


Prevalence Distribution of Chronic Obstructive Pulmonary Disease (COPD) in the City of Osorno (Chile) in 2018, and Its Association with Fine Particulate Matter PM2.5 Air Pollution

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approval
2.2. COPD Patients’ Information, Adjusted Prevalence, and Odds Ratio
2.3. Territorial Analysis
2.4. PM2.5 Air Pollution Data and Measurements
2.5. Statistical Analyses
3. Results
3.1. Sociodemographic Data
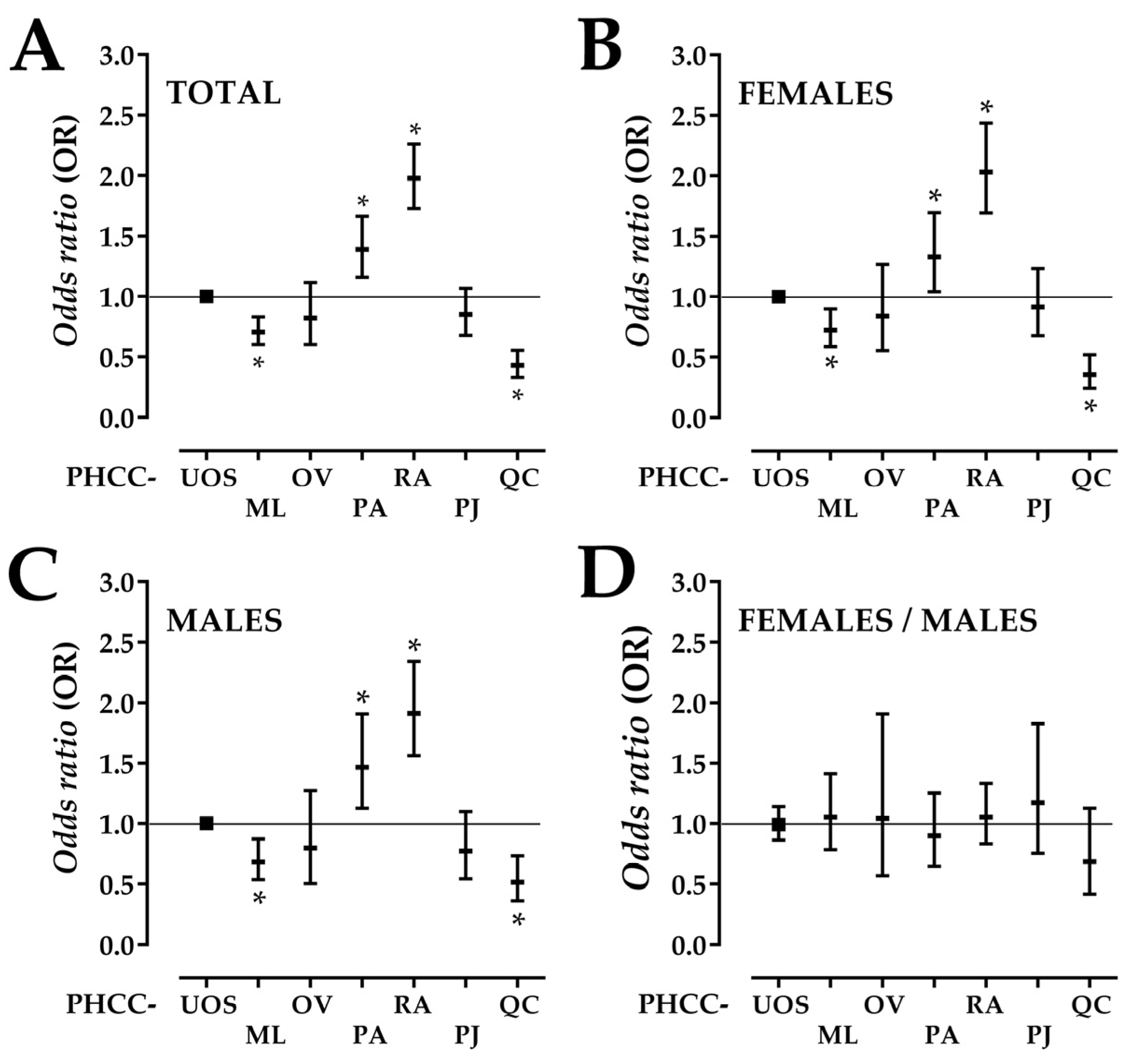
3.2. COPD Adjusted Prevalence and Odds Ratio
3.3. PM2.5 Outdoor Air Pollution in Osorno
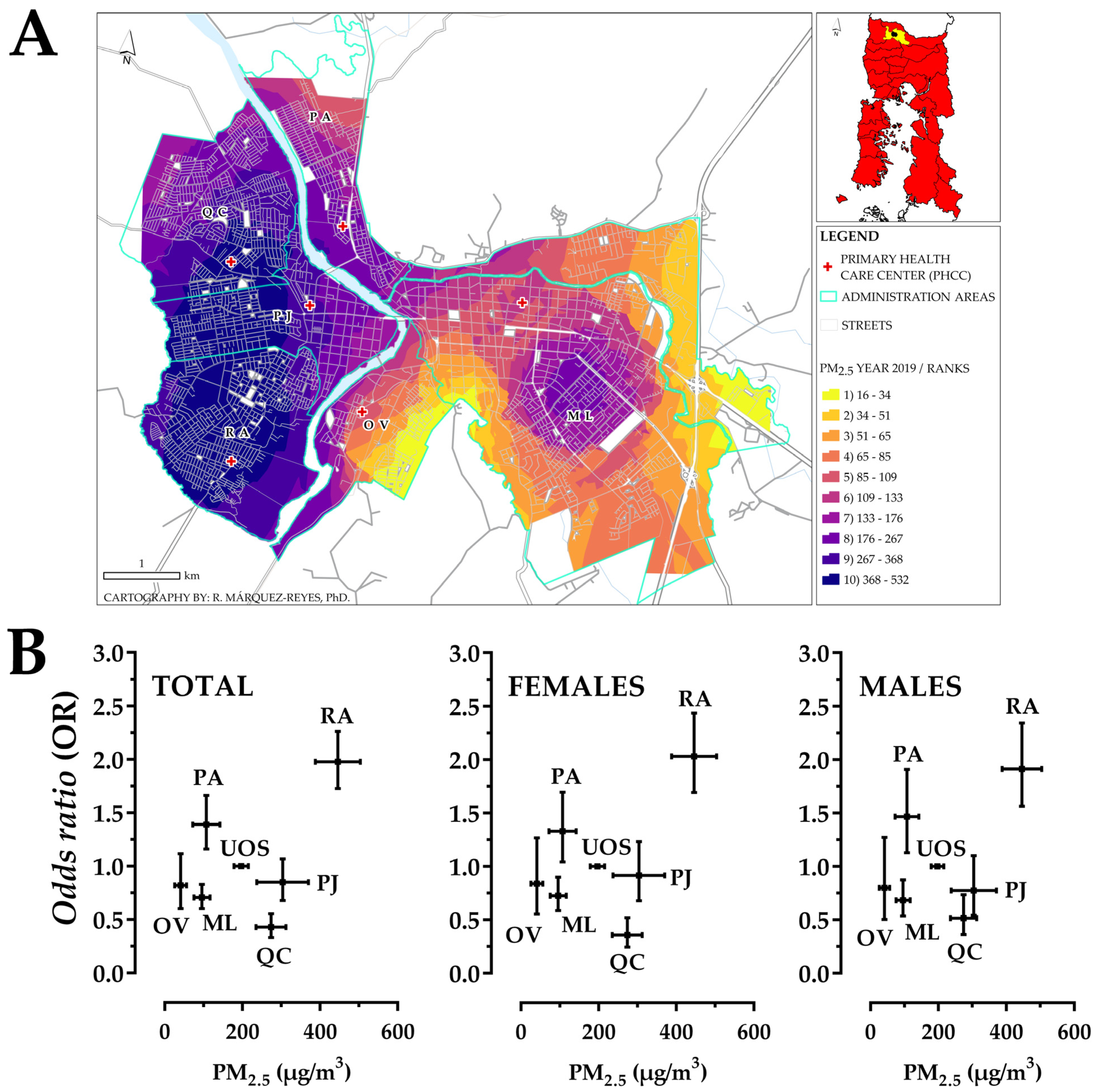
3.4. Territorial PM2.5 Air Pollution
3.5. COPD Patient Distribution in Osorno
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Campos, A.A.; Cabrera, R.O.; Arancibia, H.F. Rehabilitación respiratoria en pacientes EPOC: Experiencia en Atención Primaria de Salud. [Respiratory rehabilitation in COPD patients: Experience in a rural Primary Health Care Center]. Rev. Chil. Enferm. Respir. 2015, 31, 77–85. [Google Scholar] [CrossRef]
- Silva, R. Enfermedad pulmonar obstructiva crónica: Mirada actual a una enfermedad emergente. [Update on chronic obstructive pulmonary disease]. Rev. Med. Chil. 2010, 138, 1544–1552. