
Ozone-Induced Lung and Bronchial Injury: A Mouse Model Study

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Animal Exposures
2.2. Histopathological Observation
2.3. TEM Specimen Processing and Observation
2.4. Immunohistochemistry
2.5. Assays for CRP and IL-6 Levels
2.6. Statistical Analysis
3. Results
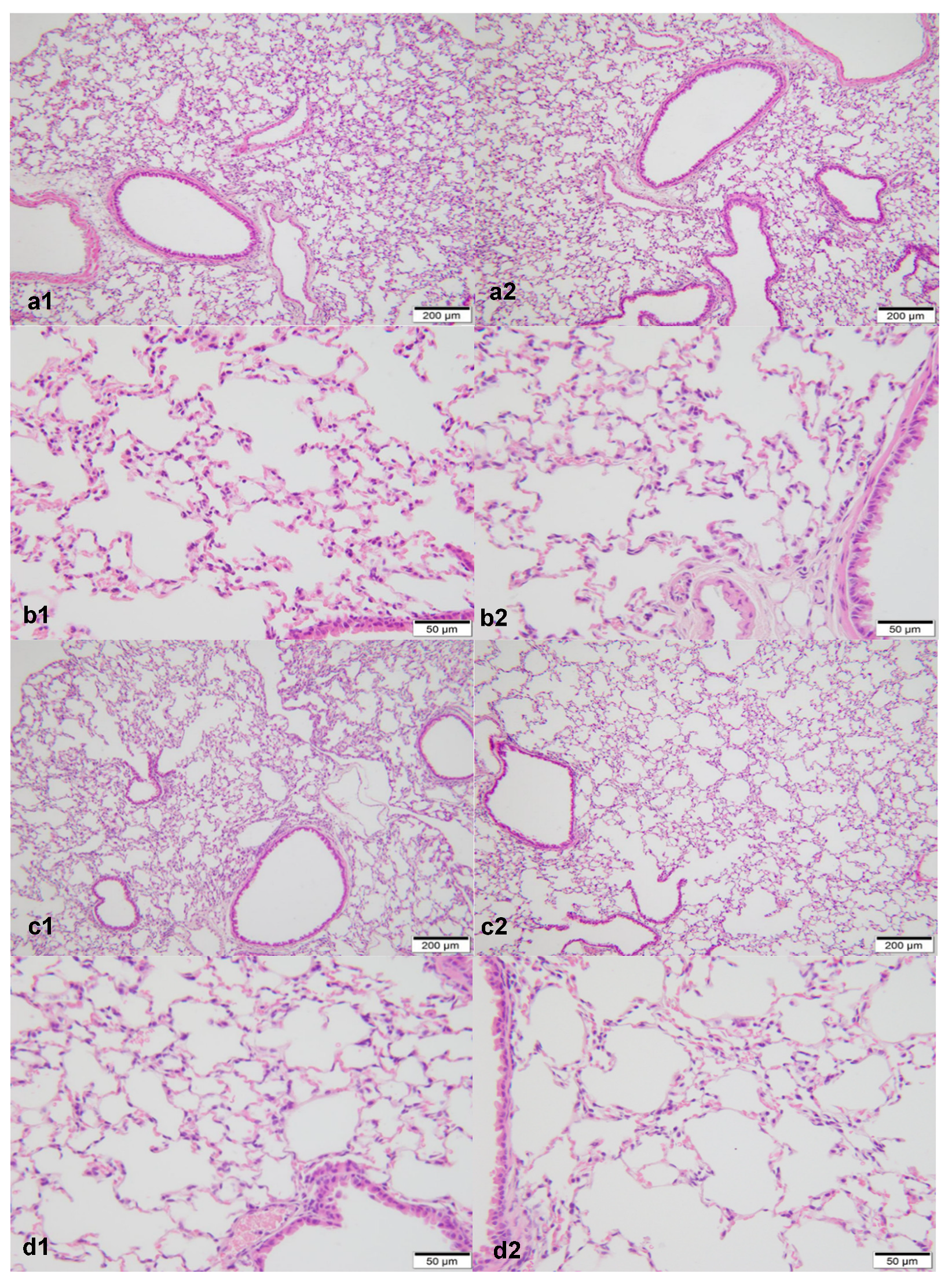
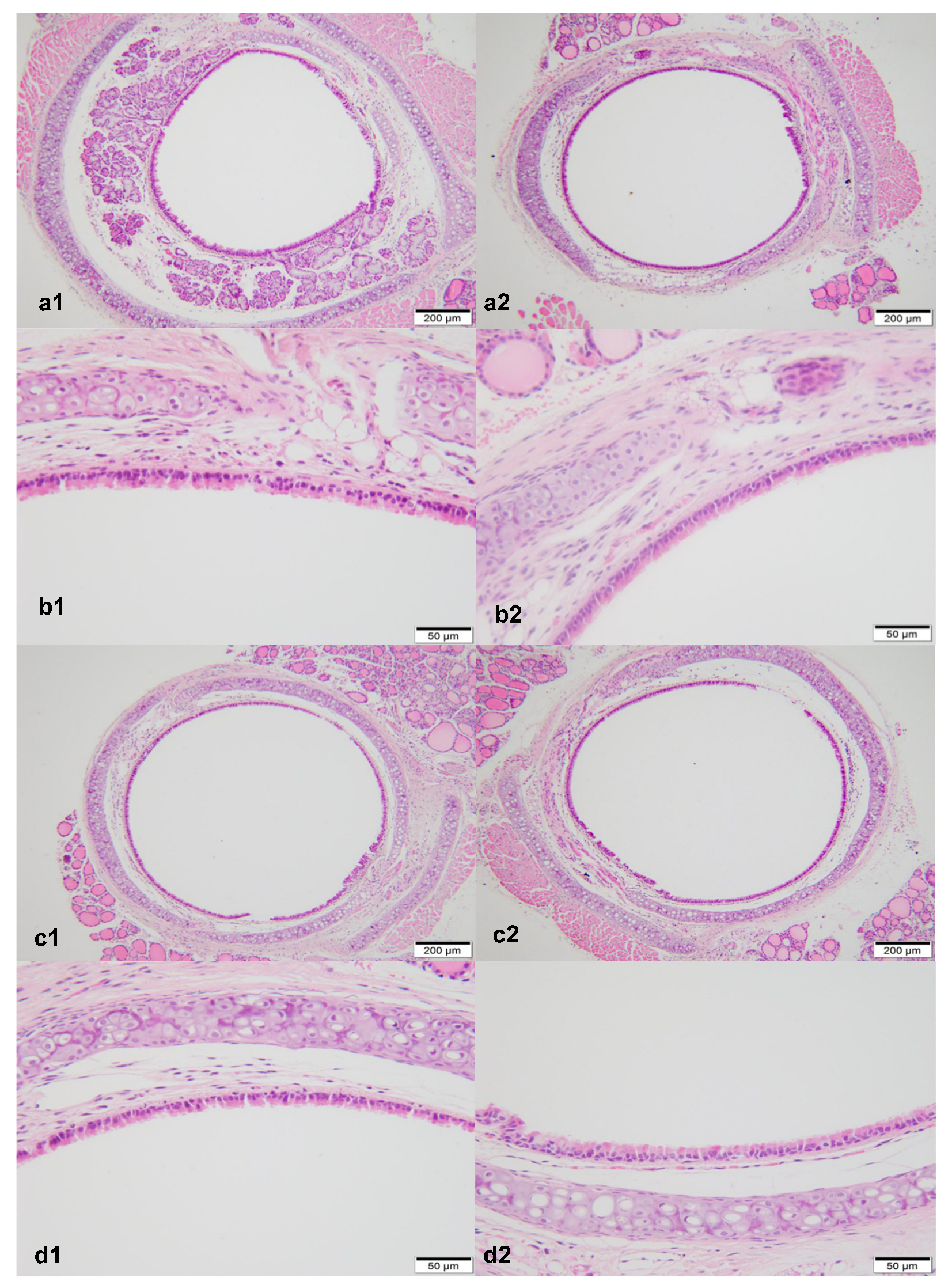
3.1. Micromorphological Observation under the Optical Microscope with HE Staining
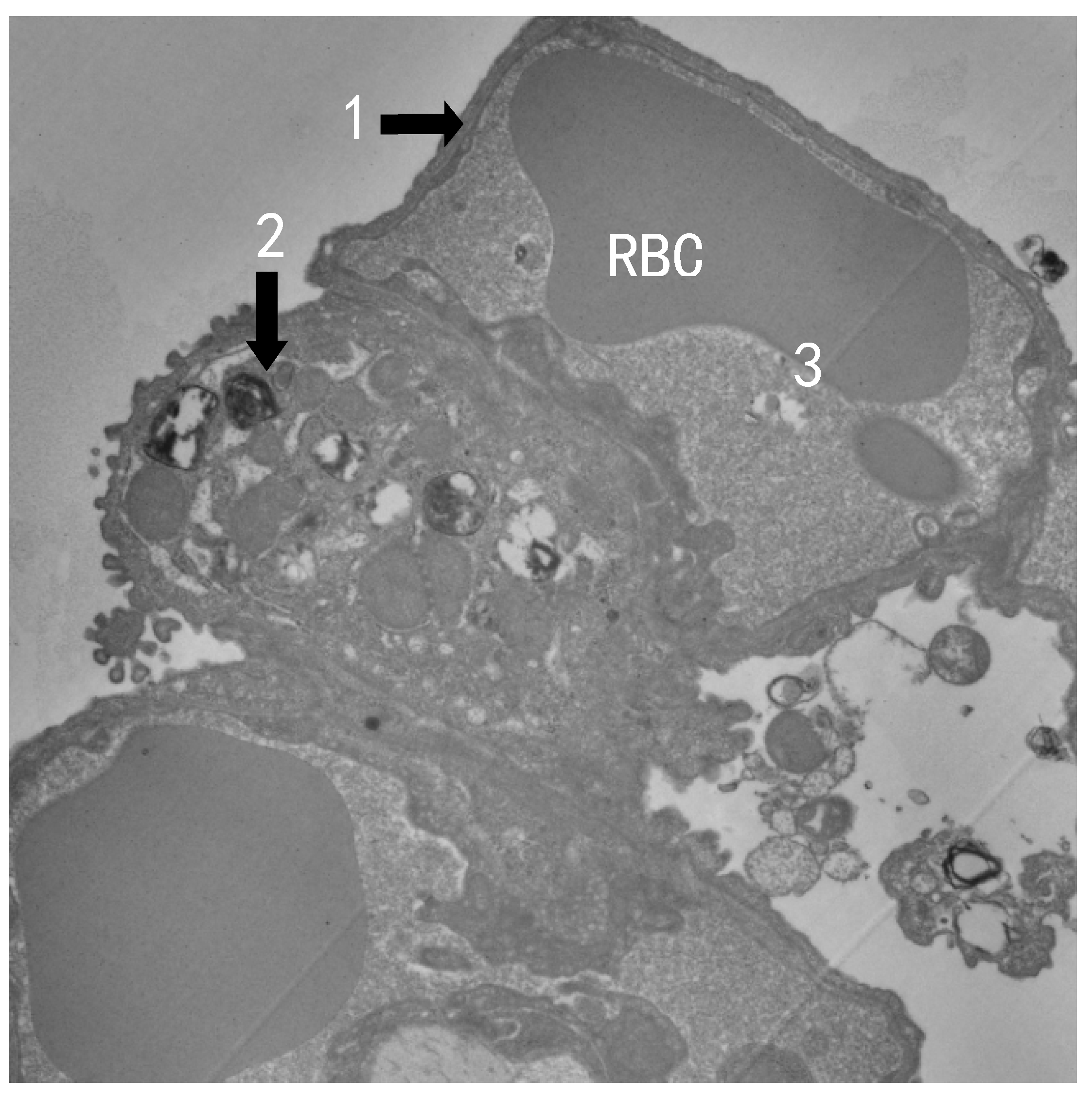
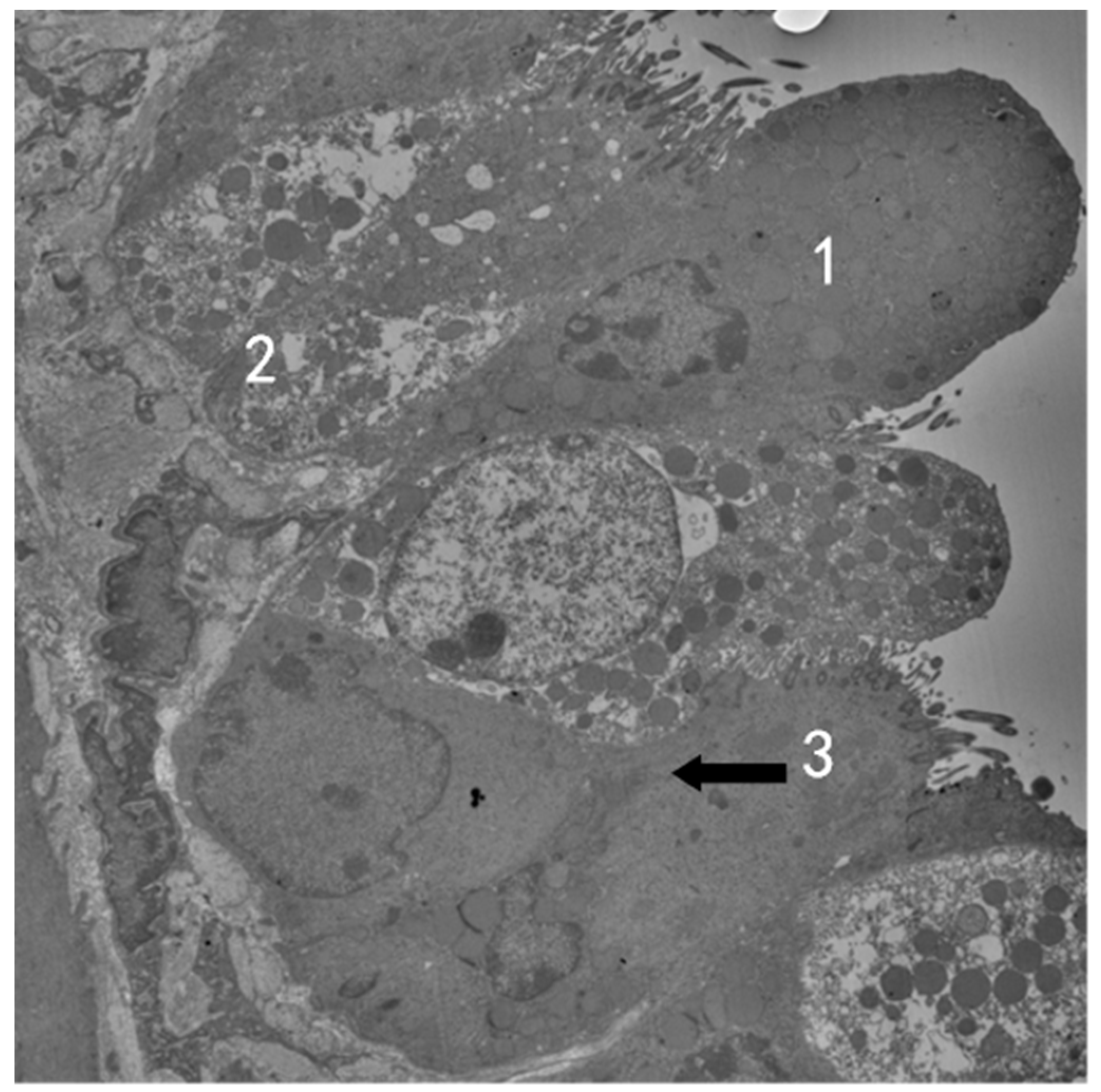
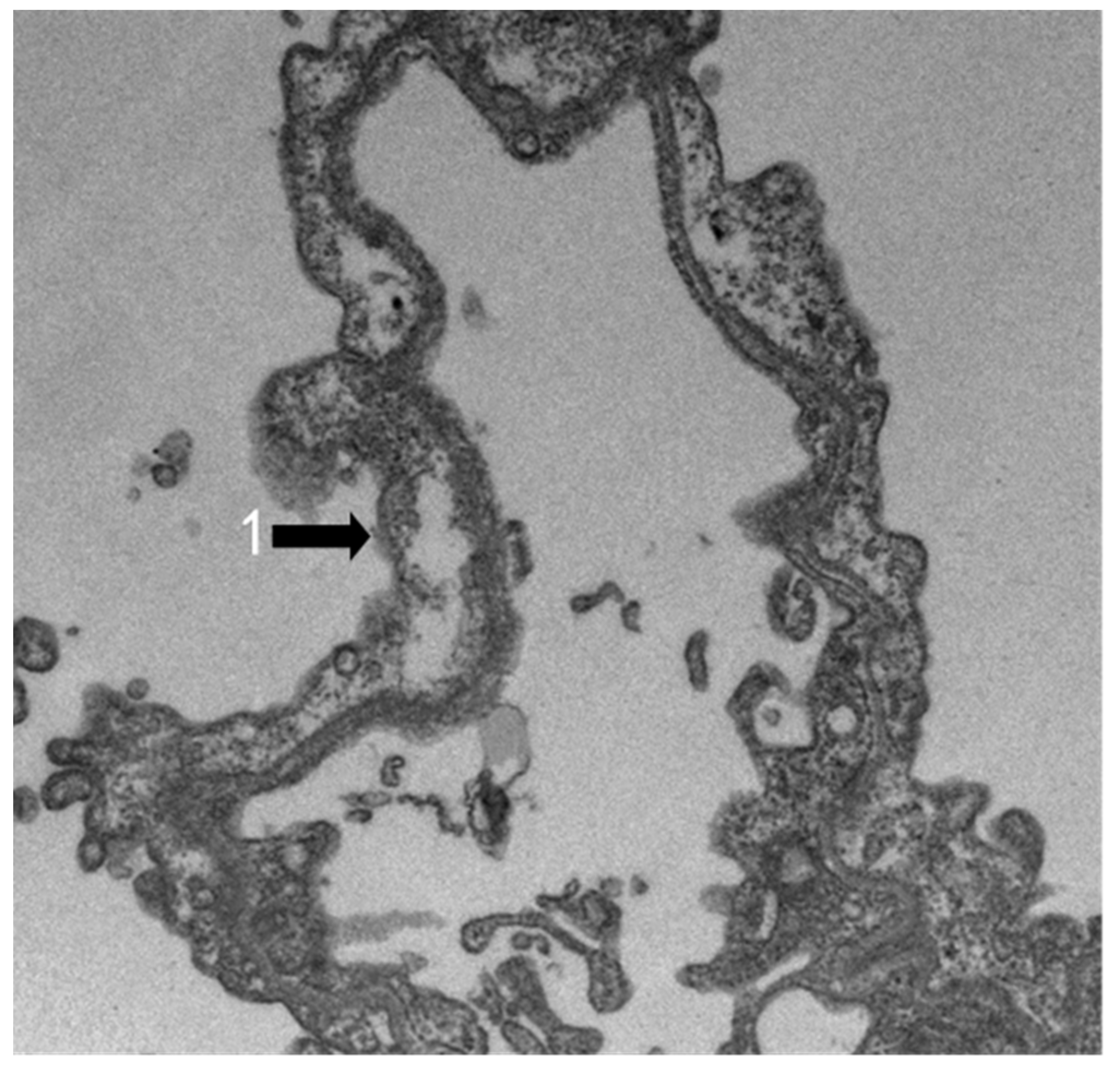
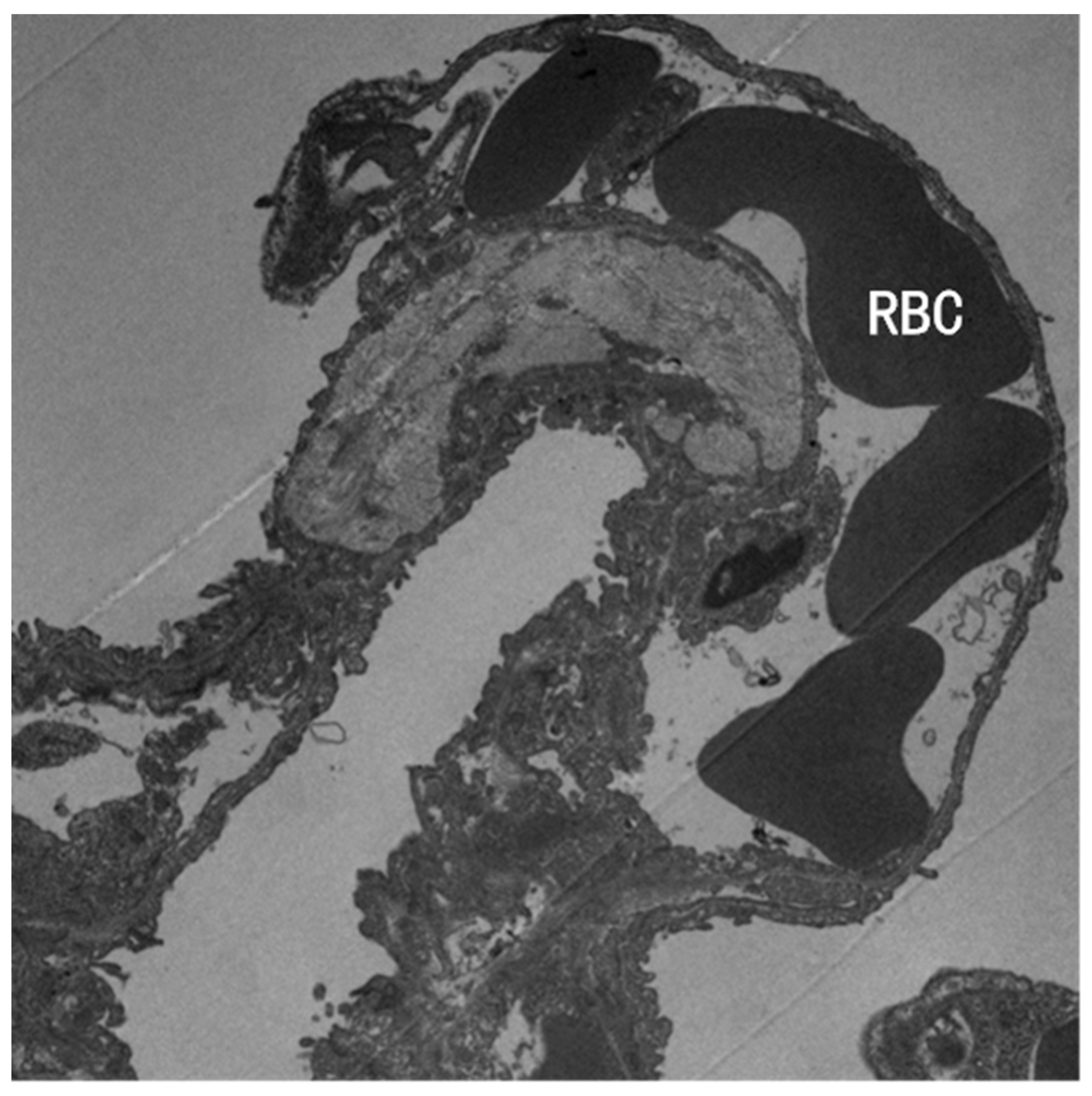
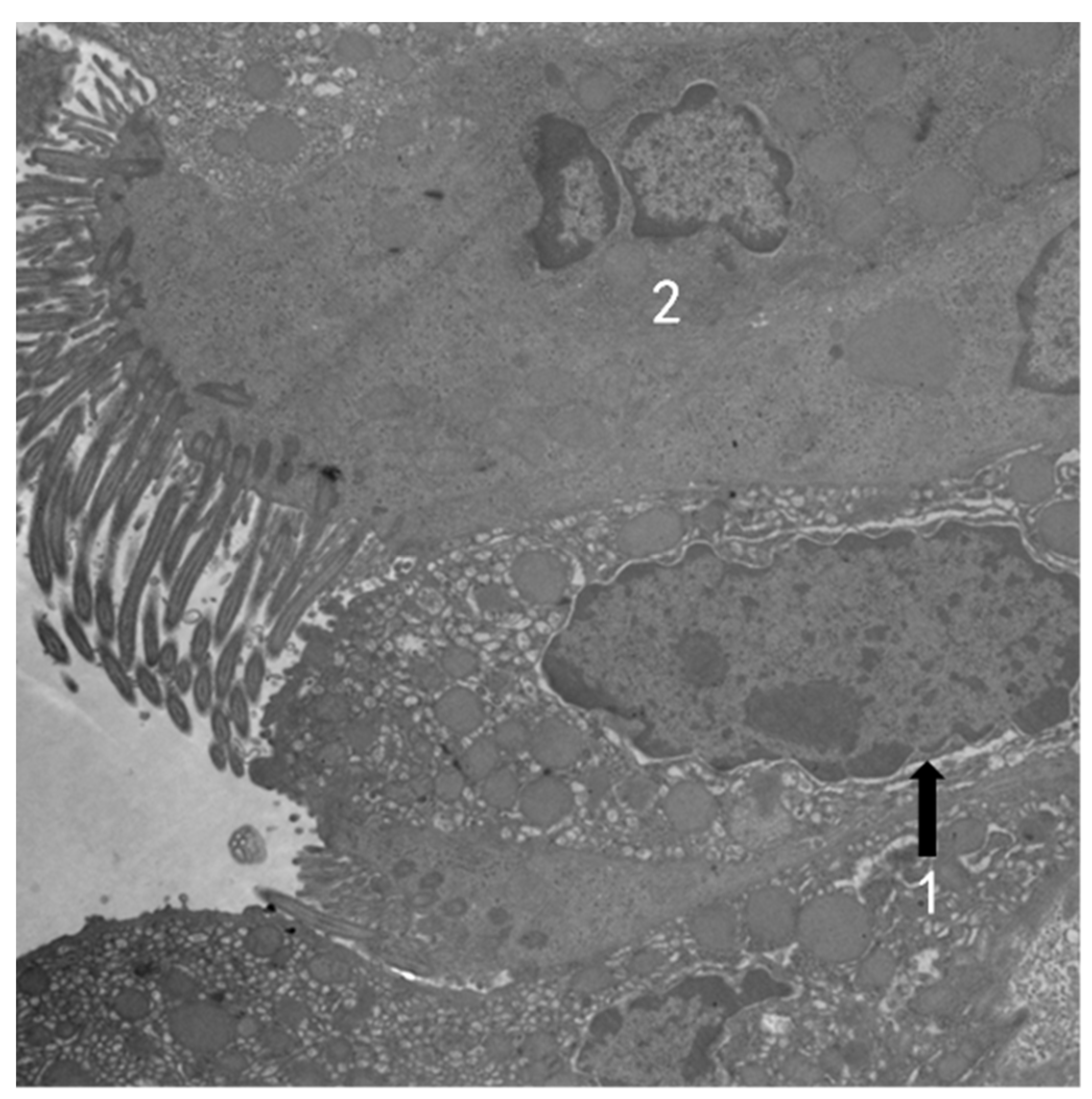
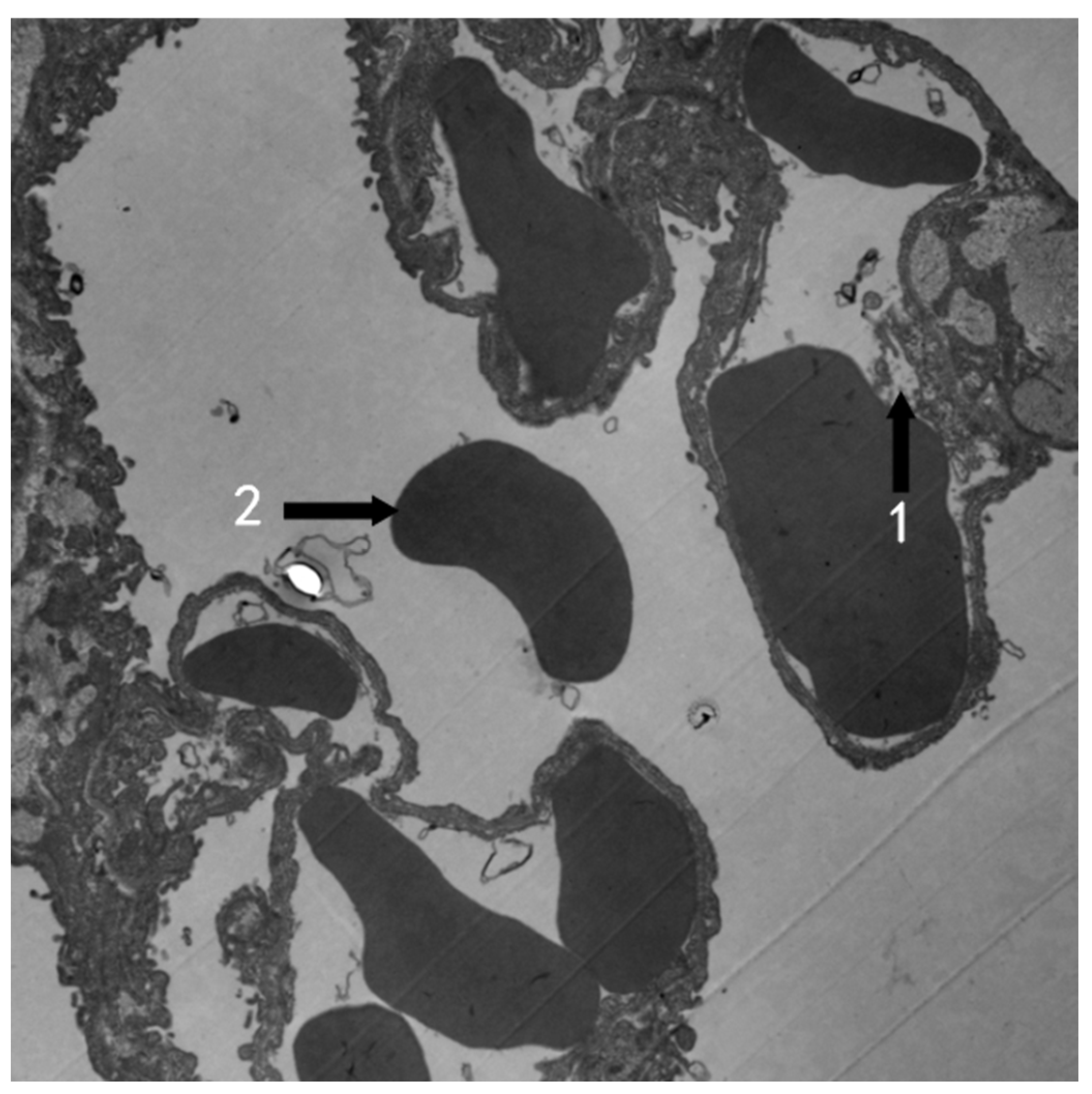
3.2. TEM Observation
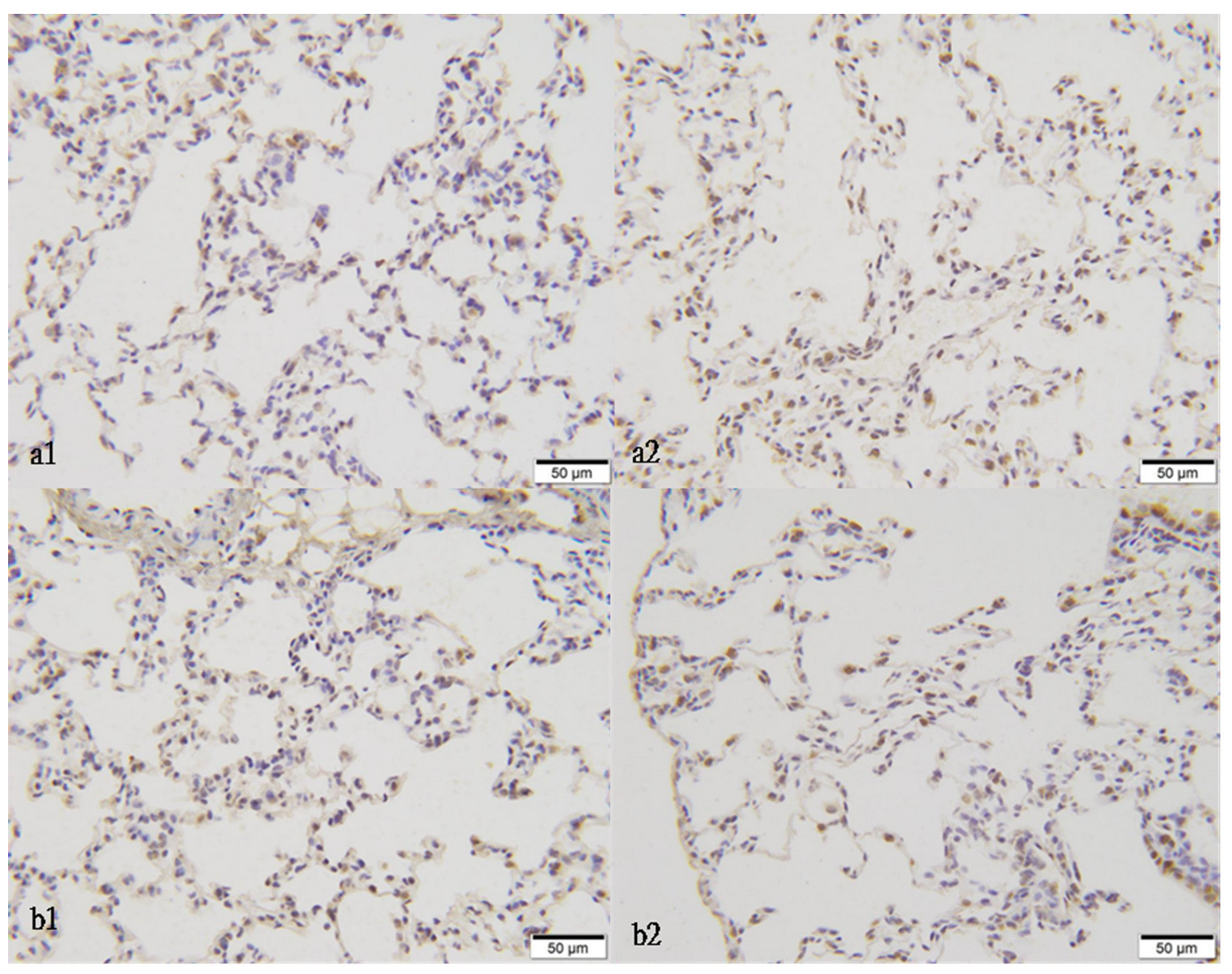
3.3. The Optical Density of NQO1, NRF2, and KEAP1 Immunohistochemistry Staining
3.4. Effect of O3 Exposure on the Serum CRP and IL-6 Levels in Mice
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erickson, L.E.; Newmark, G.L.; Higgins, M.J.; Wang, Z.X. Nitrogen oxides and ozone in urban air: A review of 50 plus years of progress. Environ. Prog. Sustain. Energy 2020, 39, e13484. [Google Scholar] [CrossRef]
- Li, W.; Shao, L.; Wang, W.; Li, H.; Wang, X.; Li, Y.; Li, W.; Jones, T.; Zhang, D. Air quality improvement in response to intensified control strategies in Beijing during 2013–2019. Sci. Total Environ. 2020, 744, 140776. [Google Scholar] [CrossRef]
- Qu, L.; Liu, S.; Ma, L.; Zhang, Z.; Du, J.; Zhou, Y.; Meng, F. Evaluating the meteorological normalized PM trend (2014–2019) in the “2+26” region of China using an ensemble learning technique. Environ. Pollut. 2020, 266, 115346. [Google Scholar] [CrossRef]
