and Cardiovascular Disease. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [Green Version]
- Jo, E.J.; Lee, W.S.; Jo, H.Y.; Kim, C.H.; Eom, J.S.; Mok, J.H.; Kim, M.H.; Lee, K.; Kim, K.U.; Lee, M.K.; et al. Effects of particulate matter on respiratory disease and the impact of meteorological factors in Busan, Korea. Respir. Med. 2017, 124, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Newell, K.; Kartsonaki, C.; Lam, K.B.H.; Kurmi, O.P. Cardiorespiratory health effects of particulate ambient air pollution exposure in low-income and middle-income countries: A systematic review and meta-analysis. Lancet Planet. Health 2017, 1, e360–e367. [Google Scholar] [CrossRef] [Green Version]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Foad, A.-A. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- Micheu, M.M.; Birsan, M.V.; Nita, I.A.; Andrei, M.D.; Nebunu, D.; Acatrinei, C.; Sfîcă, L.; Szép, R.; Keresztesi, Á.; F-dez de Arróyabe, P.; et al. Influence of meteorological variables on people with cardiovascular diseases in Bucharest (2011–2012). Rom. Rep. Phys. 2020, 73, 107. [Google Scholar]
- Krewski, D.; Jerrett, M.; Richard, T.B.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Pope, C.A., III; Turson, G.; Calle, E.E.; et al. Extended Follow-Up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality; Health Effects Institute: Boston, MA, USA, 1991. [Google Scholar]
- Dominici, F.; McDermott, A.; Daniels, M.; Zeger, S.L.; Samet, J.M. Revised analyses of the national morbidity, mortality, and air pollution study: Mortality among residents of 90 cities. J. Toxicol. Environ. Health Part A 2005, 68, 1071–1092. [Google Scholar] [CrossRef]
- Samoli, E.; Peng, R.; Ramsay, T.; Pipikou, M.; Touloumi, G.; Dominici, F.; Burnett, R.; Cohen, A.; Krewski, D.; Samet, J.; et al. Acute effects of ambient particulate matter on mortality in Europe and North America: Results from the APHENA study. Environ. Health Perspect. 2008, 116, 1480–1486. [Google Scholar] [CrossRef] [Green Version]
- Pascal, M.; Corso, M.; Chanel, O.; Declercq, C.; Badaloni, C.; Cesaroni, G.; Henschel, S.; Meister, K.; Haluza, D.; Martin-Olmedo, P.; et al. Assessing the public health impacts of urban air pollution in 25 European cities: Results of the Aphekom project. Sci. Total Environ. 2013, 449, 390–400. [Google Scholar] [CrossRef]
- Beelen, R.; Raaschou-Nielsen, O.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.; Nieuwenhuijsen, M.; et al. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 2014, 383, 785–795. [Google Scholar] [CrossRef]
- Dehbi, H.M.; Blangiardo, M.; Gulliver, J.; Fecht, D.; de Hoogh, K.; Al-Kanaani, Z.; Tillin, T.; Hardy, R.; Chaturvedi, N.; Hansell, A.L. Air pollution and cardiovascular mortality with over 25 years follow-up: A combined analysis of two British cohorts. Environ. Int. 2017, 99, 275–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandini, M.; Scarinzi, C.; Bande, S.; Berti, G.; Carnà, P.; Ciancarella, L.; Costa, G.; Demaria, M.; Ghigo, S.; Piersanti, A.; et al. Long term effect of air pollution on incident hospital admissions: Results from the Italian Longitudinal Study within LIFE MED HISS project. Environ. Int. 2018, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Qian, D.; Yan, W.; Zanobetti, A.; Wang, Y.; Koutrakis, P.; Choirat, C.; Dominici, F.; Schwartz, J.D. Air pollution and mortality in the medicare population. J. Am. Med. Assoc. 2018, 319, 2135. [Google Scholar] [CrossRef]
- Available online: berkeleyearth.org (accessed on 18 February 2021).