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Venegas, A.; Torres-Duque, C.A.; Guzman-Bouilloud, N.E.; Gonzalez-Garcia, M.; Sansores, R.H. Small airway disease in COPD associated to biomass exposure. Rev. Investig. Clin. 2019, 71, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; Aichour, M.T.E.; Alam, K.; et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, 2011–2030. [Google Scholar] [CrossRef] [PubMed]
- Lopez, M.; Mongilardi, N.; Checkley, W. Enfermedad pulmonar obstructiva crónica por exposición al humo de biomasa. [Chronic obstructive pulmonary disease by biomass smoke exposure]. Rev. Peru. Med. Exp. Salud Pública 2014, 31, 94–99. [Google Scholar] [PubMed]
- Salvi, S.S.; Barnes, P.J. Is Exposure to Biomass Smoke the Biggest Risk Factor for COPD Globally? Chest 2010, 138, 3–6. [Google Scholar] [CrossRef]
- Adeloye, D.; Chua, S.; Lee, C.; Basquill, C.; Papana, A.; Theodoratou, E.; Nair, H.; Gasevic, D.; Sridhar, D.; Campbell, H.; et al. Global and regional estimates of COPD prevalence: Systematic review and meta-analysis. J. Glob. Health 2015, 5, 020415. [Google Scholar] [CrossRef]
- Menezes, A.M.B.; Perez-Padilla, R.; Jardim, J.R.B.; Muiño, A.; Lopez, M.V.; Valdivia, G.; Montes de Oca, M.; Talamo, C.; Hallal, P.C.; Victora, C.G. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): A prevalence study. Lancet 2005, 366, 1875–1881. [Google Scholar] [CrossRef]