- Zheng, B.; Tong, D.; Li, M.; Liu, F.; Hong, C.; Geng, G.; Li, H.; Li, X.; Peng, L.; Qi, J.; et al. Trends in China’s anthropogenic emissions since 2010 as the consequence of clean air actions. Atmos. Chem. Phys. 2018, 18, 14095–14111. [Google Scholar] [CrossRef]
- Zhao, S.; Yin, D.; Yu, Y.; Kang, S.; Qin, D.; Dong, L. PM2.5 and O3 pollution during 2015–2019 over 367 Chinese cities: Spatiotemporal variations, meteorological and topographical impacts. Environ. Pollut. 2020, 264, 114694. [Google Scholar] [CrossRef]
- Ziemke, J.R.; Oman, L.D.; Strode, S.A.; Douglass, A.R.; Olsen, M.A.; McPeters, R.D.; Bhartia, P.K.; Froidevaux, L.; Labow, G.J.; Witte, J.C.; et al. Trends in global tropospheric ozone inferred from a composite record of TOMS/OMI/MLS/OMPS satellite measurements and the MERRA-2 GMI simulation. Atmos. Chem. Phys. 2019, 19, 3257–3269. [Google Scholar] [CrossRef]
- Sillman, S. The relation between ozone, NOx and hydrocarbons in urban and polluted rural environments. Atmos. Environ. 1999, 33, 1821–1845. [Google Scholar] [CrossRef]
- Galiè, M.; Covi, V.; Tabaracci, G.; Malatesta, M. The Role of NRF2 in the Antioxidant Cellular Response to Medical Ozone Exposure. Int. J. Mol. Sci. 2019, 20, 4009. [Google Scholar] [CrossRef]
- Hernández Rosales, F.A.; Calunga Fernández, J.L.; Turrent Figueras, J.; Menéndez Cepero, S.; Montenegro Perdomo, A. Ozone therapy effects on biomarkers and lung function in asthma. Arch. Med. Res. 2005, 36, 549–554. [Google Scholar] [CrossRef]
- Bocci, V.; Borrelli, E.; Travagli, V.; Zanardi, I. The ozone paradox: Ozone is a strong oxidant as well as a medical drug. Med. Res. Rev. 2009, 29, 646–682. [Google Scholar] [CrossRef]
- Santana-Rodríguez, N.; Llontop, P.; Clavo, B.; Fiuza-Pérez, M.D.; Zerecero, K.; Ayub, A.; Alshehri, K.; Yordi, N.A.; Re, L.; Raad, W.; et al. Ozone Therapy Protects Against Rejection in a Lung Transplantation Model: A New Treatment? Ann. Thorac. Surg. 2017, 104, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Jerrett, M.; Pope, I.I.I.C.A.; Krewski, D.; Gapstur, S.M.; Diver, W.R.; Beckerman, B.S.; Marshall, J.D.; Su, J.; Crouse, D.L.; et al. Long-Term Ozone Exposure and Mortality in a Large Prospective Study. Am. J. Respir. Crit. Care Med. 2016, 193, 1134–1142. [Google Scholar] [CrossRef] [PubMed]
- Paulin, L.M.; Gassett, A.J.; Alexis, N.E.; Kirwa, K.; Kanner, R.E.; Peters, S.; Krishnan, J.A.; Paine, R.; Dransfield, M.; Woodruff, P.G.; et al. Association of Long-term Ambient Ozone Exposure with Respiratory Morbidity in Smokers. JAMA Intern. Med. 2020, 180, 106–115. [Google Scholar] [CrossRef]
- Wang, M.; Aaron, C.P.; Madrigano, J.; Hoffman, E.A.; Angelini, E.; Yang, J.; Laine, A.; Vetterli, T.M.; Kinney, P.L.; Sampson, P.D.; et al. Association Between Long-term Exposure to Ambient Air Pollution and Change in Quantitatively Assessed Emphysema and Lung Function. JAMA 2019, 322, 546–556. [Google Scholar] [CrossRef]
- Bell, M.L.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Ozone and short-term mortality in 95 US urban communities, 1987–2000. JAMA 2004, 292, 2372–2378. [Google Scholar] [CrossRef] [PubMed]
- Vicedo-Cabrera, A.M.; Sera, F.; Liu, C.; Armstrong, B.; Milojevic, A.; Guo, Y.; Tong, S.; Lavigne, E.; Kyselý, J.; Urban, A.; et al. Short term association between ozone and mortality: Global two stage time series study in 406 locations in 20 countries. BMJ 2020, 368, m108. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Yao, M.; Wu, W.; Zhao, X.; Zhang, J. Spatiotemporal assessment of health burden and economic losses attributable to short-term exposure to ground-level ozone during 2015–2018 in China. BMC Public Health 2021, 21, 1069. [Google Scholar] [CrossRef]