- Xing, Y.F.; Xu, Y.H.; Shi, M.H.; Lian, Y.X. The impact of PM2.5 on the human respiratory system. J. Thorac. Dis. 2016, 8, E69–E74. [Google Scholar] [CrossRef] [PubMed]
- Leitte, A.M.; Petrescu, C.; Franck, U.; Richter, M.; Suciu, O.; Ionovici, R.; Herbarth, O.; Schlink, U. Respiratory health, effects of ambient air pollution and its modification by air humidity in Drobeta-Turnu Severin, Romania. Sci. Total Environ. 2009, 407, 4004–4011. [Google Scholar] [CrossRef]
- Szép, R.; Mateescu, E.; Nechifor, C.; Keresztesi, Á. Chemical characteristics and source analysis on ionic composition of rainwater collected in the Carpathians “Cold Pole,” Ciuc basin, Eastern Carpathians, Romania. Environ. Sci. Pollut. Res. 2017, 24, 27288–27302. [Google Scholar] [CrossRef] [PubMed]
- Szép, R.; Bodor, Z.; Miklóssy, I.; Niță, I.A.; Oprea, O.A.; Keresztesi, Á. Influence of peat fires on the rainwater chemistry in intra-mountain basins with specific atmospheric circulations (Eastern Carpathians, Romania). Sci. Total Environ. 2019, 647, 275–289. [Google Scholar] [CrossRef]
- Hersbach, H.; Bell, B.; Berrisford, P.; Hirahara, S.; Horányi, A.; Muñoz-Sabater, J.; Nicolas, J.; Peubey, C.; Radu, R.; Schepers, D.; et al. The ERA5 global reanalysis. Q. J. R. Meteorol. Soc. 2020, 146, 1999–2049. [Google Scholar] [CrossRef]
- Available online: https://rda.ucar.edu/datasets/ds630.0/. (accessed on 18 February 2021).
- Dobrinescu, A.; Busuioc, A.; Birsan, M.V.; Dumitrescu, A.; Orzan, A. Changes in thermal discomfort indices in Romania and their connections with large-scale mechanisms. Clim. Res. 2015, 64, 213–226. [Google Scholar] [CrossRef]
- Osgood, B. The Fourier Transform and its Applications—Lecture Notes. Electr. Eng. Dep. Stanf. Univ. 2010, 186–188. [Google Scholar]
- Ribeiro, K.M.; Júnior, R.A.B.; Sáfadi, T.; Horgan, G. Comparison between Fourier and Wavelets Transforms in Biospeckle Signals. Appl. Math. 2013, 4, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Aunan, K. Exposure-response functions for health effects of air pollutants based on epidemiological findings. Risk Anal. 1996, 16, 693–709. [Google Scholar] [CrossRef]
- Tan, P.; Chou, C.; Liang, J.; Chou, C.C.; Shiu, C. Air pollution “holiday effect” resulting from the Chinese New Year. Atmos. Environ. 2009, 43, 2114–2124. [Google Scholar] [CrossRef]
- Colvez, A.; Castex, A.; Carriere, I. WHO Air quality guidelines for particulate matter, ozone, nitrogen. Rev. Epidemiol. Sante Publique 2003, 51, 565–573. [Google Scholar] [CrossRef]
- Anenberg, S.C.; Belova, A.; Brandt, J.; Fann, N.; Greco, S.; Guttikunda, S.; Heroux, M.E.; Hurley, F.; Krzyzanowski, M.; Medina, S.; et al. Survey of Ambient Air Pollution Health Risk Assessment Tools. Risk Anal. 2016, 36, 1718–1736. [Google Scholar] [CrossRef]
- Li, Y.; Henze, D.K.; Jack, D.; Henderson, B.H.; Kinney, P.L. Assessing public health burden associated with exposure to ambient black carbon in the United States. Sci. Total Environ. 2016, 539, 515–525. [Google Scholar] [CrossRef] [Green Version]