- Dockery, D.W.; Pope, C.A., III; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G., Jr.; Speizer, F.E. An Association between Air Pollution and Mortality in Six U.S. Cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef]
- Pope, C.A., III. Epidemiology of fine particulate air pollution and human health: Biologic mechanisms and who’s at risk? Environ. Health Perspect. 2000, 108 (Suppl. S4), 713–723. [Google Scholar] [CrossRef]
- Liu, S.; Zhou, Y.; Liu, S.; Chen, X.; Zou, W.; Zhao, D.; Li, X.; Pu, J.; Huang, L.; Chen, J.; et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: Results from a cross-sectional study in China. Thorax 2017, 72, 788–795. [Google Scholar] [CrossRef]
- Salvi, S.S.; Barnes, P.J. Chronic obstructive pulmonary disease in non-smokers. Lancet 2009, 374, 733–743. [Google Scholar] [CrossRef]
- Amable Álvarez, I.; Méndez Martínez, J.; Bello Rodríguez, B.M.; Benítez Fuentes, B.; Escobar Blanco, L.M.; Zamora Monzón, R. Influencia de los contaminantes atmosféricos sobre la salud. [Atmospheric contaminants influence on health]. Rev. Med. Electrón. 2017, 39, 1160–1170. Available online: https://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242017000500017&lng=es&tlng=es (accessed on 27 February 2024).