- Liang, S.; Sun, C.; Liu, C.; Jiang, L.; Xie, Y.; Yan, S.; Jiang, Z.; Qi, Q.; Zhang, A. The Influence of Air Pollutants and Meteorological Conditions on the Hospitalization for Respiratory Diseases in Shenzhen City, China. Int. J. Environ. Res. Public Health 2021, 18, 5120. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Xu, M.; Wang, M.; Wang, L.; Wang, H.; Zhang, H.; Chen, Y.; Gong, J.; Zhang, J.J.; Adcock, I.M.; et al. Roles of mitochondrial ROS and NLRP3 inflammasome in multiple ozone-induced lung inflammation and emphysema. Respir. Res. 2018, 19, 230. [Google Scholar] [CrossRef]
- Bromberg, P.A. Mechanisms of the acute effects of inhaled ozone in humans. Biochim. Biophys. Acta 2016, 1860, 2771–2781. [Google Scholar] [CrossRef] [PubMed]
- Wiegman, C.H.; Li, F.; Clarke, C.J.; Jazrawi, E.; Kirkham, P.; Barnes, P.J.; Adcock, I.M.; Chung, K.F. A comprehensive analysis of oxidative stress in the ozone-induced lung inflammation mouse model. Clin. Sci. 2014, 126, 425–440. [Google Scholar] [CrossRef]
- Chung, K.F.; Togbe, D.; Ryffel, B. Editorial: Ozone as a Driver of Lung Inflammation and Innate Immunity and as a Model for Lung Disease. Front. Immunol. 2021, 12, 714161. [Google Scholar] [CrossRef]
- Dai, Y.; Qiu, H.; Sun, S.; Yang, Y.; Lin, H.; Tian, L. Age-dependent effect of ambient ozone on emergency asthma hospitalizations in Hong Kong. J. Allergy Clin. Immunol. 2018, 141, 1532–1534.e5. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.; Neugebauer, R.; Lurmann, F.; Hall, J.; Brajer, V.; Alcorn, S.; Tager, I. Ambient ozone concentrations cause increased hospitalizations for asthma in children: An 18-year study in Southern California. Environ. Health Perspect. 2008, 116, 1063–1070. [Google Scholar] [CrossRef]