- Hassanvand, M.S.; Naddafi, K.; Kashani, H.; Faridi, S.; Kunzli, N.; Nabizadeh, R.; Momeniha, F.; Gholampour, A.; Arhami, M.; Zare, A.; et al. Short-term effects of particle size fractions on circulating biomarkers of inflammation in a panel of elderly subjects and healthy young adults. Environ. Pollut. 2017, 223, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Zhang, A.; Liang, S.; Qi, Q.; Jiang, L.; Ye, Y. The association between air pollution and population health risk for respiratory infection: A case study of Shenzhen, China. Int. J. Environ. Res. Public Health 2017, 14, 950. [Google Scholar] [CrossRef] [Green Version]
- Adar, S.D.; Filigrana, P.A.; Clements, N.; Peel, J.L. Ambient Coarse Particulate Matter and Human Health: A Systematic Review and Meta-Analysis. Curr. Environ. Health Rep. 2014, 1, 258–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The mechanisms of air pollution and particulate matter in cardiovascular diseases. Heart Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Shaw, C.A.; Langrish, J.P. From particles to patients: Oxidative stress and the cardiovascular effects of air pollution. Future Cardiol. 2012, 8, 577–602. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.R.; Xiao, C.C.; Li, J.; Tang, J.; Geng, X.Y.; Cui, L.J.; Zhai, J.X. Association between air pollution and upper respiratory tract infection in hospital outpatients aged 0 e 14 years in Hefei, China: A time series study. Public Health 2017, 6. [Google Scholar] [CrossRef]
- Hamanaka, R.B.; Mutlu, G.M. Particulate Matter Air Pollution: Effects on the Cardiovascular System. Front. Endocrinol. Lausanne 2018, 9, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheol Kim, H.; Kim, E.; Bae, C.; Hoon Cho, J.; Kim, B.U.; Kim, S. Regional contributions to particulate matter concentration in the Seoul metropolitan area, South Korea: Seasonal variation and sensitivity to meteorology and emissions inventory. Atmos. Chem. Phys. 2017, 17, 10315–10332. [Google Scholar] [CrossRef] [Green Version]
- Mohtar, A.A.A.; Latif, M.T.; Baharudin, N.H.; Ahamad, F.; Chung, J.X.; Othman, M.; Juneng, L. Variation of major air pollutants in different seasonal conditions in an urban environment in Malaysia. Geosci. Lett. 2018, 5, 21. [Google Scholar] [CrossRef]
- Aikawa, M.; Kajino, M.; Hiraki, T.; Mukai, H. The contribution of site to washout and rainout: Precipitation chemistry based on sample analysis from 0.5mm precipitation increments and numerical simulation. Atmos. Environ. 2014, 95, 165–174. [Google Scholar] [CrossRef]
- Ghanizadeh, G.; Heidari, M.; Seifi, B.; Jafari, H.; Pakjouei, S. The Effect of Climate Change on Cardiopulmonary Disease—A Systematic Review. J. Clin. Diagn. Res. 2017, 1–4. [Google Scholar] [CrossRef]
- Zhang, Q.; Qi, W.; Yao, W.; Wang, M.; Chen, Y.; Zhou, Y. Ambient Particulate Matter (PM 2.5/PM 10) Exposure and Emergency Department Visits for Acute Myocardial Infarction in Chaoyang District, Beijing, China During 2014: A Case-Crossover Study. J. Epidemiol. 2016, 26, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Brunekreef, B.; Forsberg, B. Epidemiological evidence of effects of coarse airborne particles on health. Eur. Respir. J. 2005, 26, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Zhuang, G.; Tang, A.; Wang, Y.; An, Z. Chemical Characteristics of PM2.5 and PM10 in Haze—Fog Episodes in Beijing. Env. Sci. Technol. 2006, 40, 3148–3155. [Google Scholar] [CrossRef]