- Oyarzún, M. Contaminación aérea y sus efectos en la salud. [Air pollution and its effects on health]. Rev. Chil. Enferm. Respir. 2010, 26, 16–25. [Google Scholar] [CrossRef]
- Xia, X.; Yao, L.; Lu, J.; Liu, Y.; Jing, W.; Li, Y. A Comparison Analysis of Causative Impact of PM2.5 on Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD) in Two Typical Cities in China. Atmosphere 2021, 12, 970. [Google Scholar] [CrossRef]
- Román, O.; Prieto, M.J.; Mancilla, P.; Astudillo, P.; Dussaubat, A.M.; Miguel, C.; Lara, J. Daño cardiovascular por material particulado del aire. Puesta al día 2008. [Association between air pollution and cardiovascular risk]. Rev. Med. Chil. 2009, 137, 1217–1224. [Google Scholar] [CrossRef]
- World Health Organization, WHO. Ambient (Outdoor) Air Pollution. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 7 November 2023).
- Samet, J.M.; Dominici, F.; Curriero, F.C.; Coursac, I.; Zeger, S.L. Fine Particulate Air Pollution and Mortality in 20 U.S. Cities, 1987–1994. N. Engl. J. Med. 2000, 343, 1742–1749. [Google Scholar] [CrossRef]
- Pope, C.A., III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- World Health Organization, WHO. Household Air Pollution. Available online: https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health#:~:text=Household%20air%20pollution%20was%20responsible,6.7%20million%20premature%20deaths%20annually (accessed on 8 November 2023).
- Zhang, J.; Lin, X.; Bai, C. Comparison of clinical features between non-smokers with COPD and smokers with COPD: A retrospective observational study. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 57–63. [Google Scholar] [CrossRef]
- Ministerio del Medio Ambiente, Chile. Decreto 27, 2012. Declara Zona Saturada por Material Particulado Respirable MP10, Como Concentración Diaria y Anual, y Por Material Particulado Fino Respirable MP2.5, Como Concentración Diaria y Anual, a la Comuna de Osorno. [Decree 27. Declares Saturated Area by Breathable Particulate Matter PM10, as a Daily and Annual Concentration, and by Fine Breathable Particulate Matter PM2.5, as a Daily and Annual Concentration, the Commune of Osorno]. Available online: https://www.bcn.cl/leychile/navegar?idNorma=1046121&idParte=0&idVersion= (accessed on 8 November 2023).
- Ministerio del Medio Ambiente, Chile. Decreto 47, 2016. Establece Plan de Descontaminación Atmosférica para la Comuna de Osorno. [Decree 47. Establishes Atmospheric Decontamination Plan for the Commune of Osorno]. Available online: https://www.bcn.cl/leychile/navegar?i=1088771&f=2022-11-03 (accessed on 8 November 2023).
- Instituto Nacional de Estadísticas, INE, Chile. Resultados Censo 2017. [Census 2017 Results]. Available online: http://resultados.censo2017.cl/Region?R=R10 (accessed on 8 November 2023).
- Bustos, Y.; Ferrada, L.M. Consumo Residencial de Leña, Análisis para la Ciudad de Osorno en Chile. [Residential Consumption of Firewood, an Analysis of the City of Osorno in Chile]. Idesia 2017, 35, 95–105. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadísticas, INE, Chile. Microdatos Censo 2017. [Census 2017 Microdata]. Available online: http://www.censo2017.cl/microdatos/ (accessed on 8 November 2023).