- Li, X.; Chen, Q.; Zheng, X.; Li, Y.; Han, M.; Liu, T.; Xiao, J.; Guo, L.; Zeng, W.; Zhang, J.; et al. Effects of ambient ozone concentrations with different averaging times on asthma exacerbations: A meta-analysis. Sci. Total Environ. 2019, 691, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Shmool, J.L.C.; Kinnee, E.; Sheffield, P.E.; Clougherty, J.E. Spatio-temporal ozone variation in a case-crossover analysis of childhood asthma hospital visits in New York City. Environ. Res. 2016, 147, 108–114. [Google Scholar] [CrossRef]
- Gao, H.; Wang, K.; WAu, W.; Zhao, W.; Xia, Z.-L. A Systematic Review and Meta-Analysis of Short-Term Ambient Ozone Exposure and COPD Hospitalizations. Int. J. Environ. Res. Public Health 2020, 17, 2130. [Google Scholar] [CrossRef]
- Kesic, M.J.; Meyer, M.; Bauer, R.; Jaspers, I. Exposure to ozone modulates human airway protease/antiprotease balance contributing to increased influenza A infection. PLoS ONE 2012, 7, e35108. [Google Scholar] [CrossRef] [PubMed]
- Purvis, M.R.; Miller, S.; Ehrlich, R. Effect of atmospheric pollutants on susceptibility to respiratory infection. I. Effect of ozone. J. Infect. Dis. 1961, 109, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Farhat, S.C.L.; Almeida, M.B.; Silva-Filho, L.V.R.F.; Farhat, J.; Rodrigues, J.C.; Braga, A.L.F. Ozone is associated with an increased risk of respiratory exacerbations in patients with cystic fibrosis. Chest 2013, 144, 1186–1192. [Google Scholar] [CrossRef]
- Tu, W.; Wang, H.; Li, S.; Liu, Q.; Sha, H. The Anti-Inflammatory and Anti-Oxidant Mechanisms of the KEAP1/NRF2/ARE Signaling Pathway in Chronic Diseases. Aging Dis. 2019, 10, 637–651. [Google Scholar] [CrossRef] [PubMed]
- Bellezza, I.; Giambanco, I.; Minelli, A.; Donato, R. NRF2-KEAP1 signaling in oxidative and reductive stress. Biochim. Biophys. Acta Mol. Cell Res. 2018, 1865, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.-C.; Ji, J.-A.; Jiang, Z.-Y.; You, Q.-D. The KEAP1-NRF2-ARE Pathway as a Potential Preventive and Therapeutic Target: An Update. Med. Res. Rev. 2016, 36, 924–963. [Google Scholar] [CrossRef] [PubMed]