- Song, Q.; Christiani, D.C.; Wang, X.; Ren, J. The global contribution of outdoor air pollution to the incidence, prevalence, mortality and hospital admission for chronic obstructive pulmonary disease: A systematic review and meta-analysis. Int. J. Env. Res. Public Health 2014, 11, 11822–11832. [Google Scholar] [CrossRef] [Green Version]
- Lipsett, M.J.; Ostro, B.D.; Reynolds, P.; Goldberg, D.; Hertz, A.; Jerrett, M.; Smith, D.F.; Garcia, C.; Chang, E.T.; Bernstein, L. California Long-term exposure to air pollution and cardiorespiratory disease in the California teachers study cohort. Am. J. Respir. Crit. Care Med. 2011, 184, 828–835. [Google Scholar] [CrossRef]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; De Faire, U.; Erbel, R.; Eriksen, K.T.; et al. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 european cohorts from the escape project. BMJ 2014, 348. [Google Scholar] [CrossRef] [Green Version]
- Hart, J.E.; Puett, R.C.; Rexrode, K.M.; Albert, C.M.; Laden, F. Effect modification of long-term air pollution exposures and the risk of incident cardiovascular disease in US women. J. Am. Heart Assoc. 2015, 4, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, Y.; Hodgson, S.; Blangiardo, M.; Gulliver, J.; Morley, D.; Fecht, D.; Vienneau, D.; de Hoogh, K.; Key, T.; Hveem, K.; et al. Road traffic noise, air pollution and incident cardiovascular disease: A joint analysis of the HUNT, EPIC-Oxford and UK Biobank cohorts. Environ. Int. 2018, 114, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Li, H.; Wang, S.; Van Halm-Lutterodt, N.; An, J.; Liu, Y.; Liu, M.; Wang, X.; Guo, X. Short-term PM10 and emergency department admissions for selective cardiovascular and respiratory diseases in Beijing, China. Sci. Total Environ. 2019, 657, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Viegi, G.; Maio, S.; Simoni, M.; Baldacci, S.; Annesi-Maesano, I. The epidemiological link between ageing and respiratory diseases. Eur. Respir. Soc. Monogr. 2009, 43, 1–17. [Google Scholar]
- Eckel, S.P.; Louis, T.A.; Chaves, P.H.M.; Fried, L.P.; Margolis, A.H.G. Modification of the association between ambient air pollution and lung function by frailty status among older adults in the cardiovascular health study. Am. J. Epidemiol. 2012, 176, 214–223. [Google Scholar] [CrossRef] [Green Version]
- Simoni, M.; Baldacci, S.; Maio, S.; Cerrai, S.; Sarno, G.; Viegi, G. Adverse effects of outdoor pollution in the elderly. J. Thorac. Dis. 2015, 7, 34–45. [Google Scholar] [CrossRef]
- Clougherty, J.E. A growing role for gender analysis in air pollution epidemiology. Environ. Health Perspect. 2010, 118, 167–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbey, D.E.; Burchette, R.J.; Knutsen, S.F.; Mcdonnell, W.F.; Lebowitz, M.D.; Enright, P.L. Long-term particulate and other air pollutants and lung function in nonsmokers. Am. J. Respir. Crit. Care Med. 1998, 158, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Silveyra, P.; Nathalie, F.; Lidys, R. Understanding the Intersection of Environmental Pollution, Pneumonia, and Inflammation: Does Gender Play a Role? Long-Haul Travel Motiv. Int. Tour. Penang 2018, 1, 13. [Google Scholar]