- Esri. Enable Feature Binning (Data Management). Available online: https://pro.arcgis.com/en/pro-app/latest/tool-reference/data-management/enable-feature-binning.htm (accessed on 12 December 2023).
- Sharma, P.; Martin, M.; Swanlund, D. MapSafe: A complete tool for achieving geospatial data sovereignty. Trans. GIS 2023, 27, 1680–1698. [Google Scholar] [CrossRef]
- Ministerio del Medio Ambiente, Chile. Sistema Nacional de Información de Calidad del Aire, SINCA. Osorno Air Quality Monitoring Station. Available online: https://sinca.mma.gob.cl/index.php/estacion/index/key/A01 (accessed on 12 December 2023).
- Nakamura, A.; Nakatani, N.; Maruyama, F.; Fujiyoshi, S.; Márquez-Reyes, R.; Fernández, R.; Noda, J. Characteristics of PM2.5 pollution in Osorno, Chile: Ion chromatography and meteorological data analyses. Atmosphere 2022, 13, 168. [Google Scholar] [CrossRef]
- Saide, P.E.; Mena-Carrasco, M.; Tolvett, S.; Hernandez, P.; Carmichael, G.R. Air quality forecasting for winter-time PM2.5 episodes occurring in multiple cities in central and southern Chile. J. Geophys. Res. Atmos 2016, 121, 558–575. [Google Scholar] [CrossRef]
- Adeloye, D.; Song, P.; Zhu, Y.; Campbell, H.; Sheikh, A.; Rudan, I.; NIHR RESPIRE Global Respiratory Health Unit. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet Respir. Med. 2022, 10, 447–458. [Google Scholar] [CrossRef]
- Schiavi, E.; Stirbulov, R.; Hernández Vecino, R.; Mercurio, S.; Di Boscio, V. COPD Screening in primary care in four Latin American countries: Methodology of the PUMA study. Arch. Bronconeumol. 2014, 50, 469–474. [Google Scholar] [CrossRef]
- Casas Herrera, A.; Montes de Oca, M.; López Varela, M.V.; Aguirre, C.; Schiavi, E.; Jardim, J.R.; PUMA Team. COPD underdiagnosis and misdiagnosis in a high-risk primary care population in four Latin American countries. A key to enhance disease diagnosis: The PUMA Study. PLoS ONE 2016, 11, e0152266. [Google Scholar] [CrossRef]
- Lamprecht, B.; Soriano, J.B.; Studnicka, M.; Kaiser, B.; Vanfleteren, L.E.; Gnatiuc, L.; Burney, P.; Miravitlles, M.; García-Rio, F.; Akbari, K.; et al. Determinants of underdiagnosis of COPD in national and international surveys. Chest 2015, 148, 971–985. [Google Scholar] [CrossRef]
- Vandevoorde, J.; Verbanck, S.; Gijssels, L.; Schuermans, D.; Devroey, D.; De Backer, J.; Kartounian, J.; Vincken, W. Early detection of COPD: A case finding study in general practice. Respir. Med. 2007, 101, 525–530. [Google Scholar] [CrossRef]
- Bednarek, M.; Maciejewski, J.; Wozniak, M.; Kuca, P.; Zielinski, J. Prevalence, severity and underdiagnosis of COPD in the primary care setting. Thorax 2008, 63, 402–407. [Google Scholar] [CrossRef]
- Fukuchi, Y.; Nishimura, M.; Ichinose, M.; Adachi, M.; Nagai, A.; Kuriyama, T.; Takahashi, K.; Nishimura, K.; Ishioka, S.; Aizawa, H.; et al. COPD in Japan: The nippon COPD epidemiology study. Respirology 2004, 9, 458–465. [Google Scholar] [CrossRef]
- Peña, V.S.; Miravitlles, M.; Gabriel, R.; Jiménez-Ruiz, C.A.; Villasante, C.; Masa, J.F.; Viejo, J.L.; Fernández-Fau, L. Geographic variations in prevalence and underdiagnosis of COPD: Results of the IBERPOC multicenter epidemiological study. Chest 2000, 118, 981–989. [Google Scholar] [CrossRef]