- Erickson, M.A.; Jude, J.; Zhao, H.; Rhea, E.M.; Salameh, T.S.; Jester, W.; Pu, S.; Harrowitz, J.; Nguyen, N.; Banks, W.A.; et al. Serum amyloid A: An ozone-induced circulating factor with potentially important functions in the lung-brain axis. FASEB J. 2017, 31, 3950–3965. [Google Scholar] [CrossRef] [PubMed]
- Hatch, G.E.; Slade, R.; Harris, L.P.; McDonnell, W.F.; Devlin, R.B.; Koren, H.S.; Costa, D.L.; McKee, J. Ozone dose and effect in humans and rats. A comparison using oxygen-18 labeling and bronchoalveolar lavage. Am. J. Respir. Crit. Care Med. 1994, 150, 676–683. [Google Scholar] [CrossRef]
- Slade, R.; Stead, A.G.; Graham, J.A.; Hatch, G.E. Comparison of lung antioxidant levels in humans and laboratory animals. Am. Rev. Respir. Dis. 1985, 131, 742–746. [Google Scholar] [CrossRef]
- Gross, K.B.; White, H.J. Functional and pathologic consequences of a 52-week exposure to 0.5 PPM ozone followed by a clean air recovery period. Lung 1987, 165, 283–295. [Google Scholar] [CrossRef]
- Hagar, W.L.; Sweet, W.E.; Sweet, F. An in vitro system for assessing lung cell response to ozone. J. Air Pollut. Control. Assoc. 1981, 31, 933–935. [Google Scholar] [CrossRef]
- Stephens, R.J.; Evans, M.J.; Sloan, M.F.; Freeman, G. A comprehensive ultrastructural study of pulmonary injury and repair in the rat resulting from exposures to less than one PPM ozone. Chest 1974, 65, 11S–13S. [Google Scholar] [CrossRef]
- Boatman, E.S.; Frank, R. Morphologic and ultrastructural changes in the lungs of animals during acute exposure to ozone. Chest 1974, 65, 9S–11S. [Google Scholar] [CrossRef]