- Chauhan, A.J.; Johnston, S.L. Air pollution and infection in respiratory illness. Br. Med. Bull. 2003, 68, 95–112. [Google Scholar] [CrossRef]
- Darrow, L.A.; Klein, M.; Dana Flanders, W.; Mulholland, J.A.; Tolbert, P.E.; Strickland, M.J. Air pollution and acute respiratory infections among children 0–4 years of age: An 18-year time-series study. Am. J. Epidemiol. 2014, 180, 968–977. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, N.; Junger, W.L.; Romieu, I.; Cifuentes, L.A.; de Leon, A.P.; Vera, J.; Strappa, V.; Hurtado-Díaz, M.; Miranda-Soberanis, V.; Rojas-Bracho, L.; et al. Effects of air pollution on infant and children respiratory mortality in four large Latin-American cities. Env. Pollut. 2018, 232, 385–391. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, E.A.; Gehring, U.; Mölter, A.; Fuertes, E.; Klümper, C.; Krämer, U.; Quass, U.; Hoffmann, B.; Gascon, M.; Brunekreef, B.; et al. Air pollution and respiratory infections during early childhood: An analysis of 10 European birth cohorts within the ESCAPE project. Environ. Health Perspect. 2014, 122, 107–113. [Google Scholar] [CrossRef]
- Trasande, L.; Thurston, G.D. The role of air pollution in asthma and other pediatric morbidities. J. Allergy Clin. Immunol. 2005, 115, 689–699. [Google Scholar] [CrossRef]
- Saadeh, R.; Klaunig, J. Children’s Inter-Individual Variability and Asthma Development. Int. J. Health Sci. 2015, 9. [Google Scholar] [CrossRef]
- Maheswaran, R.; Pearson, T.; Smeeton, N.C.; Beevers, S.D.; Campbell, M.J.; Wolfe, C.D. Outdoor Air Pollution and Incidence of Ischemic and Hemorrhagic Stroke A Small-Area Level. Ecol. Study. 2011, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Sunyer, J. Lung function effects of chronic exposure to air pollution Can traffic-related air pollution cause asthma? BMJ 2009. [Google Scholar] [CrossRef] [Green Version]
- Sacco, R.L.; Roth, G.A.; Reddy, K.S.; Arnett, D.K.; Bonita, R.; Gaziano, T.A.; Heidenreich, P.A.; Huffman, M.D.; Mayosi, B.M.; Mendis, S.; et al. The Heart of 25 by 25: Achieving the Goal of Reducing Global and Regional Premature Deaths from Cardiovascular Diseases and Stroke: A Modeling Study from the American Heart Association and World Heart Federation. Circulation 2016, 133, e674–e690. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of Diseases | Mean + SD | CV | Min | P(25) | P(50) | P(75) | Max | CI95− | CI95+ |
|---|---|---|---|---|---|---|---|---|---|
| LC | 0.48 ± 0.34 | 0.70 | 0.03 | 0.21 | 0.39 | 0.68 | 1.39 | 0.42 | 0.54 |
| AMI | 0.13 ± 0.08 | 0.62 | 0.00 | 0.07 | 0.13 | 0.19 | 0.35 | 0.12 | 0.15 |
| IHD | 0.38 ± 0.33 | 0.88 | 0.00 | 0.13 | 0.23 | 0.55 | 1.35 | 0.31 | 0.44 |
| CCP | 0.39 ± 0.26 | 0.66 | 0.00 | 0.17 | 0.39 | 0.55 | 1.32 | 0.34 | 0.44 |
| URTI | 0.77 ± 0.45 | 0.58 | 0.10 | 0.45 | 0.69 | 1.03 | 2.39 | 0.69 | 0.86 |
| P | 2.71 ± 1.13 | 0.37 | 1.13 | 1.90 | 2.57 | 3.45 | 5.82 | 2.52 | 2.90 |
| COPD | 0.70 ± 0.26 | 0.37 | 0.19 | 0.51 | 0.68 | 0.84 | 1.65 | 0.66 | 0.75 |
| GT | 5.57 ± 1.65 | 0.30 | 2.74 | 4.30 | 5.41 | 6.32 | 11.82 | 5.26 | 5.88 |
| Meteo. conditions | |||||||||
| Prec ** | 49.31 ± 34.41 | 0.70 | 0.20 | 24.05 | 38.50 | 70.63 | 177.30 | 42.82 | 55.80 |
| LCL * | 462.23 ± 208.50 | 0.45 | 1.43 | 289.59 | 497.90 | 600.38 | 1000.63 | 422.91 | 501.56 |