- Ancochea, J.; Badiola, C.; Duran-Tauleria, E.; Garcia Rio, F.; Miravitlles, M.; Muñoz, L.; Sobradillo, V.; Soriano, J.B. Estudio EPI-SCAN: Resumen del protocolo de un estudio para estimar la prevalencia de EPOC en personas de 40 a 80 años en España. [The EPI-SCAN survey to assess the prevalence of chronic obstructive pulmonary disease in Spanish 40-to-80-year-olds: Protocol summary]. Archi. Bronconeumol. 2009, 45, 41–47. [Google Scholar] [CrossRef]
- Drope, J.; Hamill, S.; Chaloupka, F.; Guerrero, C.; Lee, H.M.; Mirza, M.; Mouton, A.; Murukutla, M.; Ngo, A.; Perl, R.; et al. The Tobacco Atlas. Vital Strategies and Tobacconomics: New York, NY, USA, 2022. Available online: https://tobaccoatlas.org/factsheets/chile/ (accessed on 10 January 2024).
- Alonso, T.; Sobradillo, P.; De Torres, J.P. Chronic obstructive pulmonary disease in women. Is it different? Arch. Bronconeumol. 2017, 53, 222–227. [Google Scholar] [CrossRef]
- Varkey, A.B. Chronic obstructive pulmonary disease in women: Exploring gender differences. Curr. Op. Pulm. Med. 2004, 10, 98–103. [Google Scholar] [CrossRef]
- De Torres, J.P.; Casanova, C. EPOC en la mujer. [Chronic obstructive pulmonary disease in women]. Arch. Bronconeumol. 2010, 46 (Suppl. 3), 23–27. [Google Scholar] [CrossRef]
- Díaz, L.A.; Carimán, E.; Moncada, J. Estudio de Consumo y Caracterización del Uso de la Leña en la Ciudad de Osorno, 2013. [Consumption and Characterization of the Use of Firewood in the City of Osorno, 2013]. Air Quality Unit, Catholic University of Temuco. Available online: https://planesynormas.mma.gob.cl/archivos/2014/proyectos/4._Estudio_de_Caracterizacion_del_Consumo_de_Lena_en_Osorno__UCT_2013_.pdf (accessed on 10 January 2024).
- Tabak, C.; Spijkerman, A.M.W.; Verschuren, W.M.M.; Smit, H.A. Does educational level influence lung function decline (Doetinchem Cohort Study)? Eur. Respir. J. 2009, 34, 940–947. [Google Scholar] [CrossRef]
- World Health Organization, WHO. WHO Global Air Quality Guidelines, 2021. Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide. Geneva. License: CCBY-NC-SA 3.0 IGO. Available online: https://www.who.int/publications/i/item/9789240034228 (accessed on 13 January 2024).
- Ministerio del Medio Ambiente, Chile. Decreto 12, 2012. Establece la Norma Primaria de Calidad Ambiental para Material Particulado Fino Respirable MP2.5. [Decree 12, 2012. Establishes the Primary Environmental Quality Standard for Fine Particulate Matter PM2.5]. Available online: https://www.bcn.cl/leychile/navegar?i=1025202&f=2012-01-01&p= (accessed on 13 January 2024).
- DeVries, R.; Kriebel, D.; Sama, S. Outdoor air pollution and COPD-related emergency department visits, hospital admissions, and mortality: A meta-analysis. COPD 2017, 14, 113–121. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, S. The effects and pathogenesis of PM2.5 and its components on chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2023, 18, 493–506. [Google Scholar] [CrossRef]
- Dyer, C.; Pugh, L. Lung health in older adults. Age Ageing 2019, 48, 319–322. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease, GOLD. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2024. Available online: http://www.goldcopd.org/ (accessed on 15 January 2024).