- López, I.; Sánchez, I.; Bizarro, P.; Acevedo, S.; Ustarroz, M.; Fortoul, T. Ultrastructural alterations during embryonic rats’ lung development caused by ozone. J. Electron. Microsc. 2008, 57, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Bils, R.F. Effects of nitrogen dioxide and ozone on monkey lung ultrastructure. Pneumonologie 1974, 150, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Cervellati, F.; Woodby, B.; Benedusi, M.; Ferrara, F.; Guiotto, A.; Valacchi, G. Evaluation of oxidative damage and NRF2 activation by combined pollution exposure in lung epithelial cells. Environ. Sci. Pollut. Res. Int. 2020, 27, 31841–31853. [Google Scholar] [CrossRef]
- Kummarapurugu, A.B.; Fischer, B.M.; Zheng, S.; Milne, G.L.; Ghio, A.J.; Potts-Kant, E.N.; Foster, W.M.; Soderblom, E.J.; Dubois, L.G.; Moseley, M.A.; et al. NADPH:quinone oxidoreductase 1 regulates host susceptibility to ozone via isoprostane generation. J. Biol. Chem. 2013, 288, 4681–4691. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, J.; Wu, Z.; Lu, Y.; You, H.; Li, R.; Li, B.; Yang, X.; Duan, L. Acute exposure of ozone induced pulmonary injury and the protective role of vitamin E through the NRF2 pathway in Balb/c mice. Toxicol. Res. 2015, 5, 268–277. [Google Scholar] [CrossRef]
- Shah, M.; Captain, J.; Vaidya, V.; Kulkarni, A.; Valsangkar, K.; Nair, P.M.; Ganu, G. Safety and efficacy of ozone therapy in mild to moderate COVID-19 patients: A phase 1/11 randomized control trial (SEOT study). Inter. Immunopharmacol. 2021, 91, 107301. [Google Scholar] [CrossRef] [PubMed]
- Epelle, E.I.; Macfarlane, A.; Cusack, M.; Burns, A.; Thissera, B.; Mackay, W.; Rateb, M.E.; Yaseen, M. Bacterial and fungal disinfection via ozonation in air. J. Microbiol. Methods 2022, 194, 106431. [Google Scholar] [CrossRef]
- Wu, Q.; Wan, M.; Li, Q.; Fu, Z. Study on the measurement method of vacuum ultraviolet (185 nm) radiation and ozone output production characteristics of ultraviolet lamps. China Lighting Electr. Appl. 2021, 8, 20. [Google Scholar]