| BL * | 428.87 ±156.49 | 0.36 | 135.78 | 278.89 | 467.57 | 549.40 | 748.20 | 399.35 | 458.38 |
| THI * | 32.33 ± 11.53 | 0.36 | −2.80 | 25.83 | 35.13 | 40.25 | 54.17 | 30.16 | 34.51 |
| WCT * | 4.95 ± 4.63 | 0.93 | −7.41 | 2.04 | 5.34 | 7.90 | 15.32 | 4.08 | 5.82 |
| PM10 | 19.00 ± 11.59 | 0.61 | 4.39 | 11.61 | 14.51 | 21.50 | 57.71 | 16.82 | 21.19 |
| PM10 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age Categories | [0–5] | (5–14] | (14–40] | (40–60] | >60 | |||||||||||||||
| W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | |
| 1. LC | * | * | * | * | * | * | * | * | ||||||||||||
| 2. AMI | * | * | * | * | * | * | ||||||||||||||
| 3. IHD | * | * | * | * | * | * | * | |||||||||||||
| 4.CCP | * | * | * | * | * | * | * | |||||||||||||
| 5. URTI | * | * | * | * | * | * | * | * | * | * | ||||||||||
| 6. P | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | |||||
| 7. COPD | * | * | * | * | * | * | * | * | ||||||||||||
| BL | ||||||||||||||||||||
| Age categories | [0–5] | (5–14] | (14–40] | (40–60] | >60 | |||||||||||||||
| W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | |
| 1. LC | * | * | * | * | * | * | ||||||||||||||
| 2. AMI | * | * | * | * | * | * | * | |||||||||||||
| 3. IHD | * | * | * | * | * | |||||||||||||||
| 4.CCP | * | * | * | * | * | * | ||||||||||||||
| 5. URTI | * | * | * | * | * | * | * | * | * | |||||||||||
| 6. P | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * |
| 7. COPD | * | * | * | * | * | * | * | * | ||||||||||||
| WCT | ||||||||||||||||||||
| Age categories | [0–5] | (5–14] | (14–40] | (40–60] | >60 | |||||||||||||||
| W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | W | Sp | Su | A | |
| 1. LC | * | * | * | * | ||||||||||||||||
| 2. AMI | * | * | * | |||||||||||||||||
| 3. IHD | * | * | ||||||||||||||||||
| 4.CCP | * | |||||||||||||||||||
| 5. URTI | * | * | * | |||||||||||||||||
| 6. P | * | * | * | * | * | * | * | |||||||||||||
| 7. COPD | * | * | * | |||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bodor, K.; Micheu, M.M.; Keresztesi, Á.; Birsan, M.-V.; Nita, I.-A.; Bodor, Z.; Petres, S.; Korodi, A.; Szép, R. Effects of PM10 and Weather on Respiratory and Cardiovascular Diseases in the Ciuc Basin (Romanian Carpathians). Atmosphere 2021, 12, 289. https://doi.org/10.3390/atmos12020289
Bodor K, Micheu MM, Keresztesi Á, Birsan M-V, Nita I-A, Bodor Z, Petres S, Korodi A, Szép R. Effects of PM10 and Weather on Respiratory and Cardiovascular Diseases in the Ciuc Basin (Romanian Carpathians). Atmosphere. 2021; 12(2):289. https://doi.org/10.3390/atmos12020289
Chicago/Turabian StyleBodor, Katalin, Miruna Mihaela Micheu, Ágnes Keresztesi, Marius-Victor Birsan, Ion-Andrei Nita, Zsolt Bodor, Sándor Petres, Attila Korodi, and Róbert Szép. 2021. "Effects of PM10 and Weather on Respiratory and Cardiovascular Diseases in the Ciuc Basin (Romanian Carpathians)" Atmosphere 12, no. 2: 289. https://doi.org/10.3390/atmos12020289
APA StyleBodor, K., Micheu, M. M., Keresztesi, Á., Birsan, M.-V., Nita, I.-A., Bodor, Z., Petres, S., Korodi, A., & Szép, R. (2021). Effects of PM10 and Weather on Respiratory and Cardiovascular Diseases in the Ciuc Basin (Romanian Carpathians). Atmosphere, 12(2), 289. https://doi.org/10.3390/atmos12020289