- Li, N.; Ma, J.; Ji, K.; Wang, L. Association of PM2.5 and PM10 with acute exacerbation of chronic obstructive pulmonary disease at lag0 to lag7: A systematic review and meta-analysis. COPD 2022, 19, 243–254. [Google Scholar] [CrossRef]
- Ni, L.; Chuang, C.; Zuo, L. Fine particulate matter in acute exacerbation of COPD. Front. Physiol. 2015, 6, 294. [Google Scholar] [CrossRef]
- Chanel, O.; Perez, L.; Künzli, N.; Medina, S.; Aphekom Group. The hidden economic burden of air pollution-related morbidity: Evidence from the Aphekom project. Eur. J. Health Econ. 2016, 17, 1101–1115. [Google Scholar] [CrossRef]
- Safiri, S.; Carson-Chahhoud, K.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Heris, J.A.; Ansarin, K.; Mansournia, M.A.; Collins, G.S.; Kolahi, A.A.; et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: Results from the Global Burden of Disease Study 2019. BMJ 2022, 378, e069679. [Google Scholar] [CrossRef]
- Sun, Q.; Liu, C.; Chen, R.; Wang, C.; Li, J.; Sun, J.; Kan, H.; Cao, J.; Bai, H. Association of fine particulate matter on acute exacerbation of chronic obstructive pulmonary disease in Yancheng, China. Sci. Total Environ. 2019, 650 Pt 2, 1665–1670. [Google Scholar] [CrossRef]
- Huh, J.Y.; Hong, J.; Han, D.W.; Park, Y.J.; Jung, J.; Lee, S.W. The impact of air pollutants and meteorological factors on chronic obstructive pulmonary disease exacerbations: A nationwide study. Ann. Am. Thorac. Soc. 2022, 19, 214–226. [Google Scholar] [CrossRef]
- Sarkar, C.; Zhang, B.; Ni, M.; Kumari, S.; Bauermeister, S.; Gallacher, J.; Webster, C. Environmental correlates of chronic obstructive pulmonary disease in 96779 participants from the UK Biobank: A cross-sectional, observational study. Lancet Planet Health 2019, 3, e478–e490. [Google Scholar] [CrossRef]
- Park, J.; Kim, H.J.; Lee, C.H.; Lee, C.H.; Lee, H.W. Impact of long-term exposure to ambient air pollution on the incidence of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Environ. Res. 2021, 194, 110703. [Google Scholar] [CrossRef]
- Hsu, H.T.; Wu, C.D.; Chung, M.C.; Shen, T.C.; Lai, T.J.; Chen, C.Y.; Wang, R.Y.; Chung, C.J. The effects of traffic-related air pollutants on chronic obstructive pulmonary disease in the community-based general population. Respir. Res. 2021, 22, 217. [Google Scholar] [CrossRef]
- Junior, D.P.M.; Bueno, C.; da Silva, C.M. The effect of urban green spaces on reduction of particulate matter concentration. Bull. Environ. Contam. Toxicol. 2022, 108, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; Verheij, R.A.; de Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Commun. Health 2009, 63, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Bo, Y.; Chang, L.Y.; Guo, C.; Lin, C.; Lau, A.K.H.; Tam, T.; Lao, X.Q. Reduced ambient PM2.5, better lung function, and decreased risk of chronic obstructive pulmonary disease. Environ. Int. 2021, 156, 106706. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency | % |
|---|---|---|
| Gender | ||
| Female | 446 | 55.1 |
| Male | 363 | 44.9 |