- Voelker, R. Warning about cleaning CPAP devices with ozone gas, UV light. JAMA 2020, 323, 1236. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exposure Days | Groups | NQO1 | NRF2 | KEAP1 |
|---|---|---|---|---|
| 15 | control | 1.36 ± 1.14 | 1.12 ± 0.40 | 1.84 ± 1.29 |
| O3 | 3.46 ± 1.80 * | 2.49 ± 2.25 | 2.41 ± 0.98 | |
| 30 | control | 2.83 ± 1.09 | 2.27 ± 0.80 | 1.96 ± 0.46 |
| O3 | 2.77 ± 1.26 | 1.74 ± 1.26 | 1.73 ± 1.17 |
| Group | 15 Days | 30 Days | ||
|---|---|---|---|---|
| CRP | IL-6 | CRP | IL-6 | |
| Control | ||||
| Female | 421.48 ± 43.18 | 32.49 ± 3.57 | 425.68 ± 45.75 | 33.28 ± 3.69 |
| Male | 419.24 ± 39.28 | 32.49 ± 3.57 | 435.76 ± 42.71 | 33.28 ± 3.23 |
| O3 | ||||
| Female | 569.51 ± 41.23 * | 67.57 ± 6.51 * | 651.37 ± 46.27 * | 53.24 ± 7.54 * |
| Male | 567.47 ± 40.21 * | 62.91 ± 5.79 * | 629.69 ± 45.15 * | 69.38 ± 6.67 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, S.; Sha, Y.; Yang, C.; Lai, H.; Sun, C.; Zhao, W.; Zhang, A.; Qi, Q.; Xie, Y. Ozone-Induced Lung and Bronchial Injury: A Mouse Model Study. Atmosphere 2022, 13, 1562. https://doi.org/10.3390/atmos13101562
Liang S, Sha Y, Yang C, Lai H, Sun C, Zhao W, Zhang A, Qi Q, Xie Y. Ozone-Induced Lung and Bronchial Injury: A Mouse Model Study. Atmosphere. 2022; 13(10):1562. https://doi.org/10.3390/atmos13101562
Chicago/Turabian StyleLiang, Shi, Yan Sha, Chuanhong Yang, Huangwen Lai, Chong Sun, Weisen Zhao, An Zhang, Qingwen Qi, and Ying Xie. 2022. "Ozone-Induced Lung and Bronchial Injury: A Mouse Model Study" Atmosphere 13, no. 10: 1562. https://doi.org/10.3390/atmos13101562
APA StyleLiang, S., Sha, Y., Yang, C., Lai, H., Sun, C., Zhao, W., Zhang, A., Qi, Q., & Xie, Y. (2022). Ozone-Induced Lung and Bronchial Injury: A Mouse Model Study. Atmosphere, 13(10), 1562. https://doi.org/10.3390/atmos13101562