| Age (Years Old) | ||
| 40–49 | 18 | 2.2 |
| 50–59 | 97 | 11.9 |
| 60–69 | 223 | 27.5 |
| 70–79 | 278 | 34.3 |
| 80 and older | 193 | 23.8 |
| Educational Level 1 | ||
| Without educational teaching | 36 | 8.6 |
| Incomplete primary education | 189 | 45.4 |
| Complete primary education | 72 | 17.3 |
| Incomplete secondary education | 38 | 9.1 |
| Complete secondary education | 60 | 14.4 |
| Incomplete higher education | 4 | 0.9 |
| Complete higher education | 17 | 4.1 |
| Ethnicity | ||
| Mapuche | 36 | 4.4 |
| None | 773 | 95.6 |
| Primary Health Care Center (PHCC) 2 | ||
| Marcelo Lopetegui (PHCC-ML) | 184 | 22.7 |
| Ovejería (PHCC-OV) | 43 | 5.3 |
| Pampa Alegre (PHCC-PA) | 144 | 17.8 |
| Rahue Alto (PHCC-RA) | 292 | 36.1 |
| Pedro Jáuregui (PHCC-PJ) | 83 | 10.3 |
| Quinto Centenario (PHCC-QC) | 63 | 7.8 |
| Nationality | ||
| Chilean | 807 | 99.8 |
| Foreigner | 2 | 0.2 |
| Territory | Females | Males | ||||
|---|---|---|---|---|---|---|
| COPD Patients | Population over 40 Years Old 1 | Age-Adjusted Prevalence (Per 1000 Inhabitants) 2 | COPD Patients | Population over 40 Years Old 1 | Age-Adjusted Prevalence (Per 1000 Inhabitants) 2 | |
| UOS | 446 | 34,764 | 13 | 363 | 28,075 | 13 |
| PHCC-ML | 105 | 11,238 | 9 | 79 | 8906 | 9 |
| PHCC-OV | 24 | 2228 | 11 | 19 | 1835 | 10 |
| PHCC-PA | 77 | 4537 | 17 | 67 | 3557 | 19 |
| PHCC-RA | 162 | 6302 | 26 | 130 | 5320 | 24 |
| PHCC-PJ | 49 | 4170 | 12 | 34 | 3391 | 10 |
| PHCC-QC | 29 | 6289 | 5 | 34 | 5066 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández, R.; Peña, R.; Bravo-Alvarado, J.; Maisey, K.R.; Reyes, E.P.; Ruiz-Plaza De Los Reyes, D.; Márquez-Reyes, R. Prevalence Distribution of Chronic Obstructive Pulmonary Disease (COPD) in the City of Osorno (Chile) in 2018, and Its Association with Fine Particulate Matter PM2.5 Air Pollution. Atmosphere 2024, 15, 482. https://doi.org/10.3390/atmos15040482
Fernández R, Peña R, Bravo-Alvarado J, Maisey KR, Reyes EP, Ruiz-Plaza De Los Reyes D, Márquez-Reyes R. Prevalence Distribution of Chronic Obstructive Pulmonary Disease (COPD) in the City of Osorno (Chile) in 2018, and Its Association with Fine Particulate Matter PM2.5 Air Pollution. Atmosphere. 2024; 15(4):482. https://doi.org/10.3390/atmos15040482
Chicago/Turabian StyleFernández, Ricardo, Romina Peña, Jaime Bravo-Alvarado, Kevin R. Maisey, Edison P. Reyes, Daniel Ruiz-Plaza De Los Reyes, and Rodrigo Márquez-Reyes. 2024. "Prevalence Distribution of Chronic Obstructive Pulmonary Disease (COPD) in the City of Osorno (Chile) in 2018, and Its Association with Fine Particulate Matter PM2.5 Air Pollution" Atmosphere 15, no. 4: 482. https://doi.org/10.3390/atmos15040482
APA StyleFernández, R., Peña, R., Bravo-Alvarado, J., Maisey, K. R., Reyes, E. P., Ruiz-Plaza De Los Reyes, D., & Márquez-Reyes, R. (2024). Prevalence Distribution of Chronic Obstructive Pulmonary Disease (COPD) in the City of Osorno (Chile) in 2018, and Its Association with Fine Particulate Matter PM2.5 Air Pollution. Atmosphere, 15(4), 482. https://doi.org/10.3390/atmos15040482